

Abstract
Background:
Cranial surgical site infections due to Salmonella species are rarely reported. Only eight cases of Salmonella enteritidis infection following intracranial surgery for brain tumor have been reported to date. We describe a unique case of both subgaleal and brain abscesses caused by S. enteritidis following craniotomy for a parafalcine giant cell glioblastoma multiforme. A literature review of the previously published cases is also provided.
Case Description:
A 36-year-old previously healthy man presented with a posterior parietal parafalcine giant cell glioblastoma multiforme. 5 weeks after craniotomy for tumor resection, the patient presented with worsening headache and painful swelling at the cranial operative site. Head computed tomography and magnetic resonance imaging scans revealed both scalp and brain abscesses in the previous surgical site. He was treated with aspiration of the subgaleal abscess and ciprofloxacin antibiotic therapy; he made a full recovery. Cultures of the aspirate identified S. enteritidis, although the primary site of infection was not detected.
Conclusions:
Although postoperative S. enteritidis infections are rare, the large numbers of patients with malignant brain tumors who require tumor resections and receive corticosteroids are at great risk. Adequate drainage (if possible), early isolation of the pathogens, and control of the infection by antibiotic therapy guided by antimicrobial susceptibility testing are vital components to prevent this potentially fatal condition.
Keywords: Brain abscess, complication, giant cell glioblastoma multiforme, infection, Salmonella enteritidis, Salmonella infection, scalp abscess, surgical site infection
INTRODUCTION
Central nervous system (CNS) infections due to Salmonella species are uncommon.[6,9,12,15] Among them, the occurrence of postoperative complications caused by Salmonella enteritidis is particularly rare.[11] Only eight cases of S. enteritidis infection following intracranial surgery for brain tumor have been reported in the world literature to date.[1,4,5,7,13,14,16] We describe a previously healthy man who developed both scalp and brain abscesses due to S. enteritidis after a craniotomy for the resection of a giant cell glioblastoma multiforme. The patient recovered as a result of aspiration of the subgaleal abscess followed by ciprofloxacin antibiotic therapy. A literature review of previously published cases is also presented.
CASE DESCRIPTION
A 36-year-old man with no significant medical history, presented to our medical center with headache, nausea, episodic seizures, and personality changes for 1 month. He was afebrile, had no focal neurologic deficits, and had no systemic abnormalities on clinical examination. Magnetic resonance imaging (MRI) of the head revealed a 3-cm diameter right posterior parietal parafalcine, dura based, enhancing lesion, suggesting an extra-axial tumor [Figure 1]. A right posterior interhemispheric approach was performed for tumor resection. At craniotomy, the tumor was found to be intra-axial with adjacent dural invasion. A near total resection of the tumor was performed. Histopathologic examination of the tumor demonstrated a giant cell glioblastoma multiforme. No bacteria were identified on histological analysis. Postoperatively, the patient demonstrated progressive improvement and was given valproic acid and methylprednisolone as antiepileptic and antiedema treatment. He was discharged to home on the 6th day postsurgery. The sutures were removed on the 14th postoperative day with normal appearing wound healing.
Figure 1:
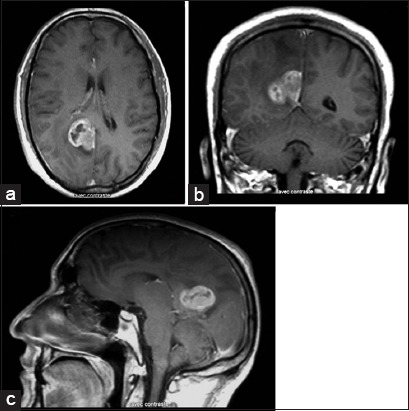
Following gadolinium injection, axial. (a) Coronal. (b) And sagittal. (c) Sections of T1-weighted magnetic resonance imaging demonstrating the parafalcine tumor localized in the right posterior parietal region before the first operation. Note the close spatial relationship of the tumor to the falx cerebri.
