

Abstract
Despite decades of animal experimentation, human translation with cell grafts, conduits, and other strategies has failed to cure patients with chronic spinal cord injury (SCI). Recent data show that motor deficits due to spinal cord transection in animal models can be reversed by local application of fusogens, such as Polyethylene glycol (PEG). Results proved superior at short term over all other treatments deployed in animal studies, opening the way to human trials. In particular, removal of the injured spinal cord segment followed by PEG fusion of the two ends along with vertebral osteotomy to shorten the spine holds the promise for a cure in many cases.
Keywords: Electrical stimulation, GEMINI, polyethylene glycol, spinal cord fusion, spinal cord transection
To L. Walter Freeman, in memoriam
Those who cannot remember the past are condemned to repeat it.
George Santayana
TREATMENT OF SPINAL PARALYSIS: STATE-OF-THE-ART
Spinal cord injury (SCI) in man often leads to severe permanent disability. Ever since the work of Ramon and Cajal,[102] long-distance regeneration of injured axons across an injured segment of the cord has proven elusive. The limited regenerative capacity of the adult mammalian spinal cord has been attributed to the formation of cavities (cysts) and scarring that interrupt the ascending and descending pathways, low intrinsic regenerative state of injured neurons, and unfavorable microenvironment, such as an inhibitory extracellular matrix (ECM) that develops around the site of injury, inhibitory myelin-associated proteins (e.g., Nogo-A, MAG, and OMgp) and a lack of growth-promoting factors, such as neurotrophins.[32,120]
Several therapeutic strategies have been deployed over the past 40 years in experimental animals, with a focus on cell grafts, particularly grafts of various types of stem cells, into the injury site, to form a neuronal relay circuit across the gap.[6,31,34] A neuronal relay calls for synapse formation between the host extending axons from the rostral area to the injury/graft site and the donor neurons in the injury/graft site of spinal cord, appropriate release of neurotransmitters of the donor neurons, extension of axons from the donor neurons to areas caudal to the injury/graft site, and finally synapse formation between the donor extending axons and the host neurons in areas caudal to the injury/graft site. Both remyelination of axons across the lesion and generation of new neurons are necessary to achieve these goals.[6,31,34]
Spurred by promising animal studies, clinical trials of a wide variety of different cell lines implanted at or around the lesional level (Schwann cells – SC, olfactory ensheathing glia – OEG - residing either in the lamina propria or along the nerve fiber layer of the olfactory bulb, mesenchymal/stromal stem cells – MSC, some of which may acquire neuronal properties, multipotent progenitor cells – MPC, neural stem/progenitor cells – NSC, embryonic stem cells – ECS, and umbilical cord blood cells) have been (and are being) conducted over the past 20 years.[6,31,34] No biological cure defined as independent, permanent, and unaided deambulation has been achieved to date. Some open-label, uncontrolled reports claimed positive effects, even years after the injury, with some patients walking again for short distances with braces and support (although far from restitutio ad integrum).[27,59,103] However, negative studies and complications are equally on record.[1,6,28,31,34,113] Scaffolds in combination with cell grafts have been implanted, but early results do not seem especially promising.[134]
In sum, while some benefit may accrue from cell grafts and other techniques, they alone cannot cure paralysis.[132] As emphasized recently, “it would be difficult to find any other branch of science with over a century of such sterile endeavour. In effect, there has been repetition of the same idea, albeit with different techniques, that is, looking at the lesion site. Are we sentenced to repeating the same experiments in the hope of expecting a different result?”[55]
In this paper, we will review the evidence supporting an idea posited half a century ago by the US neurosurgeon L. Walter Freeman, namely that a permanent, biological cure is possible in several cases, by cutting out the most damaged portion of the spinal cord and connecting the two free ends, after spinal shortening [Box 1].[42] One should notice that removing the epicenter of a damaged cord and then connecting the two fresh ends is akin to reconnecting a transected spinal cord tout court. The process would be spearheaded by the use of so-called fusogens (GEMINI protocol).[21] Another group recently upheld this same concept.[94]
Box 1:

Walter freeman and the cure of paralysis.
Box:

Rating scales in dogs.
SPINAL CORD TRANSECTION: NATURAL HISTORY
In man, no recovery follows spinal cord transection (SCT) at whatever level as seen, for example, after stab wounds.[26,74,77,105,112,117] When the transection is partial, recovery is possible: 66% of 450 patients with stab wounds could eventually walk without or with only minimal help in one series and over half of 217 patients returned to their former occupation, usually within 6 months of the injury, in another.[4,84] Brown-Sequard types of lesion (i.e., hemisections) also recover: for instance, two patients with cervical hemisection recovered walking at 10 and 2 years[35] and another recovered almost completely at 3 years.[33] If the section is >50% (of a hemisection), results are similar to a complete section: in a representative patient, whose spinal cord was almost completely divided at C7/T1, only sensory disturbance was slightly improved at 4 months after the injury.[126]
A similar assessment applies to experimental animals. Handa et al.[49] performed a T9–10 SCT on 9 adult female dogs. Follow-up lasted 6–39 months. Within several weeks, muscle tone of the hindlimbs was gradually increased accompanied by the development of flexion reflex with after-discharge in addition to monosynaptic reflexes. Alternating stepping movements also began to develop. Afterward, extensor thrust and crossed extension reflex were observed. Standing behavior of the hindlimbs was found after sufficient development of the extensor thrust and correct placement of the pads of the toes. Steady development of stepping and standing caused forward locomotion using fore – and hindlimbs; 7 out of 9 could walk on open ground. This ability of locomotion by the hindlimbs of the spinal dogs reached a plateau 6 months after the surgery. Walking behavior of the hindlimbs was not inhibited by additional SCT in the two dogs where it was done, pointing to spinal automatisms and development of responses induced by afferent inflow from outside the cord as the reason for such functional recovery. This was corroborated by the electrophysiological absence of conduction across the transection. Veterinary experience shows that a section >50% at C5–6 in dogs is lethal,[12] unlike hemisections.[78]
Rodents follow a similar pattern. In untreated mice with dorsal SCT, 33% displayed weak nonbilaterally alternating movements (NBA) at 1 week. At 2 weeks, increased NBA were observed and the first BA movements in 10% of the animals. A progressive increase of movement frequency and amplitude was found after 2–3 weeks. By the end of the month, 86% displayed mixed NBA and BA. However, none of them recovered the ability to stand or bear their own weight with the hindlimbs.[47] On the Basso-Bresnahan-Beattie (BBB) scale,[10] a successor of the Tarlov’s open field test, recovery from dorsal SCT in rats is no better than 3 out of 21 points at 6 weeks.[11] Rarely, scores of 5 have been reported, but these do not signal useful recovery, even if higher than controls [Table 1]. Conversely, most hemisection and contusion injury SCI models exhibit high rates of spontaneous recovery of locomotion[111] and are thus of dubious translational significance. In monkeys submitted to C7 hemisection, locomotor recovery is also fairly extensive.[110] In sum, in mammals, SCT leads to unrecoverable paralysis.
Table 1:
Summary of behavioral outcomes of controlled studies utilizing the Basso-Bresnahan-Beatty scale after complete spinal cord transection in rodents and associated therapeutic interventions.

SPINAL CORD TRANSECTION: EXPERIMENTAL TREATMENT IN ANIMALS
It is clear from the above section that SCT lends itself as the ideal model to study neuroregenerative strategies. However, marked differences exist between human and rodent spinal cords both in anatomy and secondary injury processes,[32,43,91,137] while strong similarities exist between humans and dogs.[86,131] Unfortunately, canine studies of SCT, despite their greater translational relevance, are sparse. One has, thus, to bank on rodent studies in selecting promising translational avenues. The outcome in rodents is often plotted on the BBB scale (above), which allows comparisons among treatments at different time points. Ideally, a promising rodent study will show strong recovery within a very short time-frame. Unfortunately, the vast majority of published studies report useful recovery – when positive – after up to 2–9 months [Table 1]. Since 1 rat month is comparable to 3 human years,[116] translation to the clinic would imply many years before any effect is seen in man. It is thus imperative that we consider only the extent of recovery at no >1 month and then evaluate the effect in larger animals.
As can be seen from Table 1, acutely deployed (i.e., immediately after SCT) polyethylene glycol (PEG) fusion is superior to any other acute strategy published to date, including various cell grafts, conduits, and gene therapy. At 4 weeks no other technique approaches the extent of recovery seen with PEG fusion. This result has been corroborated by independent replication in separate laboratories in Japan, Korea, and China. Remarkably, PEG is inexpensive and easy to deploy, while most other technologies are labor-intensive and/or costly and/or highly specialized.
