

Abstract
Objective:
We examine the importance of early life displacement and nutrition on hypertension (HTN) and diabetes in older Colombian adults (60+ years) exposed to rapid demographic, epidemiological, and nutritional transitions, and armed conflict. We compare early life nutritional status and adult health in other middle- and high-income countries.
Method:
In Colombia (Survey of Health, Wellbeing and Aging [SABE]-Bogotá), we estimate the effects of early life conditions (displacement due to armed conflict and violence, hunger, low height, and not born in the capital city) and obesity on adult health; we compare the effects of low height on adult health in Mexico, South Africa (Study on Global Ageing and Adult Health [SAGE]), the United States, and England (Health and Retirement Study [HRS], English Longitudinal Study of Ageing [ELSA]).
Results:
Early life displacement, early poor nutrition, and adult obesity increase the risk of HTN and diabetes in Colombia. Being short is most detrimental for HTN in Colombian males.
Discussion:
Colombian data provide new evidence into how early life conditions and adult obesity contribute to older adult health.
Keywords: early life, displacement due to violence, hypertension, diabetes, obesity, middle-income countries
Introduction
Heart disease, diabetes, and obesity are increasing in the developing world as the population of older adults steadily increases (He, Goodkind, & Kowal, 2016; NCD Risk Factor Collaboration, 2016; World Health Organization [WHO], 2016), adding to the burden for individuals and on health care systems. Middle-income countries are of particular interest because they are experiencing a high prevalence of chronic disease and obesity (He et al., 2016; WHO, 2016), in particular in urban areas (Ibrahim & Damasceno, 2012).
The determinants of these health conditions may be different in the developing world due to unique demographic, epidemiological, and nutritional histories of the 20th century. Rapid demographic transitions produced dramatically improved life expectancy at young ages but occurred mostly without parallel improvements in standards of living (Palloni & Souza, 2013). The rapid mortality decline resulted in cohorts largely characterized by survivorship of poor early life conditions, in particular poor or inadequate nutrition and infectious diseases. Rapid epidemiological transitions resulted in a double burden of infectious diseases, chronic conditions and obesity (Albala, Vio, & Yáüez, 1997; Filozof, Gonzalez, Sereday, Mazza, & Braguinsky, 2001; Samper-Ternent, Michaels-Obregón, Wong, & Palloni, 2012), and rapid nutritional changes produced dramatic differences between early and later life nutritional environments (Food and Agriculture Organization [FAO], 1946, 2016).
These historical circumstances add to the complexity of understanding older adult health in middle-income countries. National context and differences in environmental factors matter in terms of interpreting cross-national health patterns (Hebert et al., 1998). While adult lifestyle is an important determinant of older adult health in developed economies (Kuh & Ben-Shlomo, 2004), other factors such as early life conditions are particularly relevant in middle-income countries. If poor early life conditions affect older adult health, older adults born in the cohorts produced from these historical circumstances may be more susceptible to the long-term effects of poor early life conditions. In contrast with middle-income countries, the demographic, epidemiological, and nutritional transitions of the 20th century affecting high-income countries were more gradual and occurred earlier in the 20th century in the context of improvement in standard of living (McEniry, 2014). These very different historical circumstances affecting health provide relevant explanations for explaining differences in the health of older adults in middle- and high-income countries.
Early Life Conditions
There is ample evidence that exposure to poor nutrition and infectious diseases in early life increases the risk of chronic conditions and obesity at older ages. Inadequate nutrition in utero during critical periods can lead to poor intrauterine and postbirth growth, low birth weight and stunted babies, and an increased risk of heart disease, diabetes, and obesity at older ages (Barker, 1998). Because obesity is an important risk factor for both heart disease and diabetes, poor early life conditions that increase the risk of obesity could also increase the risk of heart disease and/or diabetes later in life. Differences in how poor early life nutrition in early life affect males and females could produce subsequent differences in older adult health for heart disease and diabetes (Eriksson, Kajantie, Osmond, Thornburg, & Barker, 2010; Janghorbani, Momeni, & Dehghani, 2012; Song et al., 2016). Infectious diseases and persistent inflammation due to infections in early life can damage organs and increase risk of poor health at older ages (Crimmins & Finch, 2006; Elo & Preston, 1992). The synergy between nutrition and infection (Scrimshaw, Taylor, & Gordon, 1968) adds to the complexity of understanding their long-term impact on older adult health.
Adverse nutritional environments in early life can result in long-lasting changes in epigenetic processes that are critical to early development and growth. These circumstances lead to mismatches in nutritional environments later on throughout the life course affecting the health of older adults. Mismatches occur between predictive physiological and metabolic adaptations to an undernourished environment in early life and more favorable nutrition-enriched environments at older ages, leading to chronic diseases and obesity (Bateson & Gluckman, 2011; Gluckman & Hanson, 2005). Increased urbanization and exposure to foods high in saturated fats affecting many developing economies could thus compound the effects of early life exposures to poor nutrition (Lloyd-Sherlock, Beard, Minicuci, Ebrahim, & Chatterji, 2014; Popkin, 2006; Schmidhuber & Shetty, 2005).
An added and yet-to-be fully examined complexity to understanding the impact of poor early life conditions on older adult health is displacement due to armed conflict and violence in the developing world. Displacement is of recognized international importance, and most displaced individuals experience adverse economic conditions including poor nutrition (Internal Displacement Monitoring Center & Norwegian Refugee Council, 2015; United Nations High Commissioner for Refugees, 2017). Displacement is a stressful life event and stress related to chronic exposure to violence poses significant risks on cardiovascular health and other health conditions that affect health throughout the life course (Wilson, Kliewer, & Sica, 2004). Displacement, experienced in particular in early life or childhood, may thus be a relevant risk factor for poor health later in life and could compound already existing risk factors due to the rapid demographic, epidemiological, and nutritional transitions of developing economies.
The Study
In this study, we examine the degree to which early life displacement from armed conflict and violence along with nutrition risk factors are associated with chronic conditions such as hypertension (HTN), diabetes, and obesity among older adults living in Bogotá, the capital city of Colombia. The middle-income country of Colombia is a relevant case study to examine older adult health because it is experiencing large increases in the older adult population and chronic conditions (Gomez, Curcio, & Duque, 2009) in the context of rapid demographic, epidemiological, and nutritional transitions of the 20th century. Colombia experienced rapid mortality decline starting at end of the 1930s through the 1980s as a result of reduced infant mortality due to public health interventions and increased access to medical technology; improvements in standard of living were not as rapid, and large migrations to urban areas since the 1950s to 1960s transformed Colombia from a predominantly rural to an urban country (Flórez, Guataquí, Mendez, & Cote, 2016). Caloric intake dramatically increased during the 20th century in Colombia (FAO, 1946, 2017), resulting in very different nutritional environments for those born in the 20th century and surviving into older ages. Urban areas, for the most part, benefited from modernization, urbanization, and education but also exposed individuals to more nontraditional foods higher in saturated fat content (Popkin, 2006). Despite the rich resources available in the country, poor socioeconomic conditions still affect many children around the country. These conditions increase the risk of stunting and development of cardiovascular and metabolic disease at older ages.