5 weeks after surgery, the patient presented with worsening headache and painful swelling at the cranial operative site. Head computed tomography (CT) scan demonstrated a subgaleal extracranial homogenous low-density lesion with rim enhancement following contrast administration. There was also another intracranial ring-enhancing collection at the glioblastoma resection cavity, suggesting a brain abscess [Figure 2a]. There was no contiguous cranial or bone flap osteomyelitis on CT bone window images. The MRI showed both extracranial and parasagittal cystic masses with homogenous, low-intensity signal on T1-weighted images, and high-intensity signal on fluid-attenuated inversion recovery sequences, with significant cerebral edema surrounding the resection cavity and peripheral enhancement after gadolinium injection [Figure 2b-2e]. Clinically, the patient was conscious and afebrile without signs of meningeal irritation or neurologic deficits. His wound was well-healed without purulent discharge. Laboratory studies disclosed a white blood cell count of 16 × 109/L (66.5% neutrophils and 22.7% lymphocytes) and a C-reactive protein (CRP) level of 36.2 mg/L, but blood cultures remained negative. Percutaneous needle aspiration of the subgaleal collection yielded approximately 80 mL of purulent material. The suppurative material was submitted for aerobic and anaerobic microbiological studies as well as for fungal analysis. Empiric antibiotic therapy was started with ciprofloxacin, gentamicin, and metronidazole. Gram stain of the pus revealed Gram-negative bacilli. Cultures demonstrated the growth of S. enterica, serotype Enteritidis. Ciprofloxacin was continued based on the culture sensitivities. The patient was discharged after 4 weeks of intravenous antibiotic therapy and was given oral ciprofloxacin at home for an additional month of treatment. Follow-up CT revealed a gradual reduction in abscess volume until its complete resolution 10 weeks after starting antibiotic therapy (CRP level was reduced to 5 mg/L). The patient was then sent to an oncologic center for further management.
Figure 2:
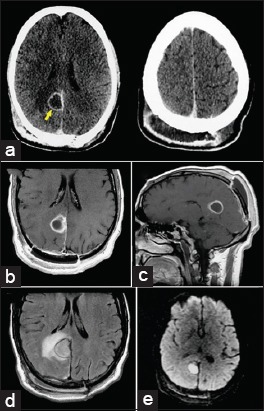
Postoperative axial computed tomography following contrast administration. (a) Revealing a subgaleal extracranial homogenous low-density lesion with rim enhancement (right). There was also another intracranial ring-enhancing collection at the site of the tumor resection cavity (left), suggesting a brain abscess (arrow). Postoperative magnetic resonance imaging showing both extracranial and parafalcine cystic masses with homogenous, low-intensity signal on T1-weighted images. (b and c) And high-intensity signal on the fluid-attenuated inversion recovery sequence. (d) There was peripheral enhancement after gadolinium injection (b and c) and significant cerebral edema surrounding the resection cavity. (d) Note the restricted diffusion-weighted image (bright signal) of the extracranial and parafalcine collections (e).
DISCUSSION
Salmonellosis is usually a self-limited disease that generally causes gastrointestinal tract infection in humans through the oral route. Extraintestinal infections are uncommon, especially in the CNS, and may remain undetected due to a lack of fever and gastroenteritis.[12,13,15] Until 2000, about 70 cases of focal intracranial salmonellosis were described in the world literature including brain abscesses, subdural empyemas, and epidural abscesses.[8] Few cases were added thereafter. However, infections following neurosurgical procedures are rare. Searches using MEDLINE database were performed and only eight cases of S. enteritidis infection following brain tumor resection were identified from 1966 to date.[1,4,5,7,13,14,16] A summary of the eight patients and the one described herein is provided in Table 1. 4 (44.4%) of the nine cases occurred in women. All but one of the nine cases was reported in a child and the average age was 41.5 years (range, 26 months–72 years). All patients were operated on for an intracranial supratentorial tumor: four patients with glioblastoma, one with a metastatic tumor due to embryonal carcinoma, one with ependymoma, one with astrocytoma, one with anaplastic oligodendroglioma, and one with craniopharyngioma. All patients were receiving systemic corticosteroid treatment except for one.[14]
Table 1:
Summary of nine cases (including our case) with Salmonella enteritidis infection following cranial tumor surgery reported in the world literature to date.