In the few canine studies, PEG fusion is again superior [Table 2]. For instance, Wu et al.[133] reported no motor function in the pelvic limbs at 15 days after the surgery (Olby score 0), with the gradual recovery of motor function of the pelvic limbs starting from the 1st month after stem cell grafting. On the contrary, in the PEG study,[80] motor recovery in treated animals began at 3 days (median cBBB score 2 vs. 0 in controls).
Table 2:
Canine studies of spinal cord transection.

Even in monkeys, cell grafts are not especially promising, despite claims to the contrary in some papers. For instance, a grafting study of human fetal spinal cord-derived neural progenitor cells after C7 hemisection reported a >25% improvement in object manipulation scores in four of five monkeys (vs. 1 out of 4 controls that improved so) and a 12% improvement in climbing score, beginning several months after grafting.[110] This is far from striking, and in line with clinical outcomes in man (see above); in addition, there was no lesioned sham control group, and monkeys with poor graft survival did not live as long as monkeys with surviving grafts. Instead, preliminary data suggest that PEG fusion is superior to this kind of grafts in a monkey model of SCT (manuscript in preparation).
It is worth mentioning that minimal retraction is seen after SCT and that in these cases PEG acts initially as a neuroprotectant (see below) and a bridge for regenerating axons across the gap. In the model suggested in this article, apposition is complete and PEG would also act as an axonal fusogen.[23] Thus, reported results of PEG fusion [Tables 1 and 2] represent an absolute minimum and these are expected to improve further both in terms of rate and extent of recovery once the severed ends of the cord are non-compressively approximated.
In conclusion, PEG fusion is an ideal candidate for a clinical trial.
UNDERSTANDING SCT
To understand the fusion process, one has to first understand the cellular processes in play in the setting of SCT.
Yoshida et al.[138] studied SCT in the rat. The sharpness of the transection turned out to be one of the most important factors for successful axonal regeneration. An extremely sharp transection produced edema-free lesions and later formed neither cysts nor scars, whereas a relatively blunt transection produced edema followed by scars and cysts around the lesions. Consequently, the spinal cord was transected using the edge of a razor which was as sharp as possible to minimize traumatic injury. However, the stump of the spinal cord developed edema, as in their model it took 10 or 20 min to bring together the two ends of the sectioned cord. This dovetails with a rodent study: the ends of the transected spinal axons remain stable for only about 10–20 min before undergoing fragmentation (the first step before classic Wallerian degeneration, or dieback) at both ends spanning 0.3 mm, only to stabilize and persist for 3–7 days; however, about 30% of proximal axons then start growing again within 6–24 h.[63]
Ramon and Cajal[102] already noticed “traumatic degeneration” in both stumps within 1 h of SCT in rabbits. Other studies showed that, immediately following SCT, axoplasm escapes from both the proximal and distal portions of some of the cut axons: the extent of the axoplasmic loss is generally greater in larger myelinated fibers. In contrast, small fibers, whether myelinated or unmyelinated, show little if any loss of axoplasm.1 h after SCT, the proximal and distal ends of the axons have retracted from the transection site, and both ends are separated by 1–2 mm or more from the transection site. The axoplasmic leakage stops within a few hours of the transection. Electron microscopic observations indicate that the tip of an axon is lined by axolemma within 1 h; in addition, layers of collapsed myelin form a septum in front of the axonal tip. At about 3 h after axonal transection, the axon becomes swollen and irregular in shape and massive accumulation of lysosomes and release of autolytic lysosomal hydrolases is observed within both the rostral and the caudal spinal cord stumps, peaking at 3–7 days and declining at 14 days: cavitation is the result.[38,62,95] Both the proximal and distal ends swell because axoplasmic transport is bidirectional. Degeneration spreads in both directions along the axon from the transection site, but only for a short distance in the proximal portion: in a clean cut, only one or two internodes may be involved within the proximal stump.[25] In the distal axon, however, Wallerian degeneration occurs.
In view of this data, it is obvious that whatever treatment must be brought to bear within minutes (<10).
FUSOGENS: THE ENGINE OF RECOVERY
Fusogens comprise a class of substances that have the capacity to reseal damaged cell membranes. Included in this class is PEG. PEG is a relatively inexpensive, stable, nontoxic, fully biocompatible, and water-soluble linear polymer that is synthesized by the living anionic ring-opening polymerization of ethylene oxide with molecular weights ranging from 0.4 to 100 kDa. It has a wide range of clinical and pharmaceutical applications, including, among others, an oral laxative, and several PEGylated drugs. PEG is FDA-approved for use as a preservative additive before organ transplantation to limit cold ischemia/reperfusion injury.[100] It does not accumulate in the body and crosses the blood–brain/spinal-barrier. It is considered immunologically inert, although anti-PEG antibodies have been detected in patients treated with and without PEGylated drugs, perhaps due to the widespread use of PEG in household products including toothpaste and shampoo.[44]
PEG has been shown to be strongly neuroprotectant thanks to its membrane sealing/fusing properties [Box 2].[70,83,108] PEG reduces both necrosis and apoptosis through two distinct yet synergistic pathways, i.e., repair of disrupted plasma membranes and protection of mitochondria through direct interaction. PEG may reduce the neuronal membrane tension and improves the membrane’s fluidity so that sealing may occur, even in low-temperature conditions.[93,135] Interestingly, Nehrt et al.[93] noted that axons with small diameters preferentially benefited from PEG-mediated axolemmal resealing: many neurons of the truncoreticulopropriospinal (TRPS) meshwork (see below) are small-sized. Zhang et al.,[139] in a lamprey model, found that axon resealing is a critical determinant of neuron survival and the artificial acceleration of resealing with PEG reduced retrograde neuronal apoptosis by 69.5% at 2 weeks after SCI. They also reported that factors other than Ca++ diffusion into the injured tip contribute to retrograde death signaling and that the larger the neuron an axon belongs to, the slower the resealing.
Box 2:

A brief history of PEG fusion in the nervous system.
Certainly, not all PEGs are created equal, and there is some evidence that molecular weight and other factors can influence the fusogenic potential and extent of recovery [Table 1],[135] but data are conflicting. Nakajima and Ikada[90] reported that PEG should be applied for 1 min to avoid overfusion (that leads to cell death) in cell cultures and that at least 10 min are necessary for significant morphological changes to occur indicating that membrane fusion does not materialize instantly on exposure but gradually proceeds with time: optimum molecular weight for fusion occurred at PEG concentrations of 50% w/w (<30% was ineffective) and a molecular weight around 1000. Hoffman et al.[53] reported that PEG at a concentration of 75% may be the optimal concentration in cell cultures. Kouhzaei et al.[71] showed that the lower PEG’s molecular weight, the higher was the ultimate recovery of spinal cord evoked potentials (i.e. PEG 200:49.5% and PEG 2000: 16.3%). Lower molecular weight PEGs caused higher membrane sealing rate (77.8 ± 3.5 for PEG400 [20% w/w] vs. 32.1 ± 6.9 for PEG2000 [20% w/w]). PEG1000 and 2000 showed no significant sealing effects at high concentrations (>50%). Our study[135] found PEG 1400 superior to PEG 4000, but both led to recovery. Wang et al.[129] found that 1, 2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[methoxy(poly (ethylene glycol)) 2000] can achieve electrophysiological conduction in isolated spinal cords as effectively as PEG 2000 (50% concentration in Krebs’ solution applied for 4 min), but at much lower concentrations than PEG. In any case, PEG has an extremely rapid action. Kim performed cervical laminectomy at C5 in a rat SCI model and then immediately applied PEG-600 or saline. Measurements of motor evoked potential (MEP) found that PEG-treated animals showed an increase in the measurement of MEP’s amplitude (mean of 0.081 vs. 0.156 mV) at 1 h after injury.[64]
PEG has been combined with graphene nanofibers that are known to promore axonal regeneration.[65,67,121] and also carry electrical charges. The nanoscale material may be useful for enhancing neuronal signaling by direct contact with the neurons: Kim et al.[65] reported near-normal recovery of SSEPs after SCT in rats at 24 h versus none in controls. In vitro, nanocomposites composed of 20% w/v PEG and 0.1% w/v multi-walled carbon nanotubes result in high neurite outgrowth and neurite length: electrical stimulation (30 V m-1 DC for 1 h) further significantly enhances this growth up to two-fold.[56]
Another fusogen is chitosan, a nontoxic, biodegradable polycationic polymer with low immunogenicity that has been extensively investigated in various biomedical applications. Topical application of chitosan after complete transection of the guinea pig spinal cord facilitated sealing of damaged neuronal membranes and restored the conduction of nerve impulses through the length of spinal cords in vivo.[30]
THE ANATOMICAL BASIS OF SPINAL CORD FUSION
Although experiments show that PEG can refuse severed spinal cord fibers, yet the number is limited (10–15%); in addition, fibers are not matched at the moment of fusion. It can be argued that the reason for its effectiveness is mostly due to PEG neuroprotectant potential of the cord gray matter cellular milieu. In other words, PEG does not actually achieve its goal by refusing a large number of long-projection fibers in the white matter brought together by manipulation of the transected ends of the spinal cord[118] rather it protects the spinal propriospinal matrix that is truly responsible for much of motor and locomotor activities.[21,22]
In mammals, including monkeys and man, there exists a network of interneuronal cells located throughout the rostrocaudal length of the brainstem and spinal cord that conveys motor (and sensory) signals and that embeds and connects the brainstem, cervical and lumbar central pattern generators [so-called cortico-truncoreticulo-propriospinal system – CTRPS – or Motor Highway 2: Box 3].[21,22] Evidence in humans supports the key role of this system in recovery from SCI.[22]
Box 3:

A brief history of propriospinal neurons: Discovered, forgotten, and rediscovered and why they matter.
