

Abstract
Introduction:
Placebo and nocebo effects represent one of the most fascinating topics in the health care field.
Objectives:
the aims of this discussion paper were (1) to briefly introduce the placebo and nocebo effects, (2) to elucidate the contextual factors able to trigger placebo and nocebo effects in the nursing field, and (3) to debate the impact of contextual factors on nursing education, practice, organisation, and research.
Methods:
a narrative review was conducted based on the available evidence.
Results:
Placebo responses (from Latin “I shall please”) are a beneficial outcome(s) triggered by a positive context. The opposite are the nocebo effects (from Latin “I shall harm”), which indicates an undesirable outcome(s) caused by a negative context. Both are complex and distinct psychoneurobiological phenomena in which behavioural and neurophysiological changes arise subsequent to an interaction between the patient and the health care context.
Conclusion:
Placebo and nocebo concepts have been recently introduced in the nursing discipline, generating a wide debate on ethical issues; however, the impact on nursing education, clinical practice, nursing administration, and research regarding contextual factors triggering nocebo and placebo effects has not been debated to date.
Keywords: Contextual factors, Placebo, Nocebo, Nursing outcomes, Nursing research, Nursing education, Nursing administration
1. Introduction
Placebo and nocebo effects represent one of the most fascinating topics in the health care field. Historically, placebo has been conceptualized as an inert treatment given in clinical randomized trials to compare the efficacy of an active treatment arm vs the placebo arm.32,95 The modern neurobiological theories differentiate between placebo and nocebo responses (eg, clinical trials) and placebo and nocebo effects as the neurobiological phenomena independent from biases, regression to the mean, natural history, and co-interventions.32,95 Overall in this discussion paper, we define placebo and nocebo effects as the result of patient's interaction with the health care context. Namely, the term “placebo effects” (from Latin placēbō, “I shall please”) have been adopted to describe a beneficial outcome(s) produced by positive contexts,9 whereas nocebo effects (from Latin nocēbō, “I shall harm”) have been defined as undesirable outcome(s) produced by negative contexts surrounding the patient and the treatment delivery.15
In medical literature, the concept of placebo effects has been debated since 1941,69 specifically in the field of medication administration, and was introduced as a Medical Subject Heading (MeSH) in 1990. On the other hand, the concept of nocebo effects was introduced by Kennedy in 1961 and recognised as a MeSH only in 2014. In the nursing discipline, while placebo concept was introduced in 1966,122 nocebo was formally introduced in the literature only 8 years ago.103 Moreover, both concepts have given rise to a wide debate mainly regarding ethical issues,5,56 despite them being proposed as promising clinical tools useful in modulating nursing outcomes.85,112
In recent years, the investigation of placebo and nocebo effects have been included the evaluation of the context supporting the patient in achieving (or not) the desired health outcomes.33 As a consequence, the misleading interpretation of placebo as inert treatment given to comfort or please the patient has been overcome; conversely, the modern conceptualization of the placebo and nocebo effects as the psychosocial context that accompanies any health care intervention, be it active or sham, has been embraced.52,100,121
The context is composed by the “whole atmosphere around the therapy”6 created by the health care team, technologies and settings. Recently, specific contextual factors have been proposed in the literature as potential triggers for placebo and nocebo effects.100,114 As suggested by many authors,7,16,36,41,86 these factors are embodied at different levels: (1) the provider and the patient features (eg, expectations), (2) the patient–provider relationship (eg, empathy), (3) the intervention (eg, the colour and shape of a medication), and (4) the health care setting (eg, the home or hospital room layout). These factors constitute the therapeutic ritual and healing symbols surrounding the encounter able to trigger placebo and nocebo effects, impacting the patient's physiology and psychology and, ultimately, influencing the expected clinical outcome.10,11
Considering that a boost of placebo and prevention of nocebo would be valuable in nursing practice, this discussion paper is aimed at (1) briefly introducing the placebo and nocebo effects, (2) elucidating the contextual factors capable of triggering placebo and nocebo effects in the nursing field, and (3) debating implications at the nursing educational, practical, organisational, and research levels.
2. Placebo and nocebo effects
Placebo and nocebo effects have been used as a model to investigate the human body systems, analysing their interaction with different systems, mechanisms, diseases, and therapeutic interventions.8 Specifically, placebo and nocebo effects have been studied in psychiatric conditions, cardiovascular, respiratory, gastrointestinal, motor, immune, and endocrine systems.47,48,101 However, pain represents the most investigated symptom of placebo and nocebo effects.15,34 Determinants explaining placebo and nocebo effects have been identified at the individual, psychological, and neurobiological levels.
