

Abstract
Objective.
Previous literature has shown an inconsistent relationship between physical activity and stressor-evoked blood pressure reactivity. Use of ecological momentary assessment (EMA) may facilitate detecting such a relationship. In this study, the moderating effects of regular physical activity on the magnitude of ambulatory blood pressure responses to psychosocial stressors experienced in daily life were examined.
Methods.
477 healthy working adults (ages 30–54) provided ambulatory blood pressure (ABP) readings and recorded their daily experiences, using electronic diaries (ED), over four monitoring days. Measures of momentary Task Strain (high demand, low control) and Social Conflict (rating of recent social interaction quality) were used as indices of stressor exposure, and an accelerometry device was used to create two indices of physical activity: weekly average and recent (30 minutes prior to each ED interview). Multilevel models were used to examine the moderating between- and within-person effects of physical activity on ABP fluctuations corresponding with the momentary psychosocial stressors.
Results.
Weekly physical activity moderated the effects of ABP responses to Task Strain (SBP: p = .033; DBP: p = .028) and Social Conflict (DBP: p = .020), with significant increases in SBP and DBP shown for less physically active individuals but not for more physically active individuals. Similarly, recent physical activity moderated within-person DBP responses to Task Strain (p = .025), with greater DBP increases following less active periods.
Conclusion.
Our results demonstrate that weekly and recent physical activity may moderate the effects of ABP responses to daily psychosocial stress.
Keywords: physical activity, ambulatory blood pressure, ecological momentary assessment, psychological stress
Accumulating evidence suggests that exaggerated cardiovascular reactivity (CVR), the tendency to show large magnitude cardiovascular (e.g., heart rate or blood pressure) responses to psychological challenges or stressors, has a small but significant association with future cardiovascular disease risk (Chida & Steptoe, 2010; Treiber et al., 2003). Regular physical activity, broadly defined as any bodily movement that results in energy expenditure (Caspersen, Powell, & Christenson, 1985), has been linked with a number of autonomic factors that may reduce stress-related cardiovascular reactivity. For instance, regular engagement in moderate-to-vigorous physical activity (MVPA) improves baroreflex function (Monahan et al., 2000), improves heart rate variability (Davy, Miniclier, Taylor, Stevenson, & Seals, 1996; Tulppo et al., 2003), a marker of parasympathetic tone, and induces neuroplastic changes to brain regions involved in important autonomic functions (Michelini & Stern, 2009; Morgan, Corrigan, & Baune, 2015). In addition to its effects on the autonomic nervous system, physical activity has antidepressant and anxiolytic effects (Petruzzello, Landers, Hatfield, Kubitz, & Salazar, 1991; Salmon, 2001). By virtue of its physiological and psychological benefits, physical activity could potentially lead to reductions in stress-related CVR.
Despite the fact that physical activity influences a number of factors linked with CVR, the literature has predominantly focused on physical fitness, which involves multiple components (i.e., aerobic capacity, muscular strength and endurance, body composition, and flexibility Caspersen et al., 1985) commonly measured by an objective fitness test (e.g., resting HR, VO2 max, treadmill test to exhaustion). However, reviews and meta-analyses on the relationship between CVR and physical fitness reveal inconsistent results. A meta-analysis of 33 cross-sectional and longitudinal studies by Forcier and colleagues (2006) showed attenuated stress-related heart rate (HR) and systolic blood pressure (SBP) reactivity among physically fit individuals relative to their unfit counterparts. On the other hand, a more inclusive meta-analysis of 73 studies by Jackson and Dishman (2006), showed that high fitness was related to slightly greater CVR. These discrepant findings may be explained by the inclusion of more small, underpowered studies with heterogeneous study designs. For instance, 80% of the studies cited in the Forcier and colleagues meta-analysis had fewer than 20 subjects. Moreover, the relationship between physical fitness and CVR may vary by study design (e.g., cross-sectional, single-session or long-term experimental trials) which may account for some of these discordant conclusions. The inclusion of small studies with varying study designs in this literature may pose a challenge to detecting a relationship between physical fitness and CVR.
Regular physical activity, though a strong correlate of physical fitness (Kohl, Blair, Paffenbarger, Macera, & Kronenfeld, 1988), may attenuate BP responses to stress without necessarily modifying physical fitness. Experimental trials assessing the acute effects of physical activity, specifically MVPA, on CVR are more consistent than studies examining fitness effects. A meta-analysis consisting of 15 trials that examine BP responses to psychosocial laboratory tasks immediately following a bout of MVPA (ranging from 10 minutes to 2 hours) found overall reductions in SBP and DBP reactivity, when compared to responses that occurred during resting periods (within-subject designs) or among non-active controls (between-subject designs; Hamer, Taylor, & Steptoe, 2006). Stronger effects of physical activity were found when the stressor was presented within 30-minutes following MVPA. Because the base rate of physical activity is higher among active individuals, any given stressor is more likely to occur in a post-activity window in this group than in a group of sedentary individuals. To the extent that acute activity bouts are an important element accounting for the relationship between regular physical activity and CVR, this relationship may be most clearly seen when physical activity, and response to stressors, are observed in the context of daily living.
The purpose of the current investigation is to assess the relationship between objective daily life measures of physical activity and blood pressure responses to stress in the natural environment. Two existing studies have examined the relationship between fitness and blood pressure responses to daily life stressors, and neither of these examined daily life measures of physical activity. Ritvanen and colleagues (2007) examined differences in resting clinic blood pressures between morning and afternoon among employed teachers and found no differential effects of the workday environment (a presumed stressor) as a function of physical fitness. Oliveira-Silva and colleagues (2016) examined ambulatory blood pressure on a day of commercial flight (another presumed stressor) and a control day (no flight) and similarly found no effects of physical fitness on BP differences between these two periods. In addition to the fact that these studies did not measure actual physical activity during the monitoring periods, other significant limitations involve a) a lack of stress appraisal measurement during the monitoring period (i.e., the investigators could not verify that the conditions they were assessing were reasonable operational definitions of psychosocial stress), and b) not controlling for important time-varying covariates (e.g., posture, recent activity) that have been shown to have a significant effects (and in this case, confounding effects) on ambulatory BP readings (Kamarck & Lovallo, 2003; Kamarck, 2003).
