

Abstract
Background:
In the present study, we evaluate the results of gamma knife surgery (GKS) for the treatment of trigeminal neuralgia (TN) using the trigeminal ganglion (TG’) and the adjacent fibers of trigeminal nerve as a target.
Methods:
From February 2013 to July 2017, we treated 30 cases of TN with GKS. In this group, all patients had an idiopathic typical TN. The radiosurgical target was conformed through two isocenters, 8 and 4 mm at the cavum de Meckel. The maximum dose was 86 Gy using the isodose line of 50%. The median age of the patients was 58.5 (range 28–94) years old, and the median time from diagnosis to GKS was 94 months (range 13–480 months). The median follow-up was 28.5 (range 12–49) months. Clinical outcomes were analyzed. Univariate and multivariate analyses were performed to evaluate factors that correlated with a favorable, pain-free outcome.
Results:
The mean time to relief of pain was 7 (range 1–40) days. The percentage of patients with significant pain relief was 93.3%. Relapse in pain was noted in four patients at 3, 16, 19, and 36 months. Nine patients were treated in acute status. Fourteen patients had intense pain between 1 and 7 days before the procedure. Among those with the recurrence of their symptoms, one patient had a microvascular decompression. Multivariate regression adjusted for age and sex suggests that, by 40 months, 70% of the patients treated with radiosurgery will remain pain free. At the last follow-up, GKS resulted in pain relief in 86.6% of patients. Our analysis suggests that, using this technique, we can expect that approximately 70% of patients with TN will have some degree of pain improvement at 3 years’ post radiosurgery.
Conclusions:
GKS on TG appears to be a reasonable treatment option with short latency period, minor collateral effects, and high percentage of pain control. The mechanism of action of radiosurgery could be related to the inactivation of the satellite glial cells in the TG.
Keywords: Facial pain, Gamma knife, Gasser ganglion, Radiosurgery, Satellite glial cells, Trigeminal ganglion, Trigeminal neuralgia
INTRODUCTION
Trigeminal neuralgia (TN) is clinically characterized by severe paroxysmal facial pain and brief, sharp, or stabbing unilateral electric shock-like sensations often triggered by facial movements or cutaneous stimulation.[7,41,49]
Although many reports have documented the efficacy of radiosurgery in the treatment of TN, controversy remains regarding the optimal treatment dose, target site, and brainstem dose.[7,19,41,49]
In 1971, Leksell[21] presented two cases of typical TN treated with stereotactic radiosurgery (SRS). The trigeminal ganglion (TG) and the adjacent root fibers were the targets. Complete relief was obtained without any loss of sensation in the face and patients remained pain free for 18 years.
In 2014, we reported[44] a case of a patient with TN secondary to vertebrobasilar ectasia. We treated the TG to relieve the painful condition because the trigeminal nerve could not be properly visualized on neuroimaging studies. Three days after the procedure, the intensity of the pain had diminished, and 15 days after the procedure, the patient was pain free. During 48 months of follow-up, the patient has remained without pain and without any kind of alteration in facial sensation.
Due to the excellent results obtained, we decided to prospectively evaluate the technique in 30 patients with idiopathic TN. The results are presented and discussed.
METHODS
Patient population
Between February 2013 and July 2017, a prospective study was conducted to analyze the responses of 30 consecutive patients with typical TN refractory to therapy that treated with gamma knife surgery (GKS) at the gamma knife center las mercedes (CDD) in Caracas, Venezuela. The median age of the patients was 58.5 years (range, 28–94 years) and the mean duration pain was 94 months (range, 13–480 months.). In the distribution of pain, a combination of branches was more frequently involved in all patients. The right side of the face was more frequently involved (71.8%). Numbness was noted in nine patients (28.1%), eight of which had previous local or invasive therapeutic procedures.
All patients received pharmacotherapy which included gabapentin, pregabalin, carbamazepine, and combinations. Ten patients had a history of previous surgical intervention, including local blocks of trigeminal branches (n = 8), cryotherapy (n = 2), radiofrequency (n = 4), peripheral neurectomy (n = 3), maxillofacial surgeries (n = 5), balloon compression (n = 1), and previous radiosurgery (n = 1). No patients had anesthesia Dolorosa. Clinical characteristics are shown in Table 1.
Table 1:
Clinical characteristics of 30 patients with TN who underwent gamma knife radiosurgery on the trigeminal ganglion.
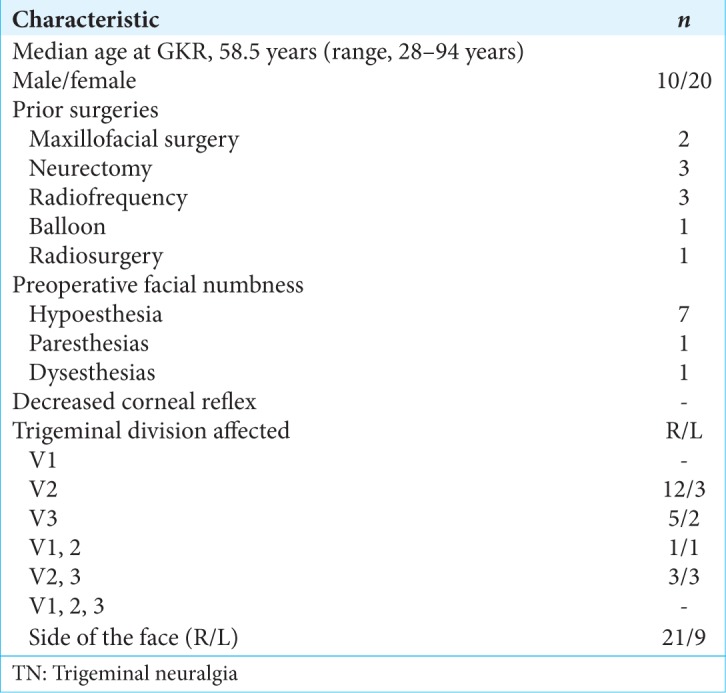
Associated pathologies were arterial hypertension (n = 17), obesity (n = 2), diabetes mellitus (n = 1), hypothyroidism (n = 1), and hemochromatosis (n = 1).
