

Abstract
Background:
Extant literature suggests that a substantial portion of athletes may not report a possible concussion and that concussion knowledge is insufficient to predict concussion reporting behavior. One area that has not been explored is reporting skill; that is, mastery of the actions required to report a concussion. This study evaluated the relationship between reporting skill and reporting intention, introducing a measure of the reporting skill construct.
Hypotheses:
Reporting intentions will be more closely associated with reporting skill than with concussion/symptom knowledge. The relationship between concussion (or symptom) knowledge and reporting intentions will differ by level of reporting skill.
Study Design:
Repeated cross-sectional study.
Level of Evidence:
Level 2.
Methods:
A set of items was administered to young adults aged 18 to 24 years from the Survey Sampling International panel. Exploratory/confirmatory factor analyses were conducted on 2 waves of data to develop the scale (n = 899). Hypotheses were tested using structural equation modeling on the responses from the third wave of participants (n = 406).
Results:
Knowing the actions to take in reporting was more important than having knowledge of concussions or concussion symptoms. Reporting skill, not concussion or concussion symptom knowledge, was associated with higher intentions to report symptoms. Among those with higher levels of reporting skill, concussion symptom knowledge (but not general concussion knowledge) was associated with higher intentions to report symptoms.
Conclusion:
Reporting skill is an important and, until now, missing ingredient in the concussion literature and practice.
Clinical Relevance:
Incorporating reporting skill development in concussion education and team activities to teach athletes how to report is likely to improve actual reporting intentions. While further study is needed with particular sports and additional age groups, reporting skill holds promise as a new avenue for increased concussion reporting.
Keywords: concussion, reporting, skill, training
Sport-related concussion (SRC) is a complex injury that presents challenges in recognition and management.37 A critical element of recovery from a concussion is early reporting, meaning telling someone you are experiencing concussion-like symptoms as soon as they are felt. Early reporting and treatment mean a speedier return to play, learning, and life with a reduced risk of other injuries.3 Yet, studies suggest 50% or more of concussion symptoms are concealed by the individual, and a variety of sport settings7,26,33,36,39,40 describe the underreporting of concussion symptoms, which further complicates the ability to manage the effects of concussions.
There have been several efforts to encourage a greater reporting of possible SRC symptoms to ensure proper evaluation, diagnosis, and treatment.11,33,36 Underlying these efforts is the belief that greater explicit knowledge of concussions is the key to increased reporting. Most educational programs assumed that if athletes had greater knowledge of signs and symptoms as well as potential effects, they would be more likely to report suspected concussion symptoms. The result was a proliferation of educational programs designed to impart such knowledge.14,37,38 However, to influence reporting behavior, there needs to be a relationship between concussion knowledge and reporting.
While these programs showed mixed results in the relationship between concussion education and increased concussion knowledge among participants,20,30,34 the associations between increased explicit knowledge of concussion facts and improved reporting of concussion symptoms are limited.11,12 Several studies raise questions about the relationship between knowledge and greater SRC reporting.15,16,19 There is some suggestion that a broader conceptualization of knowledge may prove useful in the effort to improve reporting. Studies suggest that factors beyond concussion knowledge should be examined, such as the method by which the knowledge is transmitted (eg, training in context or taking a “procedural approach” to the education15,30) and the contextual support for acting on such knowledge (eg, perceived or group norms29,31,32). In addition, studies suggest that the likelihood of reporting increases as the athlete gains confidence (conceptualized as reporting self-efficacy or perceived behavioral control) in their ability to report.1,30
This study takes up the call for a broader conceptualization of knowledge by adopting Bloom Taxonomy of Knowledge to develop a more robust understanding of knowledge in the context of concussion reporting (Figure 1).10 The Bloom taxonomy identifies 3 components of knowledge:
Figure 1.
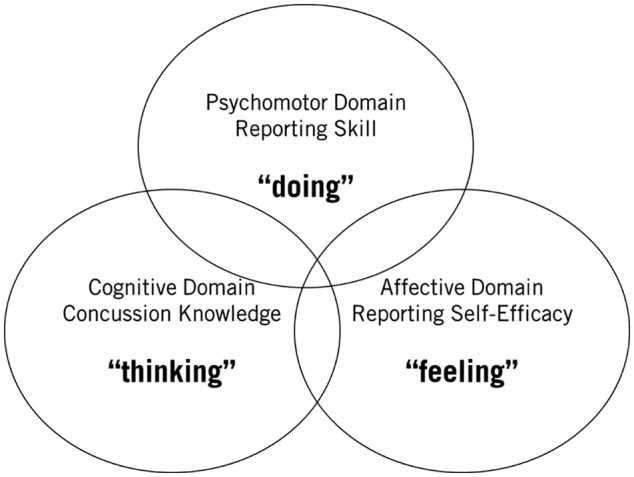
An expanded view of concussion knowledge.