However, what is particularly unique about Colombia is the social and political situation resulting from armed conflict and violence in Colombia beginning in the last decades of the 20th century, which had profound effects on population aging. Colombia has had one of the largest displacements of population in the entire Latin American region (Internal Displacement Monitoring Center & Norwegian Refugee Council, 2015; United Nations High Commissioner for Refugees, 2017). The very large displacement of Colombia’s population due to armed conflict and violence throughout the past 50 to 60 years adds to the complexity of understanding the health of its older adults. Even for individuals exposed to violence but not displaced, Colombia’s widespread violence due to armed conflict is a relevant factor in explaining the health of its older adult population.
These historical circumstances produced cohorts of older adults (60 years and older) who were born mostly in less populated areas with low levels of caloric intake (FAO, 1946; United Nations Statistical Office & the Department of Economic and Social Affairs, 1958), and who experienced increased survivorship of poor early life conditions. They are now living in more urban areas with higher caloric intake and increased exposure to nontraditional food. Many experienced the consequences of the armed conflict and violence to a degree and some were displaced from their homes in early life (Gomez et al., 2009; Internal Displacement Monitoring Center & Norwegian Refugee Council, 2015; United Nations High Commissioner for Refugees, 2017). Some have survived to older ages and are living in large urban areas (Cano-Gutierrez, 2016).
We examine our results from Colombia in a cross-national context by comparing poor early nutritional status among older adults living in urban areas from two other middle-income countries (Mexico and South Africa), benchmarking with older adults born in developed economies (United States and England). Colombia, Mexico, and South Africa are comparable in that they are all upper middle-income countries with similar rapid demographic and epidemiological transitions during the 20th century (Beinart & Dubow, 1995; Riley, 2005; Romo & Pérez, 1998)—transitions that occurred primarily in the context of stagnant improvement in standard of living thus potentially affecting the health of older adults born during these transitions. The focus on urban settings in middle-income countries is relevant because the increase in obesity and chronic conditions is predominantly concentrated in urban areas (Carrillo et al., 2016; Ford, Patel, & Narayan, 2017; Unwin & Alberti, 2006). The majority of the population is also now living in urban areas: Colombia 79% (Flórez et al., 2016), Mexico 79%, and South Africa 64% (World Bank Group, 2016). We benchmark our results with the United States and England—high-income countries with very different historical circumstances in terms of demographic, epidemiological, and nutritional transitions during the 20th century.
Data and Method
Data
Data on older Colombian adults come from the Survey of Health, Wellbeing and Aging [SABE]-Bogotá, which is a representative cross-sectional sample of 2,000 older adults 60 years and older living in Bogotá in 2012. Data from Mexico and South Africa come from the WHO Study on Study on Global Ageing and Adult Health (SAGE, 2007–2008), data from England come from the English Longitudinal Study of Ageing (ELSA; 2007), and data from the United States from the Health and Retirement Study (HRS, 2000, 2006–2008). These data are part of a harmonized, cross-national data set from major surveys of older adults (McEniry, 2015).
Measures
Older adult health.
We use measured HTN to indicate risk of heart disease. Hypertension (HTN) is defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHG, or taking medication for HTN (Yan et al., 2012). We use self-reported diabetes to indicate adult diabetes. In addition, for the United States and England, we defined risk of diabetes as taking diabetes medication or a glycated hemoglobin (HbA1c>6.5%; Yan et al., 2012) and use both variables to estimate models. Although our cross-national analyses compare self-reported diabetes, diabetes defined with biomarkers provides us with an additional reference point.
Early life conditions.
SABE asked questions regarding displacement due to violence from armed conflict in terms of if the respondent had ever been displaced and if so at what age. We define childhood displacement occurring at or before the age of 15 as reported by the respondent.
We define poor early life or childhood nutrition using height, reported hunger in childhood, and birthplace. Height reflects not only environmental conditions in early life (nutrition and infection) but also genetics. However, the interaction between genetics and environment is important. Because much of the older adult population of today’s middle-income countries were exposed to poor nutrition and infectious diseases in early life, this type of adverse environment played an important role in determining height in these populations. In contrast, older adults born during the 20th century in high-income countries experienced better environmental conditions, which influenced height. In our study, we thus use height to make comparisons between older adult populations characterized by their exposure in early life to poor nutrition and infectious diseases (middle-income countries) and older adult populations who for the most part experienced improvement in standard of living and improved nutrition (high-income countries). We use the first quartile of adult height (Q1) to indicate poor nutritional status in childhood; we also examine continuous height in relation to HTN and diabetes.
SABE asked specific questions regarding location of birthplace and questions regarding experiencing hunger during childhood. We use birthplace to identify those born/not born in Bogotá to reflect the general risk of exposure to poor nutrition and inadequate access to quality medical care. Most of the Colombian population born before the 1950s lived in less urban areas characterized by scarcity in resources (food), with mothers with no formal education, and with limited access to good medical care with scarce economic resources (Flórez et al., 2016; Gomez et al., 2009). Self-reported hunger in childhood has proven to be a valid reflection of poor early life conditions in several studies (McEniry, 2013).
Demographic and adult lifestyle risk factors.
Our models control for age, gender, years of education, smoking, and obesity. Obesity and smoking reflect adult lifestyle risk factors, but obesity can also originate in early life. We use measured height and weight to calculate body mass index (BMI) where a BMI ≥30 defines obese individuals. Smoking is defined according to current smoker versus everyone else.
Sample
We select adults 60 years and older but exclude respondents who were not born in the country and who did not have a valid blood pressure measurement. For SAGE countries, we include only urban respondents. The final samples are SABE-Bogotá (n = 1,890), SAGE-Mexico urban dwellers (n = 1,145), SAGE-South Africa urban dwellers (n = 1,146), United States (HRS, n = 6,153), and England (ELSA, n = 4,635). Missing data were imputed using previously validated imputation methods (Raghunathan, Reiter, & Rubin, 2003); we did not use imputed dependent variables (HTN, diabetes) in models. The extent of missing values that were greater than 1%: Colombia-SABE (height 17%, obesity 18%), Mexico (height 8%, obesity 8%), South Africa (height and obesity 3%, education 4%, smoking 3%), England (height 8%, obesity 9%, education 10%, diabetes with biomarker 26%), and United States (diabetes with biomarkers 23%). Biomarkers in the United States and England were obtained on a subsample of respondents, which results in a higher percentage missing.
Analyses
To examine the importance of early life conditions on older adult health, we build a series of nested logistic regression models using SABE-Bogotá estimating the effects of early life conditions (displacement, Q1 of height, hunger, and not born in a capital city) on adult HTN and diabetes controlling first for age and gender, then adding obesity, education, and smoking. If early life conditions are directly associated with older adult health, we should see little attenuation of effects of early life when adding adult lifestyle factors (obesity, smoking) and education. We are particularly interested in attenuation when we add adult obesity as obesity can originate in early life and is an important risk factor for chronic conditions. We estimate models with interaction effects between early life conditions and obesity, and between early life nutrition and displacement, where relevant, to ascertain the importance of early life conditions in relation to obesity and to ascertain the importance of early life displacement and early life nutrition.