2.1. Individual and psychological determinants
At the individual level, early stages of research aimed at evaluating the role of some genetic variants established as relevant in placebo and nocebo effects, but the available findings are not conclusive.61 Preliminary evidence focusing on goal-seeking behaviours, self-efficacy/esteem, the locus of control, optimism, fun seeking, sensation seeking, neuroticism, trust, beliefs, and body consciousness suggested that these can all act as trait predictors of placebo effects.66 On the other hand, anxiety, panic disorder, or pessimism can exacerbate nocebo effects.112 However, more evidence is available regarding the role of psychological determinants such as expectations and learning.31,38
An expectation represents a conscious deliberately reportable element through which the patient expects a beneficial or harmful outcome based on the evaluation of contextual factors such as verbal instructions (eg, communication associated with interventions provided by the nurse) or past experiences (eg, previous interaction with a nurse).38 Expectations are able to modify experiences. Anxiety can be further influenced by emotional and cognitive factors, such as self-efficacy, self-reinforcing feedback, memory, attention, and motivation.8,48,97
Learning encompasses associative, social, and reinforced expectation mechanisms.31 Associative learning emerges when a conditioned neutral stimulus such as a contextual factor (eg, the colour of a medication) is associated with an unconditioned stimulus (eg, the active molecules contained in the medication), and it is responsible for altering the symptom even when the active principle is not administered.37 Social learning occurs, for example, when a patient on a specific treatment learns to change symptoms by appreciating the effects reported by other patients.31 Moreover, in accordance with Colloca,31 expectations and learning represent an interactive phenomenon, given that learning can increase expectations or develop new ones.
2.2. Neurobiological determinants
From a neurobiological point of view, placebo and nocebo effects have been documented to be accounted for by a specific neurochemistry and neural network.101 Placebo and nocebo effects interact with the brain modulatory systems at a neurochemical level, through the release of specific neurotransmitters.101 For instance, considering pain outcome as a model, the endogenous opioids, dopamine, cannabinoids, oxytocin, and vasopressin are involved in the reduction of pain (eg, placebo analgesia) whenever the patient interacts with positive contextual factors.9,25 Conversely, cholecystokinin, dopamine, opioid deactivation, and cyclooxygenase-prostaglandins' activation are involved in the amplification of pain (eg, nocebo hyperalgesia) during health care patient encounter surrounded by negative contextual factors.15,25
Furthermore, recent advances in neuroimaging techniques, such as functional magnetic resonance imaging and positron emission tomography, suggest an involvement of specific neural correlates during placebo and nocebo effects of pain.102 The positive and negative use of contextual factors are capable of activating or inactivating the 4 key brain regions commonly associated with the descending pain processing pathway: the dorsolateral prefrontal cortex, the rostral anterior cingulate cortex, the periaqueductal gray matter, and the spinal dorsal horn.25,26 Nevertheless, other classical pain-related areas have been reported to change in their activity during placebo or nocebo effects such as the thalamus, insula, somatosensory cortex, and midcingulate regions.52,121
2.3. The trigger role of contextual factors
Contextual factors have been documented as triggering placebo and nocebo effects.100,114 Specifically, all clinical interventions have been defined as composed by 2 inseparable elements: (1) the first is the intervention itself (eg, the medication and the treatments) mainly based on biological elements, whereas the (2) second is based on the context.9 Context is not an empty dimension, but it represents a powerful healing space enriched by emotional, cognitive, affective, social, and relational factors. It is, furthermore, capable of interacting with the patient's clinical condition.121 The contextual factors convey a hidden meaning, detected and actively analysed by the patient, which is essential for the perception of care and the interpretation of the therapeutic intervention.37 When these factors are analysed from the patient's perspective, they are translated into a complex cascade of psychoneuroimmunoendocrine events capable of generating placebo/nocebo effects and eliciting expectations, memories, and emotions that, in turn, can influence the patient's health-related outcome as presented in Figure 1.37,121
Figure 1.
Contextual factors as triggers of placebo and nocebo effects. Adapted from Blasini et al. (2017).
Many studies25,26,71,84,121 have defined the context and related factors within placebo research, and recently, some have attempted to disentangle each factor,41 so that this knowledge can be translated in many areas of health science. For example, Testa and Rossettini114 have attempted to identify each factor applying the related knowledge to the field of physiotherapy and musculoskeletal pain.100 These contextual factors, capable of influencing clinical outcomes, have been identified as professional reputation, appearance, beliefs, and behaviours of health care providers; expectations, preferences, previous experience, clinical conditions, sex, and age of the patient; verbal and nonverbal elements of communication characterising the patient–health care provider relationship; the environment, architecture, and internal design of the health care setting; and the specific aspects of treatment such as a clear diagnosis, an overt therapy, observational learning and patient-centred approach, a global process of care and the therapeutic touch.