The cognitive10—the thinking component based on explicit facts;
The affective28—the feeling component based on attitudes and emotions; and
The psychomotor23—the doing component based on behavior and ability to act.
As previous studies examined the roles of cognitive (ie, concussion and concussion symptom15,16,19) and affective (ie, reporting self-efficacy1,30) knowledge, this study focused on the role of psychomotor knowledge in concussion reporting: reporting skill. Reporting skill assesses the individual’s mastery of the actions required to report a concussion. High-level reporting skills include the ability to recognize and respond to situations involving potential concussion symptoms, including knowing when you do not know enough to act, leading to the action of seeking advice or information (Figure 2). It represents knowing how to report and, if there is a realization of not knowing how, knowing how to learn.
Figure 2.

The concept of reporting skill.
We call this domain of knowledge “skill,” as it is the most active component of the 3 types of knowledge. Rather than knowing about concussions or feeling confident, it is the doing component of concussion reporting knowledge. Other domains (eg, sexual harassment reporting,9 whistleblowing,27 and financial wellness17,18) have demonstrated the importance of this “how to” component of knowledge in reporting experiences and circumstances that might otherwise be difficult to share.
This study develops a scale to measure reporting skill and examines the role of reporting skill relative to concussion knowledge and self-efficacy in the willingness to report possible concussion symptoms. Two hypotheses related to reporting skill are examined. Based on findings in the extant literature,15,30 a positive association between concussion reporting skill and concussion reporting intentions (ie, people who have higher levels of reporting skill are more likely to report) was expected (hypothesis 1). This association was expected to be stronger than the association between concussion knowledge or concussion symptom knowledge and reporting intentions. Based on findings regarding psychomotor learning,43 the interactions between reporting skill and knowledge were expected to reveal that the association between concussion/symptom knowledge and reporting intentions varied depending on whether the individual had high (or low) reporting skill (hypothesis 2). Individuals with higher levels of reporting skill were expected to have stronger associations between knowledge and intention, as indicated by a significant coefficient for the interaction of reporting skill and knowledge.
Hypothesis 1: Controlling for reporting self-efficacy, reporting intentions will be more closely associated with reporting skill than with concussion knowledge.
Hypothesis 2: Controlling for reporting self-efficacy, the relationship between concussion knowledge and reporting intentions will depend on the level of reporting skill.
Methods
Sampling Design and Participant Recruitment
The sampling design and participant recruitment was consistent across the 3 waves of data collection. A national sample of active adults aged 18 to 24 years was selected from the Survey Sampling International panel for each data collection wave in a repeated cross-sectional design. A total of 1305 active young adults completed the online survey (496 in wave 1, 403 in wave 2, and 406 in wave 3). In each wave, a national sample containing a diversity of sports and activities (including ice hockey and yoga) as well as level of competition (including Division I and intramural) was used. The focus was not on a particular sport or level of competition but on a national sample of young adults. The study was approved by the institutional review board at the University of Wisconsin–Madison. The informed consent document was presented online to each participant before the survey began, with instructions to continue to the first question if the participant consented to the study. To qualify for the study, a participant was required to be between 18 and 24 years old, inclusive, and to participate in regular physical activity.
Measures
Appendix A1 (available in the online version of this article) contains the wording of survey questions measuring each construct as well as the list of concussion and concussion symptom knowledge items used.
Reporting intention, the main outcome variable of the study, was measured using a single item: How likely would you be to tell someone if you thought you might have a concussion? Participants were asked to indicate a number between 0 and 100 using a slider. An indication of zero meant they would “definitely not tell” and of 100 meant they would “definitely tell.”
Concussion knowledge30,33,41 and concussion symptom knowledge (selected items)22,33,41 were measured using existing scales. Concussion knowledge describes understanding of known facts related to concussions, such as “Only a direct hit to the head can cause a concussion” or “Symptoms of a concussion can last for several weeks.” Concussion symptom knowledge reflects the individual’s ability to recognize symptoms of a concussion correctly (eg, headaches [true] and hives or a rash [false]).