We select best models using the Bayesian information criterion (BIC) and produce predicted probabilities for health outcomes. The predicted probabilities, based on the existence of poor early life conditions and obesity, show the magnitude of effects from estimated models. For cross-national comparisons, we estimate nested country-specific models predicting HTN and diabetes as a function of poor early life nutritional status (Q1 of height and continuous height), estimating models with age, gender, obesity, education, and smoking. To better understand cross-national results, we examine associations by estimating models by gender where relevant and then calculate predicted probabilities in instances where height is significantly associated with HTN or diabetes. We control for race in South Africa.
Results
Sample Characteristics
Cross-national comparisons of the selected countries show similarities in terms of age and gender with a majority of respondents being female and the average age close to 70 (Table 1). Average number of years of education is lowest in urban Mexico, followed by Colombia and South Africa. Older adults are shorter in the middle-income countries. Nearly a third (32%) of the SABE-Bogotá respondents reported experiencing hunger during childhood, whereas about 4% indicated displacement during childhood due to armed conflict and violence. A high percentage of respondents in Colombia were not born in a capital city (72%). In most countries, except England, a higher percentage of respondents never smoked. The highest proportion of respondents still smoking appeared in Mexico and South Africa (21% and 22%). South Africa shows a 49% prevalence of obesity and 85% prevalence of HTN. Mexico and the United States show the highest prevalence of diabetes (21% and 22%). England had the lowest prevalence of HTN (54%) but ELSA’s method for measuring blood pressure was different from the other surveys in that it excluded individuals who smoked and exercised before taking a blood pressure measurement.
Table 1.
Sample of Adults Aged 60+ Years in Middle-Income and High-Income Countries.
| COL SABE |
MX SAGE |
SA SAGE |
ENG ELSA |
US HRS |
|
|---|---|---|---|---|---|
| Demographics | |||||
| Female (%) | 56 | 51 | 62 | 56 | 59 |
| Age (SD) | 70 (7.7) | 71 (7.8) | 69 (7) | 72 (8.7) | 69 (6.6) |
| Education (SD) | 6.0 (4.7) | 4.9 (4.4) | 6.7 (4.9) | 13.4 (2.4) | 12.6 (2.8) |
| Early life | |||||
| Height (cm) | |||||
| Males (SD) | 163 (7.0) | 164 (7.1) | 164 (13) | 172 (6.8) | 178 (7.0) |
| Females (SD) | 150 (6.4) | 149 (6.5) | 155 (12) | 158 (6.7) | 163 (6.5) |
| Not born capital (%) | 72 | ||||
| Hunger as child (%) | 32 | ||||
| Displacement (%) | 4 | ||||
| Adult life | |||||
| Obesity (%) | 27 | 29 | 49 | 29 | 22 |
| Smoking (%) | |||||
| Never smoked | 52 | 57 | 67 | 36 | 66 |
| Previous smoker | 39 | 22 | 12 | 53 | 23 |
| Current smoker | 8 | 21 | 22 | 11 | 11 |
| Diabetes (%) | 19 | 21 | 14 | 10 | 12 |
| HTN (%) | 76 | 73 | 85 | 54 | 73 |
Source. SABE-Bogotá (n = 1,890); SAGE-Mexico (n = 1,145) urban dwellers; SAGE-South Africa (n = 1,146) urban dwellers; ELSA-England (n = 4,635); HRS-United States (n = 6,153).
Note. Weighted, aged 60+ years; rounding error results in totals not summing to 100.Variables in table with (SD) show averages with standard deviations (SD) in parentheses. Missing values were imputed except for HTN and continuous height. The measurement of HTN in ELSA omits individuals who had smoked, eaten, or exercised 30 min before the interview. SABE = Survey of Health, Wellbeing and Aging; SAGE = Study on Global Ageing and Adult Health; ELSA = English Longitudinal Study of Ageing; HRS = Health and Retirement Study; HTN = hypertension.
Logistic Results From Colombia
Early life conditions increase the likelihood of HTN in Bogotá (Table 2, Model 1) but the effects of low height and displacement due to violence are slightly attenuated and their significance disappears when obesity is added (Table 2, Model 2). When adding education and smoking (Model 3) results remain the same although the best model according to the BIC criterion is Model 2. Models including interactions between early life and obesity based on Model 2 produced no significant interactions; these models do not appear in the table. Using the best model according to the BIC criterion (Model 2), for those respondents not born in Bogotá, the odds of HTN are about 37% higher in comparison with those born in Bogotá. Those who experienced hunger during childhood were more likely to have HTN. Obese respondents have about 2.5 times the odds of having HTN than those who are not obese. Predicted probabilities indicate the importance of obesity. In spite of a better early life, being obese increases the probability of HTN to 85%. This is similar to those who experienced poor early life conditions but who are not obese (Figure 1) and represents an increase of about 23% higher than the predicted probability for those without poor early life conditions and not obese. Those with the highest risk of HTN are those who experienced poor early life conditions and are obese as adults. There is about a 39% increase in the probability of HTN between those with no risk factors and those with poor early life conditions who are also obese.
Table 2.
Childhood Effects on Adult HTN and Diabetes.
| Model 1 |
Model 2 |
Model 3 |
||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| HTN | ||||||
| Early life | ||||||
| Not born capital city | 1.38** | [1.08, 1.75] | 1.37** | [1.08, 1.75] | 1.35* | [1.05, 1.72] |
| Hunger childhood | 1.30* | [1.02, 1.67] | 1.33* | [1.04, 1.71] | 1.30* | [1.00, 1.68] |
| Low height | 1.36* | [1.01, 1.84] | 1.30 | [0.96, 1.76] | 1.28 | [0.94, 1.73] |
| Displacement | 2.05* | [1.03, 4.06] | 1.94 | [0.97, 3.90] | 1.92 | [0.96, 3.86] |
| Adult life | ||||||
| Obesity | 2.53*** | [1.83, 3.51] | 2.54*** | [1.83, 3.52] | ||
| LL | [−953, −951] | [−934, −929] | [−932, −926] | |||
| BIC | [1,978, 1,982] | [1,940, 1,952] | [1,958, 1,970] | |||
| Diabetes | ||||||
| Early life | ||||||
| Not born capital city | 1.41* | [1.06, 1.87] | 1.40* | [1.06, 1.86] | 1.35* | [1.01, 1.80] |
| Hunger childhood | 1.19 | [0.93, 1.53] | 1.20 | [0.93, 1.54] | 1.17 | [0.91, 1.51] |
| Low height | 0.82 | [0.62, 1.09] | 0.80 | [0.60, 1.06] | 0.78 | [0.59, 1.04] |
| Displacement | 1.84* | [1.10, 3.06] | 1.76* | [1.06, 2.95] | 1.83* | [1.10, 3.07] |
| Adult life | ||||||
| Obesity | 1.48** | [1.13, 1.93] | 1.47** | [1.13, 1.92] | ||
| LL | [−881, −880] | [−877, −876] | [−873, −868] | |||
| BIC | [1,835, 1,838] | [1,834, 1,837] | [1,841, 1,852] | |||
Source. SABE-Bogotá, those with measured HTN and born in Colombia (n = 1,890).
