

Abstract
Mindfulness intervention aims to reduce stress and to improve physical and mental health. The present study investigated feasibility and effectiveness of mindfulness intervention in a prison context, in both a qualitative and quantitative fashion. Specifically, the mindfulness-based stress reduction (MBSR) intervention was investigated, in a retrospective pre–post design, in five Dutch prisons. Twenty-two inmates (out of 25 approached, mean age: 40.1 years (SD = 11.1), convicted of murder, manslaughter, sexual offenses, drug offenses, robbery with violence, and/or illegal restraint/kidnap, and sentenced to incarceration between 15 and 209 months (M = 5.5 years; SD = 3.8) took part in a semistructured interview after completion of the MBSR intervention. The interviews addressed level of satisfaction and challenges regarding the MBSR intervention as well as potential effects on stress responsivity, coping style, impulse control, aggression, and self-esteem. Ten staff members and four MBSR instructors were interviewed about their own practical issues experienced while providing or facilitating the MBSR intervention, and about the effects or changes they observed in the inmates who underwent the intervention. Both participants and instructors/prison staff reported improvements in all of the addressed domains and expressed satisfaction with the intervention. Challenges were mainly identified in practical issues regarding the organization of the intervention sessions. Future studies should investigate mindfulness in longitudinal randomly controlled designs, should strive for a multi-method approach, and distinguish inmates according to personality characteristics.
Keywords: mindfulness-based stress reduction, prison, inmates, alternative treatment
Introduction
Mindfulness intervention is widely used to achieve stress reduction. It has proven its usefulness in the general population and for people experiencing several psychiatric conditions (see for a review: Baer, 2003). In recent years, it has been introduced in prison settings, where it also appears to be a welcome addition to behavior-based interventions that have been in place for longer periods of time (Himelstein, 2011).
Behavioral change interventions for inmates can be important tools to improve reintegration into society, and to reduce criminal recidivism (Lipsey & Cullen, 2007). It is known that inmates often suffer from mental health problems. In the Netherlands, 80% to 90% of the incarcerated population in prison had, at some point in their lifetime, a psychiatric diagnosis (Bulten, 2009). Examples of frequently occurring psychiatric diagnoses are attention deficit and hyperactivity disorder (ADHD), antisocial personality disorder, drug- and alcohol-addiction, anxiety disorder, depression, and psychotic disorder. International research also shows that incarcerated populations are more likely to have been exposed to trauma, compared with the general population, and to suffer from post-traumatic stress disorder (PTSD; Goff, 2007). Unfortunately, existing interventions are not always effective in addressing these problems or long-term reintegration into society, which may be due to intervention characteristics (e.g., the trained aspects of cognition might not sufficiently improve or sufficiently translate to behavioral improvement), to suboptimal process control (e.g., a lack of skills among instructors/coaches or a lack of facilities in certain prison settings), or to a mismatch between the interventions that are offered and particular personality structures of the targeted population (Shonin, Gordon, Slade, & Griffiths, 2013).
Mild intellectual disability, low self-esteem, and abnormal stress responsivity are well-established risk factors for criminal behavior (Froggio & Agnew, 2007; Moffitt, Krueger, Caspi, & Fagan, 2000; Van Wijk, Schoenmakers, & Manders, 2011), but they are also related to reduced responsiveness to cognitive behavioral training (CBT; Bonta & Andrews, 2003; Polaschek, 2010a; Ward, Day, Howells, & Birgden, 2004). Fischer, Captein, and Zwirs (2012) concluded in their study about available interventions in prison settings in the Netherlands that particularly these factors are not adequately addressed by the behavioral interventions currently offered to prisoners. Cognitive behavioral interventions are, for example, not tailored to persons with mild intellectual disability. They also do not address personal emotional well-being. And, importantly, incarceration brings specific additional stress to inmates, related to feelings of fear, frustration, and anger (Fogel, 1993; Perkins, 1998). It has even been suggested that the atmosphere in prisons increases the chance of aggressive and hostile behaviors in inmates, and that this could lead to more criminal behavior after release (Haney, 2006). It is therefore important that more effective interventions become available that are tailored to the cognitive abilities of the prison population and that take into account the potential lack of self-esteem and abnormal stress responsivity among prison inmates, and that fit well or easily translate to the specific setting of prisons.
Stress reduction, which can be achieved in different ways, seems to have translational effects in offenders/inmates with respect to, for example, mood, coping strategies, and drug use. For instance, positive direct effects on stress reduction and translational effects have been reported for (interventions involving) therapeutic writing (Pankey, Kelly, & Ramaswamy, 2016), theatre and music (Davey, Day, & Balfour, 2015), and yoga (Bilderbeck, Farias, Brazil, Jakobowitz, & Wikholm, 2013; Kerekes, Fielding, & Apelqvist, 2017).
Also, mindfulness-based interventions were shown to result in increased self-esteem (Brown & Ryan, 2003; Reibel, Greeson, Brainard, & Rosenzweig, 2001) and more normal levels of stress responsivity (Baer, 2003) in general populations. Such interventions may, therefore, be able to improve the conditions for cognitive behavioral intervention in prisons. These interventions could possibly also reduce psychiatric symptoms, and stimulate positive behavioral changes in prison inmates through other aspects of cognition and emotion regulation that have been associated with aggression, criminal behavior, and recidivism. Examples include (emotion-driven) impulsivity (Moore & Malinowski, 2009) and adequate coping strategies (Fuchs, Lee, Roemer, & Orsillo, 2013).
Mindfulness has been defined as “. . . paying attention in a particular way; on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1990). Several mindfulness intervention programs are in use in prison and nonprison settings, with differences between them in, for example, the type of exercises or duration of the intervention (Baer, 2003; Chiesa & Serretti, 2009), but generally their starting points comprise the components of mindfulness as defined above. The mindfulness-based stress reduction (MBSR) intervention is designed to link the Buddhist tradition of Mindfulness with contemporary insights into neurobiological and behavioral functioning, and was developed by Jon Kabat-Zinn in the 1980s (Kabat-Zinn, 1990). MBSR intervention was shown to have positive effects, in both community and clinical populations, on physical health (Barrett et al., 2012), anxiety level (Coelho, Canter, & Ernst, 2007), stress responsivity (Chiesa & Serretti, 2009), and relapse after depression (Ma & Taesdale, 2004).