Unlike these studies and other work in this area, the present study assesses CVR using ecological momentary assessment (EMA), which involves real-time measurement of psychological and physiological processes in the natural environment. Using this approach, stressors are operationalized based upon momentary self-reports of recent social and task-related demands, and responses to these demands are assessed using repeated assessments of ambulatory blood pressure. The use of EMA permits us to record and control for concurrent behaviors (such as posture and cigarette consumption) that may confound our ability to assess the effects of psychosocial stressors on physiology. A second useful feature of this study involves the use of objective, real-time measures of physical activity, including the timing of physical activity, to examine its potential moderating impact on stress-related cardiovascular responding. We hypothesized that individuals who are more physically active during daily life would show reduced SBP and DBP responses to daily stressors relative to individuals with lower levels of physical activity (a between-person effect). We also examined whether daily psychosocial stressors occurring in the period shortly following physical activity would be less likely to be associated with pronounced blood pressure changes when compared with stressors occurring following less active periods (a within-person effect).
Methods
Participants
Participants were drawn from the Adult Health and Behavior-2 (AHAB-2) cohort from the University of Pittsburgh, a study of psychosocial, behavioral, and biological risk factors and subclinical CVD in healthy, working midlife adults recruited between 2008 and 2011. To be eligible to participate, participants had to be between the ages of 30 and 54 years and working at least 25 hours per week outside the home. Exclusion criteria for this sample have been previously described (Peterson et al., 2017). Briefly, participants were excluded if they had a history of CVD, stage 2 hypertension (systolic/diastolic BP ≥ 160/100 mm Hg), or were prescribed antihypertensive or antiarrhythmic medications. The study was approved by the University of Pittsburgh Institutional Review Board, and all participants signed an informed consent agreement upon enrollment. Participants received compensation up to US $410, depending on compliance with the protocol.
Procedure
Participants completed three visits relevant to this phase of the study. Demographics and medical history were assessed at Visit 1. Participants received extensive training and practice with ambulatory monitoring equipment at Visit 2 before entering the field for monitoring. The monitoring period typically spanned 7 days and included a practice day for participants to acclimate to the equipment and protocol. During this 7-day period, participants were instructed to wear a SenseWear armband monitor (Body Media, Pittsburgh, PA; SenseWear Pro3) for measuring energy expenditure. Within this 7 day period, participants also carried an electronic diary (Palm Z22) and wore an ambulatory blood pressure monitor during the day time only (SunTech Medical, Inc, Morrisville, NC; Oscar 2 ABP monitor) over the course of two 2-day periods (totaling 3 work days and 1 non-work day) in the midst of a working week. After each hourly ABP cuff inflation, participants completed a brief electronic diary entry on a handheld personal digital assistant (Palm Z22), assessing behaviors that occurred just prior to the cuff inflation (see below). Participants wore other ambulatory equipment and collected biological samples during the monitoring period not relevant to this current report. To protect the equipment, participants were instructed to remove monitoring devices during impact and aquatic sportsa. Participants returned equipment at Visit 3 and were provided feedback on the ambulatory monitoring data collection.
Measures
Daily Psychosocial Stressors.
After each hourly ABP cuff inflation, participants completed a 43-item questionnaire administered by the electronic diary. Several items were extracted to derive two measures of daily psychosocial stressors: Task Strain and Social Conflict. This study has focused on the degree of exposure and response to these two sets of stressors due to their relevance as correlates of subclinical atherosclerosis in this population (Joseph, Kamarck, Muldoon, & Manuck, 2014b; Kamarck, Li, Wright, Muldoon, & Manuck, 2018).
Task Strain.
As part of each hourly questionnaire, participants were prompted to recall their mental and physical activity in the 10 minutes prior to the ABP cuff inflation. Participants rated three items (i.e., “Required working hard?” “Required working fast?” and “Juggling several tasks at once?”) assessing Task Demand and two items (i.e., “Could change activity if you chose to?” and “Choice in scheduling this activity?”) assessing Decision Latitude, as described in our prior work (Kamarck, 2002; Kamarck et al., 2018; Kamarck, 2003). These items were derived from the Karasek job strain model, which posits elevated cardiovascular risk among individuals rating their workplace as high in psychological demands but low in decision control (Karasek Jr, 1979). Using this approach, item responses (NO! No no yes Yes YES!) were converted to a 1- to 6-point rating, and averaged across items within each scale. A measure of Task Strain was coded as a dichotomous variable: for observations where average Demand ratings were above the grand median of 3 and average Control ratings were below or equal to the grand medial of 4, Task Strain was coded as 1. For all other observations, Task Strain was coded as 0.
Social Conflict.
During each hourly assessment, participants were also asked about their most recent social interaction, including its timing (current, within past 10 minutes, or greater than 10 minutes before the electronic diary entry), its participants (e.g., spouse, friend, family), and its quality. Only responses pertaining to interactions reported to be occurring at the time of, or within the 10-minute period preceding the cuff inflation, were included in the analysis. Social Conflict was operationalized as the mean rating assigned to two items assessing negative aspects of the interaction (“Someone in conflict with you?” and “Someone treated you badly?”) using Likert 1-to 6-point scale ratings as above (see Joseph, Kamarck, Muldoon, & Manuck, 2014a).
Physical Activity.
Physical activity measures were calculated from the SenseWear armband monitor in 1-minute epochs, using data from a bi-axial accelerometer, a heat flux sensor, a galvanic skin response, a skin temperature sensor, and a near body temperature sensor included in this device (Mackey et al., 2011). Physical activity was operationalized in two ways. First, the metabolic equivalent (METs) units during each minute over the course of the monitoring period were averaged to index weekly physical activity. Second, the METs units during the 30-minute period prior to each hourly diary entry was averaged to index recent physical activity. Use of a 30-minute period was based upon previous research observing a stronger effect on blood pressure reactivity when the stressor was presented within 30 minutes of a physical activity bout (Hamer et al., 2006). For both these physical activity measures, only days in which ambulatory blood pressure readings were collected were included for analysis (see Peterson et al., 2017).
Ambulatory Blood Pressure.
Participants were instructed to wear the oscillometric Oscar 2 ABP monitor (SunTech Medical, Inc, Morrisville, NC) on the upper arm of the non-dominant hand during waking hours on each of the four monitoring days. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) values were automatically recorded by the monitor. The Oscar 2 has been validated to the standards of several international protocols (Goodwin, Bilous, Winship, Finn, & Jones, 2007; Jones, Bilous, Winship, Finn, & Goodwin, 2004).
ABP Covariates.
As part of the questionnaire that was completed after each ABP assessment, participants were asked about a variety of factors that are known to affect blood pressure. In our analyses, these factors served as time-varying covariates: posture (standing, sitting, or lying down), temperature comfort (comfortable, too hot, or too cold), and speaking status (speaking or no) at the time of ABP assessment, self-reported physical activity (limited, light, moderate, or vigorous) in the 10 minutes before ABP assessment, and consumption of a meal, snack, caffeine, and/or alcohol in the hour before ABP assessment. Participants were instructed to record each cigarette smoked in a separate entry on the same electronic diary (see Joseph et al., 2016 for details). In addition to self-report measures of physical activity from the electronic diary, the total METs recorded in the 10 minutes prior to each BP reading was also used as a time-varying covariate.
