

Abstract
Background:
Intraoperative identification of the correct level during thoracic spine surgery is essential to avoid wrong-level procedures. Despite technological progress, intraoperative imaging modalities for identifying the correct thoracic spine level remain unreliable and often lead to wrong-level surgery. To counter potential wrong-level operations, here, we have proposed a novel pedicle/bone cylinder marking technique for use in the thoracic spine utilizing biplanar fluoroscopy and confirmed with computed tomography (CT).
Methods:
First, under fluoroscopic guidance, a bone cylinder is removed from the correct thoracic pedicle. Next, endovascular coils are packed into the cancellous bone defect followed by reinsertion of the bony plug. The patient then undergoes a CT scan of the entire thoracolumbosacral spine to precisely identify the marked level before surgery.
Results:
We utilized this bone cylinder plug/coil technique to identify the T9-T10 level in a 56-year-old female with a soft thoracic disc herniation. The index thoracic pedicle was successfully localized before performing the unilateral minimally invasive laminectomy followed by the transpedicular thoracic disc excision.
Conclusion:
The bone cylinder plug/coil technique is a safe and effective method for marking the correct level in thoracic spine surgery, while also reducing the operative time.
Keywords: Disc herniation, Interventional radiology, Intervertebral disc, Surgical discectomy, Thoracic spine, Thoracic vertebrae

INTRODUCTION
Wrong-level thoracic surgery occurs up to 15% of the time. Here, we describe a novel bone cylinder plug/coil technique utilizing endovascular coils to correctly localize thoracic pedicles before thoracic spine surgery. Wrong-level thoracic surgery is typically directly linked to misinterpretation of radiographic images (e.g., low image quality from interposing bones/shoulder), obesity, anatomical variants (e.g., accessory ribs), and skin markers/retractors that can move. Although more sophisticated computed tomography (CT) and/or magnetic resonance imaging (MRI)-based navigation modalities have enhanced the accuracy of thoracic surgery, they are not always widely available, leaving spinal surgeons to rely on intraoperative X-rays or fluoroscopy.[6]
CASE REPORT
Over 10 months, a 56-year-old female presented with progressive left lower extremity weakness and imbalance. The neurological examination revealed thoracic myelopathy (Nurick I) with a T8 sensory level. MRI and CT studies both documented a T9-10 soft herniated disc occupying 30% of the left side of the spinal canal resulting in significant spinal cord compression [Figure 1a and b].
Thoracic pedicle marking using endovascular coils
Prone, and under local anesthesia with sedation, the index level is identified using biplanar fluoroscopy. A sterile skin marker and puncture are then performed over the correct level. The local paraspinal muscles and subperiosteal space are then infiltrated with 10 ml of 1% lidocaine. An 11-gauge, 125 mm long trocar is then inserted into the posterior pedicle [Figure 1c]. A 13-gauge trepan/trephine is then introduced at a 5 mm depth into the middle portion of the pedicle, allowing for the removal of a cylindrical fragment including both cortical and cancellous bone [Figure 1d]. Two embolization microcoils measuring 2–4 mm are next inserted into the bone defect and secured in place with the bone cylindrical fragment [Figure 1e and f]. Accurate positioning of the metallic coils is then verified utilizing both biplanar fluoroscopy and CT guidance [Figure 2].
Figure 1:
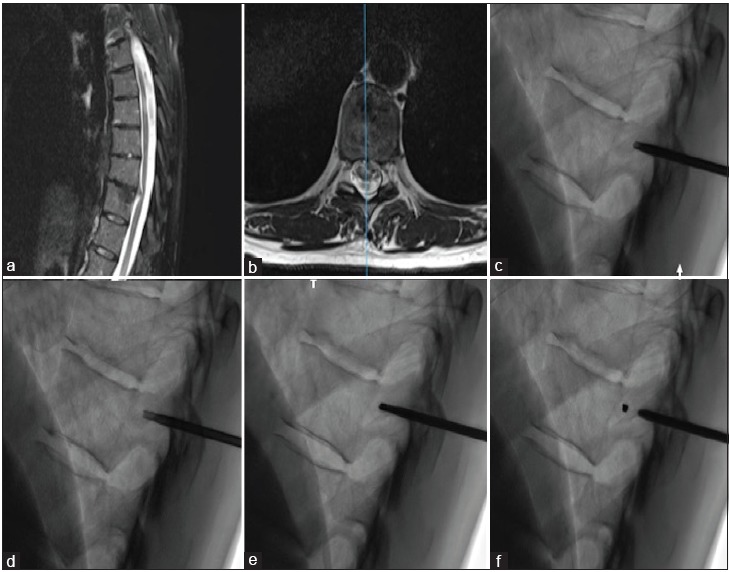
Fiducial placement procedure. Preoperative sagittal (Panel a) and axial (Panel b) T2-weighted magnetic resonance imaging of the thoracic spine showing a left thoracic disc herniation at T10-T11 in 56-year-old women resulting in spinal cord compression and myelopathy. The patient underwent preoperative pedicle marking under fluoroscopic guidance. Panel c: At the level of the index pedicle, an 11-gauge, 125 mm long trocar is inserted. Panel d: Retrieval of bony fragment with a 13-gauge trepan in the middle portion of the pedicle. Panel e: Two microcoils inserted into the bony defect. Panel f: Reinsertion of the bone cylinder in the defect to lock the fiducial in the pedicle.