With respect to relevant outcomes for incarcerated populations (as described above: self- esteem, stress responsivity, and emotion perception and regulation), a number of positive results were obtained with mindfulness and meditation interventions in general, and on a number of occasions with MBSR in particular. Regarding stress responsivity, clear and consistent effects of the MBSR intervention have been found, also after a short duration of intervention (e.g., Baer, 2003; Nyklíček & Kuijpers, 2008). Studies indicated, besides self-reported decreases of stress, also a decline in biological stress reactivity (e.g., a decreased level of blood pressure reactivity) after mindfulness intervention (Nyklíček, Mohammersteeg, Van Beugen, Ramakers, & Van Boxtel, 2013). One can imagine that this decrease in stress reactivity is related to a better regulation of emotions. In that way, mindfulness can function as an emotion regulation strategy (Bottaccioli, Bottaccioli, & Minelli, 2018). Evidence from studies into depression, anxiety, and PTSD, which are all characterized by abnormalities in stress responsivity and emotion regulation, supports this hypothesis (Hofmann, Sawyer, Witt, & Oh, 2010). Decreased levels of anxiety and worrying in a nonclinical sample (C. Robins, Keng, Ekblad, & Brantley, 2012), and decreased PTSD symptomatology in Vietnam War veterans (Polusny et al., 2015) were reported specifically after the MBSR intervention. With respect to emotion regulation, mindfulness intervention has predicted greater clarity about which emotions are felt (Hill & Updegraff, 2012), greater voluntary exposure to aversive stimuli (Arch & Craske, 2006, 2010), a faster recovery from aversive experiences (Broderick, 2005; Cioffi & Holloway, 1993), and less aggression after social exclusion (Heppner et al., 2008).
Effects of different meditation and relaxation programs have also been studied before in prison settings (for reviews, Auty, Cope, & Liebling, 2017; Himelstein, 2011; Lyons & Cantrell, 2015; S. Simpson, Mercer, Lawrence, & Wyke, 2018). First, studies investigated the effectivity of Transcendental Meditation (TM; meditation, repetitions of a mantra and yogic practices) in male inmates, incarcerated for narcotics-related crimes. Orme-Johnson and Moore (2003) found a decrease in obsessive-compulsive behavior and social introversion as well as an increased stability in the autonomic nervous system (indicating lower stress levels) after TM. Rainforth and Alexander (2003) and Alexander et al. (2003) found reductions of risk of recidivism in TM groups of male prison inmates.
Another form of meditation, the Vipassana 10-day meditation retreat, was also studied in several groups of inmates. Chandiramani, Verma, and Dhar (1995) found decreases in anxiety, hostility, and depressed feelings, and an increase of feelings of hope and well-being. Bowen and colleagues (2006) found a decrease of alcohol- and drug-use and psychiatric symptoms as well as increases in optimism and internal locus of control following Vipassana meditation in five male and four female meditation groups. These results were partly replicated by T. Simpson et al. (2007), who also found decreased use of alcohol and drugs, but no reduction of PTSD symptoms in a group of inmates (predominantly men). Interviews with male prisoners after participating in a Vipassana course showed a positive impact on the atmosphere in prison: they reported more positive relationships with the prison staff, a more positive social atmosphere, and more perceived goodness (Ronel, Frid, & Timor, 2011).
One study specifically examined MBSR in prison inmates. Samuelson, Carmody, Kabat-Zinn, and Bratt (2007) investigated the effects of MBSR in six prisons in Massachusetts. Results of this questionnaire-based study showed a decrease in hostility, an increase in self-esteem, and a reduction of mood problems.
Aims of the Study
The present study had two aims. First, to determine the level of satisfaction with the MBSR intervention in prison settings in the Netherlands, and to determine the presence of potential challenges in the execution of the intervention. Second, to address relevant outcomes of the MBSR-intervention, that is, the perceived impact on psychological functioning. Based on the literature, improvements in self-esteem, mood, coping, emotion- and stress-regulation, and impulse control were hypothesized as a result of the MBSR intervention.
Method
Participants
Twenty-five inmates from five of the six prisons in the Netherlands where the MBSR intervention is carried out were approached with a request for participation in the study. Inmates were randomly selected from a list of 69 inmates, who attended the intervention and were still in prison. This list was provided by the MBSR instructors. Three individuals did not participate because they feared loss of anonymity (response rate = 88%). The 22 prisoners were all men (because the intervention had only been carried out in all-male prisons) and had a mean age of 40.1 years (SD = 11.1; range = 23-55). The majority (59%) had a Dutch ethnic-cultural background. Other frequent ethnic cultural backgrounds were Antillean (14%) and Moroccan (9%). Convictions resulting in detention were for murder (24%), manslaughter (24%), sexual offenses (19%), drug offenses (19%), robbery with violence (10%), and illegal restraint/kidnap (5%). The duration of incarceration was calculated from the day the inmates entered the prison, until the day of data collection, and varied from 15 to 209 months (M = 5.5 years; SD = 3.8). Unfortunately, no information is known about psychiatric disorders, as psychiatric screening is not yet a standard procedure in Dutch prisons.
From every correctional facility two prison staff members were asked about their experiences with the intervention. All randomly selected staff members were willing to participate (response rate = 100%). The 10 staff members (6 men, 4 women) had three different functions in the correctional facilities: five were mentors, three were motivational coaches, and three were case managers. Mentors are guards who help inmates with a number of practicalities (e.g., obtaining a valid passport), and they provide support with execution of Detention and Reintegration (D&R) plans. When people start with their D&R plan, they receive a motivational intervention, offered by one of the motivational coaches. Case managers assist in organizing reintegration and aftercare for inmates. Case managers also play an important role in the preparation and implementation of the D&R plan. The age of the prison staff varied from 45 to 61 years (Mage = 52.5 years; SD = 4.3).
The MBSR intervention was offered by four different instructors, and they were asked about their experiences with the MBSR intervention as well. All instructors had experience working with prison inmates. Two of them were men and two women (Mage = 48.0 years; SD = 10.0; range = 33-54).
Design
This study had a retrospective pretest–posttest design. Prison inmates were asked, after completion of the MBSR intervention, about their experiences with the intervention, and about differences in their mental states and feelings before and after the intervention. The intervention, which lasted 8 weeks, was administered by four MBSR instructors. The instructors and prison staff were also interviewed and asked about their (practical) experiences with the intervention. They were also asked whether they had observed changes in the participants regarding stress responsivity, self-esteem, coping strategies, emotion regulation, and impulse control.
Procedure
Participants were informed about the aim and method of research. The confidentiality of the conversation and anonymity of participation was also explained. The participants were asked for permission for the interview, and they signed an informed consent. All interviews were conducted by one interviewer (N.B.) and a research assistant in a separate room to allow participants to speak freely. The duration of the interviews ranged from 45 to 60 min. The questionnaire was orally administered and filled out on the interview form on the spot. Interviews were audio recorded and literally transcribed afterwards by a group of research assistants, to check the quantitative data and to analyze the qualitative data.
The study was approved by the Dutch Department of Correctional Institutions of the Ministry of Justice and Security. Participation was voluntary, and in line with guidelines for scientific research in prison detention, no reward was granted.
Intervention: MBSR
The original MBSR intervention (Kabat-Zinn, 1990) was adapted by the MBSR instructors to the prison settings. MBSR is an intensive intervention program using different mindfulness exercises (body scans, object and breathing meditation exercises, and slow movement yoga exercises). Compared with the original instructions, in the prison setting there were fewer participants per course, sessions had a shorter duration (with a maximum of 2 hr instead of two and a half hours), and debriefing after the exercises took place in groups rather than in pairs. The intervention consisted of an eight-week program where participants met every week in group sessions. Furthermore, participants received homework assignments aimed at practicing mindfulness for 6 days a week, 45 min/day, throughout the course of the intervention. The homework assignments consisted of body scan exercises, meditation exercises with CD instructions (formal exercises), and pen-and-paper assignments (informal exercises, such as the writing down of positive experiences every evening). In contrast to the original instructions, no silence day was held because of institutional limitations. Participants voluntarily attended the MBSR intervention. They were approached by the instructors or other staff members to participate. All MBSR instructors were academically trained, certified, and registered in the national database of MBSR instructors.
