

Abstract
Objectives We present a patient with a prolactin-secreting adenoma with extensive secondary, noninfectious, xanthogranulomatous changes due to remote intratumoral bleeding and provide a literature review of xanthogranulomas (XGs) of the sellar region with emphasis on prolactinomas with xanthogranulomatous features.
Design Case report, with PubMed search of cases of sellar XG, focusing on neuroimaging and surgical approach.
Results A 35-year-old male was found to have a large sellar/suprasellar calcified/cystic mass. Endoscopic transsphenoidal approach for extradural resection was performed and diagnosis made. Review generated 31 patients with the diagnosis of sellar XG. In a minority (6 patients), the underlying lesion for the XG was a pituitary adenoma. Headache was the most common presenting symptom and panhypopituitarism the most common endocrinological abnormality. Examples of hyperprolactinemia associated with sellar XG are also uncommon and due to stalk effect. Neuroimaging of XG on T1-weighted magnetic resonance imaging (MRIs) showed 18 cases (56.3%) were hyperintense, 1 case (3.13%) was isointense, 4 (12.5%) had mixed-signal intensity, and 2 (6.25%) were hypointense. On T2-weighted MRIs, five lesions (15.6%) were hyperintense, three (9.38%) were isointense, nine (28.1%) were heterogeneous, and nine (28.1%) were hypointense. Only one case (3.1%) had calcifications on computed tomography scan similar to ours. In 14 cases (43.7%), the lesions enhanced with contrast administration on MRI.
Conclusion Prolactinomas with secondary xanthogranulomatous change represent a rare cause of XG of the sella. With no radiological or clinical signs specific for XG of the sellar region, preoperative diagnosis can be challenging, if not impossible.
Keywords: prolactinoma, xanthogranuloma, endoscopic transphenoidal, pituitary adenoma, craniopharyngioma
Introduction
Paulus et al first described a series of xanthogranulomas (XGs) of the sella in 1999, recognizing that these differed from adamantinomatous craniophanygioma. 1 XG contrasts with craniopharyngioma in its presentation, prognosis, and histological features. The origin of XG is unclear in some cases, although reports since Paulus et al have usually identified remnants of Rathke's cleft cyst (RCC), often with remote hemorrhage, as a predecessor for a significant subset of these lesions. 2 3 Few reports describe an association with adamantinomatous craniopharyngiomas or pituitary adenomas, 2 4 and even fewer describe prolactinomas with xanthogranulomatous features.
In this report, we present a rare case of a prolactinoma (sparsely granulated lactotroph adenoma) with xanthogranulomatous features and provide a comprehensive review of literature of similar cases described in the literature, focusing on examples without underlying craniopharyngioma. We also review the histological features, clinical, and radiographic description of XGs of the sellar region.
Methods
The methods for pituitary tissue processing, staining, and immunostaining were as previously described. 2
The literature review was conducted to identify all reported cases of XG of the sellar region. PubMed was employed as the search engine, using the following keywords: XG of sellar region, pituitary adenoma, and XG. Articles between the years 2002 and 2016 were searched.
Inclusion Criteria
Articles were included for review if they contained a formal histopathological description of XG exclusively within the sellar/suprasellar region. In addition, articles also had to include a neuroimaging description of the lesion, reports of pituitary function tests prior to intervention, and a detailed summary of the surgical intervention.
Exclusion Criteria
Articles were excluded if the histopathology report included features of craniopharyngioma or if there was no clear mention of endocrinology status in the report.
Case Report
This 35-year-old African American male had been referred to the senior neurosurgeon (SY) for treatment of a cystic, calcified mass of the sellar region diagnosed 13 months prior. The mass had been found incidentally after the patient had been arrested following an altercation in which he received a blow to the head. On admission to an outside hospital, computed tomography (CT) scan had shown a 6.5 × 5.1 × 4.0 cm mass. The CT scan showed calcification along the capsule of the cyst. The mass resulted in elevation of the optic chiasm, expansion of the sella, and compression of the hypothalamus, hippocampi, and brain stem ( Fig. 1 ).
Fig. 1.

Preoperative T1 contrasted magnetic resonance imagings showing mixed signal intensity with expansion of the sella and caudal displacement of the optic chiasm. ( A ) Coronal view. ( B ) Sagittal view. Preoperative computed tomography scan of the head showing calcifications of the cyst wall. ( C ) Coronal view. ( D ) Sagittal view.