Analysis Plan
All analyses were performed with multilevel models in SAS (version 9.4; SAS Institute, Cary, NC) using PROC MIXED. Within the multilevel models, Level 1 analyses (at the observation level) examined the within-person association between psychosocial stressors and ABP responses with the time-varying covariates detailed in the section above. Measures of daily psychosocial stressors and physical activity measures were treated as random coefficients, and all time-varying covariates were entered as fixed effects to reduce model complexity. Several of the time-varying ABP covariates were recoded into dummy variables: posture (as standing versus others and sitting versus others), physical activity as light activity (e.g., walking, light housework) versus others, moderate activity (e.g., jogging, heavier housework) versus others, and vigorous activity (e.g., running, climbing stairs) versus others. The recent consumption of a meal, snack, caffeine, and alcohol within the past hour were each dichotomized as well (1 = yes, 0 = no). The number of cigarettes used in the past hour was entered into the model as a continuous variable.
Level 2 analyses (at the person level) examined between-person covariates and weekly physical activity as a moderator of the effects of psychosocial stressors. In addition to the time-varying covariates, we controlled for demographics as between-person covariates: self-reported sex, age, race (White vs. Non-White), and highest level of education (1 = high School diploma or less, 2 = associates or technical degree, 3 = bachelor’s degree, 4 = graduate degree). Across all models, a spatial power function was used to model autocorrelated errors. The variances and covariances of the intercept and slope associated with momentary stressors (Task Strain or Social Conflict) were estimated using unstructured covariance matrices.
In the context of time-varying covariates, we first tested the main effects of Task Strain and Social Conflict on momentary SBP and DBP. Next, with between-person and time-varying covariates, we tested whether the effects of Task Strain and Social Conflict on momentary SBP and DBP were moderated by weekly physical activity. Each of the moderator models included main effects of weekly physical activity, main effects of one of the daily psychosocial stressors (either Task Strain or Social Conflict) and the appropriate interaction term (Task Strain X weekly physical activity or Social Conflict X weekly physical activity). The effects of Task Strain or Social Conflict were tested in separate models. When applicable, these tests were followed up by analysis of simple slopes, following the recommendations by Aiken and West (1991). In the simple slopes analyses, we examined the effects of daily psychosocial stressors for more active individuals (one standard deviation above the mean on the weekly physical activity variable) and for less active individuals (one standard deviation below the mean) in separate models.
For within-person analyses, we structured the model to test the effects of recent physical activity independent from the weekly physical activity effects. Following the recommendations by Hoffman (2015), the models included a person-centered term for recent physical activity (between-person mean physical activity subtracted from the within-person recent physical activity observations) and included the main effect of mean physical activity variable in the model. The procedure involving interaction terms and applicable simple slope analyses described above was repeated for the within-person analyses involving recent physical activity (Task Strain X recent physical activity and Social Conflict X recent physical activity).
Results
Sample Characteristics
A total of 494 participants completed ambulatory monitoring data collection as part of the AHAB-2 study. Sixteen participants were removed for missing SenseWear data, and one participant was removed for missing ABP data. Over the entire monitoring period, participants wore the SenseWear device an average of 5.5 days for an average of 14 hours and 26 minutes on each day. Most of the recent physical activity observations were categorized as sedentary (1.5 METS or lower) or light physical activity (1.5 to 3.0 METS) (see Table 1 for details). For the analyses, we removed participants who did not report within-person variability in Task Strain (i.e., did not report a period of Task Strain) or Social Conflict (i.e., item responses for all endorsed social interactions were identical) during the monitoring period because we were concerned that differences in blood pressure reactivity may not be accurately estimated among these participants. Accordingly, 14 subjects were removed from analytic models featuring Task Strain (yielding a sample size of 463), and 60 participants were removed from analytic models featuring Social Conflict (yielding a sample size of 417). Among 25,386 observations, 30.0% of momentary scores were coded as high in Task Strain. The average Social Conflict rating was 1.65 (SD = 0.91) among 15,478 momentary observations of recent social interactions, with 41.7% of momentary scores coded greater than one (the minimum score).
Table 1.
Sample Characteristics (N = 477)
| Characteristic | Mean or N | SD | % |
|---|---|---|---|
| Age (years) | 42.7 | 7.3 | |
| Sex, female | 241 | 52.3 | |
| Race-ethnicity, nonwhite | 85 | 18.4 | |
| Education level, college degree or greater | 331 | 71.8 | |
| Current Smokers | 62 | 13.0 | |
| Resting Clinic Systolic Blood Pressure (mmHg) | 115.3 | 10.8 | |
| Resting Clinic Diastolic Blood Pressure (mmHg) | 72.7 | 7.9 | |
| Resting Clinic Blood Pressure ≥140/90 mmHg | 15 | 3.1 | |
| Mean Ambulatory Systolic Blood Pressure (mmHg) | 133.6 | 11.6 | |
| Mean Ambulatory Diastolic Blood Pressure (mmHg) | 80.8 | 7.4 | |
| Average weekly physical activity (METs) | 1.62 | 0.29 | |
| Average recent physical activity (METs) | 1.63 | 0.71 | |
| Proportion of Recent Physical Activity by Intensity Level | |||
| Sedentary (METs < 1.5) | 54.3 | ||
| Light (METs 1.5 to 3.0) | 41.2 | ||
| Moderate-to-Vigorous(METs > 3.0 ) | 4.4 | ||
Main Effects of Daily Psychosocial Stressors on Ambulatory Blood Pressure
After covariate adjustments, we found that Task Strain was associated with momentary elevations in both SBP (b = 0.67, F(1, 23E3) = 8.74,p = .003) and DBP (b = 0.63, F(1,23E3) = 13.15,p < .001). Constraining the Task Strain term to be a fixed effect (random intercept only) significantly reduced model fit for SBP (χ2 = 37.31, df = 2, p < 0.001) and DBP (χ2 = 53.94, df = 2, p < 0.001), suggesting significant individual differences in SBP and DBP reactivity to Task Strain in this sample. In separate models, Social Conflict was also independently associated with momentary elevations in SBP (b = 0.47, F(1, 14E3) = 8.75, p = .003) but not DBP (b = 0.16, F(1, 14E3) = 1.93, p = .16). Constraining Social Conflict to be a fixed effect reduced model fit for SBP (χ2 = 8.04, df = 2, p = .018) and marginally for DBP (χ2 = 5.00, df = 2, p = .08), suggesting significant individual differences in SBP reactivity and marginally significant differences in DBP reactivity to Social Conflict. Although this DBP reactivity finding does not meet conventional standards for statistical significance, we chose to interpret the effect given that these results were significant in the same sample with a slightly different sample size (Kamarck et al., 2018).