Measures
Interviews
This study was performed using semistructured interviews in two versions: an interview for prison inmates and an interview for prison staff and instructors. The inmate interview included questions about (adherence to) the intervention program (e.g., “Did you receive the necessary materials for the intervention?” and “After each meeting you get homework. How often have you done this homework?”), as well as motivation for and satisfaction with the MBSR intervention (e.g., “How would you rate the MBSR intervention/MBSR instructors?”). Answers to these questions were quantified through the use of rating scales from 1 (very negative) to 10 (very positive). In open (i.e., qualitative) questions, the inmates were asked about the reasons for their rating. Inmates were also asked about challenges during the intervention (e.g., “Did you notice problems in the room where the intervention was carried out?”).
In addition, the inmate interview included questions about changes in different (psychological) domains following the intervention: anger, experienced stress, impulse control, coping strategies, and self-esteem. Participants were asked how often they felt angry and how often they felt stressed before and after the MBSR intervention. They could choose from five categories: (a) never, (b) occasionally, (c) on a monthly basis, (d) on a weekly basis, and (e) on a daily basis. Participants were also asked to rate the intensity of these emotions on a continuous scale from 1 to 10 about the situation before and after the intervention (e.g., “How angry/stressed were you before you started the intervention on a scale of 1 (almost not angry/not stressed) to 10 (very angry/very stressed)?” and “How angry/stressed are you now on a scale of 1 (almost not stressed/angry) to 10 (very angry/stressed)?”).
Items from validated questionnaires were selected to assess anger, stress, and impulse control:
For experienced anger, two items of the Aggression Questionnaire (AQ) were used (Buss & Perry, 1992; Meesters, Muris, Bosma, Schouten, & Beuving, 1996): “I have trouble controlling my anger” and “I feel angry and irritated.”
Five items of the Depression, Anxiety and Stress Scale (DASS) were used to measure experienced stress (Lovibond & Lovibond, 1995), for example, “I found it difficult to relax” and “I felt bad and guilty.”
To measure impulse control, six items of the Barratt Impulsiveness Scale (BIS) were used (Barrat, Monahan, & Steadman, 1994). Examples of these items are “I have racing thoughts” and “I am self-controlled.”
Participants were asked whether they rated these items as worse (score = 1), the same (score = 2), or better (score = 3) after following the MBSR intervention.
To measure coping, participants indicated which coping strategy they generally tended to use before and after the intervention (choose one out of four). It was assessed whether they used a cognitive (problem-)oriented or an emotion-oriented coping style. “Relaxation” and “finding solutions” are cognitive coping strategies, which have been related to adaptive outcomes, and “anger” and “silent or sadness based” coping strategies are emotional coping strategies, which have been related to maladaptive outcomes (Kato, 2015).
To measure self-esteem, participants rated their level of self-esteem on a continuous scale from 1 to 10 before and after the MBSR intervention (R. W. Robins, Hendin, & Trzesnieuwski, 2001).
The interviews for the prison staff and MBSR instructors also consisted of two parts. First, (qualitative) questions about their experiences with the MBSR program were asked. Second, questions were asked about their impressions of behavioral changes in the group of participants as a whole after the intervention. Questions were about the same (psychological) domains as those in the inmates’ interview (anger, experienced stress, impulse control, coping strategies, and self-esteem), and answers were quantified using the rating on a 5-point scale (1 = strong decline, 2 = some decline, 3 = neutral, 4 = some progress, 5 = strong progress).
Demographic information of inmates
Background data (age, ethnic cultural background, duration of detention, and reason for detention) were collected from the inmates’ files.
Data Analysis
The sociodemographic data and data about adherence, motivation, and satisfaction during the intervention were analyzed using descriptive statistics, and quotations were used to illustrate these descriptive results, and to illustrate the challenges during the practical implementation of the intervention. For the outcomes of the intervention, quantified questions from the interviews were analyzed using nonparametric statistical tests for the paired sample categorical data (to compare the frequency of felt angriness and stress before and after MBSR, and to compare the coping styles before and after MBSR), paired sample t tests for the paired sample continuous data (to compare intensity of anger and stress before and after MBSR, and to compare the level of self-esteem before and after MBSR), and one-sample t tests were used to measure reported changes after MBSR on domains from MBSR instructors and prison staff, for the whole group (so the instructors and prison staff together), and for both separate groups; as test value 3.0 was used, which indicated “neutral” on a 5-point scale ranging from strong decline (=1) to strong progress (=5). Descriptive statistics were used to report categorical data (reported changes after MBSR on validated items of questionnaires, concerning anger (AQ), stress (DASS), and impulse control (BIS) from MBSR participants).
Results
Adherence, Motivation, Satisfaction, and Challenges During Intervention
Eighty-two percent of the participants attended all the sessions, and all of them completed the intervention. Absence from sessions was due to the following external factors: visit of lawyers or family members, illness, sports activities, or work. Prisoners rated their motivation to attend the MBSR’s first session with a mean of 7.3 (SD = 2.6; range = 1-10). The main reason for participating in the intervention was “learn to deal with problems and stress”. One related quotation is as follows:
It is mainly that I just have a moment to just relax. And then, when I walk away again after the training, I come back on the block, and there it is just as always, chaos. But you’ve been relaxed for a while. (Participant D5)
All participants reported that they received a homework map and a CD at the start of the intervention. Sixty-four percent of participants reported that all the homework exercises were done (see Figure 1). Reasons for doing the homework were curiosity about the homework exercises and the wish to be informed about all aspects of the training (see Table 1 for quotations). Reported reasons for not doing the homework exercises were the following: difficulty to find time, level of difficulty of the exercises, being busy with other things, being tired, or lack of motivation.
Figure 1.
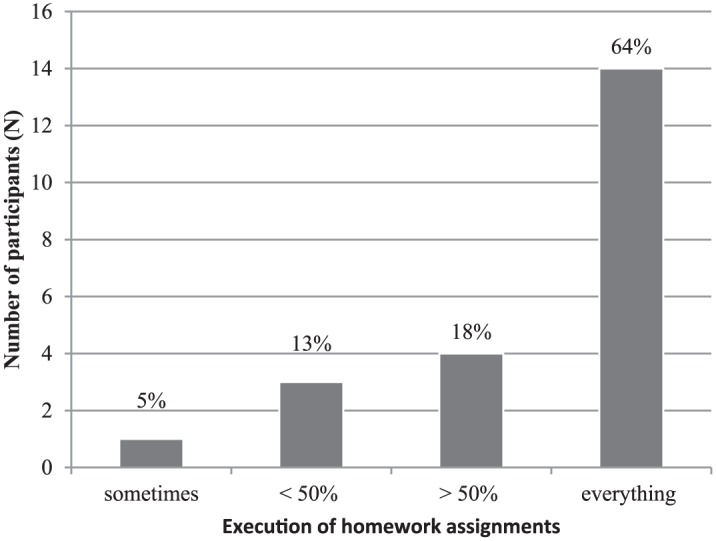
Executed homework assignments.