A partial endocrinological workup had been performed and, by report from the outside hospital, his prolactin level soon after the mass was identified was “in the 1500s.” His endocrinologist had placed him on cabergoline 0.5 twice a week and then 6 months later his care was transferred to our facility, due to incarceration. At that time his prolactin level had decreased dramatically to 22 and the endocrinologist then changed his cabergoline to 1.5 biweekly; he received this dose for 6 months, with the last prolactin level drawn 3 months prior to surgery, where it had increased to 59.1. There was a history of noncompliance with the medication. Neuroimaging from the outside hospital was not available on transfer but, by report, the size of the very large lesion appeared to be unchanged in size after medical therapy was initiated.
On transfer to our facility, he underwent formal visual field testing which showed a dense bitemporal hemianopia. He reported decreased energy but no nausea, vomiting, fever, headache, diplopia, seizures, or gait disturbance.
After admission, surgical resection was recommended. Although craniopharyngioma was a consideration, which would have required an expanded endoscopic approach, because the sella was widely expanded by the tumor, an endoscopic trans-sphenoidal approach to the sella was chosen.
Intraoperatively on direct inspection, the contents of the tumor were consistent with liquefied old blood and necrotic tissue. The capsule was calcified and extended up to the diencephalon, the circle of Willis, and medial walls of cavernous sinuses ( Fig. 2 ).
Fig. 2.
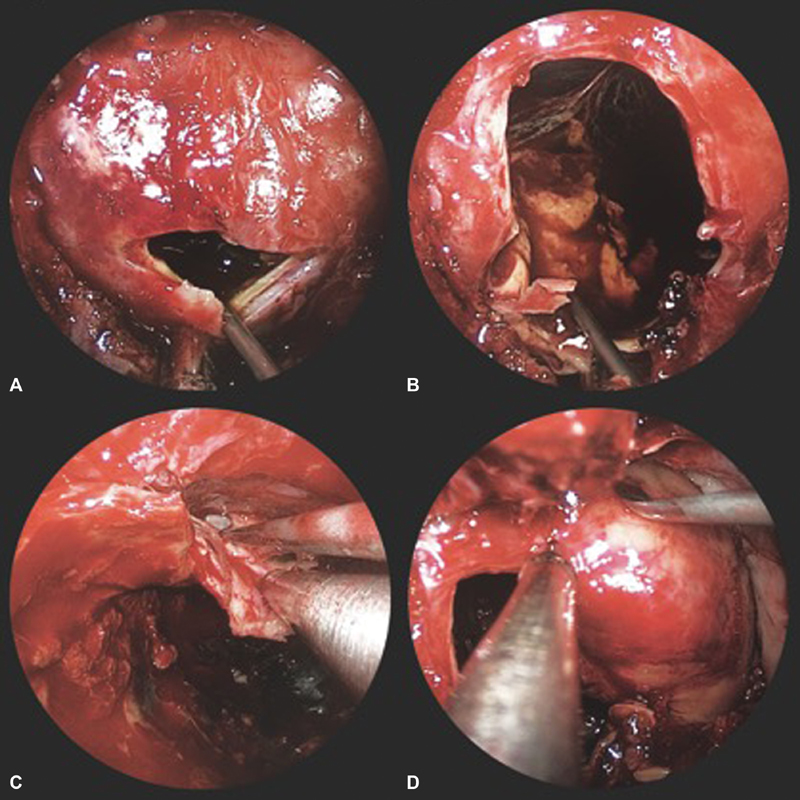
Intraoperative endoscopic view of the sellar lesion. ( A ) Incision of the capsule. ( B ) Inside view. ( C ) Bimanual dissection of the anterior capsule. ( D ) Dissection of the lateral capsule.
The capsule was tightly adherent to the skull base dura; however, a dissection plane was established between the capsule and surrounding dura over the parasellar structures. Using bimanual technique, the majority of the capsule was dissected, leaving only the posterosuperior portion on the underlying hypothalamus, brain stem, and neurovascular structures. Postoperatively, he did well without diabetes insipidus. Three months after surgery, the bitemporal hemianopsia was significantly improved from the preoperative deficit, and the prolactin levels had decreased to 25 ng/mL. A postoperative MRI of the brain showed a decrease in resection cavity volume, with decompression of the optic chiasm. It also shows the calcification of the highest point of the capsule that was tightly adherent to the diencephalon and the circle of Willis ( Fig. 3 ).