As part of our protocol for TN radiosurgery, all patients underwent clinical examination and neuroimaging with computed tomography (CT) or magnetic resonance imaging (MRI) to exclude other pathologies that could produce TN (tumors, compression by the complex of vertebrobasilar arteries and other vascular malformations, and multiple sclerosis). All patients fulfilled the criteria of the International Headache Society and had a TN1.
Criteria for using GKS
The decision to use GKS was based on criteria such as the medical condition of the patients, pain refractory to pharmacologic treatment, significant adverse effects from medication, previous unsuccessful surgical procedures, the absence of vascular or tumor compression of the involved trigeminal nerve on the MR images, and the patients’ willingness to undergo radiosurgery instead of other techniques.
Radiosurgical technique
All patients underwent SRS using a gamma knife (Leksell Gamma Knife, Elekta Instruments, Atlanta, Ga), model C. Under mild sedation and local anesthesia, the Leksell Model G stereotactic frame (Elekta Instruments) was applied. Stereotactic MRI was performed on each patient to identify the trigeminal nerve and its course from the pons, using contrast enhancement. A three-dimensional time-of-flight (3D-TOF) sequence was performed using a 1.5-Tesla MRI scanner (General Electric Signa HD). Fast imaging, employing steady-state acquisition sequence, provides images included in the MR protocol. A treatment plan was implemented using the Leksell Gamma Plan treatment planning system (Elekta AB).
Stereotactic coordinates were calculated for two isocenters; one 8-mm isocenter was placed on the Meckel’s Cavum and a 4 mm was placed at the adjacent fibers of the trigeminal nerve from the TG. The maximum dose was 86 Gy (43 Gy prescribed to the 50% isodose) [Figure 1].
Figure 1:

Axial, coronal and saggital T1 weighted images after gadolinium. Right trigeminal ganglion and exit zone of trigeminal nerve from the ganglion are visualized.
Patient outcomes and follow-up evaluation
All patients were discharged the same day after radiosurgery. They were instructed to continue their preoperative medications after the radiosurgical procedure and to gradually taper their medications over 16-week intervals.
The primary outcome after radiosurgery was based on pain intensity which was defined and assessed using the barrow neurological institute (BNI) pain intensity scoring criteria. The mean follow-up time after radiosurgery was 28.5 months (range, 12–49 months). An assessment of outcomes was performed by a blinded evaluator, trained to complete telephone follow-ups and clinical examinations as part of our protocol. It was then followed by a clinical consultation in our center, every 4 months; all of which allowed to keep updated patients’ records. Clinical evaluation included facial sensory testing, corneal reflex, and jaw motility. We evaluated the degree of pain relief, latency interval to pain relief, drugs used, development of new signs or symptoms, and the need for and response to additional surgical procedures.
Statistical analysis
Categorical variables were compared through Chi-square testing. For continuous variables, Student’s t-test was used for normally distributed variables (e.g., age); Kruskal–Wallis tests were used for non normally distributed variables (e.g., length of stay). P < 0.05 was considered to be statistically significant. Cox proportional regression was used to generate a predicted pain-free survival curve, adjusting for age and sex of patients. All statistical analyses were performed in SAS 9.4 (SAS Institute Inc., Cary, NC).
RESULTS
Clinical response
Before undergoing GKS, all patients categorized their pain as BNI IV or V. The BNI pain score at baseline and last follow-up is shown in Table 2. Criteria for improvement included a reduction in the frequency and severity of TN attacks. Treatment failure was defined as no response or slight improvement.
Table 2:
Pain outcome before and after SRS.
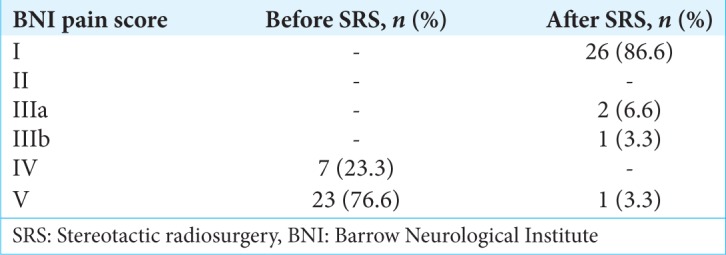
The mean latency period was 7 days (range, 1–40 days); all patients were pain free. The initial response rate in the patients was 100%, including patients with previous local and ablative procedures. In 18 patients (60%), pain relief was obtained before 8 days.
At last follow-up, significant pain relief was noted by 86.6% of patients (good plus excellent results). Relapse in pain was noted in four patients at 3, 16, 19, and 36 months. In two of them, the pain was similar to the pain before the radiosurgery procedure. One patient returned to the pain-free state with medication; although his pain presents occasionally, it is not as intense as previously recorded. One patient decided to undergo surgery; therefore, the case was considered a treatment failure.
Univariate analysis did not identify any factors associated with pain-free survival. Figure 2 shows a 40-month predicted pain-free survival of 70%.
Figure 2:
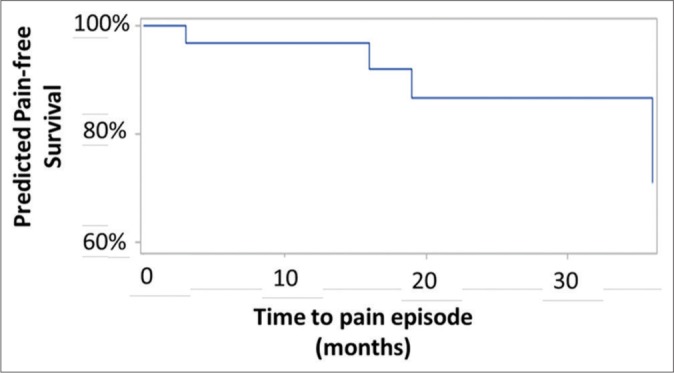
Predicted pain-free survival after gamma knife radiosurgery on the trigeminal ganglion for idiopathic trigeminal neuralgia.