Weekly Physical Activity as a Moderator of the Association between Daily Psychosocial Stressors and Ambulatory Blood Pressure
After adjusting for demographics, time-varying covariates, and main effects reported above, a significant interaction emerged between Task Strain and weekly physical activity for both SBP (b = −1.65, F(1, 23E3) = 4.54,p = .033) and DBP (b = −1.30, F(1, 23E3) = 4.81,p = .028). Simple slope analyses revealed that periods of Task Strain were associated with significant increases in SBP (b = 1.14, F(1, 23E3) = 13.02,p <.001) and DBP (b = 1.00, F(1, 23E3) = 17.02, p < 0.001) for less physically active individuals but not for more active individuals (SBP: b = 0.19, F(1, 23E3) =0.38, p = .54; DBP: b = 0.25, F(1, 23E3) = 1.032, p = .29) (see Figure 1). Using comparable models, a significant interaction emerged between Social Conflict and weekly physical activity on DBP (b = −0.89, F(1, 14E3) = 5.43, p = .020). Simple slope analyses revealed that periods of Social Conflict were associated with significant increases in DBP (b = 0.40, F(1, 14E3) = 6.40, p = .011) for less physically active individuals but not for more active individuals (b = −0.11, F(1, 14E3) = 0.49, p =.48) (see Figure 2). Unlike for DBP, there was no significant interaction between Social Conflict and weekly physical activity on SBP (b = −0.61, F(1, 14E3) = 1.28, p = .26). Though this interaction was non-significant, it is interesting to note that simple slope analyses suggested a consistent pattern of significantly elevated SBP for less active individuals but not for more active individuals, as with the other analyses (see Figure 2). In sum, these findings suggest that more physically active individuals show smaller blood pressure responses to daily psychosocial stressors when compared to those who exhibit a less active pattern.
Figure 1.
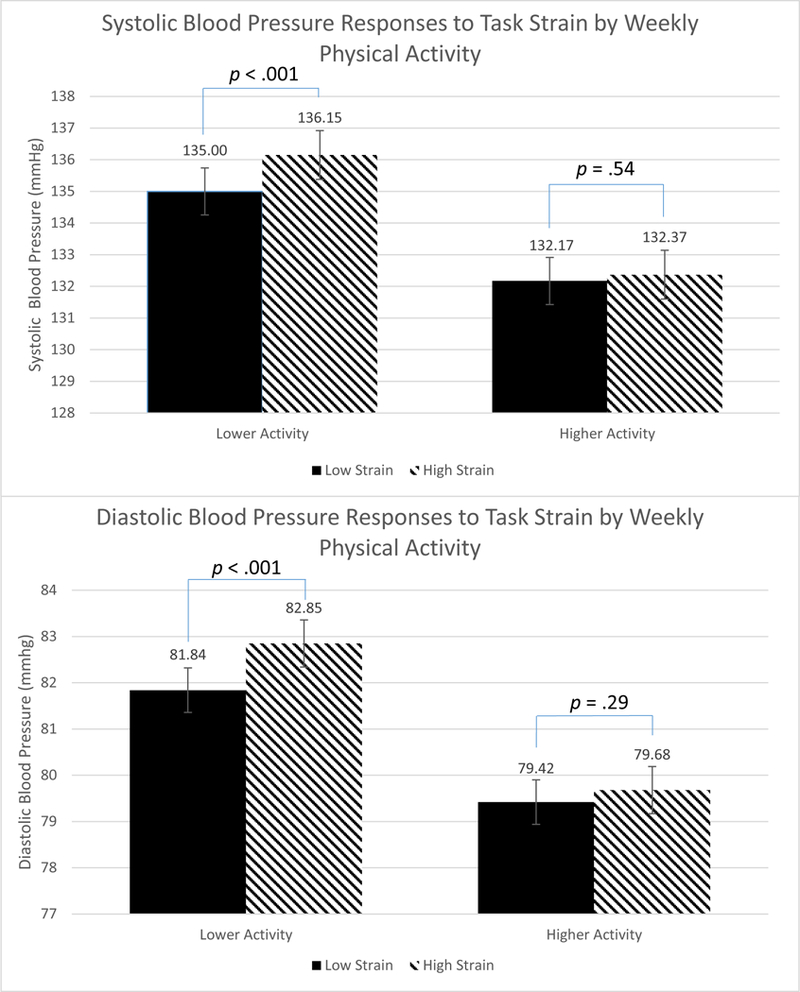
Person-level weekly physical activity as a moderator of the relationship between Ambulatory SBP and DBP Reactivity to Task Strain. N = 463 with complete data. Figures present the data where physical activity measures are centered one standard deviation above (higher activity) and below (lower activity) the sample mean (M = 1.62, SD = 0.29). Data are further stratified by periods of task strain (high demand, low control) versus no task strain. Covariates in this model include sex, age, race, education, and 14 time-varying covariates: standing, sitting, speaking, comfort level (too cold, too hot), recent consumption of meal, snack, caffeine, alcohol, or cigarettes, self-reported physical activity (light, moderate, and vigorous), and metabolic equivalent (METs) in the prior 10 minutes.
Figure 2.