Fig. 3.

Postoperative T1 contrasted magnetic resonance imagings showing tumor resection with empty tumor cavity and decompression of mass effect to the parasellar structures. ( A ) Coronal view. ( B ) Sagittal view.
At last follow-up, 2 years post-surgery his main problem is hypogonadism for which he has been prescribed Androgel 20.25 mg/L 25 g gel in dose pump.
Histological Features
At surgery, three frozen sections showed XG and possible residual adenoma but no craniopharyngioma. Permanent materials measured in aggregate 6.6 × 4.1 × 1.6 cm. and histologically the vast majority of the specimen was composed of cholesterol clefts, multinucleated giant cells ( Fig. 4A ), fibrosis ( Fig. 4A ), organizing hemorrhage ( Fig. 4A ), metaplastic bone ( Fig. 4B , arrowhead), and very scant residual monomorphic adenoma at the periphery of the mass ( Fig. 4B , arrow). The latter was estimated to compose <15% of the overall volume of resected materials. Extensive golden-brown hemosiderin pigment and cholesterol clefts ( Fig. 4C ) attested to hemorrhage, likely repeated, as the cause of the XG component. The residual adenoma was strongly and diffusely immunoreactive for prolactin in the typical Golgi pattern of the common sparsely granulated lactotroph adenoma ( Fig. 4D , lower right).
Fig. 4.

Pathological slides showing ( A ) cholesterol clefts, multinucleated giant cells fibrosis organizing hemorrhage; ( B ) metaplastic bone (arrowhead), and very scant residual monomorphic adenoma at the periphery of the mass (arrow). The latter was estimated to compose <15% of the overall volume of resected materials; ( C ) extensive golden-brown hemosiderin pigment and cholesterol clefts attested to hemorrhage, likely repeated, as the cause of the xanthogranuloma component; ( D ) the residual adenoma was strongly and diffusely immunoreactive for prolactin in the typical Golgi pattern of the common sparsely granulated lactotroph adenoma (lower right).
Results of Literature Review
Using the criteria listed above, we identified 17 published cases, reporting a total of 31 patients with the diagnosis of sellar XG unrelated to craniopharyngioma between 2002 and 2016. Including our case, a total of 32 patients were identified ( Table 1 ). 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Patients' ages ranged from 5 to 67 years old (mean age 34.9, median 34.5), with 18 men and 14 women (ratio 1.3:1).
Table 1. Summary of xanthogranulomas of the sellar region.
| Author(s) | Year published | Age, years | Sex | Pathology | Pituitary function test | Presentation | Treatment | Follow-up, month | Outcome | MRI appearance |
|---|---|---|---|---|---|---|---|---|---|---|
| Ben Nsir et al 3 | 2015 | 17 | W | Xanthogranuloma | ↓ TSH, ↓ FSH, ↓LH, ↑ prolactin 50.2 | Primary amenorrhea | Transcranial | 84 | Unchanged | T1: H + enhancement. T2:L |
| Gurcay et al 4 | 2016 | 45 | W | Xanthogranuloma | Normal | Headaches, 3rd nerve palsy | Endoscopic transnasal | 15 | Asymptomatic | T1: I + enhancement, T2: I |
| Stepan et al 5 | 2015 | 35 | M | Juvenile xanthogranuloma | Normal | Headaches, blurry vision, facial lesions | Biopsy | N/A | N/A | N/A |
| Rahmani et al 6 | 2015 | 15 | M | Xanthogranuloma | ↓ IGF | Headaches | Endoscopic transsphenoidal transplanum transtuberculum | 115 | Polyglandular autoimmune syndrome | N/A |
| 2015 | 66 | W | Benign cyst lining with xanthogranuloma | Normal | Progressive vision loss | Endoscopic transsphenoidal transplanum transtuberculum | 90 | Improved vision | N/A | |