3. Subjective nursing outcomes can be modulated by contextual factors
Nursing outcomes are defined as those changes subjectively or objectively reported by patients or by their caregivers and/or family members as a result of the nursing care received.58 Safety and efficacy outcomes have been categorised, and specific indicators have been established. Among safety outcomes, falls, pressure sores, hospital acquired infections (eg, pneumonia and surgical site infections), and medication errors leading to death have been described.58 Among efficacy outcomes, independence in activities of daily living as well as patient or family self-management competence, coping, comfort, and satisfaction with nursing care have been established and included in several national and international quality indicators and research projects.58
With the final purpose of preventing safety outcomes and of achieving efficacy outcomes, clinical nurses develop a plan of care after identifying actual or at-risk problems. On the basis of patient and caregiver preferences, values, and resources, clinical nurses decide the nursing interventions required. These interventions should be based on the available evidence and can consist of simple interventions (patient mobilisation), bundle interventions (such as the prevention of care-associated infections), or complex interventions (such as those performed to improve functional independence in nursing homes). All these interventions can be performed by the same nurse (as in the case of a family nurse or primary nurse) or by a team (as in the case of hospital-based nursing care).
Although evidence emerging from research tries to predict the likelihood of preventing a certain safety outcome or achieving the effective outcome after a specific intervention, it is always necessary to take into account the “uncertainty principle”.33 Paraphrasing Colloca and Benedetti,33 it is challenging to measure with a significant degree of accuracy the contribution of each intervention (eg, the effect of an educational session) on outcomes as the intervention itself is influenced by contextual factors. Effects determined by interventions have been conceptualized as the sum of the contextual factors effect plus the active intervention effect plus the interaction of the contextual factors and active intervention effects.119 Thus, the contextual factors surrounding the patient have the power to interact with the intervention, modulating its effect and outcomes,25,26,121 mainly influencing the experience and perceptions of illness symptoms, instead of changing the pathophysiology of disease.83
Positive contextual factors can increase the effectiveness of the intervention, whereas negative contextual factors can decrease it.47 As a consequence, contextual factors embody an unavoidable component of nursing care responsible of influencing the overall patients' outcomes,83 such as (1) the positive patient's experience with care (eg, satisfaction, involvement, empowerment, adherence, and compliance to treatments, motivation, willingness, hope, safety, and the perception of the quality of care); and (2) the symptoms experienced (eg, pain, discomfort, anxiety, nausea, stress, fatigue, social, psychological, physical, and spiritual well-being).
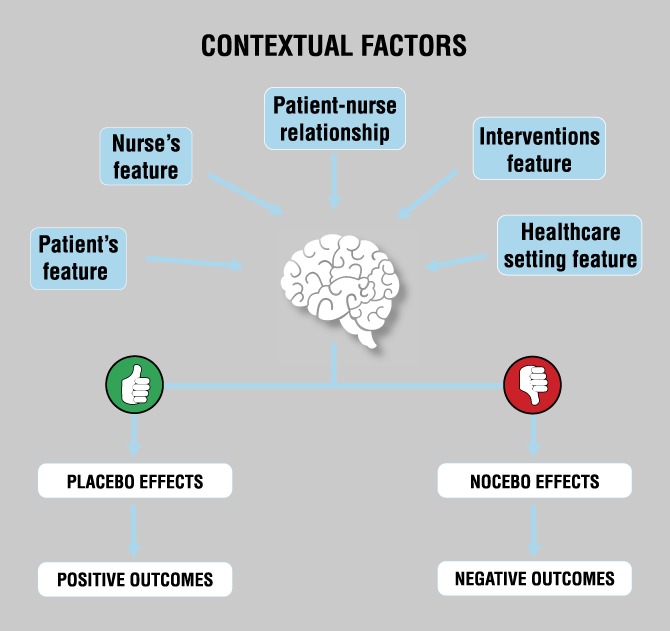
To our knowledge, no attempt has been made to develop an evidence-based clinical toolkit40 aimed at summarising contextual factors relevant in placebo and nocebo effects in the nursing disciplines. Thus, the theoretical frameworks about the role of context proposed by different authors7,16,25,26,36,41,71,84,86,100,114,121 for the different areas of health science have been considered and translated for the nursing field. A thorough analysis of the contextual factors led to categorize them into: (1) nurse's and patient's features, (2) the patient–nurse relationship, (3) interventional features, and (4) the characteristics of the health care setting, as reported in Figure 2.