Of the 30 patients, seven patients continue under medication at the last follow-up. One of them, an 83-year-old patient suffering from TN for 19 years, does not want to leave the medication even in the absence of pain.
Nine patients were treated in acute status, with pain the same day of the procedure and between 1 and 10 days before the procedure in 21 patients.
Regarding the adverse effects of radiosurgery, one patient reported moderate hypoesthesia in all three divisions, two patients had tickling sensations, and one patient reported hypoesthesia in V2, although in this case, the patient presented dysesthesias in the same region before treatment with radiosurgery.
DISCUSSION
Historical background
Radiosurgery has become an excellent treatment choice for patients who do not respond to medical therapy or other surgical procedures. In the management of the typical TN, most patients are suitable candidates for GKS which was demonstrated to be an effective and safe option.[7,19,41,43,49]
The concept of SRS was introduced by Lars Leksell, who in 1951 began performing clinical radiosurgery with a stereotactic X-ray beam in patients with essential TN. Leksell was the first to use radiosurgery for the treatment of functional disorders such as TN. Using a conventional stereotactic frame, he directed the radiation beam produced by an orthovoltage X-ray tube at the TG.[21]
After treating a series of 40 patients, the Leksell team abandoned this approach because Leksell discovered the efficacy of the glycerol injection. This injection was first used for the visualization of the Meckel cave but turned out to be sufficient to stop the pain in a significant percentage of patients.[13] However, in 1971, Leksell presented the analysis of the first two patients with TN treated using SRS. The target was the TG and the adjacent root fibers. The first patient with a classic TN was treated on April 20, 1953, when a “stereotaxic radiogangliotomy” was performed. The patient continued having frequent attacks of neuralgia for 15 days and the number of episodes diminished over 5 months until they disappeared. Neurological examination revealed no numbness or loss of sensation with normal corneal reflexes. A second patient with typical TN was treated on June 2, 1953. In this case, the patient noted a marked improvement the day after treatment but continued having attacks of pain for a few days and occasional pricking sensations. Both patients remained free of pain during a follow-up period of 18 years with a normal neurological examination. Leksell established that no definite conclusions could be made in relation to the optimal dose of radiation, the exact mechanism of action, and the site of action (the root or ganglion); however, it was clear that the pain disappeared permanently without a facial sensory loss.[21]
Lindquist et al.[22] reported, in 1991, the results obtained in the management of TN in 46 patients, using the TG as the radiosurgical target. Their results were not satisfactory. Thirteen patients were pain free after 6 months, but only four remained so after 2.5 years. The target localization was performed by stereotactic cisternography and bone landmarks. No dose options were recommended. The authors established that imperfections in the target localization and fixation techniques may contribute to inaccuracies and unsatisfactory results.
Many years after Leksell’s report, Rand et al.[38] presented their experience with 12 patients who had radiosurgery for TN. Seven were treated with an 8-mm collimator and five with a 4-mm collimator. Target localization was determined by CT or MRI. Doses varied between 57 and 75 Gy with a median of 65 Gy. The retrogasserian region was the target in eight cases. The entry zone was chosen in four patients. In seven patients, complete relief or improvement was observed. No complications were reported. The third patient treated, a 47-year old woman, had a recurrent trigeminal pain with some atypical pain after neurovascular decompression. She was treated initially at the retrogasserian region with a dose of 65 Gy without pain relief. The pain remained even after a second treatment was performed 7 months later, using a dose of 20 Gy on the TG. It is possible that low doses used in conjunction with atypical characteristics of pain in selected patients explain the results. Based on the fact that some patients did not respond, the authors concluded that the retrogasserian region was probably not appropriate as a primary target for radiosurgical treatment. As such, the entry zone appeared on the scene as the new target for TN radiosurgery treatment.[19,38]
Chen et al.[3] presented their experience treating 40 patients with typical idiopathic TN. The TG was the preferred target because the TG has long been the target of radiofrequency and it is easy to identify by MRI. The radiosurgical treatment was performed with a Linac, and the target dose used was 70 Gy with a 4-mm collimator. The isodose was not specified. A total success rate of 82.8% was reported. The mean time of initial relief was 12.5 days. Pain recurrence was observed in one patient (3%) of the 33 patients who obtained excellent and good results. Nevertheless, the median follow-up period had a median of 7.9 months (range: 1–19 months). The prescribed doses were low with a short follow-up.
Target location, accuracy, and treatment dose
Since the duration of pain relief tends to lessen over time, various modifications of the radiosurgical technique for TN have been devised to improve outcomes such as the duration of pain relief.[8,17,28,40,48] Many studies demonstrate good or excellent results when the target is placed close to the gasserian ganglion.[17,28,35,40] However, until now, it has not been clear how different targeting locations impact the rate of postoperative pain control and the morbidity of radiosurgery.[19,40,48] In general, two targeting groups have been defined: the proximal target as a location on the trigeminal nerve (root entry zone) and the distal target as a location anterior to the entrance of the nerve from the pons.[35,48]
Many authors have reported that higher the applied dose of the trigeminal nerve, the better the pain control, as well as greater benefits with the use of two isocenters.[1,5,31] However, Fountas et al.[9] found that none of the radiosurgical technique parameters (radiation dose, number of isocenters, and use of plugging or not) were correlated to the patients’ outcome. Flickinger et al.[8] and Kanner et al.[17] did not find benefits with the use of two isocenters. Conversely, Morbidini-Gaffney et al.[31] showed that patients treated with two isocenters on the trigeminal nerve and patients receiving >85 Gy had a longer duration of response.
