

Abstract
Cooperation with multiple departments is essential for the treatment of patients with rectal cancer and other pelvic cancers. In our department, we experienced two cases of rectal cancer that underwent robotic low anterior resection (LAR) and simultaneous resection of other pelvic organs (case 1 with prostatectomy and case 2 with hysterectomy) using the da Vinci Xi system. Here, we show the precise procedures of these two robotic surgeries. Under general anesthesia and lithotomy position, five da Vinci ports were symmetrically placed along the umbilical horizontal line with a 7 cm interval, and a 5 mm AirSeal Access Port was added in the right or left upper quadrant. Patients were placed with 22-degree Trendelenburg and 8-degree tilt to the right. The operators used the center port on the umbilicus as a camera port and chose the docking arms with either two-left-one-right or one-left-two-right setting depending on their preference. This port setting was quite useful for the operators from multiple departments to change the docking arms, even if their preference may be different. Moreover, assistants could use the remaining two ports to provide a well-expanded and safer surgical field. “With a familiar view” and “with a wide view” are our two concepts to safely perform extended pelvic surgeries. We have employed this symmetrical horizontal port site position as a general setting for usual rectal surgeries.
Electronic supplementary material
The online version of this article (10.1007/s13691-019-00377-3) contains supplementary material, which is available to authorized users.
Keywords: Robot-assisted surgery, Simultaneous resection, Rectal cancer, Prostatectomy, Hysterectomy
Introduction
As a minimally invasive surgery for rectal cancer, laparoscopic surgery has become the standard strategy for early and advanced rectal cancers [1]. Compared with conventional laparoscopic surgery, robot-assisted surgery is considered to have some advantages including three-dimensional vision, jointed wrist manipulation, tremor reduction, and motion scaling. Although there is little evidence of oncological superiority, robot-assisted rectal surgery can result in favorable short-term outcomes such as less blood loss and shorter postoperative hospital stay [2–4]. However, it has not yet become a standard option for rectal cancer.
We often encounter patients with multiple diseases. Likewise, rectal cancer patients sometimes have other types of cancers that need to be resected. In such cases, simultaneous combined resection is needed, and a minimally invasive approach such as robot-assisted surgery is especially useful to decrease the surgical stress caused by the simultaneous combined resection.
Here, we present two cases of rectal cancer patients who underwent simultaneous resection of pelvic organs in addition to low anterior resection (LAR) using the da Vinci Xi system (Intuitive Surgical, Sunnyvale, CA).
Case presentation
Case 1
A 67-year-old man presented to the department of urology at our hospital with elevated prostate-specific antigen (PSA) level. Transrectal ultrasound-guided prostate biopsy revealed an acinar adenocarcinoma with a Gleason score of 4 + 5 = 9. Preoperative computed tomography (CT) incidentally identified the thickening of the rectal wall (Fig. 1a). Colonoscopy revealed a rectal tumor 10 cm above the anal verge, occupying over half of the rectal lumen (Fig. 1b). Pathological examination of the rectal tumor indicated a well differentiated tubular adenocarcinoma. There was no distant metastasis suspected from either prostate or rectal cancer. To achieve curative resection of both prostate and rectal cancers, robot-assisted simultaneous surgery of LAR and radical prostatectomy was conducted.
Fig. 1.

Preoperative images of case 1. a Enhanced abdominal CT images showed wall thickening on the left side of the rectum. b Colonoscopy showed type 2 tumors 10 cm above the anal verge, from which a well differentiated tubular adenocarcinoma was detected
Case 2
A 50-year-old woman presented to our hospital with positive fecal occult blood. Colonoscopy revealed a rectal tumor 4 cm above the anal verge, occupying the posterior wall of the rectum (Fig. 2a). Pathological examination indicated a moderately differentiated tubular adenocarcinoma. Although there was no evidence of distant metastasis, the most important problem in this case was the enlarged uterus with many hysteromyomas as large as 11 × 11 × 11 cm in size (Fig. 2b). To achieve curative resection of rectal cancer safely, robot-assisted simultaneous surgery of intersphincteric resection (ISR) and a hysterectomy with bilateral salpingo-oophorectomy (HBSO) were conducted.
Fig. 2.