Spinal fusion is made possible because transection only minimally damages a thin layer of cells belonging to this matrix, allowing the gray matter neuropil to immediately resprout severed axons and dendrites (regenerative sprouting) at the interface of the apposed cords. It should be noted that a sharp transection typically generates <10 Newtons (N: SI unit of force) of force versus approximately 26,000 N experienced during clinical SCI, a 2600 times difference.[122] Iseda et al.[58] concluded that “a single severance, which minimizes damage in the lesion site,…spare(s) nearby cells. On the other hand, a repeated severance inflicts (damage to a) much larger area, which would make it difficult to recruit immature astrocytes in the early postinjur(y) period.” PEG would protect all cells damaged by the blade. The histological evidence of propriospinal circuits regenerating synaptic connections across the spinal cord transection site is clear-cut.[37,127,133]
An important concern is scarring after SCT. In all published studies, PEG has been applied immediately after SCT. Scarring becomes visible only after about 1 week: given a 1 mm/die regrowth rate, regenerating axons from both cord ends will have penetrated the opposite gray matter well by then (66 mm/h).[94] Nonetheless, there is compelling supporting evidence that the astrocytic scar may actually promote axon regrowth in the early – but not late-stages of SCI.[79,109] PEG does not prevent the formation of a scar and thus does not deprive the regrowth process of the beneficial effects of the early scar past the 1st week.[66,81]
Function will be restored also due to rewiring upstream in the central nervous system (CNS), so long as the mismatch is not extreme. Indeed, recovery from any anatomic disruption of the spinal cord utilizes the entire CNS, namely, cord, brainstem, and brain, in which a massive degree of reorganization (large-scale “rewiring”) occurs:[57] mismatches, including those seen in clinical SCI with subsequent recovery, are thus compensated, as in PNS model of fusions.[106]
PAIN AFTER SCT
SCI is followed in up to 40% of cases by so-called cord central pain (CCP).[19,20] CCP is a hugely disabling chronic pain condition that might offset any possible motor benefit of any regenerative treatment. Fortunately, in all animal studies of SCT to date, even at long term, CCP has never been reported. This is a key point. Following cordotomies in man, i.e., section of the spinothalamic (STT) pathways, CCP is seen in up to 20% of the patients. One likely explanation is that CCP is triggered in susceptible individuals by an imbalance between damaged STT and spared lemniscal pathways, which is not the case in SCT, in which both spinothalamic and lemniscal fibers are cut simultaneously.[19,20] However, CCP can follow SCT in man, so this theory does not seem viable. A likely explanation is that acute treatment immediately after SCT somehow quells the pathological cascade from engaging the central pain generator,[19,20] On the other hand, cell grafting for SCI has triggered CCP in more than half of the patients in a study.[68]
CCP is generally accompanied by hyperactivity in the TRPS pathway, which can be quelled by extensive neurosurgical destruction thereof at both brainstem and cord levels: pain is controlled to a major extent.[19,20] Given the model proposed in this review, extirpation of the damaged cord segment followed by fusion might be able to control CCP.
CLINICAL TRANSLATION
Experimental evidence [Tables 1 and 2] make it clear that PEG is most effective when applied locally and acutely on lesioning. This can be tapped with different approaches, all based on the removal of the injured segment of the cord.
Gemini
As discussed, Walter Freeman suggested the severance-reapposition model for chronic SCI; he removed the damaged segment of the cord in dogs creating a gap, performed a complete en bloc vertebrectomy thus shortening the spine, brought the two fresh cord stumps in contact with fresh plasma and sutured the dura tightly: walking animals resulted after several months. He observed direct electrophysiological conductance across the apposed stumps and provided histological evidence of axonal regeneration across the sectional interface [Box 1].[39-41,21,23,51,52] Spine-shortening vertebral osteotomy (a.k.a. vertebral column resection), which shortens the spinal column, is a surgical technique for correcting severe spinal deformities, treating congenital spinal anomalies, such as cord tethering, traumatic spine dislocations, and spine tumors at both cervical and thoracolumbar levels.[5,54,87,101,123] In the proposed GEMINI model,[21,22] section of the damaged segment of the cord is performed at the moment of removing the vertebral body; the two ends will need further trimming so that no undue pressure is exerted on either stump by pressure vectors (too much pressure would lead to squeezing and local ischemia, jeopardizing the result). PEG is applied at this moment. Notice that the vertebra has been removed and stabilization carried out simultaneously [Figure 1a].[21-23] Another way to stabilize the fusion interface has been proposed recently: Brazda et al.[14] kept the two spinal cord ends in apposition by a microconnector system incorporating a microchannel system, through which PEG was infused through a minipump. This allowed a tension-free, precise apposition of sharply transected nerve spinal cord stumps, as required by GEMINI. The spinal cord tissue staid in place within this device after the tissue opposition maintained by this vacuum system was released. The minimal, gradual stretch to the axons actually stimulated regrowth. However, until biodegradable connectors are built, this technology remains unviable in man.
Figure 1:
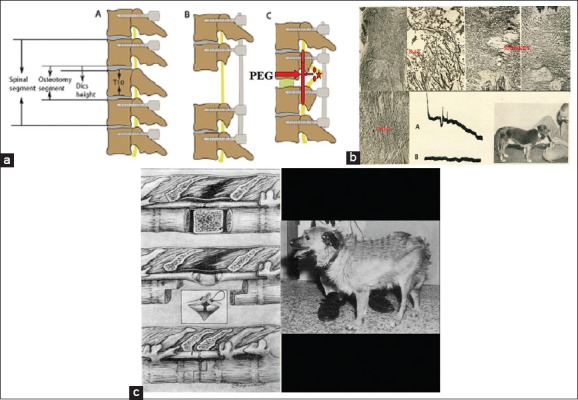
(a) Proposed model of removal of the injured segment (star), transection of the cord above and below (ovoids) and fusion with polyethylene glycol (arrow) along with vertebral shortening and stabilization (adapted from Qiu et al., 2015). (b) Box 1: Freeman discovered that regrowing fibers could be made to grow across the sectional interface in rats, dogs and monkeys and that this translated into electrophysiological transmission and behavioral recovery. (c) Box 1: Since spinal cord transection is not common, Freeman reasoned that he could leverage his technique of spinal cord regeneration in clinical models of spinal cord injury by cleanly cutting the cord above and below the level of injury, removing the injured segment of the cord (2 cm), doing a vertebrectomy and bringing the two fresh ends of the cord together and holding them in place with plasma clot before the dura mater was tightly closed. Dogs could thus be made to rewalk for short distances (the one displayed had almost two thoracic segments removed).
Hydrogelation of the GAP
PEG can be cross-linked to form porous hydrogels, which can serve as biocompatible matrices that can closely mimic the ECM. This suggests another possibility that does not require a vertebrectomy: removing half of the damaged cord, up to its border with rostral and caudal healthy tissue and filling the void with a PEG hydrogel. PEG hydrogels have high water content and porosity, which make them behave like aqueous solutions at a microscopic scale while being macroscopically solid. In an easily tailorable process, these can be optimized by adding different reactive moieties to both ends of the PEG chain. Mosley et al.[89] determined that a Young’s modulus of 907 Pa allows for the longest axonal extensions, which closely abide with the Young’s modulus of the brain and spinal cord.[99] In any case, pure PEG per se is enough to warrant clinical trials without more expensive modifications. Injectable PEG, by in situ gelling, can conform geometrically to the defect without requiring a pre-gelled patient-specific hydrogel or causing additional excision of healthy tissue.[70,83] Although PEG hydrogels can be used as supporting substrates, for example, of mesenchymal stem cells, inducing cell migration, proliferation, and differentiation,[50] this strategy has not been found to be synergistic with PEG in one rodent study.[96] Regenerating propriospinal fibers would course through this hydrogel, which has been proven to lead to recovery after many months.[37] Certainly, the use of PEG alone cannot completely mimic the three-dimensional porous structure of the spinal cord and would allow the upper and lower fiber bundles to grow in mismatched or even misplaced channels or pores, which is not the case with Freeman’s appositional model. Moreover, this approach would need months for recovery and outcomes would be partial, as when the two stumps have been joined with different strategies in chronic SCI patients.[46,125] However, microspheres loaded with neurotrophins (e.g., BDNF and GDNF) could be embedded for slow release to accelerate this regrowth.[73]
Fusion-supported cord grafting
The possibility of implanting a segment of healthy cord from an organ donor must be also entertained [Box 4].