Accuracy is a critical aspect when placing isocenters on the trigeminal nerve. However, there are inaccuracies that depend on the images, the selection of nerve target site, mechanical errors of the stereotactic frame, and mechanical errors of the radiation equipment used.[10] The addition of errors can be superior to 2 mm. Moreover, there is a minimal submillimetric respiratory movement of the cranial nerves while crossing cerebrospinal fluid space within the skull. Minimal variations of the nerve position during prolonged radiation delivery time may negatively impact the amount of clinically relevant fibers receiving the minimal radiation dose necessary to produce pain relief in conjunction with previous aspects and help explain why some patients fail radiosurgery and some patients respond sooner than others.[10]
In our study, we applied the same doses used in the trigeminal nerve to the TG and we used two isocenters which were determined by the semioval shape of the ganglion and the adjacent fibers of the nerve similar to what was previously described to completely cover the TG.[44]
The dose is one of the most important factors that improve outcomes following GKS for TN. GKS is associated with high rates of pain control. Patients report excellent or good pain relief in more than 70% of cases.[23,25,28,37,39,41,49] The trend over time has been to increase the maximum dose between 70 and 90 Gy in an attempt to achieve better pain control. Higher doses have been reported to increase the efficacy of the procedure but with an increased risk of facial numbness.[18,19,29,36]
Pollock et al.,[36] as well as Maher and Pollock[26] and Nicol et al.,[33] found that, at higher doses of radiation, there is a greater association of risk of trigeminal nerve dysfunction, as well as a better outcome in relation to pain control.
There is no dose established to be used on the TG. Chen et al.[3] reported good results with doses of 70 Gy in the management of their patients, taking the choice of the TG as the target. On the other hand, we have seen good results in our patients treated at the TG at doses of 86 Gy, with a very low rate of complications. Although we acknowledge that our follow-up is still short, it is worth noting that most of the patients have had high initial success and maintain a pain-free clinical state, contrary to what has been observed in many reports where the initial success is high and, during the follow-up, the pain-free status decreases substantially over time.[23,25,35]
On the other hand, vascular injury has been reported in vessels adjacent to the entry zone. Pollock et al.[37] reported that he has performed explorations of the posterior fossa in eight patients after failed radiosurgery. In five of these patients, a region of injury supposedly due to radiation was observed in the superior cerebellar artery at the site where the artery came into contact with the trigeminal nerve. Authors recommended that patients treated with radiosurgery for TN must be watched carefully for possible delayed ischemic events secondary to radiation-induced vascular injury.[26]
More recently, Chen et al.[2] have reported the incidence of de novo superior cerebellar artery aneurysm following radiosurgery treatment at the entry zone for TN. Uchikawa et al.[47] presented two cases of aneurysms following GKS. The first patient developed an anterior inferior cerebellar artery aneurysm at 13 years after radiosurgery. The second case also developed a superior cerebellar artery aneurysm at 9 years after GKS for TN.
It has been established that radiosurgery should not be performed on patients under acute attacks of pain, due to the known latency necessary to produce pain relief with radiosurgery and the fact that it often takes several weeks or months to reach the optimal therapeutic peak. Thus, radiosurgery is considered a second option for patients with severe pain, with difficulty speaking or maintaining adequate hydration, who need an immediate method of pain control through percutaneous procedures.[10,37] We have observed in our patients that, even though they had acute pain, the pain disappeared in the same way as with the patients who did not have acute pain at the time of radiosurgical treatment. This finding was also previously published by us.[44]
Complications, recurrence, and latency period
For excellent results, radiosurgery and other ablative techniques must find a balance between the production of an injury to trigeminal fibers that are sufficient to provide adequate pain relief without causing so much damage that it produces complications such as facial numbness, paresthesias, bothersome dysesthesia, masseter weakness, or disagreeable numbness that could transform into anesthesia Dolorosa.[36]
With radiosurgery targeting the trigeminal nerve, sensory dysfunction is less common than with ablative techniques, ranging between 6% and 66%,[19,30,36,49] and when it is present, it is associated with a high dose of radiation.[36]
In our series, the percentage of complications during the follow-up period was very low, even taking into account that the maximum dose used can be considered within the high range. Table 3 shows a comparative review of patient series treated with SRS for TN.
Table 3:
Review of patient series treated with SRS for TN.

Another important aspect to consider is the recurrence of attacks of facial pain which is contrary to the goal of obtaining a pain-free status.[15,16] We had such a recurrence in four patients. In all cases, the pain was controlled again with the use of medication, except for one case where the patient decided to undergo surgical treatment.
The effect of the latency period after SRS is reported in most series as an interval of 1–2 months.[5,20,40,50] In a recent communication, Mousavis et al.[32] reported a total of 121 patients with medically refractory TN and without prior surgery that underwent early GKS which was defined as a period <3 years of pain onset. The authors suggested that early radiosurgery provides superior pain relief for patients with TN. A short latency period seems to be important not only in terms of the early relief of the painful condition but also in terms of being a good predictor of the length of pain-free status. Patients who responded to SRS within the first 3 weeks after SRS had a longer duration of pain-free status compared to those with longer response times.
It has been suggested that this parameter should be seriously considered for radiosurgical planning. Patients with previous surgery seem to be more frequently late responders to GKS than patients with no history of previous surgery.[9]
In our cases, we observed a short latency period with a median of 7 days (range, 1–40). In 18 patients, the pain relief was obtained before 7 days. Patients with a long history of TN had similar responses to those with a short history; history of previous surgery did not have any influence on the results.