Note. Shown are odds ratios with 95% confidence intervals and significance levels based on imputation models combining five imputed data sets. LL and BIC in table show a range based on each individually imputed data set; lower values for BIC are preferred; all models were different from the null model (p < .001) except diabetes Model 1 (p < .01). HTN and diabetes as dependent variables are not imputed. Model 1 controls for age and gender; Model 2 adds obesity; Model 3 adds education and smoking. Figures 1 and 2 show predicted probabilities for early life conditions using Model 2 for HTN and diabetes. HTN = hypertension; OR = odds ratio; CI = confidence interval; LL = log likelihood; BIC = Bayesian information criterion; SABE = Survey of Health, Wellbeing and Aging.
p < .05.
p < .01.
p < .001.
Figure 1. Predicted probabilities of HTN (SABE-Bogotá).
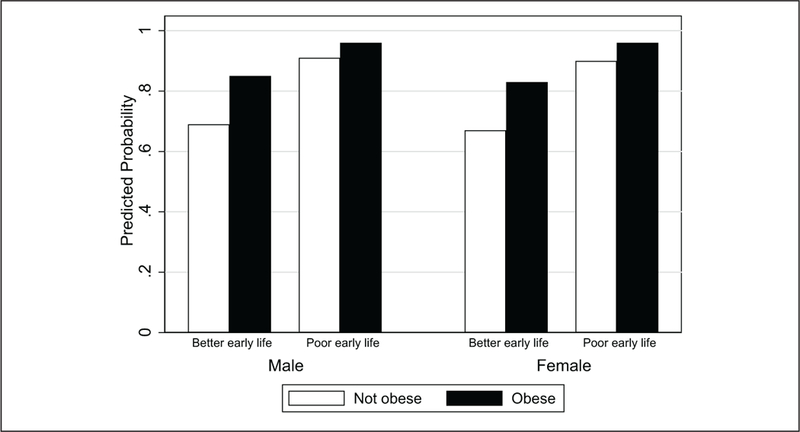
Source. Predicted probabilities derived from Table 2 Model 2 using the average response on variables and varying poor early life conditions and obesity by gender.
Note. Numbers are (from left to right bars above by gender): (A) No poor early life conditions, not obese: 0.69, 0.67 (males, females). (B) No poor early life conditions, obese: 0.85, 0.83 (males, females). (C) Poor early life conditions, not obese: 0.91, 0.90 (males, females). (D) Poor early life conditions, obese: 0.96, 0.96 (males, females). HTN = hypertension; SABE = Survey of Health, Wellbeing and Aging.
For diabetes (Table 2, Model 2), those not born in Bogotá and those who experienced displacement during childhood show increased odds of being diabetic. There is no attenuation of early life variables when we add obesity; being obese increases the odds of diabetes by about 48% compared with those who are not obese. Interactions between early life and obesity, and between early life and displacement were not significant and these models do not appear in the table. Predicted probabilities of diabetes (Figure 2) are highest among those who experienced poor early life conditions and who are obese, much higher than those who experienced better early conditions but who are nevertheless obese as adults. Those who had a better early life and were not obese showed the lowest probability of diabetes. In contrast with HTN, predicted probabilities for diabetes indicate the importance of poor early life conditions in addition to obesity. There is about a 46% increase in the predicted probability of diabetes between those with no risks and those obese but there is about a 42% increase in the predicted probability of diabetes between those with no early life risks but obese and those with early life risks and not obese. The difference between those with no early life risks and not obese and those with risk factors is very large—almost a 200% increase in the predicted probability of diabetes.
Figure 2. Predicted probabilities of diabetes (SABE-Bogotá).
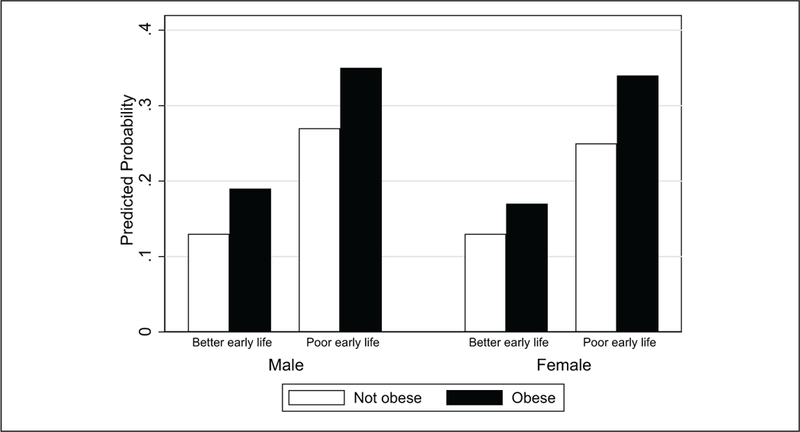
Source. Predicted probabilities derived from Table 2, Model 2 using the average response on variables and varying poor early life conditions and obesity by gender.
Note. Numbers are (from left to right bars above by gender): (A) No poor early life conditions, not obese: 0.13, 0.13 (males, females). (B) No poor early life conditions, obese: 0.19, 0.17 (males, females). (C) Poor early life conditions, not obese: 0.27, 0.25 (males, females). (D) Poor early life conditions, obese: 0.35, 0.34 (males, females). SABE = Survey of Health, Wellbeing and Aging.
Cross-National Results
Apart from Colombia, there were no significant positive effects of low height on HTN or diabetes (Appendix Table A1); adding obesity attenuates the effects of low height on HTN in Colombia. However, models estimated by gender for HTN show that being short is strongly associated with HTN in the case of Colombian males and that the effects of low height remain significant when adding obesity, education, smoking (results not shown but available upon request). When we estimate HTN models using continuous height for males controlling only for age we find significant results for height in Colombian and English males (Table 3). Predicted probabilities show a much higher predicted probability of being hypertensive for shorter Colombian males than for English males (Figure 3). Indeed, comparing predicted probabilities according to average male height, we find that the predicted probability of HTN is about 0.75 for Colombian males and about 0.49 for English males—a 53% increase in the predicted probability for HTN.
Table 3.
Effects of Continuous Height on Hypertension for Males (Aged 60+ years).
| Odds ratio | 95% CI | p value | |
|---|---|---|---|
| Bogotá | 0.96 | [0.93, 0.98] | .002 |
| Mexico urban | 1.01 | [0.98, 1.04] | .618 |
| South African urban | 1.01 | [1.00, 1.03] | .132 |
| England | 0.99 | [0.97, 1.00] | .036 |
| United States | 1.00 | [0.98, 1.01] | .515 |
Source. SABE-Bogotá, SAGE-Mexico and South Africa, ELSA-England, and HRS-United States.