| 2015 | 42 | W | Xanthogranuloma with cholesterol clefts | Normal | Vision loss left eye | Endoscopic transsphenoidal transplanum transtuberculum | 54 | Asymptomatic | T1: +enhancement | |
| 2015 | 49 | W | Xanthogranuloma | ↓ Testosterone, ↓LH, ↑ Prolactin | Headaches | Endoscopic transsphenoidal transplanum transtuberculum | N/A | N/A | T1: +enhancement | |
| Nishiuchi et al 7 | 2012 | 47 | M | Xanthogranuloma | ↓ Testosterone, ↓IG-F, ↓ Cortisol | Headache, fatigue loss | Transsphenoidal | N/A | Improved Vision | T1: E + enhancement. T2: E |
| Agarwal et al 8 | 2012 | 41 | M | Xanthogranuloma | Pan-hypopituitarism | Headache, syncope | Transsphenoidal | N/A | N/A | T1: H + enhancement. T2:L |
| Kamoshima et al 9 | 2011 | 8 | W | Xanthogranuloma | DI | Headache, bitemporal hemianopsia | Transsphenoidal | 39.5 | Improved hypopituitarism | T1: H T2: L |
| 11 | M | Xanthogranuloma | DI | Headache, bitemporal hemianopsia | Transsphenoidal | 39.5 | Improved DI | T1: H T2: I | ||
| 12 | W | Xanthogranuloma | Pan-hypopituitarism | Dwarfism | Transcranial | 39.5 | Improved hypopituitarism | T1: E T2: E | ||
| 10 | W | Xanthogranuloma | Normal | Headache, bitemporal hemianopsia | Transsphenoidal | 39.5 | Improvement | T1: H T2: E | ||
| 5 | M | Xanthogranuloma | DI | Polydipsia | Transsphenoidal | 39.5 | Improved DI | T1: H T2: L | ||
| Miyajima et al 10 | 2011 | 58 | M | Rathke's cleft cyst with xanthogranuloma | Normal | Headaches, bitemporal hemianopsia | Transcranial | N/A | DI | T1: H T2: E |
| Nishioka et al 11 | 2010 | 33 | M | Pituitary adenoma with xanthogranuloma | Pan-hypopituitarism | Visual disturbance | Transsphenoidal | N/A | N/A | T1: H +enhancement T2: L |
| 50 | W | Pituitary adenoma with xanthogranuloma | Pan-hypopituitarism | Visual disturbance | Transsphenoidal | N/A | N/A | T1: H +enhancement T2: E | ||
| 56 | W | Pituitary adenoma with xanthogranuloma | Pan-hypopituitarism | Headaches | Transsphenoidal | N/A | N/A | T1: H +enhancement T2: H | ||
| 62 | W | Pituitary adenoma with xanthogranuloma | ↓ Testosterone, ↓GH | Visual disturbance | Transsphenoidal | N/A | N/A | T1: E +enhancement T2: E | ||
| 67 | W | Pituitary adenoma with xanthogranuloma | ↓ Testosterone, ↓ACTH | Visual disturbance | Transsphenoidal | N/A | N/A | T1: E +enhancement T2: E | ||
| Sulentić et al 12 | 2010 | 41 | M | Xanthogranuloma | Pan-hypopituitarism | Headaches, loss of libido | Transsphenoidal | 6 | N/A | N/A |
| Arai et al 13 | 2010 | 55 | W | Xanthogranuloma | ↓ GH, ↓FSH, LH, ↓ACTH | Headaches, bitemporal hemianopsia | Transsphenoidal | 18 | Improvement | T1: H -enhancement T2: E |
| Sugata et al 14 | 2009 | 26 | M | Xanthogranuloma | ↓ GH, ↓FSH, LH, ↓Cortisol | Fatigue, polydipsia, bitemporal hemianopsia | Transcranial | 3 | Hypopituitarism | T1: L +enhancement T2: L |
| Liu et al 15 |
2008 | 32 | M | Xanthogranuloma | ↑ Prolactin 39.6 | Hydrocephalus | Transcranial | 6 | Improvement | T1: H -enhancement T2: H |
| Tajima et al 16 | 2006 | 9 | M | Xanthogranuloma | ↓ GH, ↓FSH | Polyuria, polydipsia | Transsphenoidal | 12 | DI, improved pituitary function tests | T1: H -enhancement T2: H |
| 6 | M | Xanthogranuloma | ↑ GH, ↑ FSH | Polyuria, polydipsia | Transsphenoidal | 12 | DI, improved pituitary function test | T1: H -enhancement T2: L | ||
| Jung et al 17 | 2006 | 57 | W | Xanthogranuloma | Normal | Headache, bitemporal hemianopsia | Transsphenoidal | N/A | Improved visual fields | T1: H +enhancement T2: H |
