

Abstract
Background:
Isolated cryptococcal osteomyelitis of the spine is extremely uncommon; there have been only seven cases identified in literature. The majority were originally misdiagnosed as tuberculosis. Here, we present a patient with cryptococcal osteomyelitis of the thoracic spine with associated fungal retinal deposits.
Case Description:
A 45-year-old, type II diabetic female presented with a 5-month history of severe back pain. Her magnetic resonance imaging (MRI) revealed osteomyelitis involving the T4 vertebral body with epidural and prevertebral extension; notably, the intervertebral disc spaces were not involved. Although the fine-needle aspiration cytologic examination was inconclusive, the patient was empirically placed on antitubercular drug therapy. One month later, she became fully paraplegic. The MRI now demonstrated osteolytic lesions involving the T4 vertebral body with cord compression. She underwent biopsy of the T4 vertebral body and a transfacet T4 decompression with T2-T6 pedicle screw fixation. Culture and histopathological examinations both documented a cryptococcal infection, and she was placed on appropriate antifungal therapy. Notably, 3 weeks after surgery, she developed a sudden loss of vision loss due to retinal fungal endophthalmitis. She recovered vision in one eye after the administration of intravitreal voriconazole but lost vision in the other eye despite a vitrectomy. Over the next 8 months, she gradually recovered with motor function of 4/5 in both lower extremities without evidence of recurrent disease.
Conclusion:
Cryptococcal infection should be among the differential diagnostic considerations for patients with vertebral osteomyelitis. Notably, diagnostic delay can lead to devastating neurological deficits and involvement of other organ systems.
Keywords: Cryptococcosis, Differential diagnosis, Endophthalmitis, Osteomyelitis, Spine infection, Thoracic vertebra

INTRODUCTION
Cryptococcus neoformans is an encapsulated fungal organism, which is abundant in topsoil, decayed food, and bird droppings (e.g., particularly pigeon fecal matter). Inhalation of C. neoformans primarily results in lung infections although, through hematogenous spread, it may also involve the meninges and other organ systems. Although meningitis is most frequently seen in immunocompromised hosts, 10–40% of cryptococcosis infections occur in those without a major primary illness or immunodeficiency. Isolated cryptococcal osteomyelitis of the spine is extremely uncommon, with only seven cases reported in literature.[1-8] Interestingly, most cases are originally misdiagnosed as tuberculosis (TB) and only correctly documented by biopsy. Here, we present an immunocompromised patient with cryptococcal T4 osteomyelitis who later developed hematogenous retinal deposits resulting in permanent unilateral vision loss.
CASE REPORT
Clinical presentation and surgery
A 45-year-old female with type II diabetes presented with a 5-month history of severe back pain. She was a homemaker who kept pigeons as pets. Her laboratory investigations revealed an erythrocyte sedimentation rate (ESR) of 38 mm/1st h and a C-reactive protein (CRP) of 18 mg/l. The magnetic resonance imaging (MRI) demonstrated T4 osteomyelitis with relatively well-preserved intervertebral disc spaces [Figure 1]. Although fine-needle aspiration cytology was inconclusive, the patient was presumptively placed on antitubercular drugs. One month later, she became fully paraplegic. At that point, the MRI demonstrated osteolytic lesions of the T4 vertebral body with cord compression, accompanied by bilateral paraspinal soft tissue masses extending to the T5-T6 level; there was, however, no disc space involvement [Figure 2]. She underwent a biopsy of the T4 vertebral body, accompanied by transfacet T4 decompression, and posterior T2- T6 pedicle screw instrumentation [Figure 3].
Figure 1:

Magnetic resonance imaging showing involvement of T4 vertebra with intervertebral disc spaces relatively preserved. (a) T2 weighted, (b) T1 weighted, (c) contrast.
Figure 2:
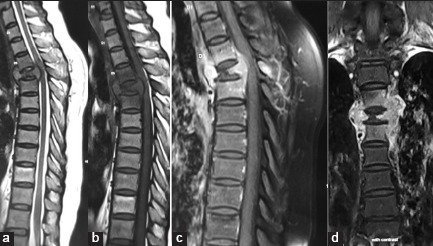
Magnetic resonance imaging showing osteolytic lesions of the fourth thoracic vertebra with cord compression, paravertebral soft tissue mass was seen on both sides of T4 vertebra up to T5-T6 disc space without disc space involvement. (a) T2 weighted, (b) T1 weighted, (c and d) contrast.
Figure 3:
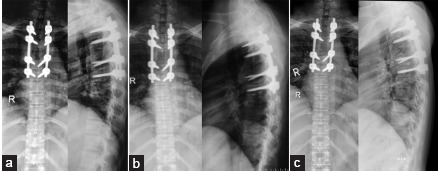
Postoperative X-rays showing fixation from T2 to T6 level. (a) Immediate postoperative, (b) 3-month follow-up, and (c) 8-month follow-up.
Cultures, histology, and further treatment
The culture and histopathological examinations revealed a cryptococcal fungal infection that was sensitive to amphotericin B; this was administered intravenously (150 mg/day) for the next 3 months [Figure 4]. However, the patient developed an abscess at the surgical site 2 weeks later, which required drainage. Three weeks postoperatively, she also developed the sudden loss of vision bilaterally; the ophthalmological examination revealed bilateral retinal fungal deposits and endophthalmitis. One eye’s vision recovered after intravitreal voriconazole, but she lost vision in the other eye despite vitrectomy. The amphotericin B antibiotic regimen was then supplemented with flucytosine (i.e., 500 mg thrice a day) until the 3rd postoperative month.
Figure 4:
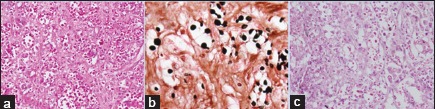
Histopathological analysis showing inflammatory granulation tissue, focal necrosis with scattered fungal organisms. (a) Periodic acid– Schiff stain, (b) silver stain, (c) mucicarmine stain.
Follow-up
Three months following the spinal surgery, she regained 4/5 function in both lower extremities. Although the MRI still showed some prevertebral collection compared with the preoperative MRI, there was resolution of the T4 cord compression [Figure 5]. Eight months postoperatively, the patient could walk with a cane but had residual unilateral loss of vision (perception of light only). Furthermore, the ESR and CRP levels both normalized. In addition, the MRI now showed complete resolution of the prevertebral abscess and the previously abnormal signal within the T3-T5 vertebral bodies [Figure 6]. After 3 postoperative months passed, intravenous amphotericin B was stopped, but she was kept on oral fluconazole 400 mg once a day, and flucytosine 500 mg thrice a day for 5 months.
Figure 5:

Three months follow-up magnetic resonance imaging showing prevertebral collection. Compared to preoperative magnetic resonance imaging, there is resolution of the compression over the spinal cord at T4 level. (a) T2 weighted, (b) T1 weighted, (c) short tau inversion recovery.
Figure 6:

Eight months follow-up magnetic resonance imaging showing complete resolution of prevertebral abscess with resolution of the signal alteration in vertebral bodies. (a) T2 weighted, (b) T1 weighted, (c) short tau inversion recovery.
DISCUSSION
Vertebral involvement with cryptococcosis is very rare, typically involves the immunocompetent population, and is usually associated with both a raised ESR and CRP (sensitivity 80% and 100%, respectively) levels.[8] Although the serum cryptococcal antigen testing is useful (i.e., accuracy of 66%), this is not necessarily true for immunocompetent individuals. Notably, the clinical presentation is very variable and cannot readily be utilized to differentiate cryptococcosis from other pathologies.
Surgery and histopathological confirmation of spinal cryptococcosis
It is important to differentiate cryptococcosis from malignant spine tumors and TB.[4] According to the Infectious Diseases Society of America, the combined strategy of antifungal medications and surgery to decompress and stabilize the spine is key to controlling this infection. Notably, histopathological examinations and microbial cultures are mandatory to correctly establish a definitive diagnosis.
Literature review – eight cases of spinal cryptococcosis
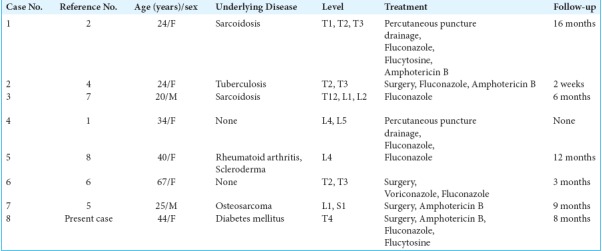
In 1955, Eisen et al.[3] first documented cryptococcosis in a 29-year-old female with both lung and L3 spinous process involvement. The eight patients reviewed in literature (including this case) who presented with spinal/vertebral Cryptococcus osteomyelitis averaged 35 years of age and included six females and two males [Table 1]. The MRI scans documented disease involving the thoracic, lumbar, and sacral levels (i.e., in descending order), with/without paravertebral and/ or intracanalicular extension. Treatment options included decompressive laminectomy, laminectomy with instrumented fusions, or anterior corpectomy/fusion with/without posterior fusions [Table 1].
Table 1:
Main characteristics of eight cases of spinal cryptococcosis.
This case summary
Our patient was initially misdiagnosed and treated for tuberculosis. The T4 biopsy, however, obtained during decompression/fusion confirmed the diagnosis of a cryptococcal fungal infection. She was then placed on amphotericin B and later required the addition of fluconazole/flucytosine.
CONCLUSION
Cryptococcal spinal infections must be considered among the differential diagnoses for patients presenting with vertebral osteomyelitis. Biopsy/histological/surgical confirmation of the diagnosis is critical to avoid undue delay, risking further hematogenous spread of infection to other organ systems.
Acknowledgment
We would like to thank Dr. Chand Sahai, Senior Anesthesiologist, as part of our surgical team and for correcting grammatical mistakes in manuscript.
Contributor Information
Nitin Adsul, Email: no1.nitinadsul@gmail.com.
K. L. Kalra, Email: kashkalra55@hotmail.com.
Nikhil Jain, Email: drnikhil.jn@gmail.com.
Mukesh Haritwal, Email: 0788muke@gmail.com.
R. S. Chahal, Email: rupinder72@hotmail.com.
Shankar Acharya, Email: spineshankar@gmail.com.
Sunila Jain, Email: s_isha19@rediffmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Al-Tawfiq JA, Ghandour J. Cryptococcus neoformans abscess and osteomyelitis in an immunocompetent patient with tuberculous lymphadenitis. Infection. 2007;35:377–82. doi: 10.1007/s15010-007-6109-9. [DOI] [PubMed] [Google Scholar]
- 2.Cook PP. Successful treatment of cryptococcal osteomyelitis and paraspinous abscess with fluconazole and flucytosine. South Med J. 2001;94:936–8. [PubMed] [Google Scholar]
- 3.Eisen D, Shapiro I, Fischer JB. A case of cryptococcosis with involvement of lungs and spine. Can Med Assoc J. 1955;72:33–5. [PMC free article] [PubMed] [Google Scholar]
- 4.Gupta SK, Chhabra R, Sharma BS, Das A, Khosla VK. Vertebral cryptococcosis simulating tuberculosis. Br J Neurosurg. 2003;17:556–9. doi: 10.1080/02688690310001626868. [DOI] [PubMed] [Google Scholar]
- 5.Lai Q, Liu Y, Yu X, Lv X, Wang Q, Zhou Y, et al. Diagnosis and treatment of nonadjacent cryptococcal infections at the L1 and S1 vertebrae. Orthopade. 2017;46:85–9. doi: 10.1007/s00132-016-3349-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang C, Jia N, Zhang L, Liu K, Liu H, Yu H, et al. Imaging findings of cryptococcal infection of the thoracic spine. Int J Infect Dis. 2014;29:162–5. doi: 10.1016/j.ijid.2014.07.013. [DOI] [PubMed] [Google Scholar]
- 7.Wildstein MS, Martin SM, Jr, Glaser JA. Cryptococcal osteomyelitis in a 20-year-old male with sarcoidosis. Spine J. 2005;5:467–70. doi: 10.1016/j.spinee.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 8.Zhou HX, Ning GZ, Feng SQ, Jia HW, Liu Y, Feng HY, et al. Cryptococcosis of lumbar vertebra in a patient with rheumatoid arthritis and scleroderma: Case report and literature review. BMC Infect Dis. 2013;13:128. doi: 10.1186/1471-2334-13-128. [DOI] [PMC free article] [PubMed] [Google Scholar]