All patients had a cranial surgical site infection (SSI). In addition, two cases also had gastroenteritis and one patient had concomitant infectious arthritis of the hip. The organism was identified from samples of the cranial SSI in all patients and also from samples outside the SSI in eight cases (six from blood cultures and two from stool cultures). The most common predisposing factors to infection were corticosteroid use and malignancy, but no patient was seropositive for HIV infection.
The clinical features of these patients did not differ from those with SSI caused by other bacteria.[3] The most frequent symptoms at presentation were fever (five cases), altered awareness (four cases), and headache (three cases). Focal neurological deficits were observed in two patients. Meningismus was noted in two instances. Scalp swelling and scalp wound infection were observed in one patient each. The duration of symptoms was documented in seven patients and had an average duration of 2.21 weeks (from 3 days to 5 weeks).
Adequate drainage (if possible), early isolation of the pathogens, and control of the infection by antibiotic therapy guided by antimicrobial susceptibility testing are essential to prevent this potentially fatal condition.[2,3] In our review, all of the nine patients were on antibiotics. Four received treatment with regimens including ceftriaxone and/or ciprofloxacin, in combination with other antimicrobial agents in three patients. Antibiotic regimens lasted between 1 and 4.5 months. Surgical drainage of the suppurative collection was undertaken in seven patients. Percutaneous scalp aspiration and bone flap removal were performed in one patient each. Complete clinical resolution was achieved in seven patients. One case recovered from neurological clinical symptoms but with subsequent sequelae (residual hemiparesis) and one patient who had severe meningitis died 8 days into antibiotic therapy. These relative favorable results reflect the fact that most of these cases received prompt surgical and antimicrobial treatment.
Among the few cases of reported S. enteritidis infection following craniotomy in literature, this is the first case of the simultaneous occurrence of brain abscess and extracranial scalp abscess. The ability of these bacteria to produce a cranial SSI remains unexplained. Although the origin of infection was unclear in our previously healthy patient, the course of corticosteroids that he received and the original malignant intracranial tumor could have predisposed him to infection followed by potential hematogenous spread to the cranial surgical site. Furthermore, the absence of underlying systemic disease seems to be crucial for the cure of our patient. Finally, the possibility of postoperative Salmonella infection should be considered in patients with malignant brain tumor having surgery.
Contributor Information
Ali Akhaddar, Email: akhaddar@hotmail.fr.
Walter Hall, Email: hallw@upstate.edu.