Table 1.
Reasons for Doing Homework Exercises.
| Examples of quotations |
|---|
| “But curiosity comes with it. I was curious what kind of influence the exercises would have. What exactly it means.” (Participant D14) |
| “Because I was curious, and I wanted to know what mindfulness exactly is. Also because I was on double cell with my brother, I did the training together with him. If I did not feel like it, he came up with something and then you tried to do it together.” (Participant D14) |
| “Just to get information. How can I best relax?” (Participant D9) |
| “I just did that because I felt a bit of . . . a bit under pressure like that. Tension. Too much tension. Bit nervous.” (Participant D19) |
With respect to the general appreciation of the MBSR intervention, participants gave it an average score of 8.7 (on a scale of 1-10; SD = 1.1; range = 6-10). The following aspects are mentioned as reasons for their ratings of the MBSR intervention: “it helps to calm down,” “to stop the thought flow,” and “it helps to relax.” Participants liked different exercises of the intervention, as shown in Table 2, and reported more awareness, greater capacity to observe themselves, and more relaxation as a result of the intervention (see Table 3 for illustrating quotations).
Table 2.
Exercises During the Mindfulness-Based Stress Reduction Intervention.
| Examples of quotations |
|---|
| “I really liked the body scan. And also another exercise . . . then we received a raisin, I held it in my hands . . . I don’t know if that was really an exercise. I had to capture the taste and smell, and then I had to observe what exactly was going on, I thought that was really a good exercise.” (Participant D9) |
| “I liked the exercise when I should lie down and the exercise where I just had to sit quietly and watch my breathing. Those two are the best.” (Participant D4) |
| “The best is just meditation, we always did that in the beginning and at the end of the training. I think that’s the best. But also because then you try, then you are very busy with just emptying your head, and just sit. And then all the thoughts come into my mind, and then I notice that, and I become distracted, and then I return to focusing my breathing. That is why the breathing is so important and helpful, and that’s why I always come back to where I am at that moment.” (Participant D8) |
Table 3.
General Evaluation of the Mindfulness-Based Stress Reduction Intervention.
| Examples of quotations |
|---|
| “I just internalized it. It is not really that I am working on it every day, but I do have it in my mind, I can deal with things differently, and don’t act in the same way I did before the training. It is better to observe things.” (Participant D4) |
| “For me it is just yes, the rest that I can find there, that is the most important thing for me. So you can just think clearly and not do things . . ., because you have so much going on in your mind, do things that you should not do, because otherwise things can go wrong. That was the reason I went there finally.” (Participant D8) |
| “For example, I sit on a bed or on a chair and I do nothing. If you do that for an hour, you will become aware of yourself every time. And you also notice that every time you become aware of yourself, you have a different face. Sometimes you are happy, the next time you are angry, then you are afraid. So that’s really something important, because I want to get to know myself very well.” (Participant D16) |
| “Attention, to keep your focus somewhere. In the past, I was very restless, for example when I heard those keys outside, I wanted to see who was outside, which keys they had. Were they guards or inmates? I really had that, an example from inside the prison. Outside I had that too, at school I always had to sit in front of the class, because when I was in the back of the classroom, I was more concerned with people who were around me than with the lesson.” (Participant D18) |
| “That I have gained a bit more self-control and control over myself.” (Participant D21) |
| “Rest and self-awareness. Yes. And do not judge myself so hard anymore.” (Participant D23) |
Participants evaluated the MBSR instructors with an average score of 9.3 (SD = 0.8; range = 7-10). Strong qualities of the instructors included that “they were interested,” “were able to communicate with and promote togetherness of different types of participants,” and that they were “calm and professional.” The participants indicated that attention could be given to the improvement of the homework assignments and the CD: three participants found the language used to explain the exercises too difficult.
MBSR instructors and prison staff all reported positively about the feasibility of the intervention in prison settings. The certified MBSR instructors all said they could readily apply the adapted protocol based on the MBSR manual of Kabat-Zinn (1990). The MBSR instructors reported that a mindfulness-based intervention added to existing interventions in prison that the focus of MBSR is more on experience of feelings, and making a connection between the body and the mind (see Table 4).
Table 4.
Instructors About the Added Value of Mindfulness-Based Stress Reduction in Prison.
| Quotations |
|---|
| “We start at the beginning of a road that involves recovery for inmates and for the road to a life that is less harmful to the inmates themselves and to others. . . . The starting point is the whole person . . . The whole atmosphere is one of appreciation for the person you are and it is very experiential.” (Instructor T1) |
| “The biggest difference is that with this training you just feel where you are, and you are not told where to go. You become aware of where you are. I find it valuable and a big difference that we do not tell people where they have to be at the end of eight weeks. The participants can find out themselves where they will be in eight weeks . . . I think that is really a valuable addition for people who, in the past, often had very unsuccessful experiences. . . . And that we are going to become aware of this: yes, it has failed and that hurts. We look at how things are going and how things can also be different and that you can discover this change.” (Instructor T2) |
| “The training focuses on experience level, which is really a different approach path. The cognitive abilities and the self-reflective ability of the inmates are often not very well-developed. They often avoid contact with what they actually feel and experience. So that level of experience is a huge addition.” (Instructor T3) |
| “An added value in this training is that it involves a physical component and that is quite unique. That brings your body and mind together, I don’t know any other method that does that in the context of a prison. So here you really have a variety of bodywork, communication and introspection. That is a total method that covers all areas . . . There is no achievement required either, we just do our exercises, and you feel your own limits, that is a mildness that is truly unique for this training.” (Instructor T4) |
Instructors, prison staff, and inmate participants also mentioned some challenges of the intervention. Most of the inmates could be on time for the start of the sessions (91%). The inmates who could not be on time indicated that they were not released from their cells or department on time. An instructor mentioned as follows:
People are not released from their department, the door is not opened. Or participants are at work and the staff there is not informed. Or the staff do not want to let them go. I often hear from participants: “they have not opened my door again.”
Guards don’t recognize this issue, but reported that the program of inmates is often full with activities:
The current day program actually has only a few hours in which activities of inmates can take place, and in those five hours there are a lot of things to do. For example, the inmate has to speak to the case manager or organize his release or do something else, and all these activities need to be performed in those few hours. (Respondent S10).