Three control variables were used in the model. Reporting self-efficacy was measured using four of the five items from the study by Kroshus et al.30 An exploratory factor analysis using principal components revealed low factor loadings (0.583) for 1 item, I would be able to recognize when I have symptoms of a concussion. This item was removed. Cronbach alpha for the 4-item measure was 0.832. Given the diversity of sports/activities, 2 additional control variables were included: competitiveness and perceived risk of injury. Competitiveness was constructed from the participant’s response to a question asking whether he or she engaged in a sport at a high level of competition. The variable was coded as played competitive sports (1) and did not play competitive sports (0), where competitive sports included those who played at select/travel, competitive club, and National Collegiate Athletic Association (NCAA) Division I, II, or III levels. Perceived risk of injury in the sport was measured as a single self-reported item: How likely are people who play your sport or engage in your activity to get injured? Very likely, somewhat likely, neither likely nor unlikely, somewhat unlikely, very unlikely.
Analytical Strategy
Analysis of waves 1 and 2 identified and confirmed the measure of the reporting skill construct. Exploratory factor analysis (EFA) with wave 1 data was used to identify the reporting skill scale. SPSS statistical software (v25; SPSS Inc) was used to complete the EFA. The objective of wave 2 was to confirm the measurement theory identified in wave 1 as well as the consistency of our scale across studies using an independent sample. The objective of wave 3 was to assess the study hypotheses. Structural equation modeling with MPlus (v8; Muthén & Muthén) was used for the confirmatory factor analysis (CFA). SPSS software was used to conduct the zero-order correlations and ordinary least squares (OLS) regression for this analysis.
Results
The Reporting Skill Scale
The first task of this study was to develop a valid and reliable measure of the reporting skill construct. This task was accomplished using data from waves 1 and 2. The objective of wave 1 was to complete the EFA. The final factor contains 5 statements that reasonably reflect the reporting skill construct (60.2% of the variance explained). Table 1 contains the statements included in the final scale. Details of the EFA can be found in Appendix A2 (available online).
Table 1.
Reporting skill scale a
| Statement | |
|---|---|
| 1 | I know where to find the advice I need when trying to decide whether I should tell someone I might have a concussion. |
| 2 | I am able to recognize a good plan of action when it comes to a possible concussion. |
| 3 | I know how to keep myself from making decisions that might have long-term consequences for my health. |
| 4 | I know how to make myself tell someone if I have a concussion. |
| 5 | I know the right sources to consult to make the right decision about reporting a possible concussion. |
The question was phrased as “To what extent do each of the following statements describe you?” The response options were “Describes me completely, Describes me somewhat, Not sure, Does not describe me very well, Does not describe me at all.”
The CFA showed reasonable fit between the reporting skill factor identified in wave 1 and the data collected in wave 2. The χ2 fit value was 11.699 (df = 5); comparative fit index (CFI) and nonnormed fit index (Tucker-Lewis index) levels were 0.991 and 0.982, respectively; and root mean square error of approximation (RMSEA) level was less than 0.06. These indices are indicative of excellent fit.24 Cronbach α in wave 2 was 0.792, suggesting internal consistency of the scale across studies. As shown in Figure 3, the items continue to reflect the reporting scale construct reasonably well with the factor loadings for 3 of the 5 items above 0.7 and 2 items falling below 0.7.
Figure 3.
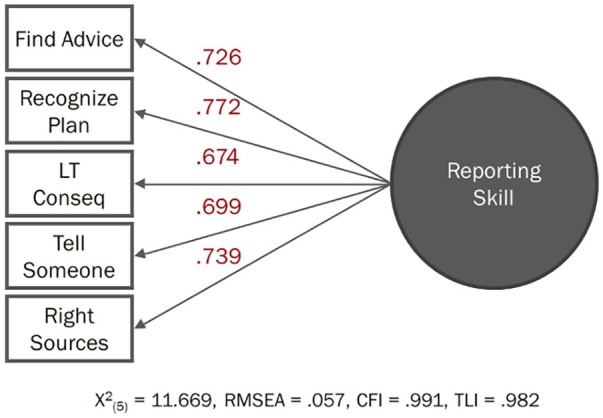
Confirmatory factor analysis results for reporting skill scale. CFI, comparative fit index; LT, long term; RMSEA, root mean square error of approximation; TLI, Tucker-Lewis index.