Box 4:

The first cord graft for SCI in man.
In this case, PEG would neuroprotect the tissue until vascularization from the healthy ends of the patient would feed the graft. Biomaterials can be effectively used for promoting and guiding blood vessel formation.[7,48] PEG hydrogels support the formation of vascularized tissue in vivo in a pore size dependent manner.[29] and PEG has been shown to promote angiogenesis in an SCI model.[37]
PEG proxies
As mentioned, another effective fusogen is chitosan. Rao et al.[104] found that NT3-loaded chitosan, when inserted into a 1-cm gap of hemisectioned and excised adult rhesus monkey thoracic spinal cord, elicited robust axonal regeneration: in particular, motor axons in the corticospinal tract not only entered the injury site within the biomaterial but also grew across the 1-cm-long lesion area and into the distal spinal cord, accompanied by motor and sensory functional recovery. Similar data with chitosan scaffolds have been reported in rodents.[92,140]
A combination of both chitosan and PEG in hydrogels promise even better results.[61,88] Blends of photocrosslinkable 4-azidobenzoic acid-modified chitosan (Az-C) and PEG form a semi-interpenetrating network (semi-IPN), where PEG interpenetrates the Az-C network and reinforces it. Nerves anastomosed with an Az-C/PEG gel tolerate a higher force than those with fibrin glue; Az-C/PEG gels are compatible with nerve tissues and cells. In addition, Az-C/PEG gels release PEG over a prolonged period, providing sustained delivery of PEG.[2]
Electrical stimulation
As originally proposed,[21] the entire fusion process can be accelerated by electrical stimulation. Progress has been made by electrical stimulation of the cord combined with intensive, months-long rehabilitation, although full independent recovery has not been achieved.[3,45,60] In GEMINI, electricity would combine central (e.g., rTMS) and/or spinal cord stimulation and/or peripheral stimulation (e.g., TENS), along with motor training, to accelerate regrowth of fibers from the TRPS network across the fusion interface.[24,130] As noted [Box 4], it was Shirres who first emphasized the ability of electricity to stimulate spinal cord regeneration.
CONCLUSION
Removing the chronically injured segment of a cord, followed by spinal shortening and PEG fusion of the healthy ends (GEMINI protocol) has the potential to restore motor function in a substantial number of chronically paralyzed (ASIA A) patients for whom no cure is available.
Contributor Information
Xiaoping Ren, Email: chinarenxg@126.com.
C-Yoon Kim, Email: vivavet@gmail.com.
Sergio Canavero, Email: sercan@inwind.it.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Al Kandari S, Prasad L, Al Kandari M, Ramachandran U, Krassioukov A. Cell transplantation and clinical reality: Kuwait experience in persons with spinal cord injury. Spinal Cord. 2018;56:674–9. doi: 10.1038/s41393-018-0074-2. [DOI] [PubMed] [Google Scholar]
- 2.Amoozgar Z, Rickett T, Park J, Tuchek C, Shi R, Yeo Y, et al. Semi-interpenetrating network of polyethylene glycol and photocrosslinkable chitosan as an in situ -forming nerve adhesive. Acta Biomater. 2012;8:1849–58. doi: 10.1016/j.actbio.2012.01.022. [DOI] [PubMed] [Google Scholar]
- 3.Angeli CA, Boakye M, Morton RA, Vogt J, Benton K, Chen Y, et al. Recovery of over-ground walking after chronic motor complete spinal cord injury. N Engl J Med. 2018;379:1244–50. doi: 10.1056/NEJMoa1803588. [DOI] [PubMed] [Google Scholar]
- 4.Anonymous. Stab wounds of the spinal cord. Br Med J. 1978;1:1093–4. [PMC free article] [PubMed] [Google Scholar]
- 5.Aoun SG, Elguindy M, Barrie U, El Ahmadieh TY, Plitt A, Moreno JR, et al. Four-level vertebrectomy for en bloc resection of a cervical chordoma. World Neurosurg. 2018;118:316–23. doi: 10.1016/j.wneu.2018.07.153. [DOI] [PubMed] [Google Scholar]
- 6.Assinck P, Duncan GJ, Hilton BJ, Plemel JR, Tetzlaff W. Cell transplantation therapy for spinal cord injury. Nat Neurosci. 2017;20:637–47. doi: 10.1038/nn.4541. [DOI] [PubMed] [Google Scholar]
- 7.Bakshi A, Fisher O, Dagci T, Himes BT, Fischer I, Lowman A, et al. Mechanically engineered hydrogel scaffolds for axonal growth and angiogenesis after transplantation in spinal cord injury. J Neurosurg Spine. 2004;1:322–9. doi: 10.3171/spi.2004.1.3.0322. [DOI] [PubMed] [Google Scholar]
- 8.Bamba R, Waitayawinyu T, Nookala R, Riley DC, Boyer RB, Sexton KW, et al. Anovel therapy to promote axonal fusion in human digital nerves. J Trauma Acute Care Surg. 2016;81:S177–S183. doi: 10.1097/TA.0000000000001203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bareyre FM, Kerschensteiner M, Raineteau O, Mettenleiter TC, Weinmann O, Schwab ME, et al. The injured spinal cord spontaneously forms a new intraspinal circuit in adult rats. Nat Neurosci. 2004;7:269–77. doi: 10.1038/nn1195. [DOI] [PubMed] [Google Scholar]
- 10.Basso DM, Beattie MS, Bresnahan JC. A sensitive and reliable locomotor rating scale for open field testing in rats. J Neurotrauma. 1995;12:1–21. doi: 10.1089/neu.1995.12.1. [DOI] [PubMed] [Google Scholar]
- 11.Basso DM, Beattie MS, Bresnahan JC. Graded histological and locomotor outcomes after spinal cord contusion using the NYU weight-drop device versus transection. Exp Neurol. 1996;139:244–56. doi: 10.1006/exnr.1996.0098. [DOI] [PubMed] [Google Scholar]
- 12.Bitar Alatorre WE, Garcia Martinez D, Rosales Corral SA, Flores Soto ME, Velarde Silva G, Portilla de Buen E, et al. Critical ischemia time in a model of spinal cord section. A study performed on dogs. Eur Spine J. 2007;16:563–72. doi: 10.1007/s00586-006-0222-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bittner GD, Ballinger ML, Raymond MA. Reconnection of severed nerve axons with polyethylene glycol. Brain Res. 1986;367:351–5. doi: 10.1016/0006-8993(86)91617-3. [DOI] [PubMed] [Google Scholar]
- 14.Brazda N, Voss C, Estrada V, Lodin H, Weinrich N, Seide K, et al. Amechanical microconnector system for restoration of tissue continuity and long-term drug application into the injured spinal cord. Biomaterials. 2013;34:10056–64. doi: 10.1016/j.biomaterials.2013.09.057. [DOI] [PubMed] [Google Scholar]
- 15.Brown BL, Asante T, Welch HR, Sandelski MM, Drejet SM, Shah K, et al. Functional and anatomical outcomes of facial nerve injury with application of polyethylene glycol in a rat model. JAMA Facial Plast Surg. 2019;21:61–8. doi: 10.1001/jamafacial.2018.0308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bucy PC, Keplinger JE, Siqueira EB. Destruction of the “pyramidal tract” in man. J Neurosurg. 1964;21:285–98. [PubMed] [Google Scholar]
- 17.Buttin G, LeGuern G, Phalente L, Cazenave PA. Production of hybrid lines secreting monoclonal anti-idiotypic antibodies by cell fusion on membrane filters. In: Melchers F, Potter M, Warner NL, editors. Lymphocyte Hybridomas. Berlin: Springer-Verlag; 1979. pp. 27–36. [DOI] [PubMed] [Google Scholar]
- 18.Canavero S. HEAVEN: The head anastomosis venture project outline for the first human head transplantation with spinal linkage (GEMINI) Surg Neurol Int. 2013;4:S335–42. doi: 10.4103/2152-7806.113444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Canavero S, Bonicalzi V. Central pain Syndrome. 2nd ed. Cambridge: Cambridge University Press; 2007. [Google Scholar]
- 20.Canavero S, Bonicalzi V. Central pain syndrome. Basingstoke: Springer-Nature; 2018. [Google Scholar]