| 5 | M | Xanthogranuloma | ↓ ACTH, ↓TSH | Headache | Transcranial | N/A | N/A | T1: L T2: L | ||
| Burt et al 18 | 2003 | 29 | M | Xanthogranuloma | ↓ Cortisol, ↓TSH, ↓ Testosterone | Headache, loss of libido, bitemporal hemianopsia | Transsphenoidal | 18 | Improved visual fields | T1: E +enhancement T2: E |
| 26 | M | Xanthogranuloma | Pan-hypopituitarism, ↑ Prolactin 38 | Loss of libido | Transcranial | 8 | Persistent pan-hypopituitarism | T1: H -enhancement T2: H | ||
| Yonezawa et al 19 | 2003 | 67 | M | Xanthogranuloma | Pan-hypopituitarism | Fatigue, weight loss | Transsphenoidal | 3 | Persistent pan-hypopituitarism | T1: H -enhancement T2: L |
| Current report | 2015 | 34 | M | Pituitary adenoma with xanthogranuloma | ↑ Prolactin 1500 | Bitemporal hemianopsia | Endoscopic transnasal | 3 | Improved prolactin and visual fields | T1: H T2: I |
Abbreviations: ↑, Increased; ↓, Decreased; ACTH, adrenocorticotropic hormone; DI, diabetes insipidus; E, heterogeneous; E, heterogeneous; FSH, follicle-stimulating hormone; GH, growth hormone; H, hyperintense; I, isointense; L, hypointense; LH, luteinizing hormone; MRI, magnetic resonance imaging; TSH, thyroid-stimulating hormone.
Headache was the most common presenting symptom in 17 cases (53.1%). Seven cases (21.9%) presented with visual disturbance, seven cases (21.9%) with endocrinological disturbance, and one case with hydrocephalus.
The most common endocrinological abnormality was panhypopituitarism, which was present in 17 cases (53.1%). Seven cases (21.9%) presented with normal pituitary function, and hyperprolactinemia was noted in only four cases (12.5%). In one case, the patient was reported to have had hyperprolactinemia; however, the actual value was not provided. In three cases, prolactin elevation could be explained by stalk effect. In Ben Nsir et al case report, it was determined that the elevation of the prolactin levels was secondary stalk effect. 3 Thus, to our knowledge this is the only reported case wherein the patient had a functioning prolactin secreting pituitary adenoma.
Radiologic Features
In 13 cases (40.6%), the lesions were described as solid, 10 cases (31.3%) were mixed solid and cystic, and 4 cases (12.5%) were purely cystic on MRI. Five cases (15.6%) were not described in sufficient morphologic detail. Four cases (12.5%) were described to have hemorrhagic contents and only one case (3.1%) had calcifications on CT scan. In 14 cases (43.7%), the lesions enhanced with contrast administration on MRI.
On T1-weighted MRIs, 18 cases (56.3%) were hyperintense, one case (3.13%) was iso-intense, four (12.5%) had mixed-signal intensity, and two (6.25%) were hypointense.
On T2-weighted MRIs, five lesions (15.6%) were hyperintense, three (9.38%) were isointense, nine (28.1%) were heterogeneous, and nine (28.1%) were hypointense. In the remaining four reports, the complete MRI description was not provided.
Of the 31 cases identified in the literature review, one case reported a benign cyst with XG, and another reported a RCC with XG. In only six patients, the diagnosis of pituitary adenoma with xanthogranulomatous features was confirmed.
Discussion
In 1999, Paulus et al described them as a separate entity from craniopharyngiomas with subsequent reports of them being associated with hemorrhage or rupture of Rathke's cleft. 1 2 Sellar XGs can be easily mistaken for craniopharyngioma, which significantly impacts the management strategy including the selection of the surgical approach and outcome prediction.