Thirty-six percent of the participants indeed mentioned that the intervention overlapped with other activities such as work obligations and sports activities. Other reported challenges during the intervention were noise in the rooms for group sessions of the MBSR intervention: Participants reported that because of these sounds of alarms and running guards it was sometimes difficult to concentrate. One participant quotes,
Sometimes I heard a lot of noise during an exercise from the other inmates . . . of from other fellow participants of the training. That was sometimes a problem. It could even have been a bigger problem if they had come into the room where we did the training, but that did not happen. (Participant D1)
Also, lack of availability of CD players for exercising mindfulness in their own cell was reported. Group composition was a central challenge for both the inmates and the staff in prison: inmates from different departments within prison meet each other during the intervention. Some prisoners indicated that they did not want to train in the same group as sex offenders. Prisoners also encountered persons with whom they had conflicts inside or outside prison, which could cause tension during the MBSR intervention (see Table 5 for participants’ quotations that illustrate this issue). The MBSR instructors and prison staff reported the same challenges, and added that continuity in offering the intervention may also be a problem, because of a lack of manpower to facilitate and provide the MBSR intervention.
Table 5.
Challenges of Group Composition (According to Participants).
| Examples of quotations |
|---|
| “I sometimes meet people whom I myself, yes, helped to another department rather ‘unkindly’. I have had a fight with someone who has been sent to another department, but we do meet each other during the training, for example . . . I am not going to fight during the training, but you will meet everyone.” (Participant D8) |
| “I had no affinity with those people, there were many people I did not know. All of them, those cool people. That is not a familiar group for me.” (Participant D23) |
| “Yes, we did have a clash between two departments. There happens to be such a guy, such a type. The type I do not want to meet. I wanted to avoid problems. I’m not looking for a fight. But that guy is a bit of a weird guy. Thinking of him being there, sometimes I thought, yes, I better not go. But I went anyway, because I do not get involved with him. He does not interfere with me, so yes. But it feels normal. Despite that there was no communication between us. I know him.” (Participant D21) |
Psychological Outcomes
Effects Perceived by Inmates
Anger
Inmates reported a significant decrease in the frequency of experienced anger before the intervention (Mdn = 3.0), compared to the frequency after the intervention (Mdn = 2.0; z = −2.151, p = .031): Compared with the experienced anger before the intervention, they more often reported feeling not or only occasionally angry (18%/23% before the intervention versus 23%/45% after the intervention), and fewer inmates reported being angry on a daily (18% before the intervention versus 9% after the intervention), weekly (27% before the intervention versus 14% after the intervention), or monthly basis (14% before the intervention versus 9% after the intervention). Also the intensity of anger decreased: Before the intervention the inmates reported a mean intensity of 6.6 (SD = 1.7) on a scale of 0 to 10, in contrast with a mean intensity of 5.4 (SD = 1.9) after the intervention, t(15) = 2.30, p = .036, Cohen’s d = .69. Furthermore, inmates were asked whether they felt they could handle anger worse (score = 1), the same (score = 2), or better (score is 3) after the intervention on two items of the AQ. None of the inmates reported that their ability to handle anger and to calm down had become worse (0%) after the intervention, 25% of the participants reported that they were able to handle anger the same, and 75% reported could handle this better after the intervention.
Stress responsivity
Inmates reported no significant difference in the frequency of experiencing stress before the intervention (Mdn = 4.0), compared to the frequency after the intervention (Mdn = 3.0), z = −1,458, p = .145. However, the intensity of experienced stress did decrease after the intervention: Before the intervention the inmates reported a mean stress intensity of 7.5 (SD = 2.3), and after the intervention a mean intensity of 5.4 was reported, SD = 2.7; t(18) = 4.16, p = .001; Cohen’s d = .82. None of the participants reported a negative change on validated items of the DASS after attending the intervention (self-acceptance, relaxation, experienced fear, experienced guilt and depression). Averaging across DASS items, over half of the participants (51%) reported a positive change after the intervention, with the remaining participants (49%) reporting no change. See Table 6 for the percentages per item.
Table 6.
Self-Reported Effect of the Intervention on Internalizing Symptoms (n, %).
| Self-acceptance | Relaxation | Anxiety | Feel guilty | Feel depressed | Average % | |
|---|---|---|---|---|---|---|
| No effect of intervention | 11 (50%) | 5 (23%) | 13 (59%) | 11 (50%) | 14 (64%) | 49 |
| Effect of intervention | 11 (50%) | 17 (87%) | 8 (36%)a | 11 (50%) | 8 (36%) | 52 |
Note. N = 22.
One missing value.
Impulse control
Participants answered items of the BIS on impulsive actions, paying attention, careful planning, decision making, racing thoughts, and lack of control. Averaging across the BIS items, over half of the participants (52%) reported a positive change in impulse control after the intervention, with the remaining participants (48%) reporting no change. See Table 7 for the percentages per item.
Table 7.
Self-Reported Effects of the Intervention on Impulse Control (n, %).
| Impulsive actions | Paying attention | Careful thoughts | Decision making | “Racing” thoughts | Perceived control | Average % | |
|---|---|---|---|---|---|---|---|
| No effect of intervention | 8 (36%) | 10 (45%) | 15 (68%) | 14 (64%) | 9 (41%) | 7 (32%) | 48 |
| Effect of intervention | 14 (64%) | 12 (55%) | 7 (32%) | 8 (36%) | 13 (59%) | 15 (68%) | 52 |
Note. N = 22.
Coping
Inmates were asked about their coping strategies before and after the intervention (cognitive vs. emotion-oriented coping styles). Results showed that, following the MBSR intervention, participants were more likely to seek solutions (50% before vs. 68% after the intervention), and less often reacted with angry behavior (14% before vs. 5% after the intervention). They also reported to be more relaxed in stressful situations (9% before vs. 23% after the intervention), and less likely to be silent or sad (27% before vs. 5% after the intervention) (see Figure 2). When the cognitive versus emotion-oriented coping styles were combined, McNemar’s test showed that there was a significant difference in the use of coping styles after the intervention (p = .016): Inmates reported that they used more cognitive-oriented coping styles and less emotion-oriented coping styles after the intervention.
Figure 2.

Coping strategies before and after intervention.
Self-esteem
Inmates retrospectively reported a mean of 7.4 (SD = 2.3) on a scale of 0 to 10 for their self-esteem before the intervention. After intervention, they marked their self-esteem a 8.3 (SD = 1.2). This was a significant increase, t(21) = 2.82, p = .010, Cohen’s d = .53.
Effects (on Inmates) Perceived by Prison Staff and Instructors
Instructors and prison staff were also asked about perceived behavioral changes in the entire group of MBSR participants (behavioral changes in individual participants were not assessed). The different domains were rated on a 5-point Likert-type scale (1 = strong decline, 2 = some decline, 3 = neutral, 4 = some progress, 5 = strong progress). Instructors and prison staff reported a significant progress on all domains after attending the MBSR intervention (see Table 8 for M %, t values, degrees of freedom, and p values).
Table 8.