Skill and self-efficacy tend to develop concomitantly6; therefore, it is important to assess whether reporting skill is a distinct construct. It could be argued that reporting self-efficacy accounts for the shared variance observed in the reporting skill items. Two CFAs tested the discriminant validity of reporting skill relative to reporting self-efficacy—one assuming reporting skill and reporting self-efficacy were distinct constructs and another assuming they were the same constructs. If the 2-factor model that assumes reporting skill and reporting self-efficacy are distinct constructs fits significantly better than the 1-factor model in which the items of the 2 scales are constrained to a single factor, evidence of discriminant validity exists.4
Tests for discriminant validity indicated that reporting skill and reporting self-efficacy are correlated but distinct constructs. The statistics for the 2-factor solution showed a much stronger fit with the data (χ2(26) = 67.215, RMSEA = 0.062, CFI = 0.972, Tucker-Lewis index [TLI] = 0.962) than the 1-factor solution (χ2(27) = 330.808, RMSEA = 0.166, CFI = 0.797, TLI = 0.729). Thus, the discriminant validity of reporting skill relative to reporting self-efficacy is supported. Taken together, these findings suggest that the measure provides a valid and reliable reflection of reporting skill. With this measure, the analysis turns to an assessment of the hypotheses.
The Relationship Between Reporting Skill and Reporting Intentions
With the measures identified, the primary objective of wave 3 was to examine the relationships between reporting skill, concussion knowledge,30,33,41 concussion symptom knowledge,22,33,41 and reporting intentions controlling for reporting self-efficacy, competitiveness, and perceived risk of injury. In wave 3, reporting skill ranged from a low of 5 to a high of 25, with a mean of 18.86 and a standard deviation of 4.50 (median, 19.00; skewness, −0.628). Appendix A3 contains the results of bivariate analyses of these variables as well as a test of OLS regression assumptions. The models met assumptions of normality, homoskedasticity, and multicollinearity.
The first hypothesis examines whether reporting intention has a stronger relationship with reporting skill than concussion knowledge. To assess this hypothesis, reporting intention (scale, 0-100) was regressed on reporting skill and concussion knowledge30,33,41 or concussion symptom knowledge (selected items) 22,33,41 using OLS regression (Table 2). Controlling for the competitive level at which the individual plays, the perceived risk of injury in his or her sport or activity, and reporting self-efficacy, the results revealed that reporting skill was significantly related to the stated probability of reporting while concussion knowledge was not.
Table 2.
The roles of reporting skill and concussion knowledge in reporting intentions a
| Dependent Variable: Probability of Reporting (0 to 100 Scale) | ||||
|---|---|---|---|---|
| Unstandardized Coefficients | Standardized Coefficients | |||
| B | SE | β | P | |
| Independent variable | ||||
| (Constant) | 3.148 | 8.111 | 0.70 | |
| Reporting skill | 1.184 | 0.397 | 0.167 | < 0.01 |
| Concussion knowledge | 0.621 | 0.580 | 0.053 | 0.28 |
| Control | ||||
| Competitiveness | −4.683 | 3.391 | −0.064 | 0.17 |
| Injury risk in your sport | 3.081 | 1.269 | 0.114 | 0.01 |
| Reporting self-efficacy | 1.843 | 0.490 | 0.208 | < 0.01 |
SE, standard error.
R2 = 0.141; F = 13.128 (P < 0.001). Competitiveness is measured by a single item asking the level of sport played (from Division 1 or select to intramural or recreational). Injury risk is measured by a single item asking how likely the individual believes someone in his or her sport is to get injured.
Similar results were obtained using concussion symptom knowledge (Table 3). Controlling for concussion symptom knowledge, competitiveness, risk of injury, and reporting self-efficacy, reporting skill had a significant relationship with reporting intention. Concussion symptom knowledge did not.
Table 3.
The roles of reporting skill and concussion symptom knowledge in reporting intentions a
| Dependent Variable: Probability of Reporting (0 to 100 Scale) | ||||
|---|---|---|---|---|
| Unstandardized Coefficients | Standardized Coefficients | |||
| B | SE | β | P | |
| Independent variable | ||||
| (Constant) | 2.244 | 8.111 | 0.78 | |
| Reporting skill | 1.132 | 0.395 | 0.160 | < 0.01 |
| Concussion symptom knowledge | 0.784 | 0.427 | 0.090 | 0.07 |
| Control | ||||
| Competitiveness | −4.527 | 3.377 | −0.062 | 0.18 |
| Injury risk in your sport | 3.237 | 1.266 | 0.120 | 0.01 |
| Reporting self-efficacy | 1.789 | 0.489 | 0.202 | < 0.01 |
SE, standard error.
R2 = 0.146; F = 13.646 (P < 0.001). Competitiveness is measured by a single item asking the level of sport played (from Division 1 or select to intramural or recreational). Injury risk is measured by a single item asking how likely the individual believes someone in his or her sport is to get injured.