The TG role of the satellite glial cells (SGC)
Although the vascular compression theory is popular, it cannot account for all phenomena associated with TN.[6,24,42] There is some evidence contrary to the neurovascular compression hypothesis. In two studies on cadavers without TN, neurovascular contact was observed in 13–32% of cadavers with neurovascular compression ranging from 8% to 10%.[12] Majoie et al.[27] presented one MRI study where they examined 170 trigeminal nerves in 85 non TN patients. Seventy-nine nerves (46%) had some point of contact with a vascular structure, 24 (14%) had cisternae contact, 52 (30%) had a contact at the root entry zone, and the remaining 3 (2%) had an actual deformity of the root entry zone.
It seems that the main feature of TN pain is its dynamic nature which is difficult to explain in purely anatomical terms. The fact that the pain is not continuous, but paroxysmal speaks against the fact that a simple compression is an ectopic generator of pain at the level of the lesion. Moreover, pain must not only occur spontaneously but must also be produced, as often happens, by innocuous tactile stimuli. Therefore, demyelination alone does not provide clear evidence of the characteristic symptoms of the disease. It has been assumed that the pain is the result of hyperactivity or abnormal discharges. These arise from the gasserian ganglion, the “injured” nerve root, and the trigeminal nucleus within the brainstem.[24]
TG seems to have a predominant role given its cellular architecture. The crescent-shaped TG lies on Meckel’s cave, which is a rigid structure. The TG has dimensions ranging from 14 to 22 mm in length and 4–5 mm in thickness and is easily identified on CT or MRI.[3,51] With these features, the TG is an easy target and there is much less possibility of movement during treatment.
The fine structure of the TG contains cells that give rise to the three divisions of the trigeminal nerve. The cell bodies of neurons are completely surrounded by specialized glial cells known as SGC that together form distinct, functional units.[14,34]
Neurons and SGCs extend processes that are thought to facilitate the exchange of chemicals between neurons and glia and can communicate directly through gap junctions that allow for the direct transfer of small molecular weight molecules, such as ions, that regulate cellular excitability, metabolic precursors, and second messengers.[14,34]
V1, V2, and V3 regions are interconnected. Stimulation of V3 neurons could cause increased levels of active signaling proteins in neuronal and SGCs in other regions of the ganglion which could explain why a pain originating in V2, for example, is propagated to V1 and/or V3, contributing to signal propagation and chronic pain.[4,14]
SGCs divide after an insult to the peripheral nerve including nerve damage.[46] These changes involve the activation of mechanisms signaling between neurons and these cells,[4,34] with an increasing of number of gap junctions between SGCs. Since gap junctions are a means for moving molecules between SGCs, it is reasonable to suppose that changes in gap junctions could cause alterations in the extracellular environment and, as a consequence, would be a change in neuronal excitability and nociception. Therefore, they play this important role through the regulation of the levels of ions as potassium and calcium and other small molecules in the environment around the neuronal cell body[45] and the regulation of their resting membrane potential. SGCs maintain normal levels of extracellular K+ around neuronal cell bodies.[34]
Therefore, the glial cells have the ability to communicate with neurons and modulate their activity, particularly in TG where SGCs establish a privileged relationship with the surrounding neuronal bodies. The increased neuron-glial interactions are thought to play an important role in the induction and maintenance of peripheral sensitization of trigeminal nociceptors.[14,34]
TG may become the first level of the pathophysiological changes of modulation of afferent signaling, as it allows the interaction between different types of information and seems to be a trigger of the central sensitization mechanism as observed also in the spinal cord dorsal horn neurons in relation to the spinal ganglion.[45]
Thus, knowledge about the SGC and its mechanisms of interaction with the neuronal body assumes a growing importance in the search for new targets for chronic pain treatment, which includes TN.[14,45]
The occurrence of a refractory period of seconds to minutes after an attack of TN is well known, during which further attacks cannot be provoked. Besides demyelination, other factors could delay the restoration of membrane potentials and excitability after an episode of TN.[6,11]
The refractoriness period could be explained by the release of potassium ions due to the activation of potassium channels by calcium, leading to neuronal hyperpolarization and the trigger stop.[6,10,24]
Our findings suggest that there is a longer refractory period as a consequence of the treatment of the ganglion and nerve adjacent fibers, probably affecting primarily the SGCs and, as a consequence, the repolarization process which would produce a delay of a possible new attack.
How does radiosurgery act on trigeminal pain?
At present, from a pathological point of view, the exact mechanism of pain relief is unknown. There is the assumption that there exists a critical region in which the central myelin (oligodendrocyte) becomes peripheral (Schwann cell) myelin. The oligodendrocytes are more sensitive to irradiation than Schwann cells, and consequently, a stronger radiobiological effect would occur on the root entry zone.[19]
However, Régis et al. treated the trigeminal nerve at the pontine cistern where the myelin is peripheral (Schwan cells) obtaining the same results.[41]
In any case, after the treatment, it is observed that patients report an immediate decrease in the intensity of pain even if the attacks still occur. This is postulated to be the result of an immediate interruption of ephaptic transmission. Several weeks later, there is a complete cessation of the attacks. This is probably secondary to delayed demyelination injury to the nerve. The compact union of fibers from different divisions would facilitate the irradiation of the entire nerve with the smallest volume of energy (4-mm collimator).[19] Even though demyelination can contribute to the generation of TN episodes, other mechanisms could help explain how radiosurgery acts in the process of pain relief.
There is a growing body of evidence that glial satellite cells undergo structural and biochemical changes after nerve injury which influence neuronal excitability and consequently the development and/or maintenance of pain in different animal models of chronic pain.[4,11] The activation of SGC is believed to both increase and prolong the effects of peripherally induced nociception that occurs with the activation of central glia.[11] The manner in which this occurs remains to be clarified, but results suggest that radiosurgery may deactivate SGC contributing to the elimination of the pain or the decreasing of its intensity. The few adverse effects observed in our cases could be explained by the less compact conformation of nerve fibers at the ganglion level. On the TG, the major effect is more likely to be on the perineural satellite cells, which leads to several important achievements such as cessation of pain with a lower risk of secondary effects, probably due to hyperpolarization of the perineural space. In addition, a short latency period and a longer pain-free period have been observed in our patients.