Mohammed Boucetta, Email: boucetta.mohamed@hotmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Aissaoui Y, Azendour H, Balkhi H, Haimeur C, Atmani M. Postoperative meningitis caused by an unusual etiological agent Salmonella enteritidis. Neurochirurgie. 2006;52:547–50. doi: 10.1016/s0028-3770(06)71365-0. [DOI] [PubMed] [Google Scholar]
- 2.Akhaddar A, Zalagh M, Gazzaz M, Boucetta M. Brain abscess as a complication of intranasal ethmoidectomy for sinonasal polyposis. Surg Infect (Larchmt) 2010;11:483–5. doi: 10.1089/sur.2009.031. [DOI] [PubMed] [Google Scholar]
- 3.Akhaddar A. Surgical site infections in cranial surgery. In: Akhaddar A, editor. Atlas of Infections in Neurosurgery and Spinal surgery. Switzerland: Springer International Publishing; 2017. pp. 191–215. [Google Scholar]
- 4.Blázquez D, Muñoz M, Gil C, Ruibal JL, El Knaichi F, Aleo E, et al. Brain abscess and epidural empyema caused by Salmonella enteritidis in a child: Successful treatment with ciprofloxacin: A case report. Cases J. 2009;2:7131. doi: 10.1186/1757-1626-2-7131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bossi P, Mion G, Brinquin L, Bonsignour JP. Postoperative brain abscess caused by Salmonella enteritidis. Presse Med. 1993;22:130. [PubMed] [Google Scholar]
- 6.Diebold P, Humbert J, Djientcheu Vde P, Gudinchet F, Rilliet B. Salmonella epidural abscess in sickle cell disease: Failure of the nonsurgical treatment. J Natl Med Assoc. 2003;95:1095–1098. [PMC free article] [PubMed] [Google Scholar]
- 7.Fiteni I, Ruiz FJ, Crusells MJ, Sanjoaquin I, Guillen G. Salmonella enteritidis multifocal infection of the central nervous system. Efficacy of new cephalosporins. Presse Med. 1995;24:309–11. [PubMed] [Google Scholar]
- 8.Hanel RA, Araújo JC, Antoniuk A, da Silva Ditzel LF, Flenik Martins LT, Linhares MN, et al. Multiple brain abscesses caused by Salmonella typhi : Case report. Surg Neurol. 2000;53:86–90. doi: 10.1016/s0090-3019(99)00161-5. [DOI] [PubMed] [Google Scholar]
- 9.Lloret MD, Escudero JR, Hospedales J, Viver E. Mycotic aneurysm of the carotid artery due to Salmonella enteritidis associated with multiple brain abscesses. Eur J Vasc Endovasc Surg. 1996;12:250–2. doi: 10.1016/s1078-5884(96)80116-x. [DOI] [PubMed] [Google Scholar]
- 10.Luciani L, Dubourg G, Graillon T, Honnorat E, Lepidi H, Drancourt M, et al. Salmonella enterica serovar enteritidis brain abscess mimicking meningitis after surgery for glioblastoma multiforme: A case report and review of the literature. J Med Case Rep. 2016;10:192. doi: 10.1186/s13256-016-0973-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Millward CP, McMullan NK, Vaiude P, da Rosa SP, Riordan A, Burn SC, et al. Extradural abscess secondary to Salmonella enteritidis in a child following fronto-orbital facial advancement and remodeling surgery. J Craniofac Surg. 2014;25:489–91. doi: 10.1097/SCS.0000000000000643. [DOI] [PubMed] [Google Scholar]
- 12.Noguerado A, Cabanyes J, Vivancos J, Navarro E, Lopez F, Isasia T, et al. Abscess caused by Salmonella enteritidis within a glioblastoma multiforme. J Infect. 1987;15:61–3. doi: 10.1016/s0163-4453(87)91476-9. [DOI] [PubMed] [Google Scholar]
- 13.Rodriguez RE, Valero V, Watanakunakorn C. Salmonella focal intracranial infections: Review of the world literature (1884-1984) and report of an unusual case. Rev Infect Dis. 1986;8:31–41. doi: 10.1093/clinids/8.1.31. [DOI] [PubMed] [Google Scholar]
- 14.Sait M, Rahmathulla G, Chen TL, Barnett GH. Rare case of intracranial Salmonella enteritidis abscess following glioblastoma resection: Case report and review of the literature. Surg Neurol Int. 2011;2:149. doi: 10.4103/2152-7806.86226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sarria JC, Vidal AM, Kimbrough RC., 3rd Salmonella enteritidis brain abscess: Case report and review. Clin Neurol Neurosurg. 2000;102:236–9. doi: 10.1016/s0303-8467(00)00099-8. [DOI] [PubMed] [Google Scholar]
- 16.Schröder J, Palkovic S, Kipp F, Wassmann H. Salmonella enteritidis causing brain abscess and coxitis following intracranial surgery. Acta Neurochir (Wien) 2003;145:919–21. doi: 10.1007/s00701-003-0106-2. [DOI] [PubMed] [Google Scholar]