Preoperative images of case 2. a Colonoscopy revealed type 2 tumors on the posterior wall of the rectum 4 cm above the anal verge, from which a moderately differentiated tubular adenocarcinoma was detected. b Magnetic resonance imaging demonstrated an enlarged uterus with multiple hysteromyomas
Technique
Robot-assisted surgeries were performed using the da Vinci Xi system. The port site position we generally employ is described in Fig. 3. Under general anesthesia, the patients were placed in a lithotomy position. We first checked the position of the promontorium by palpation and decided the position of the first camera port as 5 cm above it, which is close to the umbilicus in most cases. A 3 cm longitudinal incision was placed on the umbilicus, and Lap Protector (Hakko, Nagano, Japan) and E-Z Access (Hakko) were inserted there. The first da Vinci 8-mm port was inserted through the E-Z Access at the decided camera port position, and pneumoperitoneum was started. By inserting the camera port through the E-Z Access, the operators can move its position a little during surgery if necessary, because promontorium sometimes prevents the camera scope to enter into the deep pelvis. A total of five da Vinci trocars were inserted symmetrically along the horizontal line of the first port with about 7 cm intervals. Next, a 5-mm AirSeal Access Port (ConMed, Utica, NY) was added in the right or left upper quadrant of the abdomen (Fig. 3). Then the patients were placed with 22-degree Trendelenburg and 8-degree tilt to the right, and the patient cart of da Vinci Xi was positioned at the left side of the patient.
Fig. 3.
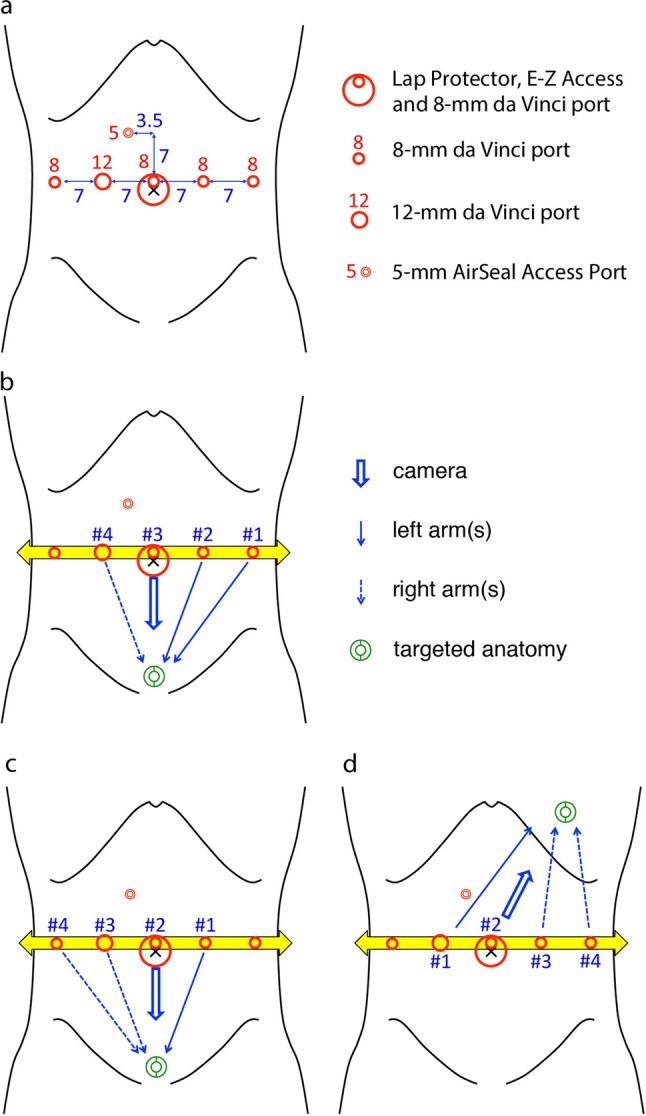
Port site position we generally employ for rectal surgery. a Five da Vinci ports are placed on an umbilical horizontal line symmetrically with about 7 cm interval. A 5-mm AirSeal Access Port is placed on right or left upper quadrant. b, c Using the symmetrical horizontal port site setting, operators can choose either two-left-one-right (b) or one-left-two-right (c) arms during pelvic surgery. d Splenic flexure can be mobilized by rotating the arm overhead 180-degree and re-targeting
During the LAR procedure, four arms of the patient cart were connected as shown in Fig. 3b, and an assistant sat at the right side of the patients. For the prostatectomy or hysterectomy, the arms were connected as shown in Fig. 3c. Splenic flexure was mobilized at the arm position shown in Fig. 3d (180-degree rotated) if necessary. In this symmetrical horizontal port site setting, operators can choose either two-left-one-right or one-left-two-right according to their preference (Fig. 4).