Figure 2.

Contextual factors as modulators of the nursing outcomes. Adapted from Testa and Rossettini (2016).
Table 1 reports a summary of contextual factors triggering placebo and nocebo effects that clinical nurses should consider in their daily care.
Table 1.
Contextual factors increasing placebo effects and minimizing nocebo effects: a summary for clinical practice (adapted from Testa and Rossettini 2016).

3.1. Nurse's features
Nurses embody a specific “effect” because they convey information to the patient through appearance and behaviour that communicate the essence of nursing care. At a first glance, a nurse's uniform is capable of influencing the perception of nursing professionalism and competence by patients.64,73,96,115
Professional qualifications, expertise, competences, and technical skills of nurses can influence patient satisfaction, treatment adherence, and compliance with care.14,43,68,82,125,130 Moreover, personal qualities such as leadership, attitudes, and beliefs are components known to influence patient satisfaction and the overall experience of nursing care.120,128,129 Other personal qualities include honesty, candour, trustworthiness, empathy, compassion, confidentiality, and commitment to providing the best care. Authenticity, assertiveness, humility, and the ability to provide holistic care have also been associated with patient satisfaction and perception of quality with nursing care.99,117 Moreover, awareness of unvoiced needs by encouraging patients to share their concerns has also been documented as influencing outcomes. When caring for patients and caregivers, demonstrating compassion, tolerance, and respect, accepting patient preferences and decisions, and providing information regarding illness and health processes, all influence nursing outcomes.14,43,68,99,117,125
On the other hand, failure to anticipate or recognise patient needs, depersonalising the patient by referring to him or her using the medical diagnosis or bed number, neglecting care responsibilities, in which patients feel abandoned, vulnerable, ashamed, ignored, or insecure can negatively affect nursing outcomes by increasing the occurrence of safety issues.43,55,62,99
3.2. Patient's features
The patient's previous experiences, preferences, and expectations are significant elements influencing both placebo and nocebo effects.
The expectations regarding an intervention can determine the patient's involvement, satisfaction, and experience as well as the outcomes regarding pain control.91,126,131 Positive expectations, desires, and hopes may increase nursing outcomes,91,126 while, as reported recently by Woo,131 negative expectations of discomfort during wound dressing changes have been associated with an increased occurrence of pain (also known as nocebo hyperalgesia), wound exudate, and occurrence of necrotic tissues.
Moreover, previous experience of care and preferences can also influence outcomes.106 According to a recent systematic review, the likelihood of nocebo effects is increased when previous negative knowledge or expectations exist. In addition, pre-existing psychological traits (eg, anxiety) may exacerbate the nocebo effect.112
Furthermore, the sociodemographic background of patients such as age and sex has also been documented as contributing to nursing outcome. Elderly patients have been reported to be more satisfied with nursing care; moreover, men report a higher level of satisfaction with nursing care compared with women, similarly to patients with lower education levels.70 On the other hand, the nocebo effects have been reported more often among women.112
3.3. The patient–nurse relationship
A patient-centred communication based on verbal and nonverbal strategies positively influences the clinical encounter between the nurse and the patient, improving satisfaction, empowerment, adherence to care treatments, trust, pain catastrophizing, stress, fear, anxiety, and symptom resolution.29,53,78,98 Differently, as documented recently by Doyle et al.,44 poor patient outcomes occur when the nurse's behaviour is callous and lacks empathy.