Average Ratings of Perceived Behavioral Change in Group of Mindfulness-Based Stress Reduction Participants (M %), and Results of One-Sample t Test.
| Prison staff (n = 9, Missing Value = 1) |
Instructors (n = 4) |
Average of combined ratings (n = 13) | Results One-sample t testa |
|
|---|---|---|---|---|
| Experienced stress | 4.22 | 4.63 | 4.35 | t(12) = 7.76, p < .001 |
| Self-esteem | 4.00 | 4.25 | 4.08 | t(12) = 5.11, p < .001 |
| Emotional stability | 3.88 | 3.75 | 3.85 | t(12) = 5.50, p < .001 |
| Dealing with difficult emotions | 4.11 | 3.88 | 4.04 | t(12) = 5.20, p < .001 |
| Problem-solving skills | 4.00 | 3.50 | 3.85 | t(12) = 3.94, p = .002 |
| Anger | 4.33 | 4.13 | 4.27 | t(12) = 7.64, p < .001 |
| Aggressive behavior | 4.11 | 3.75 | 4.00 | t(12) = 5.10, p < .001 |
| Aggression regulation | 4.11 | 4.13 | 4.12 | t(12) = 5.24, p < .001 |
| Hostility | 4.00 | 3.63 | 3.88 | t(12) = 3.89, p = .002 |
| Overall behavioral change | 4.08 | 3.96 | 4.05 |
Test value = 3.0.
Discussion
Mindfulness-based intervention has been gaining popularity in the last few decades. Generally, it appears to have beneficial effects, mainly by reducing suboptimal stress responsivity, but also through transfer effects related to self-esteem, emotional responsivity, and impulse control. Prison populations were shown to have increased difficulties with these aspects of psychological and social functioning (Van Wijk et al., 2011), and may therefore strongly benefit from mindfulness-based interventions. However, scientific studies into the effects of mindfulness training in prison populations are still rare. The specific constraints and circumstances in prison settings have not yet been comprehensively mapped either. The present study is the first study in Europe to determine both the feasibility of MBSR intervention in detention and the possible effects of MBSR on the psychological functioning and well-being of inmates.
Findings provided a clear picture: In general, participating inmates were very positive about the intervention, as were instructors and involved prison staff members (guards, motivational coaches, and case managers). These findings provide an empirical basis to further expand the (study of) MBSR intervention in prison settings, in both male and female groups and for prisoners with shorter and longer incarceration times. Study participants (instructors, prison staff, and inmates) do however point out several logistic issues that need to be taken into account when a program such as MBSR is implemented in prisons. The most important issue is the limited sharing of background knowledge and goals of the intervention among all involved staff members. For example, guards must more emphatically be made aware that this intervention program is not only important for the well-being of the participants, but potentially also has important benefits for society, so that they will be more motivated to facilitate (timely) participation in the group sessions. Moreover, of all staff members, guards are generally those who are best informed about the sensitivities of individual inmates, and therefore can signal in advance potential difficulties to be expected during the intervention, for example, when putting certain inmates together in one intervention group. Participants also reported practical issues regarding the MBSR intervention: CD players were not always available, and for some participants the language used to explain the homework exercises was too difficult. Instructors could pay more attention to adapting the level of all instructional material to address these difficulties. As we know from earlier studies, mild intellectual disability is relatively common in inmate populations, which is an issue that should be taken into account when selecting and offering particular interventions (Kaal, 2011).
Regarding the beneficial outcomes following the intervention, we were able to assess a number of primary outcomes, that is, self-esteem, stress responsivity, anger, anxiety/depressions, coping mechanisms, and emotion-driven inhibitory control. We found that beneficial effects of MBSR were reported for all these important psychological domains underlying social-adaptive behavior and psychological well-being, both reported by participants of the MBSR intervention themselves, and by the instructors and prison staff. These findings are in agreement with those of many studies showing multifactorial benefits of mindfulness-based interventions for different clinical and nonclinical populations, and they also confirm and extend the findings from Samuelson and colleagues (2007), who, to our knowledge, are the only other group examining MBSR in prison settings.
For this population, it would also be of great importance to establish how the effects of MBSR translate into (less) criminogenic cognitions and societal outcomes after imprisonment (secondary and long-term effects). Whereas the first results on translational effects generally appeared positive, a nuanced approach seems to be required. For example, a recent study showed that nonjudgment of self (a core component of mindfulness) was positively related to more criminogenic cognitions (Tangney, Dobbins, Stuewig, & Schrader, 2017). Thus, certain components of mindfulness intervention may inadvertently have negative effects when translated to societal outcomes. Moreover, there appears to be a lack of consensus about which behavioral factors or psychological phenomena are (mindfulness-specific or generic) mechanisms rather than outcomes or vice versa. To facilitate research into the effectiveness of mindfulness intervention, we suggest to make clearer distinctions between (a) core mindfulness mechanisms (Present Awareness, Metacognition, Quiet Mind, Willingness and Acceptance, Nonjudgment of Self, Nonjudgment of Others; Brown & Ryan, 2003; Tangney et al., 2017); (b) intermediate outcomes, such as emotion- and stress-regulation; and (c) personal, social, and societal outcomes, that is, personal well-being, adaptive social behavior, and constructive social participation.
Obviously, the study presented here also has a number of limitations. One of these is that we did not follow the theoretical framework proposed above ourselves, that is, we did not assess core mindfulness mechanisms, and could not assess societal outcomes as participants were still incarcerated. It would be good to include an assessment of core mindfulness mechanisms in future studies because of their possible direct links with the psychological constructs where we found such strong effects. Another possible limitation is that data were obtained through interviews (rather than, for example, direct observations or performance on (neuro)cognitive stress tasks). Furthermore, circumstances allowed only for a retrospective design rather than a preferred pre- post-test design with a control group (without intervention or a comparable intervention). This also influenced the materials we worked with: As we wanted to measure change in several psychological constructs following the MBSR intervention, we had to adapt the answer formats of the questions that were asked. Also, the small sample size of the study could lead to underpowered statistical tests and an increased likelihood of type 1 error. Furthermore, little information was known, or could be retrieved, about the background of the prisoners (e.g., the level of psychiatric symptoms, etc.). However, it should be noted that this is only the second study that has used a scientific approach to evaluate MBSR in a prison setting. Another strong point of the study is that it gave a voice to incarcerated individuals, which is very scarce in scientific research.
More research is needed to gain further insight into the mechanisms underlying the apparent beneficial effects of MBSR training in prison settings and into long-term effects of MBSR training. Future research in incarcerated populations should investigate core mindfulness mechanisms, cognitions, emotion- and stress-regulation, and social and societal outcomes in a more structured and comprehensive fashion, both theoretically and regarding the study design and choice of instruments for assessment. Regarding the latter, the simultaneous use of multiple methods (questionnaires, interview, neuropsychological tasks, but also, for example, neurobiological markers associated with stress responsivity) may be preferable. Psychosocial functioning (e.g., peer relationships, romantic relationships, hierarchical relationships in work context, but also presence of psychopathology) and societal outcomes indicating constructive social participation (e.g., employment, socioeconomic status, and recidivism) deserve special attention. Sample sizes must be large enough to also investigate the effects of mindfulness intervention in different groups of inmates. Factors that might influence intervention success include duration of incarceration, presence of different psychiatric disorders, exposure to trauma, presence of mild intellectual disabilities, High Impact Crime status, and presence of psychopathy, which were all issues that could not be addressed in the present study due to administrative and logistical constraints.