CONCLUSIONS
Radiosurgery on TG for the treatment of TN has several positive aspects: short latency period, minor collateral effects, a high percentage of pain control, and the pain relief which is not related to the time of the diagnosis of TN. In general, a better understanding of the radiobiology and pathophysiology of NT is important to explain the mechanism of action of radiosurgery.
The current series investigates the use of TG to treat NT using GK with commonly used doses and high-resolution images. A comparative prospective randomized trial is necessary for the use of GKR on the TG for idiopathic TN.
Aknowledgement
We thank Dr. Roman Liscak who provided insight and expertise for reviewing and for his comments that greatly improved the manuscript, although he may not agree with all of the interpretations/conclusions of this paper.
Contributor Information
Salvador Somaza, Email: ssomaza@gmail.com.
Eglee M. Montilla, Email: .
Maria C. Mora, Email: .
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Alpert TE, Chung CT, Mitchell LT, Hodge CJ, Montgomery CT, Bogart JA, et al. Gamma knife surgery for trigeminal neuralgia: Improved initial response with two isocenters and increasing dose. J Neurosurg. 2005;(102 Suppl):185–8. doi: 10.3171/jns.2005.102.s_supplement.0185. [DOI] [PubMed] [Google Scholar]
- 2.Chen JC, Chao K, Rahimian J. De novo superior cerebellar artery aneurysm following radiosurgery for trigeminal neuralgia. J Clin Neurosci. 2017;38:87–90. doi: 10.1016/j.jocn.2016.12.026. [DOI] [PubMed] [Google Scholar]
- 3.Chen MJ, Shao ZY, Zhang WJ, Wang ZH, Zhang WH, Hu HS, et al. X-knife stereotactic radiosurgery on the trigeminal ganglion to treat trigeminal neuralgia: A preliminary study. Minim Invasive Neurosurg. 2010;53:223–8. doi: 10.1055/s-0030-1269926. [DOI] [PubMed] [Google Scholar]
- 4.Costa FA, Moreira Neto FL. Satellite glial cells in sensory ganglia: Its role in pain. Rev Bras Anestesiol. 2015;65:73–81. doi: 10.1016/j.bjan.2013.07.013. [DOI] [PubMed] [Google Scholar]
- 5.Dellaretti M, Reyns N, Touzet G, Sarrazin T, Dubois F, Lartigau E, et al. Clinical outcomes after gamma knife surgery for idiopathic trigeminal neuralgia: Review of 76 consecutive cases. J Neurosurg. 2008;(109 Suppl):173–8. doi: 10.3171/JNS/2008/109/12/S26. [DOI] [PubMed] [Google Scholar]
- 6.Devor M, Amir R, Rappaport ZH. Pathophysiology of trigeminal neuralgia: The ignition hypothesis. Clin J Pain. 2002;18:4–13. doi: 10.1097/00002508-200201000-00002. [DOI] [PubMed] [Google Scholar]
- 7.Dhople AA, Adams JR, Maggio WW, Naqvi SA, Regine WF, Kwok Y, et al. Long-term outcomes of gamma knife radiosurgery for classic trigeminal neuralgia: Implications of treatment and critical review of the literature. Clinical article. J Neurosurg. 2009;111:351–8. doi: 10.3171/2009.2.JNS08977. [DOI] [PubMed] [Google Scholar]
- 8.Flickinger JC, Pollock BE, Kondziolka D, Phuong LK, Foote RL, Stafford SL, et al. Does increased nerve length within the treatment volume improve trigeminal neuralgia radiosurgery? A prospective double-blind, randomized study. Int J Radiat Oncol Biol Phys. 2001;51:449–54. doi: 10.1016/s0360-3016(01)01606-6. [DOI] [PubMed] [Google Scholar]
- 9.Fountas KN, Smith JR, Lee GP, Jenkins PD, Cantrell RR, Sheils WC, et al. Gamma knife stereotactic radiosurgical treatment of idiopathic trigeminal neuralgia: Long-term outcome and complications. Neurosurg Focus. 2007;23:E8. doi: 10.3171/FOC-07/12/E8. [DOI] [PubMed] [Google Scholar]
- 10.Gorgulho A. Radiation mechanisms of pain control in classical trigeminal neuralgia. Surg Neurol Int. 2012;3:S17–25. doi: 10.4103/2152-7806.91606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Grasso G, Landi A, Alafaci C. A novel pathophysiological mechanism contributing to trigeminal neuralgia. Mol Med. 2016;22:452–4. doi: 10.2119/molmed.2016.00172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haines SJ, Jannetta PJ, Zorub DS. Microvascular relations of the trigeminal nerve. An anatomical study with clinical correlation. J Neurosurg. 1980;52:381–6. doi: 10.3171/jns.1980.52.3.0381. [DOI] [PubMed] [Google Scholar]
- 13.Håkanson S. Trigeminal neuralgia treated by the injection of glycerol into the trigeminal cistern. Neurosurgery. 1981;9:638–46. doi: 10.1227/00006123-198112000-00005. [DOI] [PubMed] [Google Scholar]
- 14.Hanani M. Satellite glial cells in sensory ganglia: From form to function. Brain Res Brain Res Rev. 2005;48:457–76. doi: 10.1016/j.brainresrev.2004.09.001. [DOI] [PubMed] [Google Scholar]