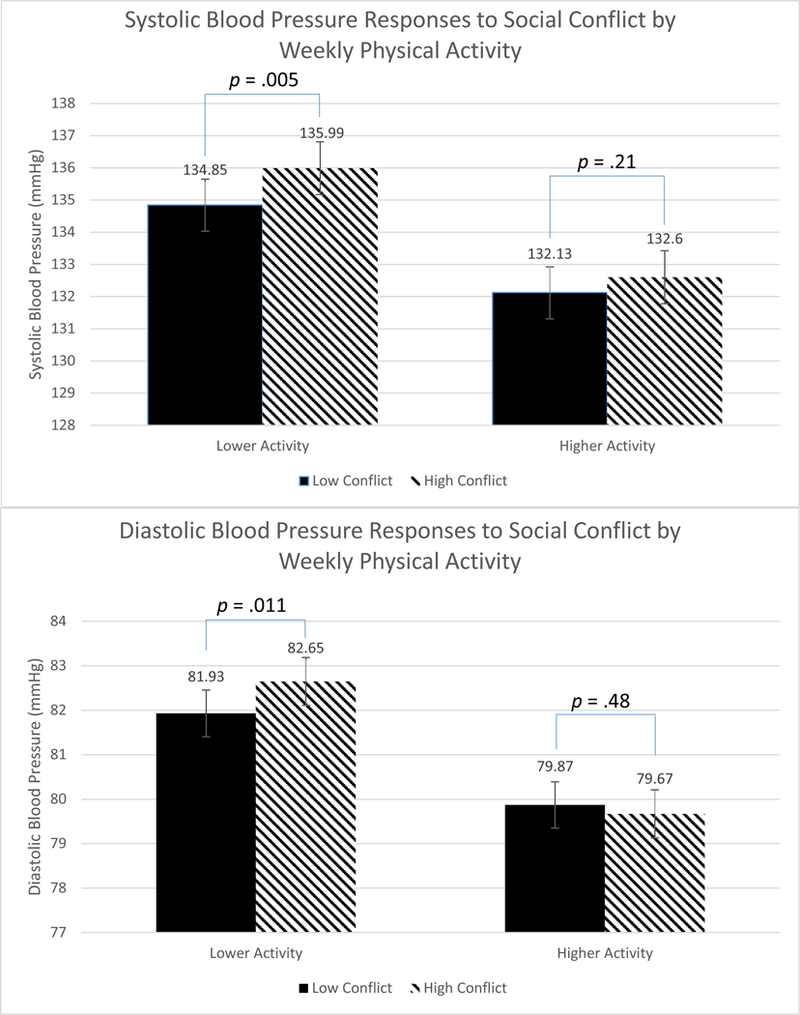
Person-level weekly physical activity as a moderator of the relationship between Ambulatory SBP and DBP Reactivity to Social Conflict. N = 417 with complete data. Figures present the data where physical activity is centered one standard deviation above (higher activity) and below (lower activity) the sample mean (M = 1.62, SD = 0.28), and Social Conflict is centered one standard deviation above (high conflict) and below (low conflict) the sample mean (M = 1.65, SD = 0.91). Covariates in this model include sex, age, race, education, and 14 time-varying covariates: standing, sitting, speaking, comfort level (too cold, too hot), recent consumption of meal, snack, caffeine, alcohol, or cigarettes, self-reported physical activity (light, moderate, and vigorous), and metabolic equivalent (METs) in the prior 10 minutes.
Recent Physical Activity as a Moderator of the Association between Daily Psychosocial Stressors and Ambulatory Blood Pressure
Next, analyses were conducted using the within-subject average METs calculated in the 30 minutes prior to each hourly electronic diary entry in order to understand whether fluctuations in physical activity throughout the day were associated with effects similar to those observed when we compared the activity levels of individuals. These models retained the main effect of weekly physical activity as a covariate in order to detect the independent effects of recent physical activity.
After adjustment for time-varying covariates and main effects, a significant within-person interaction emerged between Task Strain and recent physical activity on DBP (b = −0.45, F(1,24E3 = 4.99, p = .025) but not for SBP (b = −0.20, F(1,24E3)=0.55, p = .46).Consistent with the analyses reported earlier on weekly physical activity, simple slope analyses suggested that periods of Task Strain were associated with significant increases in DBP (b = 1.00, F(1,24E3 ) = 19.50, p <.001) following periods of less activity in the prior 30 minutes. In contrast, Task Strain was not significantly associated with DBP elevations following periods of greater recent activity (b = 0.37, F(1,24E3) = 3.12, p = .08; see Figure 3). Unlike Task Strain, no significant interactions emerged between Social Conflict and recent physical activity on SBP (b = 0.02, F(1,14E3) = 0.01, p = .93) or DBP (b = −0.23, F(1,14E3) = 2.09, p = .15). Only DBP responses to periods of Task Strain were moderated by recent physical activity prior to the stressor.
Figure 3.
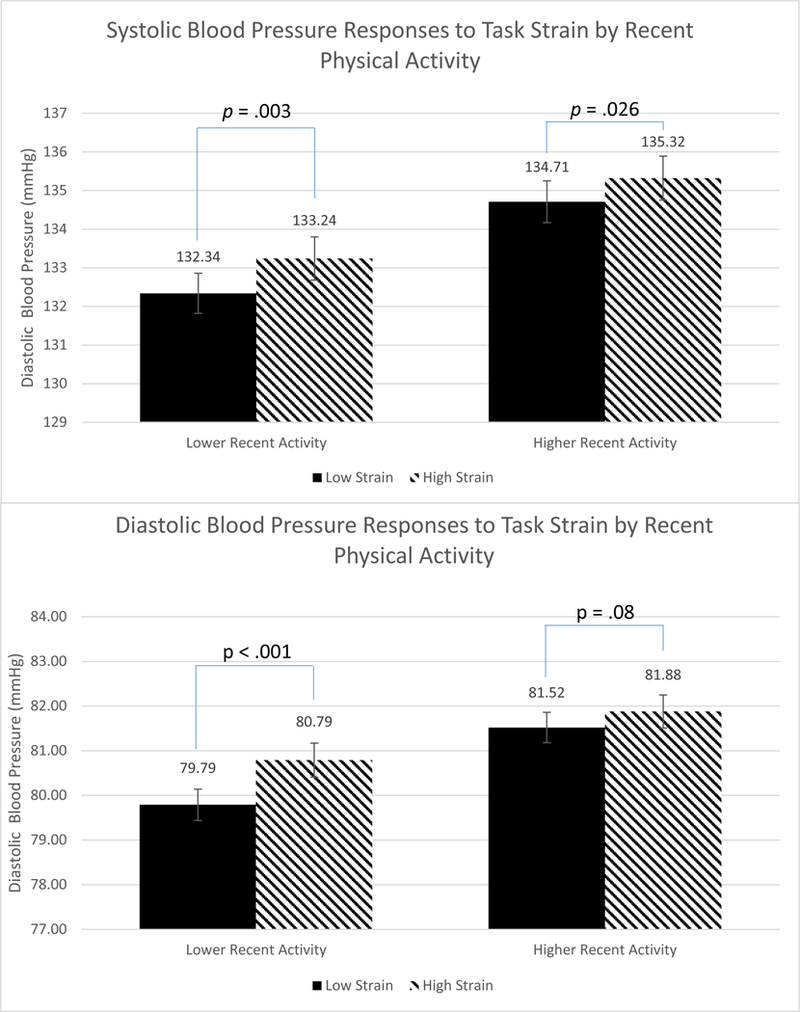
Momentary-level recent physical activity as a moderator of the relationship between Ambulatory SBP and DBP Reactivity and Task Strain. N = 463 with complete data. Figures present the data where physical activity measures are centered one standard deviation above (higher activity) and below (lower activity) the sample mean (M = 1.62, SD = 0.71). Data are further stratified by periods of task strain (high demand, low control) versus no task strain. Covariates in this model include average weekly physical activity and 14 time-varying covariates: standing, sitting, speaking, comfort level (too cold, too hot), recent consumption of meal, snack, caffeine, alcohol, or cigarettes, self-reported physical activity (light, moderate, and vigorous) and metabolic equivalent (METs) in the prior 10 minutes.