Verbal communication is emphasised by open-ended and affective questions, the ability to clarify, summarise, and negotiate as well to listen actively; moreover, nonverbal communication is also considered a key factor influencing nursing outcomes such as those techniques aimed at increasing the understanding of the patient's concerns, eg, communicating with empathy, paraphrasing, and following-up cues.80,90,103 For example, verbal communication used by nurses during medication administration has been documented to influence the patient's satisfaction and symptoms: pain is influenced positively by verbal suggestion of amelioration and negatively by verbal sentences of aggravation.2,88,90,109,118
In addition, the nurse's ability to interpret nonverbal body language expressions of emotion and/or distress may affect patient satisfaction.80,90 Tailoring nonverbal communication to patients' sensory deficits is crucial: deaf patients report an increased sense of vulnerability, a risk of delayed recognition of their symptoms and needs, and in receiving appropriate interventions.108
3.4. Intervention features
Several elements of nursing interventions can affect patient outcome(s). Showing or telling a patient that an intervention is being undertaken can stimulate placebo effects.13 Moreover, presenting information about side effects of treatment in form of probability instead of a mere list, as well as balancing positive and negative information can all reduce the nocebo effects.124
Creating a therapeutic context in which patients can share their experiences with other patients or can watch videos where other patients report their positive experience with the same intervention may increase the likelihood of positive effects of the treatment.102 Similarly, reducing exposure to patients experiencing side effects of the medication can reduce nocebo effects.72,104,124 In addition, in the field of educational interventions, offering in-group sessions by nurses instead of individual interventions can trigger some effects105: according to the literature available, patients who receive education sessions in a group can increase motivation, willingness, compliance, and hope, and also positive interactions with other participants.89 Educational interventions have also been documented to improve pain, anxiety, stress, satisfaction with nursing care, and to reduce side effects of medications.45,50,54,60,134
This patient-centred approach is also able to modulate nursing care effects. Tailoring nursing interventions by considering the patient's preferences and needs, empowering them in self-care management and ensuring continuity of care, as well as offering visits by the same nurse, can all positively influence outcomes such as patient's satisfaction, compliance, anxiety, depression, quality of life, and experience with care.4,14,23,39,43,51,68,94,99,116,125 On the other hand, higher workloads, long waiting times, the use of medical and sophisticated language, or the use of nurse-centred approaches with a lack of patient understanding and proximity can hamper patient satisfaction.4,23,43,55,68,99 In addition, the above-mentioned factors can positively influence the agreement between patients and nurses regarding the care plan, thus increasing its quality.93
The comfort touch adopted by nurses has also been recognised as a contextual factor. Touch represents the basis of social interaction conveying information about the emotional and mental state of individuals involved in the relationship.75 In nursing care, touching has been documented as a useful intervention that alleviates pain, anxiety, depression, sleep disturbances, nausea, and fatigue, thus increasing quality of life.3,18,19,30,46,57,92,113,132 While touching patients, nurses communicate empathy, compassion, affection, concern, and security, thus facilitating the achievement of the expected outcomes.75
3.5. Health care setting features
Sensory cues, structural aspects, decorations, and ornaments are the most important elements of the healing environment that should be considered when planning and designing the care settings.22,28,125
In general, clear indication of health care settings can improve health care accessibility.59 Specifically, environments with natural lighting (eg, full-spectrum lighting), low noise levels (eg, adoption of sound-absorbing ceilings or earplugs/earmuffs), and relaxing and soft sounds (eg, music, bird songs, rain showers, and ocean waves) have been documented as greatly appreciated by patients and capable to improve outcomes of anxiety, pain, delirium, satisfaction, and emotional well-being.1,20,21,42,76,79,107,110,133 Also the adoption of pleasant aromas and an adequate temperature and microclimate (eg, filters, airflow control, and ventilation systems) all create a positive therapeutic setting.42
Moreover, environments that integrate windows and skylights, with comfortable and private settings (eg, single-bed or private patient rooms) have also been documented as positive elements by patients.27 Nature artwork, such as flowers or green vegetation in nursing homes, can have a calming effect, thus improving pain, delirium, sleep, and satisfaction.20,27,42,79 The presence of healing gardens close to wards (eg, plants and water) and social spaces (eg, lounge, day rooms, and waiting rooms) have been documented as increasing connections between patients and their caregivers, thus reducing stress and pain and promoting well-being. Colour frames based on calming tones also mitigate patient involvement in nursing care; however, the meaning of colour is culturally based and can differ between patients.42
Finally, combining positive distractors has been documented as modulating pain, stress, anxiety, and safety, promoting social, psychological, physical, and spiritual well-being.74 However, uncomfortable, frightening, oppressive, claustrophobic, and dirty rooms have been associated with patient dissatisfaction and negative outcomes.24,67
4. Implications for the nursing discipline
Although the placebo effects have a longer history in the nursing literature,85,122 the recent introduction of the nocebo effects103,112 suggests that these concepts require complete consideration at different levels of the nursing discipline, eg, from education to clinical practice, nursing administration, and research. Because of the relationship with the patient's clinical outcome, it is necessary to identify future directions for inquiry and application starting with a critical evaluation of current nursing practices.