Figure 2:
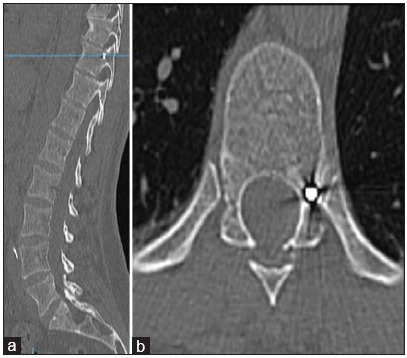
Preoperative computed tomography scan of the thoracic spine including the sacrum. Sagittal (Panel a) and axial (Panel b) computed tomography scan confirming the placement of the coils at the level of the left T10 pedicle.
Surgery and outcome
The patient successfully underwent a unilateral laminectomy, with minimally invasive transpedicular thoracic disc excision. Postoperatively, she demonstrated marked neurological improvement (e.g., Nurick I residual mild myelopathy), while the postoperative MR documented adequate disc excision/decompression.
DISCUSSION
Factors leading to wrong-level thoracic surgery have included spinous process dye infusion/cutaneous marking (e.g., risk of widespread diffusion), movement/shift of the skin marker (e.g., obesity, severe scoliosis, and heavy skin folding), and spine hypermobility.[7] There are currently several options to avoid such wrong-level surgery, and these include skin marking with biplane fluoroscopy, CT-guided transpleural needle localization, vascular coils (e.g., in the segmental artery or the pedicle), cement (PMMA), pedicle screws, and metallic fiducials.[1-7] Other methods like cement placed into the vertebral bodies risk extravasation are more costly and more time consuming.[1-4] Pedicle screw placement may interfere with retractor placement during minimally invasive procedures. Percutaneous placement of other markers such as coils or clips into the vertebral pedicle has been shown to be accurate.
Proposed “Plug and Coil” technique
Our technique consisted of removing a cylindric bone fragment from the pedicle and its replacement. After coil application, this procedure locks the coils in place and minimizes the risk of coil migration. It differs from those described by Madaelil et al.[4] and Binning and Schmidt,[1] in which the authors did not secure the intraosseous markers inside the pedicles, thus increasing the risk of marker migration. Macki et al. also secured a gold fiducial, but as they only utilized bone wax, it was not secure/unreliable.[3]
CONCLUSION
Preoperative pedicle marking using bone plug removal, the application of endovascular coils within the pedicle, followed by reapplication of the bone plug appears to be a safe and effective procedure for the correct preoperative localization of thoracic spinal surgical levels. Further, experience is needed to confirm these findings.
Contributor Information
Rodolfo Maduri, Email: rodolfo.maduri@gmail.com.
Daniele Starnoni, Email: daniele.starnoni@chuv.ch.
Juan Barges-Coll, Email: juan.barges-coll@chuv.ch.
Steven David Hajdu, Email: steven.hajdu@chuv.ch.
John Michael Duff, Email: johnmichael.duff@gmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Binning MJ, Schmidt MH. Percutaneous placement of radiopaque markers at the pedicle of interest for preoperative localization of thoracic spine level. Spine (Phila Pa 1976) 2010;35:1821–5. doi: 10.1097/BRS.0b013e3181c90bdf. [DOI] [PubMed] [Google Scholar]
- 2.Chin KR, Seale J, Cumming V. Avoidance of wrong-level thoracic spine surgery using sterile spinal needles: A Technical report. Clin Spine Surg. 2017;30:E54–E58. doi: 10.1097/BSD.0b013e3182a35762. [DOI] [PubMed] [Google Scholar]
- 3.Macki M, Bydon M, McGovern K, Abt N, de la Garza-Ramos R, Naff N, et al. Gold fiducials are a unique marker for localization in the thoracic spine: A cost comparison with percutaneous vertebroplasty. Neurol Res. 2014;36:925–7. doi: 10.1179/1743132814Y.0000000413. [DOI] [PubMed] [Google Scholar]
- 4.Madaelil TP, Long JR, Wallace AN, Baker JC, Ray WZ, Santiago P, et al. Preoperative fiducial marker placement in the thoracic spine: A Technical report. Spine (Phila Pa 1976) 2017;42:E624–8. doi: 10.1097/BRS.0000000000001890. [DOI] [PubMed] [Google Scholar]
- 5.Marquardt G, Berkefeld J, Seifert V, Gerlach R. Preoperative coil marking to facilitate intraoperative localization of spinal dural arteriovenous fistulas. Eur Spine J. 2009;18:1117–20. doi: 10.1007/s00586-009-0946-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nowitzke A, Wood M, Cooney K. Improving accuracy and reducing errors in spinal surgery a new technique for thoracolumbar-level localization using computer-assisted image guidance. Spine J. 2008;8:597–604. doi: 10.1016/j.spinee.2007.06.005. [DOI] [PubMed] [Google Scholar]
- 7.Upadhyaya CD, Wu JC, Chin CT, Balamurali G, Mummaneni PV. Avoidance of wrong-level thoracic spine surgery: Intraoperative localization with preoperative percutaneous fiducial screw placement. J Neurosurg Spine. 2012;16:280–4. doi: 10.3171/2011.3.SPINE10445. [DOI] [PubMed] [Google Scholar]