Fig. 4.
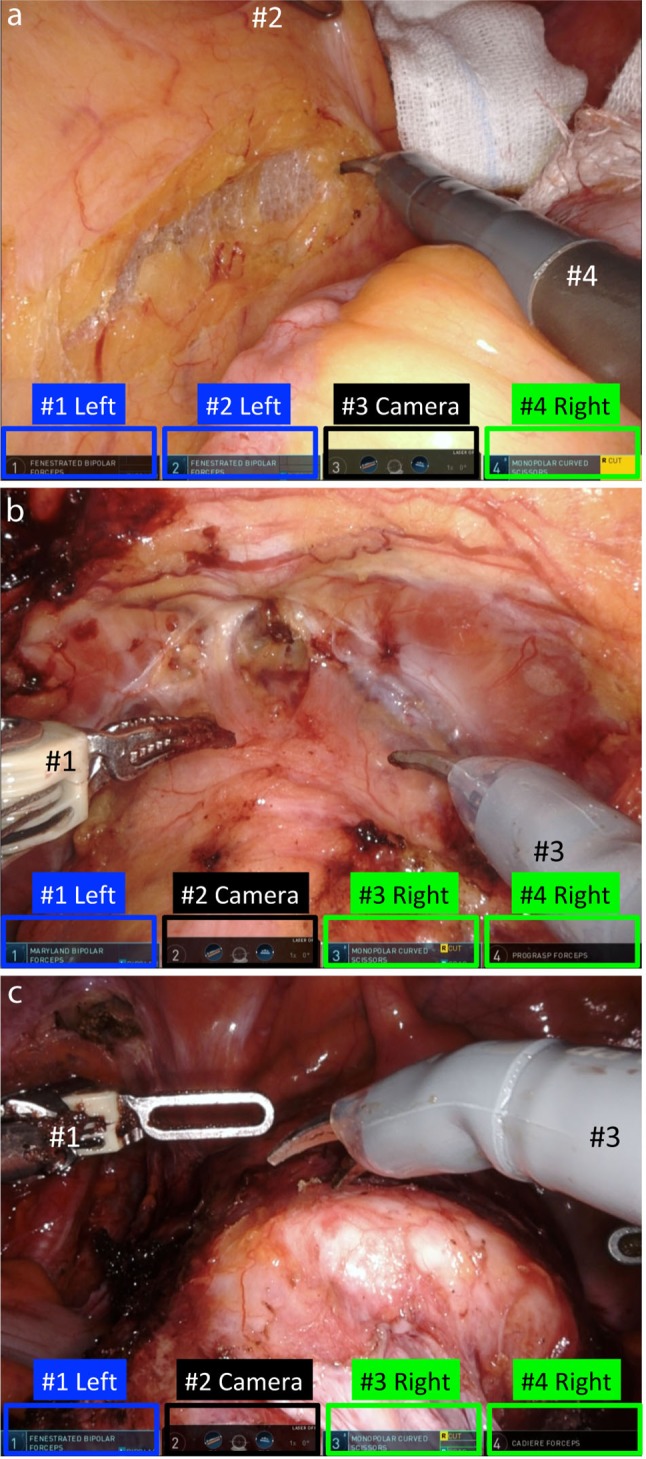
Representative pictures of robot-assisted pelvic surgery. Rectal surgery (a) with two-left-one-right arm setting, and prostatectomy (b) and HBSO (c) with one-left-two-right setting
Precise procedures for robot-assisted radical prostatectomy and HBSO were reported elsewhere [5, 6]. In case 1, division of the inferior mesenteric artery and mobilization of the left side colon were performed first. A transabdominal approach for total mesorectal excision (TME) was continued until the arms reached the pelvic floor. After reaching the pelvic floor, the mesorectum was dissected as a tumor-specific mesorectal excision (TSME), followed by the division of the rectum with EndoWrist Staplers (two 45-mm Blue). Then the mesocolon of the proximal side was divided, the specimen was removed from the umbilical incision, and an end-to-end anastomosis with double-stapling technique (29-mm ECS, Ethicon, Tokyo, Japan) was performed. Prostatectomy was done after LAR, and the prostate was removed from the umbilical incision. In case 2, HBSO was initiated prior to ISR, and uterus and ovaries were removed transvaginally. After TME, the mesocolon at the proximal side was first dissected, and ISR via transanal approach was performed for the appropriate safety margin of the distal side. The surgical specimen was taken out from the anus, and vertical mattress suture was performed with absorbable monofilament strings circumferentially for anastomosis.