Hypothesis 2 states that the relationship between concussion/symptom knowledge and reporting intention will depend on the level of reporting skill. To examine the moderating effect of reporting skill on the concussion knowledge/reporting intention relationship, interaction terms were added to the models in Tables 4 and 5. Interaction terms were calculated using the mean-centered main effects variables to reduce the possibility of multicollinearity. Variance inflation factors for the interaction models were all below 2.000. No significant interaction was observed between concussion knowledge and reporting skill (Table 4).
Table 4.
The interaction of reporting skill and concussion knowledge in reporting intentions a
| Dependent Variable: Probability of Reporting (0 to 100 Scale) | ||||
|---|---|---|---|---|
| Unstandardized Coefficients | Standardized Coefficients | |||
| B | SE | β | P | |
| Independent variable | ||||
| (Constant) | 3.871 | 8.190 | 0.65 | |
| Reporting skill | 1.196 | 0.398 | 0.169 | <0.01 |
| Concussion knowledge | 0.547 | 0.591 | 0.046 | 0.35 |
| Interaction of reporting skill and concussion knowledge | −0.760 | 0.116 | −0.031 | 0.51 |
| Control | ||||
| Competitiveness | −4.815 | 3.399 | −0.066 | 0.16 |
| Injury risk in your sport | 3.019 | 1.274 | 0.112 | 0.02 |
| Reporting self-efficacy | 1.840 | 0.490 | 0.227 | <0.01 |
SE, standard error.
R2 = 0.142; F = 10.997 (P < 0.001). Competitiveness is measured by a single item asking the level of sport played (from Division 1 or select to intramural or recreational). Injury risk is measured by a single item asking how likely the individual believes someone in his or her sport is to get injured.
Table 5.
The interaction of reporting skill and concussion symptom knowledge in reporting intentions a
| Dependent Variable: Probability of Reporting (0 to 100 Scale) | ||||
|---|---|---|---|---|
| Unstandardized Coefficients | Standardized Coefficients | |||
| B | SE | β | P | |
| Independent variable | ||||
| (Constant) | −3.786 | 8.213 | 0.01 | |
| Reporting skill | 1.143 | 0.390 | 0.161 | <0.01 |
| Concussion symptom knowledge | 1.035 | 0.428 | 0.118 | 0.02 |
| Interaction of reporting skill and concussion symptom knowledge | 0.289 | 0.087 | 0.157 | <0.01 |
| Control | ||||
| Competitiveness | −3.862 | 3.341 | −0.053 | 0.25 |
| Injury risk in your sport | 3.633 | 1.256 | 0.135 | <0.01 |
| Reporting self-efficacy | 1.877 | 0.483 | 0.212 | <0.01 |
SE, standard error.
R2 = 0.169; F = 13.508 (P < 0.001). Competitiveness is measured by a single item asking the level of sport played (from Division 1 or select to intramural or recreational). Injury risk is measured by a single item asking how likely the individual believes someone in his or her sport is to get injured.
There was, however, a significant interaction between concussion symptom knowledge and reporting skill (Table 5). These findings suggest that reporting skill may be the missing ingredient in supporting the translation of knowledge into reporting behavior. They also suggest that concussion education should focus more on the symptoms of a concussion and less on general concussion knowledge.
Across the 3 models, there were no significant differences in the reporting intentions of competitive and noncompetitive athletes. Perceived risk of injury and reporting self-efficacy were both positively and significantly associated with reporting intention in all 3 models.
These findings suggest that knowing the actions to take in reporting was more important than having knowledge of concussions or concussion symptoms. Reporting skill, not concussion or concussion symptom knowledge, was associated with greater intentions to report symptoms. Among those with higher levels of reporting skill, however, concussion symptom knowledge (but not general concussion knowledge) was associated with greater intentions to report symptoms.
Discussion
Despite a proliferation of concussion education interventions,13,14,35,37 concussion knowledge and concussion symptom knowledge have had limited effects on reporting.11,12,15,16,19,30 This cross-sectional study broadens the concept of concussion knowledge to include reporting self-efficacy and reporting skill to answer the call for a more “procedural approach” in the concussion reporting discussion.15,30 Reporting intentions seem to be more closely associated with the individual’s reporting skill than his or her concussion knowledge. Furthermore, reporting skill appears to be an important ingredient in the translation of concussion symptom knowledge into the behavioral intention of reporting. These findings suggest that a combination of reporting skill and concussion symptom knowledge (not general concussion knowledge) offers the most promising path to increased concussion reporting. It is reasonable to expect that self-efficacy, a significant variable in all models examined, increases as skill increases.5 Findings from this study provide evidence that a more robust view of knowledge in the context of concussion reporting offers a promising avenue for increased reporting intentions.