Incidence
Jun et al reported XGs of the sellar region with an incidence of 1.2% in a series of 159 patients with sellar and parasellar lesions. 17 In another study, Rahmani et al reported an incidence of only 0.6% of such tumors in a series of 643 patients who underwent endoscopic endonasal procedures between 2003 and 2013. 6 Discovering hyperprolactinemia together with XG is rare and usually not due to a pituitary adenoma. In a review by Nishioka et al of 231 consecutive cases of patients undergoing pituitary adenoma resection, only five (0.02%) were found to have xanthogranulomatous features. 11 All five of their cases were nonsecreting adenomas, unlike our case that was a functioning, prolactin-secreting adenoma. Additionally, all five cases of XG described in this same review presented with some degree of pituitary insufficiency. To our knowledge, there is no other report of a functional prolactinoma with XG. In a case described by Ben Nsir et al in a 17-year old woman with primary amenorrhea proved to have hyperprolactinemia due to stalk effect since no adenoma was found. 3 In this case, the tumor had originally been thought to be a craniopharyngioma because the capsule was adherent to the pituitary stalk, which is a common site of origin of craniopharyngiomas. 20 This contrasts with our case because the tumor expanded the sella and suprasellar dura against the parasellar structures such as cavernous sinuses, the diencephalon, and blood vessels rather than the pituitary stalk. Given the cabergoline treatment in our case, it is possible that this contributed to the hemorrhage, although by history the patient had been noncompliant with his medication and the size of the mass when originally encountered was very similar by report to that prior to his surgery. Therefore, we feel the best explanation is a spontaneous hemorrhage into his sparsely granulated lactotroph adenoma prior to his initial presentation.
Histology and Etiology of XGs
The histopathology of XG is characterized by an accumulation of foamy macrophages, multinucleated giant cells, cholesterol clefts, lymphocytic infiltration, deposits of hemosiderin, and fibrous proliferation. 6 Immunohistochemistry is positive for factor XIIIa, CD 68, and vimentin with variable expression of S100. 5 As described by Kleinschmidt-DeMasters et al 2 and Burt et al, 18 xanthomatous lesions of the sella which include XH, XGH, and XG have been hypothesized to represent a continuum or spectrum. 2 18 In the series of 23 cases from our joint adult and pediatric hospitals, Kleinschmidt-DeMasters et al identified 10 sellar XG cases associated with epithelium from RCC, 5 XG cases associated with scant epithelium with or without associated mucin and thus no definitive underlying cause, and 5 with no underlying epithelium, tumor or causation for the sellar XG. Only two were related to adamantinomatous craniopharyngioma, one to epidermoid cyst and one to pituitary adenoma, the current case which is detailed in the current report. 2
Thus, while an underlying RCC is found in a significant subset of XGs of the sella, the etiology and pathogenesis of many examples of this entity remain unclear. The granulomatous entity might occur secondary to inflammation, hemorrhage, infarction, or necrosis. 21 It is thought that the xanthogranulomatous reaction is due to a chronic inflammatory reaction in craniopharyngiomas and in the cyst wall of RCC. 1 7 In pituitary adenomas, degenerative changes can also be a factor. 7 In our case, we noted the presence of old liquefied blood during the decompression, and this likely explains the development of xanthogranulomatous features.
Radiology
The preoperative diagnosis of these lesions is challenging as they do not have distinct morphologic or radiographic features. In the series by Nishioka et al, they noted that all adenomas with XGs had mixed signal intensity on both T1- and T2-weighted images with heterogeneous enhancement. 11 In Yang's et al series, contrast-enhanced T1-weighted images revealed rim enhancement in seven cases and heterogeneous enhancement of the entire solid tumor in four cases. 21 Other studies have made the observation that XGs could be characterized by hypointensity of T2-weighted images and iso-intensity to hyperintensity on T1-weighted imaging. 9 11 16 19 21 These findings can be representations of portions composed mainly of cholesterol clefts. 3 However, these findings are not solely applicable to XGs as craniopharyngiomas can also present with heterogeneous signal intensity in T1- and T2-weighted images as well as T2-hypointensity caused by calcifications. In contrast to craniopharyngiomas, calcification is a rare finding in sellar XGs, which can facilitate the differentiation. 9 14 21
In our case, the lack of contrast enhancement and the T2 isointensity with T1 hyperintensity and calcifications on the periphery were more consistent with a cystic adenoma or craniopharyngioma. With all the variability seen on MRI, specific radiologic criteria have not been established.