To conclude, this study aimed to determine the motivation for and satisfaction with the MBSR intervention in a prison setting and to investigate changes in psychological outcomes following the intervention. It was found that inmates, MBSR instructors, and prison staff were satisfied with the intervention. Challenges were identified in practical issues, such as organization of the intervention sessions. Both participants of the intervention, and MBSR instructors and prison staff reported improvements in all investigated psychological domains.
Acknowledgments
The authors thank the participating inmates, MBSR instructors and prison staff, and research assistants. We are especially grateful to [Nelleke van Zessen] (MBSR instructor) who was very helpful in reaching the inmates, and by collecting the data.
Footnotes
Ethical Approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research and Documentation Centre of the Ministry of Justice and Security in the Netherlands.
ORCID iD: N. Bouw  https://orcid.org/0000-0002-4858-6085
https://orcid.org/0000-0002-4858-6085
References
- Alexander C., Rainforth M., Frank P., Grant J., Von Stade C., Walton K. (2003). Walpole study of the Transcendental Meditation program in maximum security prisoners: III. Reduced recidivism. Journal of Offender Rehabilitation, 36, 161-180. [Google Scholar]
- Arch J., Craske M. (2006). Mechanisms of mindfulness: Emotion regulation following a focused breathing induction. Behaviour Research and Therapy, 44, 1849-1858. [DOI] [PubMed] [Google Scholar]
- Arch J., Craske M. (2010). Laboratory stressors in clinically anxious and non-anxious individuals: The moderating role of mindfulness. Behaviour Research and Therapy, 48, 495-505. [DOI] [PubMed] [Google Scholar]
- Auty K., Cope A., Liebling A. (2017). A systematic review and meta-analysis of yoga and mindfulness meditation in prison. International Journal of Offender Therapy and Comparative Criminology, 61, 689-710. [DOI] [PubMed] [Google Scholar]
- Baer R. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10, 125-143. [Google Scholar]
- Barrat E., Monahan J., Steadman H. (1994). Impulsiveness and aggression. Violence and Mental Disorder: Developments in Risk Assessment, 10, 61-79. [Google Scholar]
- Barrett B., Hayney M., Muller D., Rakel D., Ward A., Obasi C. N., . . . Coe C. L. (2012). Meditation or exercise for preventing acute respiratory infection: A randomized controlled trial. Annals of Family Medicine, 104, 337-346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bilderbeck A., Farias M., Brazil I., Jakobowitz S., Wikholm C. (2013). Participation in a 10-week course of yoga improves behavioural control and decreases psychological distress in a prison population. Journal of Psychiatric Research, 47, 1438-1445. [DOI] [PubMed] [Google Scholar]
- Bonta J., Andrews D. (2003). Commentary on Ward and Stewart’s model of human needs. Psychology, Crime & Law, 93, 215-218. [Google Scholar]
- Bottaccioli A., Bottaccioli F., Minelli A. (2018). Stress and the psyche–brain–immune network in psychiatric diseases based on psychoneuroendocrineimmunology: A concise review. Annals of the New York Academy of Sciences, 1437, 31-42. [DOI] [PubMed] [Google Scholar]
- Bowen S., Witkiewitz K., Dillworth T., Chawla N., Simpson T., Ostafin B., . . . Marlatt G. A. (2006). Mindfulness meditation and substance use in an incarcerated population. Psychology of Addictive Behavior, 15, 343-347. [DOI] [PubMed] [Google Scholar]
- Broderick P. (2005). Mindfulness and coping with dysphoric mood: Contrasts with rumination and distraction. Cognitive Therapy and Research, 29, 501-510. [Google Scholar]
- Brown K., Ryan R. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84, 822-848. [DOI] [PubMed] [Google Scholar]
- Bulten E. (2009). Veel psychiatrische stoornissen onder gedetineerden op reguliere afdelingen van penitentiaire inrichtingen [High prevalence of psychiatric disorders among detainees in regular prisons]. Nederlands Tijdschrift Geneeskunde, 1, 6. [Google Scholar]
- Buss A., Perry M. (1992). The Aggression Questionnaire. Journal of Personality and Social Psychology, 63, 452-459. [DOI] [PubMed] [Google Scholar]
- Chandiramani K., Verma S., Dhar P. (1995). Psychological effects of Vipassana on Tihar Jail inmates: Research report. Igatpuri, India: Vipassana Research Institute. [Google Scholar]
- Chiesa A., Serretti A. (2009). Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. The Journal of Alternative and Complementary Medicine, 15, 593-600. [DOI] [PubMed] [Google Scholar]
- Cioffi D., Holloway J. (1993). Delayed costs of suppressed pain. Journal of Personality and Social Psychology, 64, 274-282. [DOI] [PubMed] [Google Scholar]
- Coelho H., Canter P., Ernst E. (2007). The effectiveness of hypnosis for the treatment of anxiety: A systematic review. Primary Care and Community Psychiatry, 12, 49-63. [Google Scholar]
- Davey L., Day A., Balfour M. (2015). Performing desistance: How might theories of desistance from crime help us understand the possibility of prison theatre? International Journal of Offender Therapy and Comparative Criminology, 59, 798-809. [DOI] [PubMed] [Google Scholar]
- Fischer T., Captein W., Zwirs B. (2012). Gedragsinterventies voor justitiabelen. STand van zaken en mogelijkheden voor innovatie [Behavioural interventions for convicted offenders: state of affairs and possibilities for innovation]. Den Haag, The Netherlands: WODC. [Google Scholar]
- Fogel C. (1993). Hard time: The stressful nature of incarceration for women. Issues in Mental Health Nursing, 14, 367-377. [DOI] [PubMed] [Google Scholar]
- Froggio G., Agnew R. (2007). The relationship between crime and “objective” versus “subjective” strains. Journal of Criminal Justice, 35, 81-87. [Google Scholar]
- Fuchs C., Lee J., Roemer L., Orsillo S. (2013). Using mindfulness- and acceptance-based treatments with client from nondominant cultural and/or marginalized backgrounds: Clinical considerations, meta-analysis findings, and introduction to the special series-clinical considerations in using acceptance-. Cognitive and Behavioural Practice, 20, 1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goff A. R. (2007). Does PTSD occur in sentenced prison populations? A systematic literature review. Criminal Behaviour and Mental Health, 17, 152-162. [DOI] [PubMed] [Google Scholar]
- Haney C. (2006). Reforming punishment: Psychological limits to the pains of imprisonment. Washington, DC: American Psychological Association. [Google Scholar]
- Heppner W., Kernis M., Lakey C., Campbell W., Goldman B., Davis P., Cascio E. V. (2008). Mindfulness as a means of reducing aggressive behavior: Dispositional and situational evidence. Aggressive Behavior, 34, 486-496. [DOI] [PubMed] [Google Scholar]