From a practitioner point of view, these findings suggest that concussion education programs should incorporate content beyond explicit concussion and concussion symptom knowledge to include a focus on reporting skill and self-efficacy. Findings from this study suggest that incorporating reporting skill in program content will improve the impact of the educational program and provide a better indication of future reporting intention. This requires moving beyond a general call to “tell someone.” Developing reporting skill includes assessing whether the individual understands how to report and can execute the steps in reporting. In this way, reporting skill is similar to any other skill required in one’s activity or sport.
Sports teams and, when present, their sports health care team have several roles to play in the development of reporting skill. One role has to do with establishing a game plan for responding to possible concussions that is then taught to players. By elevating the importance of knowing how to report, athletes and their teammates are more likely to recognize that they do not know how to report and should learn. With greater importance placed on this skill, athletes will be more likely to allocate attentional resources to developing the skill.42 This development can begin at fairly young ages. There is evidence that metacognitive abilities appear among preschoolers and develop over time.21,44 Jonker et al25 found that 12- to 16-year-old elite athletes can be distinguished by greater metacognitive ability, especially reflection regarding what they are and are not able to perform in their sport.
With awareness of the need, reporting skill training is an “if this–then that” type of training, similar to how athletes train for circumstances that may be fluid and require an actionable decision. For example, mandatory concussion education could include rehearsing the sequence of events in reporting a concussion rather than describing them. The objective is to make the steps involved feel familiar so when the time comes to report, the barriers associated with lack of skill and self-efficacy are removed.
A focus on reporting skill in a team context may also serve to reinforce group norms related to concussion disclosure. Such norms encourage athletes and bystanders (eg, teammates) to report.29,31,32 Understanding the norms and expectations is 1 component of an athlete’s socialization into team culture. Practicing how to act in accordance with those norms is another.2 Communicating and practicing a team game plan offers meaningful reinforcement of the value a team places on responding to a concussion for the athlete and any teammates who might find themselves bystanders to a possible concussion event.
In some team environments with robust access to sports medicine staff, reporting skill or knowing the steps to report may seem obvious. However, even in such team environments, there are instances when highly competitive athletes must make an individual determination to report, and must have the skill to do so. There are many other team environments in which athletes do not have easy access to sports medicine care, have no athletic trainers on-site, and have no one observing injuries to facilitate reporting. Yet student-athletes in these settings may still be subject to mandatory concussion education that currently includes only the cognitive pillar of knowledge.35 In these environments, designing educational programs that incorporate reporting skill is of greater importance: knowing where to find advice, recognizing a plan of action, making a good health care decision, and recognizing the sources of information for a reporting decision.
Finally, programs mandated to provide concussion education should routinely assess the efficacy of their educational programs through the broader framework of knowledge as described here. Findings from this study suggest that including an assessment of reporting skill using the reporting skill scale as presented will provide a better indication of future reporting intention.
Limitations
There are several limitations to this study. Participants in this study are a national sample of young adults who engage in a wide variety of sports and activities. This scale has not yet been tested with elite athletes or a particular sport or team or as part of a program evaluation. It will be interesting to learn how the scale behaves with a specific tier of competitive performance or with a very concussion education–saturated sport like football. Additional work is required to examine scale performance with additional age groups beyond the 18- to 24-year-olds included here. Given the cross-sectional panel samples used, the scale was not evaluated using test-retest reliability. Testing the scale with a particular team will allow for such determination.
Future research might examine the role of reporting skill in various contexts and with different types of reporting decisions. Baugh et al8 found that reporting intention declines with concussion event accumulation. Future research might explore whether reporting skill attenuates the decline or how an actual reporting experience influences the association between knowing how to report and reporting.
Supplemental Material
Supplemental material, Reporting_Skill_Appendices for Reporting Skill: The Missing Ingredient in Concussion Reporting Intention Assessment by Dee Warmath and Andrew P. Winterstein in Sports Health: A Multidisciplinary Approach
Acknowledgments
The authors would like to thank Johna Register-Mihalik, Chris D’Lauro, and our anonymous reviewers for their very helpful comments on drafts of this manuscript.
Footnotes
The following authors declared potential conflicts of interest: D.W. and A.P.W. report grants from NCAA Mind Matters Challenge. This study was supported by the National Collegiate Athletic Association and Department of Defense through a Mind Matters Challenge Grant.