4.1. Nursing education
Although the concept of caring as learnt during nursing education embodies several of the above-mentioned factors,123 these are not always clearly introduced in nursing programs.81 Specifically, if contextual factors are not taught during theoretical lessons and experienced during clinical rotation, there is a risk to consider them as irrelevant by students and faculty members, thus reducing their aware clinical application.35 Thus, the nursing programme should consider the contextual factors as core components of the curricula.
Students at different levels of education (from bachelor's and master's nursing degrees) with different degrees of nursing competence should be coached to analyse and consider the relevance of contextual factors in influencing nursing outcomes.16 They should be trained to progressively increase their awareness of their own attitudes and traits. In addition, they should learn to develop complex competences in assessing patient and caregiver needs and preferences, also taking into consideration their sociocultural context (eg, culture and ethnicity).
Students should have the opportunity to reflect on how their personal qualities evolve based on clinical experiences.49 On the other hand, supervisors at both the faculty and clinical levels should consider student aptitudes and qualities (such as honesty) as specific traits on which students need to receive feedback with the aim of promoting their personal and professional growth. Students should also have the opportunity to reflect with experienced nurses on unexpected negative patient outcomes, by identifying the relevant contribution of some contextual factors in addition to other well-known mechanisms such as nurse-to-patient ratio or physiopathology mechanisms.
Moreover, the clinical context in which students undertake their rotations should promote their learning processes: contextual elements triggering placebo and nocebo effects can also have a role in student learning outcomes, preventing or facilitating their achievements, an area that has not attracted the attention of researchers to date.
4.2. Nursing clinical practice
The manner in which clinical nurses consider the contextual factors triggering nocebo/placebo effects in their daily practice has not been extensively documented.85 In those clinical settings in which nurses work in groups as in hospitals, shift after shift, the variability of the adoption regarded contextual factors may offset the positive effects obtained or reinforce negative ones. Patients switching from one nursing team to another at the end of shifts, or transiting from one context to another (the medical unit to rehabilitation unit), can experience uncertainty or confusion even if nursing interventions are similar. These effects can be different due to different contextual factors.
Moreover, experienced clinical nurses may identify other factors not clearly included in the available frameworks87 by their clinical wisdom and expertise, as well as their close relationship with patients, and may develop an in-depth knowledge of other factors that may modulate the relationship between nursing care and patient outcomes. Therefore, it is ideal to ensure continuity in care by providing the same nurse (eg, primary nursing model of care delivery). When this is not possible, it is advisable for care plans to contain documentation regarding relevant contextual factors and their clinical effects, aiming at ensuring consistency across shifts and contexts to increase the likelihood of a positive nursing outcome.
Clinical nurses should also be supported in developing and maintaining their competences by carrying on educational strategies not only concerning interventions but also the context in which they are implemented. Moreover, with regard to the ethical implications of the contextual factors, clinical nurses have been documented to consider placebo effects as real, with therapeutic benefits, and acceptable within the ethical borders in daily practice.63 Therefore, the elicitation of placebo and the avoidance of nocebo effects by contextual factors have been considered ethical.100,114 In fact, the conscious use of contextual factors symbolises a useful chance to improve evidence-based nursing care without threatening the principle of nonmaleficence, the patient's autonomy, and informed consent. Therefore, this approach is markedly different from that replacing the required treatment with a potentially ineffective treatment.17,47,48
4.3. Nursing care management
The clinical settings have received increased attention in recent years as mediators of the quality of nursing care.111,127 Examples may be detected in recent studies where the organisational support perceived by clinical nurses may modulate patient outcomes by increasing or decreasing their occurrence.65,77 Differently, in light of placebo/nocebo effects, contextual factors may directly influence patients and promote (or hamper) the achievement of expected outcomes. Therefore, the role of the environment should be considered not only as affecting the performance of the nursing workforce, but also as relating to patient outcomes with direct effects.
Nurse leaders should be prepared to continually assess, design, and promote interventions to improve the quality of the environment while cooperating with other leaders both at the hospital, at the community and at the residential levels. There is also a need to develop and validate instruments capable of measuring the quality of factors implied in placebo/nocebo effects, aiming at monitoring the amelioration of the contextual factors over time.
Any form of nursing care standardisation, addressing patients' needs without considering preferences, expectations, and unique needs, should be detected early and avoided. Specifically, some models of nursing care delivery (eg, functional models) should be immediately replaced with person-centred models of care delivery where evidence-based approaches, capable of identifying the best interventions within those documented in the literature, are implemented in an appropriate environment, capable of maximising the effects of the intervention delivered.