Exploratory Analyses
In an exploratory analysis, we sought to understand if the within-person physical activity effects accounted for the between-person effects of physical activity on DBP responses to Task Strain. Both two-way interactions (e.g., Task Strain X weekly physical activity and Task Strain X recent physical activity) were included in these models while controlling for time-varying covariates, demographics, and main effects. For Task Strain, the interaction involving recent physical activity remained significant (b = −0.52, F(1,24E3) = 5.79, p = .0167), but the interaction involving weekly physical activity became non-significant (b = −0.99, F(1,24E3) = 3.00, p = .08). These data are consistent with the possibility that the moderating effects of habitual physical activity on DBP responses to Task Strain may be accounted for, in part, by recent physical activity.
To better understand the intensity of recent physical activity involved in attenuated blood pressure responses to daily psychosocial stressors, we counted the number of minutes in the 30 minutes prior to the hourly interview that were spent in each of the conventional intensity ranges: sedentary (<1.5 METs), light (1.5 – 3.0 METs), and moderate-to-vigorous activity (>3.0 METs). See Table 2 for descriptive statistics. Controlling for time-varying covariates and main effects, multilevel models revealed that the number of minutes in sedentary and light activity but not MVPA moderated SBP and DBP responses to Task Strain (see Table 3). Simple slope analyses revealed that such periods of Task Strain were associated with larger increases in SBP (b = 1.09, F(1,22E3) = 12.71,p < .001) and DBP (b = 1.04, F(1,22E3) = 20.33,p < 0.001) for fewer minutes of recent light physical activity than for more minutes of light physical activity (SBP: b = 0.15, F(1,22E3) = 0.28, p = .594; DBP: b = −0.02, F(1,22E3) = 0.02, p = .899). Unlike for Task Strain, no significant associations emerged in these analyses when ABP responses to Social Conflict were examined. Time spent in light activity was associated with more favorable blood pressure responses to Task Strain, but no such associations emerged for MVPA.
Table 2.
Recent Physical Activity Intensity Ranges
| Physical Activity Ranges | N (in minutes) | SD |
|---|---|---|
| Sedentary (METs < 1.5) | 20.2 | 8.7 |
| Light (METs 1.5 to 3.0) | 8.0 | 6.8 |
| Moderate-to-Vigorous (METs > 3.0) | 2.8 | 5.2 |
Table 3.
Interaction Terms of Daily Psychosocial Stressors and Recent Physical Activity Intensity Ranges
| SBP | DBP | |||||||
|---|---|---|---|---|---|---|---|---|
| Interaction Terms | b | df | F | p | b | df | F | p |
| Task | ||||||||
| Strain*Sedentary | 0.04 | 1(22E3) | 4.63 | .031 | 0.06 | 1(22E3) | 15.05 | <.001 |
| Task Strain*Light | −0.07 | 1(22E3) | 6.89 | .009 | −0.08 | 1(22E3) | 15.94 | <.001 |
| Task Strain*MVPA | 0.02 | 1(22E3) | 0.49 | .49 | −0.02 | 1(22E3) | 0.86 | .35 |
| Social | ||||||||
| Conflict*Sedentary | −0.003 | 1(13E3) | 0.04 | .83 | 0.02 | 1(13E3) | 2.59 | .086 |
| Social Conflict*Light Social | 0.008 | 1(13E3) | 0.19 | .66 | −0.01 | 1(13E3) | 0.6 | .44 |
| Conflict*MVPA | −0.003 | 1(13E3) | 0.02 | .90 | −0.03 | 1(13E3) | 3.2 | .074 |
Discussion
The current investigation assessed the relationship between objective measures of physical activity and ambulatory blood pressure responses to daily psychosocial stressors captured in real time by EMA. This is the first study to demonstrate that individuals exhibiting greater weekly physical activity showed lower stress-related ambulatory SBP and DBP responses compared to their less active counterparts. Interestingly, such effects were shown across two different types of daily psychosocial stressors. The present findings further suggested that physical activity in the prior 30 minutes moderated the relationship between ambulatory DBP and periods of Task Strain. The integration of several novel methodological features in this study may have facilitated the detection of these between-person and within-person effects.
The existing literature on physical fitness and stress-related blood pressure responses has been generally inconsistent, such that two meta-analyses of this literature have reached opposite conclusions. We suspected that blood pressure responses to stress might be more reliably moderated by individual differences in physical activity exposure, and that such effects might emerge more clearly when psychosocial stressors encountered during daily life were examined. Three novel features of the current investigation may explain our positive findings: use of objective measures of physical activity, repeated assessment of natural daily stressors, and statistical control for known confounders of ambulatory blood pressure readings. These methodological improvements in the context of a large, midlife sample extend our understanding of the relationship between physical activity and stress-induced BP responses.
Across the between-person and within-person analyses, there appears to be a more consistent moderating effect for Task Strain than for Social Conflict, and for DBP than for SBP responses. Regarding the first point, analyses with Task Strain may be associated with greater statistical power than analyses with Social Conflict. Experiences of Task Strain were common in this sample, with nearly a third of EMA observations coded as such. However, Social Conflict ratings were generally low in variability. It is possible that the moderating effects of physical activity on the relationship between Social Conflict and ABP were underpowered in the present sample. Regarding the second point, it is unclear why our findings were more consistent for DBP than for SBP. Changes in peripheral vasodilation may be a more important determinant of DBP than SBP, and it is possible that these types of changes are an important mechanism linking physical activity to reduced CVR. For instance, West and colleagues (1998) found significant reductions in DBP reactivity and total peripheral resistance (TPR) but not in SBP reactivity following 20 minutes of moderate activity in a small sample of sedentary adults (but also see Brownley et al., 2003). As the precise mechanisms involved in the attenuating effects of physical activity on BP responses to stress are not well understood, further research in this area is warranted.