References
- 1. Ajzen I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior 1. J Appl Soc Psychol. 2002;32:665-683. [Google Scholar]
- 2. Arnett JJ. Broad and narrow socialization: the family in the context of a cultural theory. J Marriage Fam. 1995;57:617-628. [Google Scholar]
- 3. Asken BM, McCrea MA, Clugston JR, Snyder AR, Houck ZM, Bauer RM. “Playing through it”: delayed reporting and removal from athletic activity after concussion predicts prolonged recovery. J Athl Train 2016;51:329-335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bagozzi RP, Yi Y. On the evaluation of structural equation models. J Acad Mark Sci. 1988;16:74-94. [Google Scholar]
- 5. Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. 1993;28:117-148. [Google Scholar]
- 6. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191-215. [DOI] [PubMed] [Google Scholar]
- 7. Baugh CM, Kroshus E, Daneshvar DH, Filali NA, Hiscox MJ, Glantz LH. Concussion management in United States college sports: compliance with National Collegiate Athletic Association concussion policy and areas for improvement. Am J Sports Med. 2015;43:47-56. [DOI] [PubMed] [Google Scholar]
- 8. Baugh CM, Meehan W, Kroshus E, McGuire TG, Hatfield LA. College football players less likely to report concussions and other injuries with increased injury accumulation [published online January 28, 2019]. J Neurotraum. doi: 10.1089/neu.2018.6161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bergman ME, Langhout RD, Palmieri PA, Cortina LM, Fitzgerald LF. The (un)reasonableness of reporting: antecedents and consequences of reporting sexual harassment. J Appl Psychol. 2002;87:230-242. [DOI] [PubMed] [Google Scholar]
- 10. Bloom BS, Engelhart MD, Furst EJ, Hill WH, Krathwohl DR. Taxonomy of Educational Objectives: Handbook 1: Cognitive Domain. New York, NY: Longman, Green and Co; 1956. [Google Scholar]
- 11. Bramley H, Patrick K, Lehman E, Silvis M. High school soccer players with concussion education are more likely to notify their coach of a suspected concussion. Clin Pediatr. 2012;51:332-336. [DOI] [PubMed] [Google Scholar]
- 12. Caron JG, Bloom GA, Falcão WR, Sweet SN. An examination of concussion education programmes: a scoping review methodology. Inj Prev. 2015;21:301-308. [DOI] [PubMed] [Google Scholar]
- 13. Carroll-Alfano M. Mandated high school concussion education and collegiate athletes’ understanding of concussion. J Athl Train. 2017;52:689-697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Centers for Disease Control and Prevention. Heads Up to youth sports. https://www.cdc.gov/headsup/youthsports/index.html. Accessed September 14, 2018.
- 15. Chinn NR, Porter P. Concussion reporting behaviours of community college student-athletes and limits of transferring concussion knowledge during the stress of competition. BMJ Open Sport Exerc Med. 2016;2(1):e000118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Chrisman SP, Quitiquit C, Rivara FP. Qualitative study of barriers to concussive symptom reporting in high school athletics. J Adolesc Health. 2013;52:330-335. [DOI] [PubMed] [Google Scholar]
- 17. Consumer Financial Protection Bureau. Financial well-being: the goal of financial education, 2015. http://www.consumerfinance.gov/reports/financial-well-being. Accessed September 14, 2018.
- 18. Consumer Financial Protection Bureau. Measuring financial skill: a guide to using the Bureau of Consumer Financial Protection’s Financial Skill Scale, 2018. https://www.consumerfinance.gov/data-research/research-reports/measuring-financial-skill/. Accessed December 31, 2018.