Note. Models control for age. CI = confidence interval; SABE = Survey of Health, Wellbeing and Aging; SAGE = Study on Global Ageing and Adult Health; ELSA = English Longitudinal Study of Ageing; HRS = Health and Retirement Study.
Figure 3. Predicted probabilities of hypertension for males by continuous height.
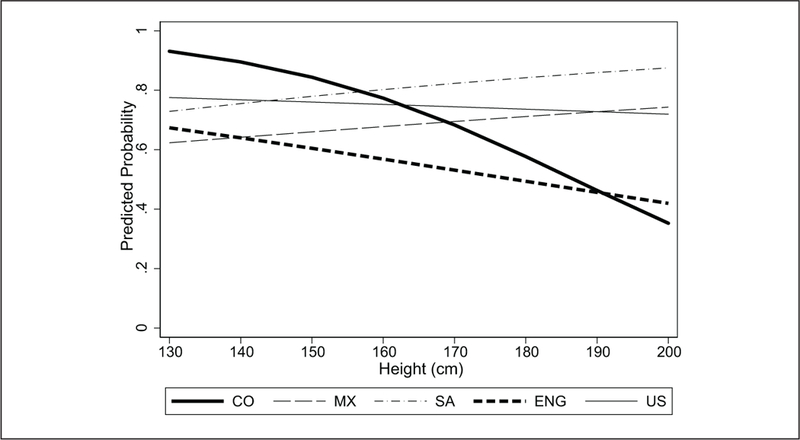
Note. (A) Based on logistic models controlling for age. (B) Bolded lines in graph indicate countries where continuous height is significant in predicting hypertension: Colombia and England. (C) The average height for males in CO (Colombia), MX (Mexico), and SA (South Africa) is 163 to 164 cm; ENG (England) and US (United States) 172 to 178 cm. The predicted probability for HTN using the average height for Colombian males is about .75, whereas for English males the predicted probability is about .49. HTN = hypertension.
Being short in Mexico had a protective effect on the likelihood of diabetes in Mexico and England (Appendix Table A1). Obesity was strongly associated with HTN across all countries (Models 2 and 3) and with diabetes in Colombia, England, and the United States. Models using biomarkers to define diabetes produced similar results for the United States but produced no significant protective effects on diabetes for England (results not shown).
Discussion
We examined early life conditions and obesity and their association with adult HTN and diabetes in three middle-income countries with similar rapid demographic, epidemiological, and nutritional transitions in the early to mid-20th century and two high-income countries. We found that, in Colombia, older adults displaced as children and not born in the capital and who are now obese are most at risk of being diabetic. While displacement and being short are associated with HTN, their effects disappear when adding obesity, whereas experiencing hunger in childhood and being born in less urban areas remains significantly associated with HTN. There were no significant interaction effects between obesity and early conditions in HTN and diabetes models. Cross-national comparisons with older adults living in urban areas in Mexico and South Africa and living anywhere in the United States show no significant associations between low height and chronic conditions. Being short predicts higher risk of HTN for males in Colombia and England although the steeper pattern for height appearing in Colombia suggests higher inequality associated with being short.
Our study contributes to the literature that demonstrates the importance of poor early life conditions and older adult health in the developing world, using large comprehensive surveys of older adults (McEniry, 2013). In addressing the long-term consequences of childhood displacement due to armed conflict and violence on older adult health, our study highlights a topic not yet fully examined. We know of no other studies that show the importance of early life displacement in relation to older adult HTN and diabetes. Recent studies indicate an association between short height and older adult HTN in both developing and developed world economies (Asao, Kao, & Baptiste-Roberts, 2006; Korhonen, Kautiainen, & Eriksson, 2017; Song et al., 2016). However, we also know of no recent studies that show a positive association between being short and older adult HTN in the Latin American region. While the underlying mechanisms by which a person’s height affects his blood pressure are not completely understood, one plausible theory is that early life exposures affect well-being, determine height, and cardiovascular health (Korhonen et al., 2017; Song et al., 2016). Given the history of Colombia in terms of exposure of its population to violence from armed conflict, this is a particularly relevant finding.
The results from Colombia point to a couple of conclusions. First, early life conditions are particularly relevant for older adult health in middle-income countries such as Colombia, whether they be physiological (hunger, height) or external (displacement due to violence, birthplace). Not surprisingly, obesity is a strong predictor of HTN and diabetes, but our study further suggests that the least desirable circumstance in regard to these diseases is to have also experienced poor early life conditions. We cannot identify precise mechanisms to explain the effects of poor early life conditions on older adult health. However, our results showing that poor early life conditions plus adult obesity produce a higher risk of poor health among Colombian older adults corroborate the possibility of a mismatch between predictive physiological and metabolic adaptations to an undernourished environment in early life and more favorable nutrition-enriched environments at older ages (Bateson & Gluckman, 2011; Gluckman & Hanson, 2005; Taylor, 2010). Urban/rural birthplace in early life and displacement due to violence combined with adult obesity provide an explanation for differences in risk of diabetes among Colombians living in the large urban setting of Bogotá. Being born in less urban areas for older adults reflects not only less access to quality health care and adequate nutrition for those with fewer resources, but also the potential for exposure to violence given the history of armed conflict over the last several decades, which occurred primarily in the more rural regions of Colombia (Gomez et al., 2009). Displacement due to violence from armed conflict during early life may worsen the family’s ability to provide adequate nutrition and health care particularly for its youngest members, thus setting the stage for an accumulation of difficulties throughout their life course leading to poor health at older ages (Internal Displacement Monitoring Center & Norwegian Refugee Council, 2015; United Nations High Commissioner for Refugees, 2017).
Self-reported chronic health conditions such as diabetes may be problematic although in some settings underestimation of chronic conditions such as diabetes produces reliable estimates of disease (Banks, Marmot, Oldfield, & Smith, 2006; Goldman, Lin, Weinstein, & Lin, 2003). In our study, we found that diabetes defined using self-reported or biomarkers produced similar results for the United States; in contrast, in England we found differences in results—suggesting that even in developed economies with better access to quality medical care, we need to use caution when using self-reported diabetes. In developing countries, underestimation may be more problematic in low-income countries or rural areas with less access to quality health care. Recent evidence from Colombia shows that self-reported diabetes and biomarker assessments of diabetes produce very similar estimates of the prevalence of diabetes, especially in its capital city (Vargas-Uricoechea & Casas-Figueroa, 2015).