4.4. Nursing research
Although placebo and nocebo effects are well documented, there has been minimal research in the nursing field.85,112
Designing and implementing a trial for placebo and nocebo investigation represents a challenge, and several confounding factors should be controlled.119 The history of disease, the influence of uncontrolled biases, unidentified co-interventions, and adverse side effects can all modulate nursing care outcomes.12 Research on placebo and nocebo should adopt placebo ethically as an enhancing strategy associated with the best evidence-based available interventions to prevent nocebo and improve nursing outcomes.17,48 Moreover, research on placebo and nocebo effects should be based on contextual factors effect.100,114 Limiting the influence of the contextual factors around the intervention can help to identify the specific effect of the intervention itself. On the other hand, boosting the context around an active intervention can disclose the role of contextual factors in modulating clinical outcomes.13
Different lines of research can be designed and promoted in specialist (eg, critical care nursing, oncology care, mental health, or chronic care) or in general areas, at national and international levels, also considering the cultural differences that may affect placebo and nocebo effects. First, there is a need to explore the knowledge and expertise on placebo and nocebo effects both among undergraduates, registered and advanced nurses, aiming at assessing their awareness in the field and promoting improvements to increase the latter. There is also a need to discover the effect of single and/or combined contextual factors affecting nursing care outcomes, possibly through incremental study designs to weigh the effect of each component. Finally, exploring patient perceptions regarding the contextual elements capable of positively or negatively influencing expected nursing outcomes, as well as researching psychological and genetic traits of placebo and nocebo responders given the documented variability across patients, is recommended.114
5. Conclusions
To our best knowledge, this is one of the first discussion paper deliberately linking the conceptualization of contextual factors as triggers of placebo and nocebo effects to the nursing discipline, practice, managements, education, and research. The ultimate goal is to raise awareness about the potential effects of contextual factors, placebo and nocebo effects on clinical outcomes managed by nurses.
Contextual factors can trigger positively or negatively the achievement of nursing outcomes. Besides appropriate evidence-based interventions, nurse educators, clinicians, leaders, and researchers should pay further specific attention to contextual factors to develop and to unveil their mechanisms of action by considering their implementation in daily practice. The theoretical framework developed for nurses can be easily generalized to pain medicine in general.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements
The authors thank Paola Di Giulio for her comments to the early version of this manuscript, which has provided insights. The authors received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
References
- [1].Aalbers S, Fusar-Poli L, Freeman RE, Spreen M, Ket JC, Vink AC, Maratos A, Crawford M, Chen XJ, Gold C. Music therapy for depression. Cochrane Database Syst Rev 2017;11:CD004517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Alaloul F, Williams K, Myers J, Jones KD, Sullivan K, Logsdon MC. Contextual factors impacting a pain management intervention. J Nurs Scholarsh 2017;49:504–12. [DOI] [PubMed] [Google Scholar]
- [3].Anderson JG, Taylor AG. Effects of healing touch in clinical practice: a systematic review of randomized clinical trials. J Holist Nurs 2011;29:221–8. [DOI] [PubMed] [Google Scholar]
- [4].Angel S, Frederiksen KN. Challenges in achieving patient participation: a review of how patient participation is addressed in empirical studies. Int J Nurs Stud 2015;52:1525–38. [DOI] [PubMed] [Google Scholar]
- [5].Arnstein P. Placebo: no relief for Ms. Mahoney's pain. Working with the patient, family, and staff to diminish pain. Am J Nurs 2006;106:54–7. [DOI] [PubMed] [Google Scholar]
- [6].Balint M. The doctor, his patient, and the illness. Lancet 1955;268:683–8. [DOI] [PubMed] [Google Scholar]
- [7].Benedetti F. How the doctor's words affect the patient's brain. Eval Health Prof 2002;25:369–86. [DOI] [PubMed] [Google Scholar]
- [8].Benedetti F. Mechanisms of placebo and placebo-related effects across diseases and treatments. Annu Rev Pharmacol Toxicol 2008;48:33–60. [DOI] [PubMed] [Google Scholar]