- 19. Cusimano MD, Topolovec-Vranic J, Zhang S, Mullen SJ, Wong M, Ilie G. Factors influencing the underreporting of concussion in sports: a qualitative study of minor hockey participants. Clin J Sport Med. 2017;27:375-380. [DOI] [PubMed] [Google Scholar]
- 20. Echlin PS, Johnson AM, Riverin S, et al. A prospective study of concussion education in 2 junior ice hockey teams: implications for sports concussion education. Neurosurg Focus. 2010;29(5):e6. [DOI] [PubMed] [Google Scholar]
- 21. Fang Z, Cox BE. Emergent metacognition: a study of preschoolers’ literate behavior. J Res Child Educ. 1999;13:175-187. [Google Scholar]
- 22. Guskiewicz KM, Register-Mihalik J, McCrory P, et al. Evidence-based approach to revising the SCAT2: introducing the SCAT3. Br J Sports Med. 2013;47:289-293. [DOI] [PubMed] [Google Scholar]
- 23. Harrow AJ. A Taxonomy of the Psychomotor Domain: A Guide for Developing Behavioral Objectives. New York, NY: David McKay Company; 1972. [Google Scholar]
- 24. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equat Modeling. 1999;6:1-55. [Google Scholar]
- 25. Jonker L, Elferink-Gemser MT, Visscher C. Differences in self-regulatory skills among talented athletes: the significance of competitive level and type of sport. J Sport Sci. 2010;28:901-908. [DOI] [PubMed] [Google Scholar]
- 26. Kaut KP, DePompei R, Kerr J, Congeni J. Reports of head injury and symptom knowledge among college athletes: implications for assessment and educational intervention. Clin J Sport Med. 2003;13:213-221. [DOI] [PubMed] [Google Scholar]
- 27. Keenan JP. Upper-level managers and whistle-blowing: determinants of perceptions of company encouragement and information about where to blow the whistle. J Business Psychol. 1990;5:223-235. [Google Scholar]
- 28. Krathwohl DR, Bloom BS, Masia BB. Taxonomy of Educational Objectives: Handbook II: Affective Domain. New York, NY: David McKay Company; 1964. [Google Scholar]
- 29. Kroshus E, Baugh CM. Concussion education in US collegiate sport: what is happening and what do athletes want? Health Educ Behav. 2016;43:182-190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Kroshus E, Baugh CM, Daneshvar DH, Viswanath K. Understanding concussion reporting using a model based on the theory of planned behavior. J Adolesc Health. 2014;54:269-274. [DOI] [PubMed] [Google Scholar]
- 31. Kroshus E, Garnett BR, Baugh CM, Calzo JP. Engaging teammates in the promotion of concussion help seeking. Health Educ Behav. 2016;43:442-451. [DOI] [PubMed] [Google Scholar]
- 32. Kroshus E, Garnett BR, Baugh CM, Calzo JP. Social norms theory and concussion education. Health Educ Res. 2015;30:1004-1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kroshus E, Garnett B, Hawrilenko M, Baugh CM, Calzo JP. Concussion under-reporting and pressure from coaches, teammates, fans, and parents. Soc Sci Med. 2015;134:66-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Kurowski BG, Pomerantz WJ, Schaiper C, Ho M, Gittelman MA. Impact of preseason concussion education on knowledge, attitudes, and behaviors of high school athletes. J Trauma Acute Care Surg. 2015;79(3suppl 1):S21-S28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. LaRoche AA, Nelson LD, Connelly PK, Walter KD, McCrea MA. Sport-related concussion reporting and state legislative effects. Clin J Sport Med. 2016;26:33-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004;14:13-17. [DOI] [PubMed] [Google Scholar]
- 37. McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport—the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017;51:838-847. [DOI] [PubMed] [Google Scholar]
- 38. National Collegiate Athletic Association. Concussion educational resources. Retrieved from http://www.ncaa.org/sport-science-institute/concussion-educational-resources. Accessed September 14, 2018.
- 39. Register-Mihalik JK, Guskiewicz KM, McLeod TC, Linnan LA, Mueller FO, Marshall SW. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Athl Train. 2013;48:645-653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Register-Mihalik JK, Linnan LA, Marshall SW, McLeod TC, Mueller FO, Guskiewicz KM. Using theory to understand high school aged athletes’ intentions to report sport-related concussion: implications for concussion education initiatives. Brain Inj. 2013;27:878-886. [DOI] [PubMed] [Google Scholar]
- 41. Rosenbaum AM, Arnett PA. The development of a survey to examine knowledge about and attitudes toward concussion in high-school students. J Clin Exp Neuropsychol. 2010;32:44-55. [DOI] [PubMed] [Google Scholar]
- 42. Schneider W, Bjorklund DF. Memory. In: Damon W, Series ed; Kuhn D, Siegler RS, Vol eds. Handbook of Child Psychology: Vol. 2. Cognitive, Language, and Perceptual Development. 5th ed. New York, NY: Wiley; 1998:467-521. [Google Scholar]
- 43. Shin S, Park JH, Kim JH. Effectiveness of patient simulation in nursing education: meta-analysis. Nurse Educ Today. 2015;35:176-182. [DOI] [PubMed] [Google Scholar]
- 44. Zelazo PD, Frye D. Cognitive complexity and control: II. The development of executive function in childhood. Curr Dir Psychol Sci. 1998;7:121-126. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Reporting_Skill_Appendices for Reporting Skill: The Missing Ingredient in Concussion Reporting Intention Assessment by Dee Warmath and Andrew P. Winterstein in Sports Health: A Multidisciplinary Approach