- 21.Canavero S. The “Gemini” spinal cord fusion protocol: Reloaded. Surg Neurol Int. 2015;6:18. doi: 10.4103/2152-7806.150674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Canavero S, Ren X, Kim CY, Rosati E. Neurologic foundations of spinal cord fusion (GEMINI) Surgery. 2016;160:11–9. doi: 10.1016/j.surg.2016.01.027. [DOI] [PubMed] [Google Scholar]
- 23.Canavero S, Ren X. Houston, GEMINI has landed: Spinal cord fusion achieved. Surg Neurol Int. 2016;7:S626–8. doi: 10.4103/2152-7806.190473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Canavero S, Ren XP. The spark of life: Engaging the cortico-truncoreticulo-propriospinal pathway by electrical stimulation. CNS Neurosci Ther. 2016;22:260–1. doi: 10.1111/cns.12520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Carpenter MB, Sutin J. Human Neuroanatomy. Philadelphia, PA: Williams and Wilkins; 1983. [Google Scholar]
- 26.Cha YH, Cho TH, Suh JK. Traumatic cervical cord transection without facet dislocations a proposal of combined hyperflexion-hyperextension mechanism: A case report. J Korean Med Sci. 2010;25:1247–50. doi: 10.3346/jkms.2010.25.8.1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chen L, Huang H, Xi H, Zhang F, Liu Y, Chen D, et al. Aprospective randomized double-blind clinical trial using a combination of olfactory ensheathing cells and Schwann cells for the treatment of chronic complete spinal cord injuries. Cell Transplant. 2014;23(Suppl 1):S35–44. doi: 10.3727/096368914X685014. [DOI] [PubMed] [Google Scholar]
- 28.Chhabra HS, Sarda K. Clinical translation of stem cell based interventions for spinal cord injury are we there yet? Adv Drug Deliv Rev. 2017;120:41–9. doi: 10.1016/j.addr.2017.09.021. [DOI] [PubMed] [Google Scholar]
- 29.Chiu YC, Kocagöz S, Larson JC, Brey EM. Evaluation of physical and mechanical properties of porous poly (ethylene glycol)-co-(L-lactic acid) hydrogels during degradation. PLoS One. 2013;8:e60728. doi: 10.1371/journal.pone.0060728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cho Y, Shi R, Borgens RB. Chitosan produces potent neuroprotection and physiological recovery following traumatic spinal cord injury. J Exp Biol. 2010;213:1513–20. doi: 10.1242/jeb.035162. [DOI] [PubMed] [Google Scholar]
- 31.Dalamagkas K, Tsintou M, Seifalian A, Seifalian AM. Translational regenerative therapies for chronic spinal cord injury. Int J Mol Sci. 2018;19:e1776. doi: 10.3390/ijms19061776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dietz V, Schwab ME. From the rodent spinal cord injury model to human application: Promises and challenges. J Neurotrauma. 2017;34:1826–30. doi: 10.1089/neu.2016.4513. [DOI] [PubMed] [Google Scholar]
- 33.Dlouhy BJ, Dahdaleh NS, Howard MA., 3rd Radiographic and intraoperative imaging of a hemisection of the spinal cord resulting in a pure brown-séquard syndrome: Case report and review of the literature. J Neurosurg Sci. 2013;57:81–6. [PubMed] [Google Scholar]
- 34.Donovan J, Kirshblum S. Clinical trials in traumatic spinal cord injury. Neurotherapeutics. 2018;15:654–68. doi: 10.1007/s13311-018-0632-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Dran G, Fontaine D, Litrico S, Grellier P, Paquis P. Stabwound of the cervical spinal cord. Two case reports. Neurochirurgie. 2005;51:476–80. doi: 10.1016/s0028-3770(05)83506-4. [DOI] [PubMed] [Google Scholar]
- 36.Edinger L. Vorlesungen ueber den Bau der nervoesen Centralorgane des Menschen und der Thiere. 5th ed. Leipzig: Verlag von F.C.W, Vogel; 1896. [Google Scholar]
- 37.Estrada V, Brazda N, Schmitz C, Heller S, Blazyca H, Martini R, et al. Long-lasting significant functional improvement in chronic severe spinal cord injury following scar resection and polyethylene glycol implantation. Neurobiol Dis. 2014;67:165–79. doi: 10.1016/j.nbd.2014.03.018. [DOI] [PubMed] [Google Scholar]
- 38.Feringa ER, Kowalski TF, Vahlsing HL. Basal lamina formation at the site of spinal cord transection. Ann Neurol. 1980;8:148–54. doi: 10.1002/ana.410080204. [DOI] [PubMed] [Google Scholar]
- 39.Freeman LW. Return of spinal cord function in mammals after transecting lesions. Ann NY Acad Med Sci. 1954;58:564–9. [Google Scholar]
- 40.Freeman LW. Functional recovery in spinal rats. In: Windle WF, editor. Regeneration in the Central Nervous System. Springfield: Charles C. Thomas; 1955. pp. 195–207. [Google Scholar]
- 41.Freeman LW. Experimental observations upon axonal regeneration in the transected spinal cord of mammals. Clin Neurosurg. 1962;8:294–319. doi: 10.1093/neurosurgery/8.cn_suppl_1.294. [DOI] [PubMed] [Google Scholar]
- 42.Freeman LW Observation on the Regeneration of Spinal Axons in Mammals. Proceedings, X Congreso Latinoamericano de Neurochirurgia. Brazil: Editorial Don Bosco; 1963. pp. 135–44. [Google Scholar]
- 43.Friedli L, Rosenzweig ES, Barraud Q, Schubert M, Dominici N, Awai L, et al. Pronounced species divergence in corticospinal tract reorganization and functional recovery after lateralized spinal cord injury favors primates. Sci Transl Med. 2015;7:302ra134. doi: 10.1126/scitranslmed.aac5811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Garay RP, El-Gewely R, Armstrong JK, Garratty G, Richette P. Antibodies against polyethylene glycol in healthy subjects and in patients treated with PEG-conjugated agents. Expert Opin Drug Deliv. 2012;9:1319–23. doi: 10.1517/17425247.2012.720969. [DOI] [PubMed] [Google Scholar]
- 45.Gill ML, Grahn PJ, Calvert JS, Linde MB, Lavrov IA, Strommen JA, et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat Med. 2018;24:1677–82. doi: 10.1038/s41591-018-0175-7. [DOI] [PubMed] [Google Scholar]
- 46.Goldsmith HS, Fonseca A, Jr, Porter J. Spinal cord separation: MRI evidence of healing after omentum-collagen reconstruction. Neurol Res. 2005;27:115–23. doi: 10.1179/016164105X21995. [DOI] [PubMed] [Google Scholar]
- 47.Guertin PA. Semiquantitative assessment of hindlimb movement recovery without intervention in adult paraplegic mice. Spinal Cord. 2005;43:162–6. doi: 10.1038/sj.sc.3101701. [DOI] [PubMed] [Google Scholar]
- 48.Haggerty AE, Maldonado-Lasunción I, Oudega M. Biomaterials for revascularization and immunomodulation after spinal cord injury. Biomed Mater. 2018;13:044105. doi: 10.1088/1748-605X/aaa9d8. [DOI] [PubMed] [Google Scholar]
- 49.Handa Y, Naito A, Watanabe S, Komatsu S, Shimizu Y. Functional recovery of locomotive behavior in the adult spinal dog. Tohoku J Exp Med. 1986;148:373–84. doi: 10.1620/tjem.148.373. [DOI] [PubMed] [Google Scholar]
- 50.Hardy JG, Lin P, Schmidt CE. Biodegradable hydrogels composed of oxime crosslinked poly(ethylene glycol), hyaluronic acid and collagen: A tunable platform for soft tissue engineering. J Biomater Sci Polym Ed. 2015;26:143–61. doi: 10.1080/09205063.2014.975393. [DOI] [PubMed] [Google Scholar]
- 51.Heimburger RF. Return of function after spinal cord transection. Spinal Cord. 2005;43:438–40. doi: 10.1038/sj.sc.3101748. [DOI] [PubMed] [Google Scholar]
- 52.Heimburger RF. Is there hope for return of function in lower extremities paralyzed by spinal cord injury? J Am Coll Surg. 2006;202:1001–4. doi: 10.1016/j.jamcollsurg.2006.02.022. [DOI] [PubMed] [Google Scholar]
- 53.Hoffman AN, Bamba R, Pollins AC, Thayer WP. Analysis of polyethylene glycol (PEG) fusion in cultured neuroblastoma cells via flow cytometry: Techniques and optimization. J Clin Neurosci. 2017;36:125–8. doi: 10.1016/j.jocn.2016.10.032. [DOI] [PubMed] [Google Scholar]