When placed within the context of cross-national comparisons, older Colombian adults show similar health trends with other middle-income countries in terms of high prevalence of HTN, diabetes, and obesity. The prevalence of diabetes is probably higher in Mexico and South Africa because diabetes is self-reported. South Africa presents an extreme among the three selected middle-income countries and there may be multiple reasons, including social and historical circumstances, to explain differences (Beinart & Dubow, 1995). That the prevalence of HTN and obesity are also generally higher in the middle-income countries, particularly in South Africa, gives credence to the conjecture that the profile of older adult health will be worse in the developing world as compared with high-income countries due to early life conditions and rapid demographic and epidemiological changes (McEniry, 2014; Palloni & Souza, 2013).
That shorter Colombian males (but not females) are more likely to be hypertensive is puzzling. While there is mixed evidence in terms of height and adult health in terms of gender differences, most of the evidence has appeared in females (Eriksson et al., 2010; Janghorbani et al., 2012; Song et al., 2016). Inequality is a relevant explanation for the large difference in predicted probability between Colombia and English males because Colombia has higher inequality than England (World Bank Group, 2017a). Uneven development may explain the lack of association or protective effects between height and health. The protective effects of height on diabetes that we observe in Mexico could reflect uneven development where more disadvantaged groups with higher mortality rates have yet have to experience nutritional changes and, therefore, are less prone to chronic conditions such as diabetes.
A second conclusion from the Colombian results is in regard to the complexity of health profiles in older adults in countries born during the rapid demographic, epidemiological, and nutritional transitions of the 20th century. A mixed health profile appears, part of which highlights the importance of early life conditions and obesity among some older adults—not surprising as others have already pointed this out (Palloni & Souza, 2013). However, the health profile also highlights the potential for worsening health for those who had a better start in life but who are obese perhaps because of their adult lifestyle—a profile more in line with what the developed world has been experiencing (Banks et al., 2006; Crimmins, Preston, & Cohen, 2010). The unknown impact of the double burden of infectious and chronic disease on the health of these older adults only adds to the complexity of this mixed health profile (Samper-Ternent et al., 2012).
The study has limitations. First, survey data of older adults, while containing very comprehensive data, do not always have the level of detail needed. Information on childhood conditions is based mostly on self-reports from older adults and the possibility of recall bias clearly exists. High blood pressure may be due to other factors not adequately captured in surveys (e.g., urban environment, diet, salt consumption). (Exercise could also influence high blood pressure and we estimated models with exercise but the results remained the same.) The data we use are cross-sectional data. Panel data at different stages of the life course would help clarify older adult health, especially in terms of having obesity at different points in childhood or early/middle adulthood—periods that can be very relevant to the development of chronic conditions. Having longitudinal data would also reduce concerns regarding endogenous selection biases, which could possibly distort the association between early life and adult disease due to controlling for obesity if obesity were a common effect of both early life and adult disease.
Second, comparisons between middle-income and high-income countries are never perfect due to country and survey differences. Although Colombia, Mexico, and South Africa are comparable in that they are all upper middle-income countries with similar demographic transitions, there are country differences in life expectancy, health care systems, and inequality, with Colombia doing better and South Africa just the opposite (Hosegood & Timaeus, 2006; World Bank Group, 2017b; WHO, 2000, 2015). The puzzling results such as the lack of association between obesity and diabetes in Mexico and South Africa point to the complexity of interpreting cross-national comparisons of health.
Third, height; height tends to diminish with age, and shorter height in some instances may not reflect poor early life conditions. Thus, studies showing the inverse associations between height and HTN and diabetes (Asao et al., 2006; Korhonen et al., 2017; Song et al., 2016) are difficult to replicate for older adults. Height may be a better indicator for HTN and leg length may be a more sensitive measure for diabetes than height. However, more sensitive measures of poor early life environments using the components of height such as leg length were not available in our study. Furthermore, there are no agreed-upon cutoff points for adult height that reflect equivalent levels of poor early life conditions and stunting across countries. Country differences in the levels of exposure to environmental and genetic aspects affecting height make cross-national comparisons with height more difficult to interpret. This may partially explain why short height almost consistently is protective of adult diabetes; the shortest (and also the poorest) in Colombia, Mexico, and South Africa may not yet be affected by the nutritional transitions to a diet higher in saturated fats as are the more economically better off and taller older adults.
Fourth, our study examines displacement due to violence in early life but the group of older adults in our study has been exposed to other types of violence (Cano-Gutierrez, 2016). The accumulation of exposure to different types of violence may be an important factor to consider. Fifth, all surveys analyzed and compared were not conducted in the same year. Guidelines for diagnosis of chronic conditions such as HTN change often, new medications are introduced, and many social changes occur in short periods of time.
Conclusion
The present study emphasizes the importance of the long-term consequences of early life displacement due to armed conflict and violence along with poor early life nutrition on adult chronic conditions in populations that have experienced rapid demographic, epidemiological, and nutritional transitions throughout their lifetimes. Differences in historical circumstances are relevant to understanding the health of older adults in middle-income countries. Results from Colombia reinforce the idea that the determinants of older adult health in these settings will be very different from that of high-income countries.
Acknowledgments
We are particularly grateful to Robert M. Hauser, Alberto Palloni, and Emily Agree without whom this project would not have been possible. Many thanks to Sarah Moen for editing the final version of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fulbright Commission in Colombia, the Colombian Department of Science, Technology, and Innovation (Colciencias), and the Aging Institute at the Pontificia Universidad Javeriana, Bogotá, within the framework of the Fulbright U.S. Scholar program, Cohort 2016–2017. University of Wisconsin–Madison researchers are supported by core National Institute of Health grants to the Center for Demography and Ecology, University of Wisconsin (P2C HD047873) and the Center for Demography of Health and Aging, University of Wisconsin (P30 AG017266). Dr. Samper-Ternent was supported by the Sealy Center on Aging at the University of Texas Medical Branch in Galveston, Claude D. Pepper OAIC (P30-AG024832) and The Mexican Health and Aging Study (R01AG018016) from grants of the National Institutes of Health/National Institute on Aging.
Appendix
Table A1.
Cross-National Comparison of Effects of Low Height and Obesity on Adult HTN and Diabetes.