Clinical Presentation
The clinical diagnosis of XG is also challenging. As described by Paulus et al, XGs are generally present in the second and third decade of life. 1 XGs of the sella tend to be smaller than adamantinomatous craniopharyngiomas, yet can show intrasellar extension. In contrast, adamantinomatous craniopharyngiomas have more retrosellar involvement. Marked endocrinological deficits are a common presentation in patients with sellar XGs, specifically anterior pituitary insufficiency. 1 The patients with XGs experience a longer duration of symptoms with a greater degree of pituitary hormone deficiency, but less frequently they experience visual disturbance or hydrocephalus. 1 In our case, the patient had the same age distribution as it was initially described by Paulus et al; however, the lesion was large and his symptoms were due to compression of the optic apparatus with progressive visual loss. 1 Similar to our case, Rahmani et al reported a series of patients with XG where the most common presenting symptoms were vision loss and headache. 6
Endocrine Function
The most common endocrinological abnormality appears to panhypopituitarism as shown in the literature review. Hyperprolactinemia was noted in only four cases. Of the five reported cases of pituitary adenoma with xanthogranulomatous features, none had a clinical presentation of an apoplectic event such as sudden intense headache, rapid deterioration of vision or general condition, and none of the specimens had any hemorrhagic soft tissue that could be consistent with apoplexy. 11 In our case, the patient had a progressive deterioration of his vision and headaches. During the operation, there was note of a cystic component with old liquefied blood that could have represented an internal hemorrhagic episode of the tumor. There is a possibility of the lesion having an apoplectic event, and with this, the prolactin levels decreased.
Clinical Case
Sellar XG is a benign pathological entity that likely has behavior parallel to the underlying condition, that is, RCC, adamantinomatous craniopharyngioma, or pituitary adenoma. Even in examples with no underlying identifiable cause, XG appears to have a good prognosis and no adjuvant therapy is indicated. Surgical intervention is indicated when the lesion is causing neurological deficits due to compression of the optic apparatus resulting in visual field deficits. Given the benign nature of sellar XGs, the goal of surgery is maximal safe resection, taking into consideration that the tumor capsule can be strongly adherent to surrounding structures. 21 When the tumor is solid and has the appearance of a classical adenoma, a straightforward transsphenoidal surgery is the optimum approach. However, these tumors can have atypical appearance as in our case report.
The choice of an endoscopic transsphenoidal approach rather than a transtubercular transplanum approach was made after thorough consideration of the past history of hyperprolactinemia and wide expansion of the sella; features that are not seen in craniopharyngioma. Old liquefied blood was found filling the tumor cavity during surgery. It is possible that xanthogranulomatous degeneration happened secondary to hemorrhage in a preexisting prolactinoma.
Conclusion
Prolactinomas with secondary xanthogranulomatous change represent a rare cause of XG of the sella. With no radiological or clinical signs specific for XG of the sellar region, preoperative diagnosis can be challenging, if not impossible. This is the first case report of XG in a preexisting true prolactinoma.
Notes
This article has not been presented at a conference.
No clinical trial registration number required.
References
- 1.Paulus W, Honegger J, Keyvani K, Fahlbusch R. Xanthogranuloma of the sellar region: a clinicopathological entity different from adamantinomatous craniopharyngioma. Acta Neuropathol. 1999;97(04):377–382. doi: 10.1007/s004010051001. [DOI] [PubMed] [Google Scholar]