There are several limitations to these findings. First, we cannot infer that the differences in physical activity are causally related to the reduced blood pressure reactivity to daily life stressors shown in this study due to the correlational design of this study. The replication of the pattern of effects across within- and between-person analyses are suggestive of a possible causal influence, but experimental studies would be required in order to enable us to ascertain causal inferences. Second, the objective measures of physical activity used here are not designed to capture all forms of physical activity, such as impact and aquatic sports that may damage the accelerometry devices. Despite these device limitations, daily physical activity was measured for a large proportion of the waking day, and excluding those who had endorsed these types of activities did not influence the results. Third, the lack of a statistically significant association between recent MVPA and reactivity in the exploratory analyses is most likely a function of insufficient power due to so few observations. Thus, we cannot draw conclusions about a moderating role of MVPA of ABP responses to daily psychosocial stressors. Finally, we do not have direct measures of cardiorespiratory fitness on the participants in this sample. The gold standard in this literature is maximal oxygen uptake (VO2 max) using a graded exercise test performed on a treadmill. Without such information, we cannot determine the degree to which higher cardiorespiratory fitness, an expected result of regular MVPA, may account for results of the between-person analyses. Future work should examine both physical activity and physical fitness with the goal of understanding which is the “active ingredient” in the moderating effects of physical activity on cardiovascular responses to daily psychosocial stressors.
These physical activity findings have important implications for the design of future interventions intended to reduce cardiovascular responses to stress. To date, the focus of randomized controlled trials (RCTs) in this context have been on aerobic exercise training. The use of exercise training interventions to reduce stressor-provoked BP responses has been somewhat mixed (Hamer et al., 2006), with two large, recent well-controlled RCTs finding null effects of aerobic exercise interventions on CVR (Alex et al., 2013; Sloan et al., 2011). One reason for the inconsistent findings among these studies may be that physical activity is commonly considered a confounder for laboratory-based cardiovascular reactivity testing, resulting in participants being asked to abstain from activity in the hours prior to testing. Rather than being a confounder, acute physical activity may instead play a key role in moderating stressor-evoked BP responses. Future trials should consider the potential role of physical activity in attenuating BP responses in the natural environment to yield more ecologically valid results. An important finding in this study is the attenuating effects of light physical activity on BP responses to daily psychosocial stress. This finding would suggest that lighter periods of activity, rather than only bouts of MVPA used in this literature, may be sufficient to modify BP reactivity. A form of activity that could be performed virtually anywhere, light periods of activity may be particularly advantageous for certain populations where more intense activity may be a barrier or unsafe, such as the elderly or the socioeconomically disadvantaged. Altogether, future research should consider examining the acute effects of physical activity, especially lighter levels, on stressor-evoked BP reactivity measured in the natural environment.
The findings shown in this study represent relatively small effects - for example, differences of only 1–2 mmHg in cardiovascular reactivity were shown between those one standard deviation above and one standard deviation below the mean in regular physical activity. Prior laboratory studies have shown that an increase in blood pressure reactivity of this magnitude may be associated with a mean increase of 0.02 to 0.03 mm increase of carotid intima-medial thickness (IMT; Kamarck et al., 1997), a marker of CVD that, in turn, can be linked with increased risk for myocardial infarction and stroke (van den Oord et al., 2013). Given this link between small changes in reactivity, IMT, and clinical endpoints, we can surmise that even small reductions in reactivity may have positive health implications.
Conclusion
The extant literature has been mixed on the extent to which physical activity attenuates blood pressure responses to stress. These findings from a large, healthy midlife sample suggest that physical activity during daily life may moderate the relationship between daily psychosocial stressors and stress-related ambulatory blood pressure responding, and these results were generally consistent across within- and between-person analyses. Several novel methodological features included here may have facilitated the detection of a relationship between physical activity and cardiovascular responses to stress in the expected direction. Future research should involve experimental designs to ascertain causality, should focus on mechanisms, and should include measures of cardiorespiratory fitness. These current findings are consistent with the possibility that physical activity may be an important moderator of the relationship between daily psychosocial stressor exposure and cardiovascular health.
Acknowledgements:
I would like to acknowledge and thank Aidan Wright for his statistical consultation, and Barbara Anderson and the AHAB staff for their role in data collection and preparation.
Source of Funding: This research was supported by the National Heart, Lung, and Blood Institute (HL040962, 4T32HL007560).
Footnotes
Conflicts of Interest: No conflicts of interest were declared.
43 participants reported at least one bout of water or impact sports during the 4-day monitoring period. Removing these participants from subsequent analyses did not alter the general pattern of findings. Thus, the removal of the SenseWear device during these types of activities appear not to confound the results reported here.
References
- Aiken LS, & West SG (1991). Multiple regression: Testing and interpreting interactions. Newbury Park: Sage. [Google Scholar]
- Alex C, Lindgren M, Shapiro PA, McKinley PS, Brondolo EN, Myers MM, … Sloan RP (2013). Aerobic exercise and strength training effects on cardiovascular sympathetic function in healthy adults: a randomized controlled trial. Psychosomatic medicine, 75(4), 375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brownley KA, Hinderliter AL, West SG, Girdler SS, Sherwood A, & Light KC (2003). Sympathoadrenergic mechanisms in reduced hemodynamic stress responses after exercise. Medicine & Science in Sports & Exercise, 35(6), 978–986. [DOI] [PubMed] [Google Scholar]
- Caspersen CJ, Powell KE, & Christenson GM (1985). Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public health reports, 100(2), 126. [PMC free article] [PubMed] [Google Scholar]
- Chida Y, & Steptoe A (2010). Greater cardiovascular responses to laboratory mental stress are associated with poor subsequent cardiovascular risk status. Hypertension, 55(4), 1026–1032. [DOI] [PubMed] [Google Scholar]