- 54.Hsieh PC, Stapleton CJ, Moldavskiy P, Koski TR, Ondra SL, Gokaslan ZL, et al. Posterior vertebral column subtraction osteotomy for the treatment of tethered cord syndrome: Review of the literature and clinical outcomes of all cases reported to date. Neurosurg Focus. 2010;29:E6. doi: 10.3171/2010.4.FOCUS1070. [DOI] [PubMed] [Google Scholar]
- 55.Illis LS. Central nervous system regeneration does not occur. Spinal Cord. 2012;50:259–63. doi: 10.1038/sc.2011.132. [DOI] [PubMed] [Google Scholar]
- 56.Imaninezhad M, Pemberton K, Xu F, Kalinowski K, Bera R, Zustiak SP, et al. Directed and enhanced neurite outgrowth following exogenous electrical stimulation on carbon nanotube-hydrogel composites. J Neural Eng. 2018;15:56034. doi: 10.1088/1741-2552/aad65b. [DOI] [PubMed] [Google Scholar]
- 57.Isa T. The brain is needed to cure spinal cord injury. Trends Neurosci. 2017;40:625–36. doi: 10.1016/j.tins.2017.08.002. [DOI] [PubMed] [Google Scholar]
- 58.Iseda T, Nishio T, Kawaguchi S, Yamanoto M, Kawasaki T, Wakisaka S, et al. Spontaneous regeneration of the corticospinal tract after transection in young rats: A key role of reactive astrocytes in making favorable and unfavorable conditions for regeneration. Neuroscience. 2004;126:365–74. doi: 10.1016/j.neuroscience.2004.03.056. [DOI] [PubMed] [Google Scholar]
- 59.Iwatsuki K, Tajima F, Sankai Y, Ohnishi YI, Nakamura T, Ishihara M, et al. Motor evoked potential and voluntary EMG activity after olfactory mucosal autograft transplantation in a case of chronic, complete spinal cord injury: Case report. Spinal Cord Ser Cases. 2016;2:15018. doi: 10.1038/scsandc.2015.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.James ND, McMahon SB, Field-Fote EC, Bradbury EJ. Neuromodulation in the restoration of function after spinal cord injury. Lancet Neurol. 2018;17:905–17. doi: 10.1016/S1474-4422(18)30287-4. [DOI] [PubMed] [Google Scholar]
- 61.Jiang G, Sun J, Ding F. PEG-g-chitosan thermosensitive hydrogel for implant drug delivery: Cytotoxicity in vivo degradation and drug release. J Biomater Sci Polym Ed. 2014;25:241–56. doi: 10.1080/09205063.2013.851542. [DOI] [PubMed] [Google Scholar]
- 62.Kao CC. Spinal cord cavitation after injury. In: Wirile WF, editor. The Spinal Cord and Its Reaction to Traumatic Injury. New York: Marcel Dekker, Inc; 1980. pp. 249–70. [Google Scholar]
- 63.Kerschensteiner M, Schwab ME, Lichtman JW, Misgeld T. In vivo imaging of axonal degeneration and regeneration in the injured spinal cord. Nat Med. 2005;11:572–7. doi: 10.1038/nm1229. [DOI] [PubMed] [Google Scholar]
- 64.Kim CY. PEG-assisted reconstruction of the cervical spinal cord in rats: Effects on motor conduction at 1 h. Spinal Cord. 2016;54:910–2. doi: 10.1038/sc.2016.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kim CY, Sikkema WK, Hwang IK, Oh H, Kim UJ, Lee BH, et al. Spinal cord fusion with PEG-GNRs (TexasPEG): Neurophysiological recovery in 24 hours in rats. Surg Neurol Int. 2016;7:S632–6. doi: 10.4103/2152-7806.190475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kim CY, Oh H, Ren X, Canavero S. Immunohistochemical evidence of axonal regrowth across polyethylene glycol-fused cervical cords in mice. Neural Regen Res. 2017;12:149–50. doi: 10.4103/1673-5374.199014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Kim CY, Sikkema WKA, Kim J, Kim JA, Walter J, Dieter R, et al. Effect of graphene nanoribbons (TexasPEG) on locomotor function recovery in a rat model of lumbar spinal cord transection. Neural Regen Res. 2018;13:1440–6. doi: 10.4103/1673-5374.235301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kishk NA, Gabr H, Hamdy S, Afifi L, Abokresha N, Mahmoud H, et al. Case control series of intrathecal autologous bone marrow mesenchymal stem cell therapy for chronic spinal cord injury. Neurorehabil Neural Repair. 2010;24:702–8. doi: 10.1177/1545968310369801. [DOI] [PubMed] [Google Scholar]
- 69.Knutton S, Pasternak CA. The mechanism of cell-cell fusion. Trends Biochem Sci. 1979;4:220–3. [Google Scholar]
- 70.Kong XB, Tang QY, Chen XY, Tu Y, Sun SZ, Sun ZL, et al. Polyethylene glycol as a promising synthetic material for repair of spinal cord injury. Neural Regen Res. 2017;12:1003–8. doi: 10.4103/1673-5374.208597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kouhzaei S, Rad I, Mousavidoust S, Mobasheri H. Protective effect of low molecular weight polyethylene glycol on the repair of experimentally damaged neural membranes in rat's spinal cord. Neurol Res. 2013;35:415–23. doi: 10.1179/1743132812Y.0000000133. [DOI] [PubMed] [Google Scholar]
- 72.Krause TL, Bittner GD. Rapid morphological fusion of severed myelinated axons by polyethylene glycol. Proc Natl Acad Sci U S A. 1990;87:1471–5. doi: 10.1073/pnas.87.4.1471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lampe KJ, Kern DS, Mahoney MJ, Bjugstad KB. The administration of BDNF and GDNF to the brain via PLGA microparticles patterned within a degradable PEG-based hydrogel: Protein distribution and the glial response. J Biomed Mater Res A. 2011;96:595–607. doi: 10.1002/jbm.a.33011. [DOI] [PubMed] [Google Scholar]
- 74.Lao LF, Zhong GB, Liu ZD. Transection of double-level spinal cord without radiographic abnormalities in an adult: A case report. Orthop Surg. 2013;5:302–4. doi: 10.1111/os.12065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Laverty PH, Leskovar A, Breur GJ, Coates JR, Bergman RL, Widmer WR, et al. Apreliminary study of intravenous surfactants in paraplegic dogs: Polymer therapy in canine clinical SCI. J Neurotrauma. 2004;21:1767–77. doi: 10.1089/neu.2004.21.1767. [DOI] [PubMed] [Google Scholar]
- 76.Lawrence DG, Kuypers HG. The functional organization of the motor system in the monkey. II. The effects of lesions of the descending brain-stem pathways. Brain. 1968;91:15–36. doi: 10.1093/brain/91.1.15. [DOI] [PubMed] [Google Scholar]
- 77.Lee HM, Kim NH, Park CI. Spinal cord injury caused by a stab wound a case report. Yonsei Med J. 1990;31:280–4. doi: 10.3349/ymj.1990.31.3.280. [DOI] [PubMed] [Google Scholar]
- 78.Lee SH, Chung YN, Kim YH, Kim YJ, Park JP, Kwon DK, et al. Effects of human neural stem cell transplantation in canine spinal cord hemisection. Neurol Res. 2009;31:996–1002. doi: 10.1179/174313209X385626. [DOI] [PubMed] [Google Scholar]
- 79.Li X, Yang B, Xiao Z, Zhao Y, Han S, Yin Y, et al. Comparison of subacute and chronic scar tissues after complete spinal cord transection. Exp Neurol. 2018;306:132–7. doi: 10.1016/j.expneurol.2018.05.008. [DOI] [PubMed] [Google Scholar]
- 80.Liu Z, Ren S, Fu K, Wu Q, Wu J, Hou L, et al. Restoration of motor function after operative reconstruction of the acutely transected spinal cord in the canine model. Surgery. 2018;163:976–83. doi: 10.1016/j.surg.2017.10.015. [DOI] [PubMed] [Google Scholar]
- 81.Ren S, Liu Z, Kim CY, Fu K, Wu Q, Hou L, et al. Reconstruction of the spinal cord of spinal transected dogs with polyethylene glycol. Surg Neurol Int. 2019;10:50. doi: 10.25259/SNI-73-2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Lloyd DP. Activity in neurons of the bulbospinal correlation system. J Neurophysiol. 1941;4:115–34. [Google Scholar]
- 82b.Lloyd DP. Mediation of descending long spinal reflex activity. J Neurophysiol. 1942;5:435–58. [Google Scholar]