- 15.Hasegawa T, Kondziolka D, Spiro R, Flickinger JC, Lunsford LD. Repeat radiosurgery for refractory trigeminal neuralgia. Neurosurgery. 2002;50:494–500. doi: 10.1097/00006123-200203000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Herman JM, Petit JH, Amin P, Kwok Y, Dutta PR, Chin LS, et al. Repeat gamma knife radiosurgery for refractory or recurrent trigeminal neuralgia: Treatment outcomes and quality-of-life assessment. Int J Radiat Oncol Biol Phys. 2004;59:112–6. doi: 10.1016/j.ijrobp.2003.10.041. [DOI] [PubMed] [Google Scholar]
- 17.Kanner AA, Neyman G, Suh JH, Weinhous MS, Lee SY, Barnett GH, et al. Gamma knife radiosurgery for trigeminal neuralgia: Comparing the use of a 4-mm versus concentric 4-and 8-mm collimators. Stereotact Funct Neurosurg. 2004;82:49–57. doi: 10.1159/000076661. [DOI] [PubMed] [Google Scholar]
- 18.Kim YH, Kim DG, Kim JW, Kim YH, Han JH, Chung HT, et al. Is it effective to raise the irradiation dose from 80 to 85 gy in gamma knife radiosurgery for trigeminal neuralgia ? Stereotact Funct Neurosurg. 2010;88:169–76. doi: 10.1159/000313869. [DOI] [PubMed] [Google Scholar]
- 19.Kondziolka D, Lunsford LD, Flickinger JC, Young RF, Vermeulen S, Duma CM, et al. Stereotactic radiosurgery for trigeminal neuralgia: A multiinstitutional study using the gamma unit. J Neurosurg. 1996;84:940–5. doi: 10.3171/jns.1996.84.6.0940. [DOI] [PubMed] [Google Scholar]
- 20.Kondziolka D, Perez B, Flickinger JC, Habeck M, Lunsford LD. Gamma knife radiosurgery for trigeminal neuralgia: Results and expectations. Arch Neurol. 1998;55:1524–9. doi: 10.1001/archneur.55.12.1524. [DOI] [PubMed] [Google Scholar]
- 21.Leksell L. Sterotaxic radiosurgery in trigeminal neuralgia. Acta Chir Scand. 1971;137:311–4. [PubMed] [Google Scholar]
- 22.Lindquist C, Kihlström L, Hellstrand E. Functional neurosurgery-a future for the gamma knife ? Stereotact Funct Neurosurg. 1991;57:72–81. doi: 10.1159/000099557. [DOI] [PubMed] [Google Scholar]
- 23.Little AS, Shetter AG, Shetter ME, Bay C, Rogers CL. Long-term pain response and quality of life in patients with typical trigeminal neuralgia treated with gamma knife stereotactic radiosurgery. Neurosurgery. 2008;63:915–23. doi: 10.1227/01.NEU.0000327689.05823.28. [DOI] [PubMed] [Google Scholar]
- 24.Love S, Coakham HB. Trigeminal neuralgia: Pathology and pathogenesis. Brain. 2001;124:2347–60. doi: 10.1093/brain/124.12.2347. [DOI] [PubMed] [Google Scholar]
- 25.Maesawa S, Salame C, Flickinger JC, Pirris S, Kondziolka D, Lunsford LD, et al. Clinical outcomes after stereotactic radiosurgery for idiopathic trigeminal neuralgia. J Neurosurg. 2001;94:14–20. doi: 10.3171/jns.2001.94.1.0014. [DOI] [PubMed] [Google Scholar]
- 26.Maher CO, Pollock BE. Radiation induced vascular injury after stereotactic radiosurgery for trigeminal neuralgia: Case report. Surg Neurol. 2000;54:189–93. doi: 10.1016/s0090-3019(00)00266-4. [DOI] [PubMed] [Google Scholar]
- 27.Majoie CB, Hulsmans FJ, Verbeeten B, Jr, Castelijns JA, van Beek EJ, Valk J, et al. Trigeminal neuralgia: Comparison of two MR imaging techniques in the demonstration of neurovascular contact. Radiology. 1997;204:455–60. doi: 10.1148/radiology.204.2.9240535. [DOI] [PubMed] [Google Scholar]
- 28.Massager N, Lorenzoni J, Devriendt D, Desmedt F, Brotchi J, Levivier M, et al. Gamma knife surgery for idiopathic trigeminal neuralgia performed using a far-anterior cisternal target and a high dose of radiation. J Neurosurg. 2004;100:597–605. doi: 10.3171/jns.2004.100.4.0597. [DOI] [PubMed] [Google Scholar]
- 29.Massager N, Murata N, Tamura M, Devriendt D, Levivier M, Régis J, et al. Influence of nerve radiation dose in the incidence of trigeminal dysfunction after trigeminal neuralgia radiosurgery. Neurosurgery. 2007;60:681–7. doi: 10.1227/01.NEU.0000255393.77538.75. [DOI] [PubMed] [Google Scholar]
- 30.Matsuda S, Serizawa T, Sato M, Ono J. Gamma knife radiosurgery for trigeminal neuralgia: The dry-eye complication. J Neurosurg. 2002;97:525–8. doi: 10.3171/jns.2002.97.supplement. [DOI] [PubMed] [Google Scholar]
- 31.Morbidini-Gaffney S, Chung CT, Alpert TE, Newman N, Hahn SS, Shah H, et al. Doses greater than 85 gy and two isocenters in gamma knife surgery for trigeminal neuralgia: Updated results. J Neurosurg. 2006;(105 Suppl):107–11. doi: 10.3171/sup.2006.105.7.107. [DOI] [PubMed] [Google Scholar]
- 32.Mousavi SH, Niranjan A, Huang MJ, Laghari FJ, Shin SS, Mindlin JL, et al. Early radiosurgery provides superior pain relief for trigeminal neuralgia patients. Neurology. 2015;85:2159–65. doi: 10.1212/WNL.0000000000002216. [DOI] [PubMed] [Google Scholar]
- 33.Nicol B, Regine WF, Courtney C, Meigooni A, Sanders M, Young B, et al. Gamma knife radiosurgery using 90 gy for trigeminal neuralgia. J Neurosurg. 2000;93(Suppl 3):152–4. doi: 10.3171/jns.2000.93.supplement. [DOI] [PubMed] [Google Scholar]