- Davy KP, Miniclier NL, Taylor JA, Stevenson ET, & Seals DR (1996). Elevated heart rate variability in physically active postmenopausal women: a cardioprotective effect? American Journal of Physiology-Heart and Circulatory Physiology, 271(2), H455–H460. [DOI] [PubMed] [Google Scholar]
- Forcier K, Stroud LR, Papandonatos GD, Hitsman B, Reiches M, Krishnamoorthy J, & Niaura R (2006). Links between physical fitness and cardiovascular reactivity and recovery to psychological stressors: A meta-analysis: American Psychological Association. [DOI] [PubMed] [Google Scholar]
- Goodwin J, Bilous M, Winship S, Finn P, & Jones SC (2007). Validation of the Oscar 2 oscillometric 24-h ambulatory blood pressure monitor according to the British Hypertension Society protocol. Blood Pressure Monitoring, 12, 113–117. [DOI] [PubMed] [Google Scholar]
- Hamer M, Taylor A, & Steptoe A (2006). The effect of acute aerobic exercise on stress related blood pressure responses: a systematic review and meta-analysis. Biological psychology, 71(2), 183–190. [DOI] [PubMed] [Google Scholar]
- Hoffman L (2015). Longitudinal analysis: Modeling within-person fluctuation and change: Routledge. [Google Scholar]
- Jackson EM, & Dishman RK (2006). Cardiorespiratory fitness and laboratory stress: A meta-regression analysis. Psychophysiology, 43(1), 57–72. [DOI] [PubMed] [Google Scholar]
- Jones CS, Bilous M, Winship S, Finn P, & Goodwin J (2004). Validation of the OSCAR 2 oscillometric 24-hour ambulatory blood pressure monitor according to the International Protocol for the validation of blood pressure measuring devices. Blood Pressure Monitoring, 9, 219–223. [DOI] [PubMed] [Google Scholar]
- Joseph NT, Kamarck T, Muldoon MF, & Manuck SB (2014a). Daily marital interaction quality and carotid intima-medial thickness in healthy middle-aged adults. Psychosomatic medicine, 76, 347–354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joseph NT, Kamarck TW, Muldoon MF, & Manuck SB (2014b). Daily Marital Interaction Quality and Carotid Artery Intima Medial Thickness in Healthy Middle Aged Adults. Psychosomatic medicine, 76(5), 347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joseph NT, Muldoon MF, Manuck SB, Matthews KA, MacDonald LA, Grosch J, & Kamarck TW (2016). The Role of Occupational Status in the Association Between Job Strain and Ambulatory Blood Pressure During Working and Nonworking Days. Psychosomatic medicine, 78(8), 940–949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamarck TW, Everson SA, Kaplan GA, Manuck SB, Jennings JR, Salonen R, & Salonen JT (1997). Exaggerated blood pressure responses during mental stress are associated with enhanced carotid atherosclerosis in middle-aged Finnish men: findings from the Kuopio Ischemic Heart Disease Study. Circulation, 96(11), 3842–3848. [DOI] [PubMed] [Google Scholar]
- Kamarck TW, Janicki DL, Shiffman S, Polk DE, Muldoon MF, Liebenauer LL & Schwartz JE (2002). Psychosocial demands and ambulatory blood pressure: A field assessment approach. Physiology and Behavior, 77, 699–704. [DOI] [PubMed] [Google Scholar]
- Kamarck TW, Li X, Wright AG, Muldoon MF, & Manuck SB (2018). Ambulatory Blood Pressure Reactivity as a Moderator in the Association Between Daily Life Psychosocial Stress and Carotid Artery Atherosclerosis. Psychosomatic medicine. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamarck TW, & Lovallo WR (2003). Cardiovascular reactivity to psychological challenge: conceptual and measurement considerations. Psychosomatic medicine, 65(1), 9–21. [DOI] [PubMed] [Google Scholar]
- Kamarck TW, Schwartz JE, Janicki DL, Shiffman S & Raynor DA (2003). Correspondence between laboratory and ambulatory measures of cardiovascular reactivity: A multilevel modeling approach. Psychosomatic medicine, 40, 675–683. [DOI] [PubMed] [Google Scholar]
- Karasek RA Jr (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative science quarterly, 285–308. [Google Scholar]
- Kohl HW, Blair SN, Paffenbarger RS, Macera CA, & Kronenfeld JJ (1988). A mail survey of physical activity habits as related to measured physical fitness. American Journal of Epidemiology, 127(6), 1228–1239. [DOI] [PubMed] [Google Scholar]
- Mackey DC, Manini TM, Schoeller DA, Koster A, Glynn NW, Goodpaster BH, … Cummings SR (2011). Validation of an armband to measure daily energy expenditure in older adults. Journal of Gerontology: Medical Sciences, 66A, 1108–1113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michelini LC, & Stern JE (2009). Exercise-induced neuronal plasticity in central autonomic networks: role in cardiovascular control. Experimental physiology, 94(9), 947–960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monahan KD, Dinenno FA, Tanaka H, Clevenger CM, DeSouza CA, & Seals DR (2000). Regular aerobic exercise modulates age-associated declines in cardiovagal baroreflex sensitivity in healthy men. The Journal of physiology, 529(1), 263–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan JA, Corrigan F, & Baune BT (2015). Effects of physical exercise on central nervous system functions: a review of brain region specific adaptations. Journal of molecular psychiatry, 3(1), 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oliveira-Silva I, Leicht AS, Moraes MR, Simões HG, Del Rosso S, Córdova C, & Boullosa DA (2016). Heart Rate and Cardiovascular Responses to Commercial Flights: Relationships with Physical Fitness. Frontiers in Physiology, 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson LM, Miller KG, Wong PM, Anderson BP, Kamarck TW, Matthews KA, … Manuck SB (2017). Sleep duration partially accounts for race differences in diurnal cortisol dynamics. Health Psychology, 36(5), 502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petruzzello SJ, Landers DM, Hatfield BD, Kubitz KA, & Salazar W (1991). A meta-analysis on the anxiety-reducing effects of acute and chronic exercise. Sports medicine, 11(3), 143–182. [DOI] [PubMed] [Google Scholar]
- Ritvanen T, Louhevaara V, Helin P, Halonen T, & Hanninen O (2007). Effect of aerobic fitness on the physiological stress responses at work. International Journal of Occupational Medicine and Environmental Health, 20(1), 1–8. [DOI] [PubMed] [Google Scholar]
- Salmon P (2001). Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clinical psychology review, 21(1), 33–61. [DOI] [PubMed] [Google Scholar]
- Sloan RP, Shapiro PA, DeMeersman RE, Bagiella E, Brondolo EN, McKinley PS, … Myers MM. (2011). The Impact of Aerobic Training on Cardiovascular Reactivity to and Recovery from Challenge. Psychosomatic medicine, 73(2), 134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treiber FA, Kamarck TW, Schneiderman N, Sheffield D, Kapuku G, & Taylor T (2003). Cardiovascular reactivity and development of preclinical and clinical disease states. Psychosomatic medicine, 65, 46–62. [DOI] [PubMed] [Google Scholar]
- Tulppo MP, Hautala AJ, Makikallio TH, Laukkanen RT, Nissilä S, Hughson RL, & Huikuri HV (2003). Effects of aerobic training on heart rate dynamics in sedentary subjects. Journal of Applied Physiology, 95(1), 364–372. [DOI] [PubMed] [Google Scholar]
- van den Oord SC, Sijbrands EJ, Gerrit L, van Klaveren D, van Domburg RT, van der Steen AF, & Schinkel AF (2013). Carotid intima-media thickness for cardiovascular risk assessment: systematic review and meta-analysis. Atherosclerosis, 228(1), 1–11. [DOI] [PubMed] [Google Scholar]
- West SG, Brownley KA, & Light KC (1998). Postexercise vasodilatation reduces diastolic blood pressure responses to stress. Annals of Behavioral Medicine, 20(2), 77–83. [DOI] [PubMed] [Google Scholar]