- 2.Kleinschmidt-DeMasters B K, Lillehei K O, Hankinson T C. Review of xanthomatous lesions of the sella. Brain Pathol. 2017;27(03):377–395. doi: 10.1111/bpa.12498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ben Nsir A, Thai Q A, Chaieb L, Jemel H.Calcified suprasellar xanthogranuloma presenting with primary amenorrhea in a 17-year-old girl: case report and literature review World Neurosurg 201584038.66E13–866..e14 [DOI] [PubMed] [Google Scholar]
- 4.Gurcay A G, Gurcan O, Kazanci A et al. Xanthogranuloma of the sellar region. Neurol India. 2016;64(05):1075–1079. doi: 10.4103/0028-3886.190238. [DOI] [PubMed] [Google Scholar]
- 5.Stepan K O, Sharma A, Chicoine M R, Uppaluri R, Dahiya S. Juvenile xanthogranuloma of supra-sellar region: a rare presentation. Clin Neuropathol. 2015;34(06):368–370. doi: 10.5414/NP300854. [DOI] [PubMed] [Google Scholar]
- 6.Rahmani R, Sukumaran M, Donaldson A M, Akselrod O, Lavi E, Schwartz T H. Parasellar xanthogranulomas. J Neurosurg. 2015;122(04):812–817. doi: 10.3171/2014.12.JNS14542. [DOI] [PubMed] [Google Scholar]
- 7.Nishiuchi T, Murao K, Imachi H et al. Xanthogranuloma of the intrasellar region presenting in pituitary dysfunction: a case report. J Med Case Reports. 2012;6:119. doi: 10.1186/1752-1947-6-119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Agarwal A, Agarwal K, Lee H K. Xanthogranuloma of the sellar region. A case report. Neuroradiol J. 2012;25(02):181–184. doi: 10.1177/197140091202500204. [DOI] [PubMed] [Google Scholar]
- 9.Kamoshima Y, Sawamura Y, Motegi H, Kubota K, Houkin K. Xanthogranuloma of the sellar region of children: series of five cases and literature review. Neurol Med Chir (Tokyo) 2011;51(10):689–693. doi: 10.2176/nmc.51.689. [DOI] [PubMed] [Google Scholar]
- 10.Miyajima Y, Oka H, Utsuki S, Fujii K. Rathke's cleft cyst with xanthogranulomatous change--case report. Neurol Med Chir (Tokyo) 2011;51(10):740–742. doi: 10.2176/nmc.51.740. [DOI] [PubMed] [Google Scholar]
- 11.Nishioka H, Shibuya M, Ohtsuka K, Ikeda Y, Haraoka J. Endocrinological and MRI features of pituitary adenomas with marked xanthogranulomatous reaction. Neuroradiology. 2010;52(11):997–1002. doi: 10.1007/s00234-010-0675-8. [DOI] [PubMed] [Google Scholar]
- 12.Sulentić P, Cupić H, Cerina V, Vrkljan M. Xanthogranuloma of the sellar region in a patient with sarcoidosis. Acta Clin Croat. 2010;49(01):61–65. [PubMed] [Google Scholar]
- 13.Arai A, Nishihara M, Sasayama T et al. Xanthogranuloma of the sellar region--case report. Neurol Med Chir (Tokyo) 2010;50(06):488–491. doi: 10.2176/nmc.50.488. [DOI] [PubMed] [Google Scholar]
- 14.Sugata S, Hirano H, Yatsushiro K, Yunoue S, Nakamura K, Arita K. Xanthogranuloma in the suprasellar region. Neurol Med Chir (Tokyo) 2009;49(03):124–127. doi: 10.2176/nmc.49.124. [DOI] [PubMed] [Google Scholar]
- 15.Liu Z H, Tzaan W C, Wu Y Y, Chen H C. Sellar xanthogranuloma manifesting as obstructive hydrocephalus. J Clin Neurosci. 2008;15(08):929–933. doi: 10.1016/j.jocn.2007.05.028. [DOI] [PubMed] [Google Scholar]
- 16.Tajima T, Sawamura Y, Ishizu K, Tsubaki J. Two children with xanthogranuloma of the sellar region. Clin Pediatr Endocrinol. 2006;15(03):85–91. doi: 10.1297/cpe.15.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jung C S, Schänzer A, Hattingen E, Plate K H, Seifert V. Xanthogranuloma of the sellar region. Acta Neurochir (Wien) 2006;148(04):473–477. doi: 10.1007/s00701-005-0700-6. [DOI] [PubMed] [Google Scholar]
- 18.Burt M G, Morey A L, Turner J J, Pell M, Sheehy J P, Ho K K. Xanthomatous pituitary lesions: a report of two cases and review of the literature. Pituitary. 2003;6(03):161–168. doi: 10.1023/b:pitu.0000011177.43408.56. [DOI] [PubMed] [Google Scholar]
- 19.Yonezawa K, Shirataki K, Sakagami Y, Kohmura E. Panhypopituitarism induced by cholesterol granuloma in the sellar region--case report. Neurol Med Chir (Tokyo) 2003;43(05):259–262. doi: 10.2176/nmc.43.259. [DOI] [PubMed] [Google Scholar]
- 20.Osborn A.Nonastrocytic glial neoplasms. In: Osborn A, ed. Osborn' Brain Imaging, Pathology and Anatomy. Manitoba Canada: Amirsys Publishing Inc;2013:510 [Google Scholar]
- 21.Yang B, Yang C, Fang J et al. Clinicoradiologic features and surgical outcomes of sellar xanthogranulomas: A single-center 10-year experience. World Neurosurg. 2017;99:439–447. doi: 10.1016/j.wneu.2016.12.017. [DOI] [PubMed] [Google Scholar]