- 83.Lu X, Perera TH, Aria AB, Callahan LAS. Polyethylene glycol in spinal cord injury repair: A critical review. J Exp Pharmacol. 2018;10:37–49. doi: 10.2147/JEP.S148944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Manzone P, Domenech V, Forlino D. Stab injury of the spinal cord surgically treated. J Spinal Disord. 2001;14:264–7. doi: 10.1097/00002517-200106000-00014. [DOI] [PubMed] [Google Scholar]
- 85.Marzullo TC, Britt JM, Stavisky RC, Bittner GD. Cooling enhances in vitro survival and fusion-repair of severed axons taken from the peripheral and central nervous systems of rats. Neurosci Lett. 2002;327:9–12. doi: 10.1016/s0304-3940(02)00378-6. [DOI] [PubMed] [Google Scholar]
- 86.McMahill BG, Borjesson DL, Sieber-Blum M, Nolta JA, Sturges BK. Stem cells in canine spinal cord injury promise for regenerative therapy in a large animal model of human disease. Stem Cell Rev. 2015;11:180–93. doi: 10.1007/s12015-014-9553-9. [DOI] [PubMed] [Google Scholar]
- 87.Mody GN, Bravo Iñiguez C, Armstrong K, Perez Martinez M, Ferrone M, Bono C, et al. Early surgical outcomes of en bloc resection requiring vertebrectomy for malignancy invading the thoracic spine. Ann Thorac Surg. 2016;101:231–6. doi: 10.1016/j.athoracsur.2015.05.113. [DOI] [PubMed] [Google Scholar]
- 88.Mohrman AE, Farrag M, Grimm RK, Leipzig ND. Evaluation of in situ gelling chitosan-PEG copolymer for use in the spinal cord. J Biomater Appl. 2018;33:435–46. doi: 10.1177/0885328218792824. [DOI] [PubMed] [Google Scholar]
- 89.Mosley MC, Lim HJ, Chen J, Yang YH, Li S, Liu Y, et al. Neurite extension and neuronal differentiation of human induced pluripotent stem cell derived neural stem cells on polyethylene glycol hydrogels containing a continuous young's modulus gradient. J Biomed Mater Res A. 2017;105:824–33. doi: 10.1002/jbm.a.35955. [DOI] [PubMed] [Google Scholar]
- 90.Nakajima N, Ikada Y. Effects of concentration, molecular weight, and exposure time of poly(ethylene glycol) on cell fusion. Polymer J. 1995;27:211–9. [Google Scholar]
- 91.Nardone R, Florea C, Höller Y, Brigo F, Versace V, Lochner P, et al. Rodent, large animal and non-human primate models of spinal cord injury. Zoology (Jena) 2017;123:101–14. doi: 10.1016/j.zool.2017.06.004. [DOI] [PubMed] [Google Scholar]
- 92.Nawrotek K, Marqueste T, Modrzejewska Z, Zarzycki R, Rusak A, Decherchi P, et al. Thermogelling chitosan lactate hydrogel improves functional recovery after a C2 spinal cord hemisection in rat. J Biomed Mater Res A. 2017;105:2004–19. doi: 10.1002/jbm.a.36067. [DOI] [PubMed] [Google Scholar]
- 93.Nehrt A, Hamann K, Ouyang H, Shi R. Polyethylene glycol enhances axolemmal resealing following transection in cultured cells and in ex vivo spinal cord. J Neurotrauma. 2010;27:151–61. doi: 10.1089/neu.2009.0993. [DOI] [PubMed] [Google Scholar]
- 94.Nishio T, Fujiwara H, Kanno I. Immediate elimination of injured white matter tissue achieves a rapid axonal growth across the severed spinal cord in adult rats. Neurosci Res. 2018;131:19–29. doi: 10.1016/j.neures.2017.10.011. [DOI] [PubMed] [Google Scholar]
- 95.Noble LJ, Maxwell DS. Blood-spinal cord barrier response to transection. Exp Neurol. 1983;79:188–99. doi: 10.1016/0014-4886(83)90390-4. [DOI] [PubMed] [Google Scholar]
- 96.Oda Y, Tani K, Isozaki A, Haraguchi T, Itamoto K, Nakazawa H, et al. Effects of polyethylene glycol administration and bone marrow stromal cell transplantation therapy in spinal cord injury mice. J Vet Med Sci. 2014;76:415–21. doi: 10.1292/jvms.13-0167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.O'Lague PH, Huttner SL. Physiological and morphological studies of rat pheochromocytoma cells (PC12) chemically fused and grown in culture. Proc Natl Acad Sci U S A. 1980;77:1701–5. doi: 10.1073/pnas.77.3.1701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Olby NJ, Muguet-Chanoit AC, Lim JH, Davidian M, Mariani CL, Freeman AC, et al. Aplacebo-controlled, prospective, randomized clinical trial of polyethylene glycol and methylprednisolone sodium succinate in dogs with intervertebral disk herniation. J Vet Intern Med. 2016;30:206–14. doi: 10.1111/jvim.13657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Ozawa H, Matsumoto T, Ohashi T, Sato M, Kokubun S. Comparison of spinal cord gray matter and white matter softness: Measurement by pipette aspiration method. J Neurosurg. 2001;95:221–4. doi: 10.3171/spi.2001.95.2.0221. [DOI] [PubMed] [Google Scholar]
- 100.Pasut G, Panisello A, Folch-Puy E, Lopez A, Castro-Benítez C, Calvo M, et al. Polyethylene glycols: An effective strategy for limiting liver ischemia reperfusion injury. World J Gastroenterol. 2016;22:6501–8. doi: 10.3748/wjg.v22.i28.6501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Qiu F, Yang JC, Ma XY, Xu JJ, Yang QL, Zhou X, et al. Relationship between spinal cord volume and spinal cord injury due to spinal shortening. PLoS One. 2015;10:e0127624. doi: 10.1371/journal.pone.0127624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Ramon Y, Cajal S. Degeneration and Regeneration in the Nervous System. New York: Haffner Press; 1928. [Google Scholar]
- 103.Rao YJ, Zhu WX, Du ZQ, Jia CX, Du TX, Zhao QA, et al. Effectiveness of olfactory ensheathing cell transplantation for treatment of spinal cord injury. Genet Mol Res. 2014;13:4124–9. doi: 10.4238/2014.May.30.7. [DOI] [PubMed] [Google Scholar]
- 104.Rao JS, Zhao C, Zhang A, Duan H, Hao P, Wei RH, et al. NT3-chitosan enables de novo regeneration and functional recovery in monkeys after spinal cord injury. Proc Natl Acad Sci U S A. 2018;115:E5595–604. doi: 10.1073/pnas.1804735115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Richter-Turtur M, Krueger P, Wilker D, Angstwurm H. Cervical transverse spinal cord injury caused by knife stab injury. Unfallchirurg. 1990;93:4–5. [PubMed] [Google Scholar]
- 106.Riley DC, Bittner GD, Mikesh M, Cardwell NL, Pollins AC, Ghergherehchi CL, et al. Polyethylene glycol-fused allografts produce rapid behavioral recovery after ablation of sciatic nerve segments. J Neurosci Res. 2015;93:572–83. doi: 10.1002/jnr.23514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Robinson GA, Madison RD. Polyethylene glycol fusion repair prevents reinnervation accuracy in rat peripheral nerve. J Neurosci Res. 2016;94:636–44. doi: 10.1002/jnr.23734. [DOI] [PubMed] [Google Scholar]
- 108.Rodemer W, Selzer ME. Role of axon resealing in retrograde neuronal death and regeneration after spinal cord injury. Neural Regen Res. 2019;14:399–404. doi: 10.4103/1673-5374.245330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Rolls A, Shechter R, Schwartz M. The bright side of the glial scar in CNS repair. Nat Rev Neurosci. 2009;10:235–41. doi: 10.1038/nrn2591. [DOI] [PubMed] [Google Scholar]
- 110.Rosenzweig ES, Brock JH, Lu P, Kumamaru H, Salegio EA, Kadoya K, et al. Restorative effects of human neural stem cell grafts on the primate spinal cord. Nat Med. 2018;24:484–90. doi: 10.1038/nm.4502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Rossignol S, Barrière G, Alluin O, Frigon A. Re-expression of locomotor function after partial spinal cord injury. Physiology (Bethesda) 2009;24:127–39. doi: 10.1152/physiol.00042.2008. [DOI] [PubMed] [Google Scholar]
- 112.Rubin G, Tallman D, Sagan L, Melgar M. An unusual stab wound of the cervical spinal cord: A case report. Spine (Phila Pa 1976) 2001;26:444–7. doi: 10.1097/00007632-200102150-00023. [DOI] [PubMed] [Google Scholar]