- Hill C., Updegraff J. (2012). Mindfulness and its relationship to emotional regulation. Emotion, 121, 81-90. [DOI] [PubMed] [Google Scholar]
- Himelstein S. (2011). Mediation research: The state of the art in correctional settings. International Journal of Offender Therapy and Comparative Criminology, 55, 646-661. [DOI] [PubMed] [Google Scholar]
- Hofmann S., Sawyer A., Witt A., Oh D. (2010). The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. Journal of Consulting and Clinical Psychology, 78, 169-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaal H. N. (2011). De problematiek van gedetineerden met een licht verstandelijke beperking in het gevangeniswezen [Challenges and difficulties of prison inmates with mild intellectual disabilities]. Den Haag, The Netherlands: WODC. [Google Scholar]
- Kabat-Zinn J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York, NY: Bantam Dell. [Google Scholar]
- Kato T. (2015). Frequently used coping scales: A meta-analysis. Stress and Health, 31, 315-323. [DOI] [PubMed] [Google Scholar]
- Kerekes N., Fielding C., Apelqvist S. (2017). Yoga in correctional settings: A randomized controlled study. Frontiers in Psychiatry, 8, 204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipsey M., Cullen F. (2007). The effectiveness of correctional rehabilitation: A review of systematic reviews. Annual Review of Law and Social Science, 3, 297-320. [Google Scholar]
- Lovibond S., Lovibond P. (1995). Manual for the Depression Anxiety Stress Scales. Sydney, New South Wales, Australia: The Psychology Foundation of Australia. [Google Scholar]
- Lyons T., Cantrell W. (2015). Prison meditation movements and mass incarceration. Internal Journal of Offender Therapy and Comparative Criminology, 60, 798-809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma S., Taesdale J. (2004). Mindfulness-based cognitive therapy for depression: Replication and exploration of differential relapse prevention effects. Journal of Consulting and Clinical Psychology, 72, 31-40. [DOI] [PubMed] [Google Scholar]
- Meesters C., Muris P., Bosma H., Schouten E., Beuving S. (1996). Psychometric evaluation of the Dutch version of the Aggression Questionnaire. Behaviour Research and Therapy, 34, 839-843. [DOI] [PubMed] [Google Scholar]
- Moffitt T., Krueger R., Caspi A., Fagan J. (2000). Partner abuse and general crime: How are they the same? How are they different? Criminology, 38, 199-232. [Google Scholar]
- Moore A., Malinowski P. (2009). Meditation, mindfulness and cognitive flexibility. Consciousness and Cognition, 181, 176-186. [DOI] [PubMed] [Google Scholar]
- Nyklíček I., Kuijpers K. (2008). Effects of mindfulness-based stress reduction intervention on psychological well-being and quality of life: Is increased mindfulness indeed the mechanism? Annals of Behavioral Medicine, 35, 331-340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyklíček I., Mohammersteeg P., Van Beugen S., Ramakers C., Van Boxtel G. (2013). Mindfulness-based stress reduction and physiological activity during acute stress: A randomized controlled trail. Health Psychology, 32, 1110. [DOI] [PubMed] [Google Scholar]
- Orme-Johnson D., Moore R. (2003). First prison study using the Transcendental Meditation program: La Tuna Federal Penitentiary, 1971. Journal of Offender Rehabilitation, 36, 89-95. [Google Scholar]
- Pankey T., Kelly P., Ramaswamy M. (2016). Stress reduction through a brief writing intervention with women in jail. Journal of Correctional Health Care, 22, 240-246. [DOI] [PubMed] [Google Scholar]
- Perkins R. (1998). The efficacy of mindfulness-based techniques in the reduction of stress in a sample of incarcerated women (Doctoral dissertation). Florida State University. [Google Scholar]
- Polaschek D. (2010. a). Treatment non-completion in high-risk violent offenders: Looking beyond criminal risk and criminogenic needs. Psychology, Crime & Law, 16, 525-540. [Google Scholar]
- Polusny M. A., Erbes C. R., Thuras P., Moran A., Lamberty G. J., Collins R. C., . . . Lim K. O. (2015). Mindfulness-based stress reduction for posttraumatic stress disorder among veterans: A randomized clinical trial. JAMA, 314, 456-465. [DOI] [PubMed] [Google Scholar]
- Rainforth M., Alexander C. C. (2003). Effects of the Transcendental Meditation program on recidivism among former inmates of Folsom Prison: Survival analysis of 15-year follow-up data; Journal of Offender Rehabilitation, 36, 181-203. [Google Scholar]
- Reibel D., Greeson J., Brainard G., Rosenzweig S. (2001). Mindfulness-based stress reduction and health-related quality of life in a heterogeneous patient population. General Hospital Psychiatry, 23, 183-192. [DOI] [PubMed] [Google Scholar]
- Robins C., Keng S., Ekblad A., Brantley J. (2012). Effects of mindfulness-based stress reduction on emotional experience and expression: A randomized controlled trial. Journal of Clinical Psychology, 68, 117-131. [DOI] [PubMed] [Google Scholar]
- Robins R. W., Hendin H. M., Trzesnieuwski K. H. (2001). Measuring global self-esteem: Construct validation of a single-item measure and the Rosenberg Self-esteem scale. Personality and Social Psychology Bulletin, 272, 151-161. [Google Scholar]
- Ronel N., Frid N., Timor U. (2011). The practice of positive criminology: A Vipassana course in prison. International Journal of Offender Therapy and Comparative Criminology, 57, 133-153. [DOI] [PubMed] [Google Scholar]
- Samuelson M., Carmody J., Kabat-Zinn J., Bratt M. (2007). Mindfulness-based stress reduction in Massachusetts correctional facilities. The Prison Journal, 87, 254-268. [Google Scholar]
- Shonin E., Gordon W., Slade K., Griffiths M. (2013). Mindfulness and other Buddhist-derived interventions in correctional settings: A systematic review. Aggression and Violent Behavior, 18, 365-372. [Google Scholar]
- Simpson S., Mercer S. S., Lawrence M., Wyke S. (2018). Mindfulness-based interventions for young offenders: A scoping review. Mindfulness, 9, 1330-1343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson T., Kaysen D., Bowen S., MacPherson L., Chawla N., Blume A., . . . Larimer M. (2007). PTSD symptoms, substance use, and Vipassana meditation among incarcerated individuals. Journal of Traumatic Stress, 20, 239-249. [DOI] [PubMed] [Google Scholar]
- Tangney J., Dobbins A., Stuewig J., Schrader S. (2017). Is there a dark side to mindfulness? Relation of mindfulness to criminogenic cognitions. Personality and Social Psychology Bulletin, 43, 1415-1426. [DOI] [PubMed] [Google Scholar]
- Van Wijk A., Schoenmakers Y., Manders A. (2011). Wapenfeiten; Een onderzoek naar overvallen en overvallers in Nijmegen [Robbers and robberies in the city of Nijmegen]. Arnhem, The Netherlands: Beke. [Google Scholar]
- Ward T., Day A., Howells K., Birgden A. (2004). The multifactor offender readiness model. Aggression and Violent Behaviour, 96, 645-673. [Google Scholar]