| HTN |
Diabetes |
|||||
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Bogotá | ||||||
| Low height | 1.38 [1.02–1.86] | 1.33 [0.98–1.79] | 1.29 [0.96–1.75] | 0.79 [0.59–1.06] | 0.76 [0.57–1.03] | 0.74 [0.55–0.99] |
| Obese | 2.53 [1.83–3.50] | 2.53 [1.83–3.49] | 1.65 [1.23–2.22] | 1.65 [1.23–2.21] | ||
| Mexico | ||||||
| Low height | 0.89 [0.65–1.21] | 0.86 [0.63–1.17] | 0.81 [0.59–1.1 1] | 0.64 [0.45–0.89] | 0.63 [0.45–0.89] | 0.61 [0.43–0.86] |
| Obese | 1.61 [1.19–2.18] | 1.59 [1.18–2.16] | 1.06 [0.78–1.43] | 1.06 [0.79–1.44] | ||
| S. Africa | ||||||
| Low height | 0.79 [0.56–1.11] | 0.74 [0.52–1.05] | 0.74 [0.52–1.05] | 0.83 [0.57–1.22] | 0.79 [0.54–1.17] | 0.81 [0.55–1.20] |
| Obese | 1.36 [0.96–1.91] | 1.47 [1.00–1.99] | 1.39 [0.98–1.97] | 1.24 [0.87–1.78] | ||
| England | ||||||
| Low height | 1.11 [0.97–1.28] | 1.07 [0.93–1.23] | 1.04 [0.91–1.20] | 0.81 [0.65–1.02] | 0.76 [0.61–0.96] | 0.75 [0.60–0.94] |
| Obese | 1.76 [1.51–2.04] | 1.76 [1.52–2.05] | 2.47 [2.02–3.02] | 2.46 [2.01–3.01] | ||
| US | ||||||
| Low height | 1.14 [0.97–1.34] | 1.12 [0.95–1.32] | 1.08 [0.91–1.27] | 0.98 [0.79–1.20] | 0.96 [0.77–1.18] | 0.90 [0.73–1.11] |
| Obese | 2.16 [1.85–2.53] | 2.06 [1.76–2.41] | 2.56 [2.18–3.00] | 2.38 [2.02–2.79] | ||
Source. SABE-Bogotá; SAGE-Mexico, SAG E-South Africa; ELSA-England; and HRS-US.
Note. Shown are odds ratios with 95% confidence intervals based on imputation models using five imputed data sets. HTN and diabetes as dependent variables are not imputed. Model I controls for age and gender; Model 2 controls adds obesity; Model 3 also controls for education and smoking. Best models, according to BIC, are noted in italics; lower values for BIC are preferred. Models for the United States and England and Colombia (HTN) were different from the null model (p < .001); models for Colombia, Mexico, and South Africa were different at p < .05 with the exception of South Africa HTN and Colombia diabetes. HTN = hypertension.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Albala C, Vio F, & Yáñez M (1997). Epidemiological transition in Latin America: A comparison of four countries. Revista médica de Chile, 125, 719–727. [PubMed] [Google Scholar]
- Asao K, Kao WHL, & Baptiste-Roberts K (2006). Short stature and the risk of adiposity, insulin resistance, and type 2 diabetes in middle age. Diabetes Care, 29, 1632–1637. [DOI] [PubMed] [Google Scholar]
- Banks J, Marmot M, Oldfield Z, & Smith JP (2006). Disease and disadvantage in the United States and in England. Journal of the American Medical Association, 295, 2037–2045. doi: 10.1001/jama.295.17.2037 [DOI] [PubMed] [Google Scholar]
- Barker DJ (1998). Mothers, babies and health in later life (2nd ed.). Edinburgh, UK: Churchill Livingstone. [Google Scholar]
- Bateson P, & Gluckman P (2011). Plasticity, robustness, development and evolution. Cambridge, UK: Cambridge University Press. [Google Scholar]
- Beinart W, & Dubow S (Eds.). (1995). Segregation and apartheid in twentieth-century South Africa. London, England: Routledge. [Google Scholar]
- Cano-Gutierrez C (2016). Markers of violence in the older adult population in the city of Bogotá [Marcadores de violencia en la población adulta mayor de la ciudad de Bogotá]. Bogota, Colombia: Aging Institute, Pontificia Javeriana University. [Google Scholar]
- Carrillo R, Barnabe-Ortiz A, Pillay TD, Gilman RH, Sanchez JF, Poterico J, . . . Miranda JJ (2016). Obesity risk in rural, urban and rural-to-urban migrants: Prospective results of the PERU MIGRANT study. International Journal of Obesity, 40, 181–185. doi: 10.1038/ijo.2015.140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crimmins EM, & Finch C (2006). Infection, inflammation, height, and longevity. Proceedings of the National Academy of Sciences of the United States of America, 103, 498–503. doi: 10.1073/pnas.0501470103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crimmins EM, Preston SH, & Cohen B (2010). International differences in mortality at older ages: Dimensions and sources. Washington, DC: The National Academies Press. doi: 10.17226/12945 [DOI] [PubMed] [Google Scholar]
- Elo IT, & Preston SH (1992). Effects of early-life conditions on adult mortality: A review. Population Index, 58, 186–212. doi: 10.2307/3644718 [DOI] [PubMed] [Google Scholar]
- Eriksson J, Kajantie E, Osmond C, Thornburg K, & Barker D (2010). Boys live dangerously in the womb. American Journal of Human Biology, 22, 330–335. doi: 10.1002/ajhb.20995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Filozof C, Gonzalez C, Sereday M, Mazza C, & Braguinsky J (2001). Obesity prevalence and trends in Latin-American countries. Obesity Reviews, 2, 99–106. [DOI] [PubMed] [Google Scholar]
- Flórez CE, Guataquí JC, Mendez R, & Cote H (2016). Las Transformaciones Sociodemográfics en Colombia Durante el Siglo XX y Principios del Siglo XXI [Sociodemographic transitions in Colombia during the 20th century and at the beginning of the 21st century] (Working paper). Department of Economics, Universidad del Rosario, Bogotá, Colombia. [Google Scholar]
- Food and Agriculture Organization. (1946). World Food Survey. Washington, DC: United Nations. [Google Scholar]
- Food and Agriculture Organization. (2016). Food balance sheets. Retrieved from http://faostat.fao.org/site/368/default.aspx#ancor
- Ford ND, Patel SA, & Narayan KV (2017). Obesity in low- and middle-income countries: Burden, drivers, and emerging challenges. Annual Review of Public Health, 38, 145–164. doi: 10.1146/annurev-publhealth-031816-044604 [DOI] [PubMed] [Google Scholar]
- Gluckman P, & Hanson M (2005). The fetal matrix: Evolution, development and disease. Cambridge, UK: Cambridge University Press. [Google Scholar]
- Goldman N, Lin IF, Weinstein M, & Lin YH (2003). Evaluating the quality of self-reports of hypertension and diabetes. Journal of Clinical Epidemiology, 56, 148–154. doi: 10.1016/S0895-4356(02)00580-2 [DOI] [PubMed] [Google Scholar]
- Gomez F, Curcio C-L, & Duque G (2009). Health care for older persons in Colombia: A country profile. Journal of the American Geriatrics Society, 57, 1692–1696. doi: 10.1111/j.1532-5415.2009.02341.x [DOI] [PubMed] [Google Scholar]
- He W, Goodkind D, & Kowal P (2016). An aging world: 2015 (International Population Reports, P95/16–1). Washington, DC: U.S. Census Bureau. [Google Scholar]
- Hebert JR, Hurley TG, Olendzki BC, Teas J, Ma Y, & Hampl JS (1998). Nutritional and socioeconomic factors in relation to prostate cancer mortality: A cross-national study. Journal of the National Cancer Institute, 90, 1637–1647. doi: 10.1093/jnci/90.21.1637 [DOI] [PubMed] [Google Scholar]
- Hosegood V, & Timaeus IM (2006). HIV/AIDS and older people in South Africa In Cohen B & Menken J (Eds.), Aging in Sub-Saharan Africa: Recommendation for furthering research (pp. 250–275). Washington, DC: The National Academies Press. [PubMed] [Google Scholar]