- 113.Sahni V, Kessler JA. Stem cell therapies for spinal cord injury. Nat Rev Neurol. 2010;6:363–72. doi: 10.1038/nrneurol.2010.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Salomone R, Jácomo AL, Nascimento SB, Lezirovitz K, Hojaij FC, Costa HJ, et al. Polyethylene glycol fusion associated with antioxidants: A new promise in the treatment of traumatic facial paralysis. Head Neck. 2018;40:1489–97. doi: 10.1002/hed.25122. [DOI] [PubMed] [Google Scholar]
- 115.Sawada M, Kato K, Kunieda T, Mikuni N, Miyamoto S, Onoe H, et al. Function of the nucleus accumbens in motor control during recovery after spinal cord injury. Science. 2015;350:98–101. doi: 10.1126/science.aab3825. [DOI] [PubMed] [Google Scholar]
- 116.Sengupta P. The laboratory rat: Relating its age with human's. Int J Prev Med. 2013;4:624–30. [PMC free article] [PubMed] [Google Scholar]
- 117.Shahlaie K, Chang DJ, Anderson JT. Nonmissile penetrating spinal injury. Case report and review of the literature. J Neurosurg Spine. 2006;4:400–8. doi: 10.3171/spi.2006.4.5.400. [DOI] [PubMed] [Google Scholar]
- 118.Shi R, Borgens RB, Blight AR. Functional reconnection of severed mammalian spinal cord axons with polyethylene glycol. J Neurotrauma. 1999;16:727–38. doi: 10.1089/neu.1999.16.727. [DOI] [PubMed] [Google Scholar]
- 119.Shirres DA. Regeneration of the spinal neurones in man. Montreal Med J. 1905;34:239. [Google Scholar]
- 120.Siddiqui AM, Khazaei M, Fehlings MG. Translating mechanisms of neuroprotection, regeneration, and repair to treatment of spinal cord injury. Prog Brain Res. 2015;218:15–54. doi: 10.1016/bs.pbr.2014.12.007. [DOI] [PubMed] [Google Scholar]
- 121.Sikkema WKA, Metzger AB, Wang T, Tour JM. Physical and electrical characterization of texasPEG: An electrically conductive neuronal scaffold. Surg Neurol Int. 2017;8:84. doi: 10.4103/sni.sni_361_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Sledge J, Graham WA, Westmoreland S, Sejdic E, Miller A, Hoggatt A, et al. Spinal cord injury models in non human primates: Are lesions created by sharp instruments relevant to human injuries? Med Hypotheses. 2013;81:747–8. doi: 10.1016/j.mehy.2013.07.040. [DOI] [PubMed] [Google Scholar]
- 123.Steinberg JA, Wali AR, Martin J, Santiago-Dieppa DR, Gonda D, Taylor W, et al. Spinal shortening for recurrent tethered cord syndrome via a lateral retropleural approach: A Novel operative technique. Cureus. 2017;9:e1632. doi: 10.7759/cureus.1632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Stewart FT, Harte RH. A case of severed spinal cord in which myelorrhaphy was followed by partial return of function. Med J. 1902;9:1016–20. [Google Scholar]
- 125.Tabakow P, Raisman G, Fortuna W, Czyz M, Huber J, Li D, et al. Functional regeneration of supraspinal connections in a patient with transected spinal cord following transplantation of bulbar olfactory ensheathing cells with peripheral nerve bridging. Cell Transplant. 2014;23:1631–55. doi: 10.3727/096368914X685131. [DOI] [PubMed] [Google Scholar]
- 126.Takahashi I, Iwasaki Y, Abumiya T, Imamura H, Houkin K, Saitoh H, et al. Stab wounds of the spinal cord by a kitchen knife: Report of a case. No Shinkei Geka. 1991;19:255–8. [PubMed] [Google Scholar]
- 127.Thornton MA, Mehta MD, Morad TT, Ingraham KL, Khankan RR, Griffis KG, et al. Evidence of axon connectivity across a spinal cord transection in rats treated with epidural stimulation and motor training combined with olfactory ensheathing cell transplantation. Exp Neurol. 2018;309:119–33. doi: 10.1016/j.expneurol.2018.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Todorov AT, Yogev D, Qi P, Fendler JH, Rodziewicz GS. Electric-field-induced reconnection of severed axons. Brain Res. 1992;582:329–34. doi: 10.1016/0006-8993(92)90151-x. [DOI] [PubMed] [Google Scholar]
- 129.Wang A, Huo X, Zhang G, Wang X, Zhang C, Wu C, et al. Effect of DSPE-PEG on compound action potential, injury potential and ion concentration following compression in ex vivo spinal cord. Neurosci Lett. 2016;620:50–6. doi: 10.1016/j.neulet.2016.03.045. [DOI] [PubMed] [Google Scholar]
- 130.Wang A, Zhang G, Xiaochen W, Zhang C, Tao S, Huo X Combination of Applied Electric Field and Polyethylene Glycol Effectively Enhance Functional Recovery in Acute Spinal Cord Injury of Rats. Paper Presented at: 2016 Asia-Pacific International Symposium on Electromagnetic Compatibility (APEMC) 2016:17–21. [Google Scholar]
- 131.Wang GD, Zhai W, Yang HC, Fan RX, Cao X, Zhong L, et al. The genomics of selection in dogs and the parallel evolution between dogs and humans. Nat Commun. 2013;4:1860. doi: 10.1038/ncomms2814. [DOI] [PubMed] [Google Scholar]
- 132.Willyard C. A time to heal. Nature. 2013;503:S4–6. doi: 10.1038/503S4a. [DOI] [PubMed] [Google Scholar]
- 133.Wu GH, Shi HJ, Che MT, Huang MY, Wei QS, Feng B, et al. Recovery of paralyzed limb motor function in canine with complete spinal cord injury following implantation of MSC-derived neural network tissue. Biomaterials. 2018;181:15–34. doi: 10.1016/j.biomaterials.2018.07.010. [DOI] [PubMed] [Google Scholar]
- 134.Xiao Z, Tang F, Tang J, Yang H, Zhao Y, Chen B, et al. One-year clinical study of neuroregen scaffold implantation following scar resection in complete chronic spinal cord injury patients. Sci China Life Sci. 2016;59:647–55. doi: 10.1007/s11427-016-5080-z. [DOI] [PubMed] [Google Scholar]
- 135.Ye Y, Kim CY, Miao Q, Ren X. Fusogen-assisted rapid reconstitution of anatomophysiologic continuity of the transected spinal cord. Surgery. 2016;160:20–5. doi: 10.1016/j.surg.2016.03.023. [DOI] [PubMed] [Google Scholar]
- 136.Yogev D, Todorov AT, Qi P, Fendler JH, Rodziewicz GS. Laser-induced reconnection of severed axons. Biochem Biophys Res Commun. 1991;180:874–80. doi: 10.1016/s0006-291x(05)81146-5. [DOI] [PubMed] [Google Scholar]
- 137.Yoon C, Tuszynski MH. Frontiers of spinal cord and spine repair: Experimental approaches for repair of spinal cord injury. Adv Exp Med Biol. 2012;760:1–5. doi: 10.1007/978-1-4614-4090-1_1. [DOI] [PubMed] [Google Scholar]
- 138.Yoshida Y, Kataoka H, Kanchiku T, Suzuki H, Imajyo Y, Kato H, et al. Transection method for shortening the rat spine and spinal cord. Exp Ther Med. 2013;5:384–8. doi: 10.3892/etm.2012.841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Zhang G, Rodemer W, Lee T, Hu J, Selzer ME. The effect of axon resealing on retrograde neuronal death after spinal cord injury in lamprey. Brain Sci. 2018;8:65. doi: 10.3390/brainsci8040065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Zhang J, Lu X, Feng G, Gu Z, Sun Y, Bao G, et al. Chitosan scaffolds induce human dental pulp stem cells to neural differentiation: Potential roles for spinal cord injury therapy. Cell Tissue Res. 2016;366:129–42. doi: 10.1007/s00441-016-2402-1. [DOI] [PubMed] [Google Scholar]
- 141.Zhang S, Johnston L, Zhang Z, Ma Y, Hu Y, Wang J, et al. Restoration of stepping-forward and ambulatory function in patients with paraplegia: Rerouting of vascularized intercostal nerves to lumbar nerve roots using selected interfascicular anastomosis. Surg Technol Int. 2003;11:244–8. [PubMed] [Google Scholar]
- 142.Zholudeva LV, Qiang L, Marchenko V, Dougherty KJ, Sakiyama-Elbert SE, Lane MA, et al. The aneuroplastic and therapeutic potential of spinal interneurons in the injured spinal cord. Trends Neurosci. 2018;41:625–39. doi: 10.1016/j.tins.2018.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]