Result
In case 1, the total operative time was 640 min (240 for prostatectomy and 400 for LAR) and total blood loss was 510 ml including urine. In case 2, the total operative time was 503 min (146 for HBSO and 357 for ISR) and total blood loss was 57 ml. The rectal cancer staging of case 1 was Stage IIIB (pT4aN1bM0 according to the 8th edition UICC) with negative CRM, and that of case 2 was Stage IIIA (pT2N1aM0) with negative CRM.
Discussion
Laparoscopic surgery for rectal cancer is widely accepted, but it is sometimes technically challenging, especially in the cases of very low tumor location, narrow and deep male pelvis, and/or visceral obesity. Furthermore, additional tumors in other pelvic organs make it more complicated to plan surgical strategies. Therefore, there is no standard procedure for combined resection of other pelvic organs under robotic surgery. For safe pelvic surgeries, it is inevitable to prepare for familiar settings such as port site positioning and surgical devices. In most cases, combined resection of multiple pelvic organs requires the operators to change among colorectal surgeons, urologists and gynecologists, whose preference may also be different. In such cases, robot-assisted surgery brings a great benefit to overcome such problem. The symmetrical horizontal port site position for the da Vinci Xi system described in Fig. 3 with EndoWrist manipulation enables us, all the pelvic surgeons, to reach almost at the deepest pelvic floor with familiar view. More importantly, we can choose either two-left-one-right or one-left-two-right arm setting by switching the connection of the da Vinci Xi arms with the ports depending on their preference. We employ this port site setting as a standard one for all the rectal surgeries for rectal cancer.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (MPG 389607 kb)
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants and/or animals
For this type of study, formal consent is not required.
Informed consent
Written informed consent was obtained from both patients for publication of this case report. Copies of the documents are available for review by the Editor-in-Chief of the journal.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Kim CW, Kim CH, Baik SH. Outcomes of robotic-assisted colorectal surgery compared with laparoscopic and open surgery: a systematic review. J Gastrointest Surg. 2014;18(4):816–830. doi: 10.1007/s11605-014-2469-5. [DOI] [PubMed] [Google Scholar]
- 2.Yamaguchi T, Kinugasa Y, Shiomi A, Kagawa H, Yamakawa Y, Furutani A, Manabe S, Yamaoka Y, Hino H. Oncological outcomes of robotic-assisted laparoscopic versus open lateral lymph node dissection for locally advanced low rectal cancer. Surg Endosc. 2018;32(11):4498–4505. doi: 10.1007/s00464-018-6197-x. [DOI] [PubMed] [Google Scholar]
- 3.Shiomi A, Kinugasa Y, Yamaguchi T, Kagawa H, Yamakawa Y. Robot-assisted versus laparoscopic surgery for lower rectal cancer: the impact of visceral obesity on surgical outcomes. Int J Colorectal Dis. 2016;31(10):1701–1710. doi: 10.1007/s00384-016-2653-z. [DOI] [PubMed] [Google Scholar]
- 4.Yamaguchi T, Kinugasa Y, Shiomi A, Tomioka H, Kagawa H, Yamakawa Y. Robotic-assisted vs. conventional laparoscopic surgery for rectal cancer: short-term outcomes at a single center. Surg Today. 2016;46(8):957–962. doi: 10.1007/s00595-015-1266-4. [DOI] [PubMed] [Google Scholar]
- 5.Menon M, Tewari A. Robotic radical prostatectomy and the Vattikuti Urology Institute technique: an interim analysis of results and technical points. Urology. 2003;61(4 Suppl 1):15–20. doi: 10.1016/S0090-4295(03)00116-X. [DOI] [PubMed] [Google Scholar]
- 6.Mandai M. Application of robot-assisted surgery in nerve-sparing radical hysterectomy for uterine cervical cancer. Acta Med Kinki Univ. 2013;38(1):1–5. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material 1 (MPG 389607 kb)