- 34.Ohara PT, Vit JP, Bhargava A, Romero M, Sundberg C, Charles AC, et al. Gliopathic pain: When satellite glial cells go bad. Neuroscientist. 2009;15:450–63. doi: 10.1177/1073858409336094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Park SH, Hwang SK, Kang DH, Park J, Hwang JH, Sung JK, et al. The retrogasserian zone versus dorsal root entry zone: Comparison of two targeting techniques of gamma knife radiosurgery for trigeminal neuralgia. Acta Neurochir (Wien) 2010;152:1165–70. doi: 10.1007/s00701-010-0610-0. [DOI] [PubMed] [Google Scholar]
- 36.Pollock BE, Phuong LK, Foote RL, Stafford SL, Gorman DA. High-dose trigeminal neuralgia radiosurgery associated with increased risk of trigeminal nerve dysfunction. Neurosurgery. 2001;49:58–62. doi: 10.1097/00006123-200107000-00008. [DOI] [PubMed] [Google Scholar]
- 37.Pollock BE, Phuong LK, Gorman DA, Foote RL, Stafford SL. Stereotactic radiosurgery for idiopathic trigeminal neuralgia. J Neurosurg. 2002;97:347–53. doi: 10.3171/jns.2002.97.2.0347. [DOI] [PubMed] [Google Scholar]
- 38.Rand RW, Jacques DB, Melbye RW, Copcutt BG, Levenick MN, Fisher MR, et al. Leksell gamma knife treatment of tic douloureux. Stereotact Funct Neurosurg. 1993;61(Suppl 1):93–102. doi: 10.1159/000100663. [DOI] [PubMed] [Google Scholar]
- 39.Régis J, Bartolomei F, Metellus P, Rey M, Genton P, Dravet C, et al. Radiosurgery for trigeminal neuralgia and epilepsy. Neurosurg Clin N Am. 1999;10:359–77. [PubMed] [Google Scholar]
- 40.Régis J, Metellus P, Hayashi M, Roussel P, Donnet A, Bille-Turc F, et al. Prospective controlled trial of gamma knife surgery for essential trigeminal neuralgia. J Neurosurg. 2006;104:913–24. doi: 10.3171/jns.2006.104.6.913. [DOI] [PubMed] [Google Scholar]
- 41.Régis J, Tuleasca C, Resseguier N, Carron R, Donnet A, Gaudart J, et al. Long-term safety and efficacy of gamma knife surgery in classical trigeminal neuralgia: A 497-patient historical cohort study. J Neurosurg. 2016;124:1079–87. doi: 10.3171/2015.2.JNS142144. [DOI] [PubMed] [Google Scholar]
- 42.Sabalys G, Juodzbalys G, Wang HL. Aetiology and pathogenesis of trigeminal neuralgia: A comprehensive review. J Oral Maxillofac Res. 2013;3:e2. doi: 10.5037/jomr.2012.3402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Singh R, Davis J, Sharma S. Stereotactic radiosurgery for trigeminal neuralgia: A retrospective multi-institutional examination of treatment outcomes. Cureus. 2016;8:e554. doi: 10.7759/cureus.554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Somaza S, Hurtado W, Montilla E, Ghaleb J. Gamma knife radiosurgery to the trigeminal ganglion for treatment of trigeminal neuralgia secondary to vertebrobasilar ectasia. Surg Neurol Int. 2014;5:S580–5. doi: 10.4103/2152-7806.148056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Takeda M, Takahashi M, Matsumoto S. Contribution of the activation of satellite glia in sensory ganglia to pathological pain. Neurosci Biobehav Rev. 2009;33:784–92. doi: 10.1016/j.neubiorev.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 46.Thalakoti S, Patil VV, Damodaram S, Vause CV, Langford LE, Freeman SE, et al. Neuron-glia signaling in trigeminal ganglion: Implications for migraine pathology. Headache. 2007;47:1008–23. doi: 10.1111/j.1526-4610.2007.00854.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Uchikawa H, Nishi T, Kaku Y, Goto T, Kuratsu JI, Yano S, et al. Delayed development of aneurysms following gamma knife surgery for trigeminal neuralgia: Report of 2 cases. World Neurosurg. 2017;99:813.e13–21. doi: 10.1016/j.wneu.2016.11.069. [DOI] [PubMed] [Google Scholar]
- 48.Xu Z, Schlesinger D, Moldovan K, Przybylowski C, Sun X, Lee CC, et al. Impact of target location on the response of trigeminal neuralgia to stereotactic radiosurgery. J Neurosurg. 2014;120:716–24. doi: 10.3171/2013.10.JNS131596. [DOI] [PubMed] [Google Scholar]
- 49.Young B, Shivazad A, Kryscio RJ, St Clair W, Bush HM. Long-term outcome of high-dose γ knife surgery in treatment of trigeminal neuralgia. J Neurosurg. 2013;119:1166–75. doi: 10.3171/2013.1.JNS12875. [DOI] [PubMed] [Google Scholar]
- 50.Young RF, Vermeulen SS, Grimm P, Blasko J, Posewitz A. Gamma knife radiosurgery for treatment of trigeminal neuralgia: Idiopathic and tumor related. Neurology. 1997;48:608–14. doi: 10.1212/wnl.48.3.608. [DOI] [PubMed] [Google Scholar]
- 51.Yousry I, Moriggl B, Schmid UD, Naidich TP, Yousry TA. Trigeminal ganglion and its divisions: Detailed anatomic MR imaging with contrast-enhanced 3D constructive interference in the steady state sequences. AJNR Am J Neuroradiol. 2005;26:1128–35. [PMC free article] [PubMed] [Google Scholar]