- Ibrahim MM, & Damasceno A (2012). Hypertension in developing countries. The Lancet, 380, 611–619. [DOI] [PubMed] [Google Scholar]
- Internal Displacement Monitoring Centre & Norwegian Refugee Council. (2015). Global overview 2015: People internally displaced by conflict and violence. Retrieved from http://www.internal-displacement.org/library/publications/2015/global-overview-2015-people-internally-displaced-by-conflict-and-violence/
- Janghorbani M, Momeni F, & Dehghani M (2012). Hip circumference, height and risk of type 2 diabetes: Systematic review and meta-analysis. Obesity Reviews, 13, 1172–1181. doi: 10.1111/j.1467-789X.2012.01030.x [DOI] [PubMed] [Google Scholar]
- Korhonen PE, Kautiainen H, & Eriksson JG (2017). The shorter the person, the higher the blood pressure: A birth cohort study. Journal of Hypertension, 35, 1170−1177. doi: 10.1097/HJH.0000000000001300 [DOI] [PubMed] [Google Scholar]
- Kuh D, & Ben-Shlomo Y (2004). A life course approach to chronic disease epidemiology. New York, NY: Oxford University Press. doi: 10.1093/acprof:oso/9780198578154.001.0001. [DOI] [Google Scholar]
- Lloyd-Sherlock P, Beard J, Minicuci N, Ebrahim S, & Chatterji S (2014). Hypertension among older adults in low- and middle-income countries: Prevalence, awareness and control. International Journal of Epidemiology, 43, 116–128. doi: 10.1093/ije/dyt215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEniry MC (2013). Early life conditions and older adult health in low and middle income countries: A review. Journal of the Developmental Origins of Health and Disease, 4(1), 10–29. doi: 10.1017/S2040174412000499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEniry MC (2014). Early life conditions and rapid demographic changes in the developing world: Consequences for older adult health. Dordrecht, The Netherlands: Springer Science+Business Media. [Google Scholar]
- McEniry MC (2015). Research on Early Life and Aging: Trends and Effects (RELATE): A cross-national study (ICPSR34241-v1). Ann Arbor, MI: Inter-university Consortium for Political and Social Research. [Google Scholar]
- NCD Risk Factor Collaboration. (2016). Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4–4 million participants. The Lancet, 387, 1513–1530. doi: 10.1016/S0140-6736(16)00618-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palloni A, & Souza L (2013). The fragility of the future and the tug of the past: Longevity in Latin America and the Caribbean. Demographic Research, 29, 543–578. doi: 10.4054/DemRes.2013.29.21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popkin BM (2006). Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases (NCDs). The American Journal of Clinical Nutrition, 84, 289–298. doi: 10.1093/ajcn/84.1.289 [DOI] [PubMed] [Google Scholar]
- Raghunathan T, Reiter JP, & Rubin D (2003). Multiple imputation for disclosure limitation. Journal of Official Statistics, 19, 1–16. [Google Scholar]
- Riley JC (2005). Bibliography of works providing estimates of life expectancy at birth and estimates of the beginning period of health transitions in countries with a population in 2000 of at least 400,000. Retrieved from http://www.lifetable.de/RileyBib.htm
- Romo A. C. R. d., & Pérez M. E. R. d. (1998). Historia de la salud pública en México: Siglos XIX y XX [History of public health in Mexico: 19th and 20th century]. História, Ciências, Saúde-manguinhos, 5, 293–310. doi: 10.1590/S0104-59701998000200002 [DOI] [PubMed] [Google Scholar]
- Samper-Ternent R, Michaels-Obregón A, Wong R, & Palloni A (2012). Older adults under a mix regime of infectious and chronic diseases. Salud Pública de México, 54, 487–495. doi: 10.1590/S0036-36342012000500005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidhuber J, & Shetty P (2005). The nutrition transition to 2030: Why developing countries are likely to bear the major burden. Acta Agriculturae Scandinavica, Section C — Food Economics, 3–4, 150–166. doi: 10.1080/16507540500534812 [DOI] [Google Scholar]
- Scrimshaw NS, Taylor C, & Gordon J (1968). Interactions of nutrition and infection. New York, NY: World Health Organization. [PubMed] [Google Scholar]
- Song L, Shen L, Ji H, Liu B, Zheng X, Liang Y, . . . Wang Y (2016). Height and prevalence of hypertension in a middle-aged and older Chinese population. Scientific Reports, 6, Article 39480. doi: 10.1038/srep39480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor SE (2010). Mechanisms linking early life stress to adult health outcomes. Proceedings of the National Academy of Sciences of the United States of America, 107, 8507–8512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations High Commissioner for Refugees. (2017). Global trends: Forced displacement in 2016. Retrieved from http://www.unhcr.org/figures-at-a-glance.html
- United Nations Statistical Office & the Department of Economic and Social Affairs.(1958). Statistical yearbook (Vol. 10). New York, NY: United Nations. [Google Scholar]
- Unwin N, & Alberti K (2006). Chronic non-communicable diseases. Annals of Tropical Medicine & Parasitology, 100, 455–464. doi: 10.1179/136485906X97453 [DOI] [PubMed] [Google Scholar]
- Vargas-Uricoechea H, & Casas-Figueroa LÁ (2015). An epidemiologic analysis of diabetes in Colombia. Annals of Global Health, 81, 742–753. doi: 10.1016/j.aogh.2015.11.001 [DOI] [PubMed] [Google Scholar]
- Wilson D, Kliewer W, & Sica D (2004). The relationship between exposure to violence and blood pressure mechanisms. Current Hypertension Reports, 6, 321–326. [DOI] [PubMed] [Google Scholar]
- World Bank Group. (2016). Urban population (% of total). Retrieved from http://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS
- World Bank Group. (2017a). GINI Index (World Bank estimate). Retrieved from http://data.worldbank.org/indicator/SI.POV.GINI
- World Bank Group. (2017b). GNI per capita, Atlas method (current US$). Retrieved from http://data.worldbank.org/indicator/NY.GNP.ATLS.CD
- World Health Organization. (2000). The world health report 2000: Health systems: Improving performance (Haden A & Campanini B, Eds.). Geneva, Switzerland: Author. [Google Scholar]
- World Health Organization. (2015). World health statistics 2015. Geneva, Switzerland: Author. [Google Scholar]
- World Health Organization. (2016). Global report on diabetes. Geneva, Switzerland: Author. [Google Scholar]
- Yan S, Li J, Li S, Zhang B, Du S, Gordon-Larsen P, . . . Popkin BM (2012). The expanding burden of cardiometabolic risk in China: The China Health and Nutrition Survey. Obesity Reviews, 13, 810–821. doi: 10.1111/j.1467-789X.2012.01016.x [DOI] [PMC free article] [PubMed] [Google Scholar]