- [9].Benedetti F. Placebo and the new physiology of the doctor-patient relationship. Physiol Rev 2013;93:1207–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Benedetti F. Placebo-induced improvements: how therapeutic rituals affect the patient's brain. J Acupunct Meridian Stud 2012;5:97–103. [DOI] [PubMed] [Google Scholar]
- [11].Benedetti F, Amanzio M. The placebo response: how words and rituals change the patient's brain. Patient Educ Couns 2011;84:413–9. [DOI] [PubMed] [Google Scholar]
- [12].Benedetti F, Carlino E, Piedimonte A. Increasing uncertainty in CNS clinical trials: the role of placebo, nocebo, and Hawthorne effects. Lancet Neurol 2016;15:736–47. [DOI] [PubMed] [Google Scholar]
- [13].Benedetti F, Carlino E, Pollo A. Hidden administration of drugs. Clin Pharmacol Ther 2011;90:651–61. [DOI] [PubMed] [Google Scholar]
- [14].Bentley M, Stirling C, Robinson A, Minstrell M. The nurse practitioner-client therapeutic encounter: an integrative review of interaction in aged and primary care settings. J Adv Nurs 2016;72:1991–2002. [DOI] [PubMed] [Google Scholar]
- [15].Blasini M, Corsi N, Klinger R, Colloca L. Nocebo and pain: an overview of the psychoneurobiological mechanisms. Pain Rep 2017;2:e585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Blasini M, Peiris N, Wright T, Colloca L. The role of patient-practitioner relationships in placebo and nocebo phenomena. Int Rev Neurobiol 2018;139:211–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Blease C, Colloca L, Kaptchuk TJ. Are open-label placebos ethical? Informed consent and ethical equivocations. Bioethics 2016;30:407–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Boitor M, Gélinas C, Richard-Lalonde M, Thombs BD. The effect of massage on acute postoperative pain in critically and acutely Ill adults post-thoracic surgery: systematic review and meta-analysis of randomized controlled trials. Heart Lung 2017;46:339–46. [DOI] [PubMed] [Google Scholar]
- [19].Bouya S, Ahmadidarehsima S, Badakhsh M, Balouchi A, Koochakzai M. Effect of aromatherapy interventions on hemodialysis complications: a systematic review. Complement Ther Clin Pract 2018;32:130–38. [DOI] [PubMed] [Google Scholar]
- [20].Bradt J, Dileo C, Magill L, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev 2016;15:CD006911. [DOI] [PubMed] [Google Scholar]
- [21].Bradt J, Dileo C, Potvin N. Music for stress and anxiety reduction in coronary heart disease patients. Cochrane Database Syst Rev 2013:CD006577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Braun D, Barnhardt K. Critical thinking: optimal outcomes through end user involvement in the design of critical care areas. Crit Care Nurs Q 2014;37:33–40. [DOI] [PubMed] [Google Scholar]
- [23].Brereton L, Gardiner C, Gott M, Ingleton C, Barnes S, Carroll C. The hospital environment for end of life care of older adults and their families: an integrative review. J Adv Nurs 2012;68:981–93. [DOI] [PubMed] [Google Scholar]
- [24].Brown B, Rutherford P, Crawford P. The role of noise in clinical environments with particular reference to mental health care: a narrative review. Int J Nurs Stud 2015;52:1514–24. [DOI] [PubMed] [Google Scholar]
- [25].Carlino E, Benedetti F. Different contexts, different pains, different experiences. Neuroscience 2016;338:19–26. [DOI] [PubMed] [Google Scholar]
- [26].Carlino E, Frisaldi E, Benedetti F. Pain and the context. Nat Rev Rheumatol 2014;10:348–55. [DOI] [PubMed] [Google Scholar]
- [27].Cesario SK. Designing health care environments: Part I. Basic concepts, principles, and issues related to evidence-based design. J Contin Educ Nurs 2009;40:280–8. [DOI] [PubMed] [Google Scholar]
- [28].Cesario SK, Stichler J. Designing health care environments: Part II. Preparing nurses to be design team members. J Contin Educ Nurs 2009;40:324–28. [DOI] [PubMed] [Google Scholar]
- [29].Charlton CR, Dearing KS, Berry JA, Johnson MJ. Nurse practitioners' communication styles and their impact on patient outcomes: an integrated literature review. J Am Acad Nurse Pract 2008;20:382–8. [DOI] [PubMed] [Google Scholar]
- [30].Coakley AB, Barron AM. Energy therapies in oncology nursing. Semin Oncol Nurs 2012;28:55–63. [DOI] [PubMed] [Google Scholar]
- [31].Colloca L. Placebo, nocebo, and learning mechanisms. Handb Exp Pharmacol 2014;225:17–35. [DOI] [PubMed] [Google Scholar]
- [32].Colloca L. The placebo effect in pain therapies. Annu Rev Pharmacol Toxicol 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Colloca L, Benedetti F. Placebos and painkillers: is mind as real as matter? Nat Rev Neurosci 2005;6:545–52. [DOI] [PubMed] [Google Scholar]
- [34].Colloca L, Enck P, DeGrazia D. Relieving pain using dose-extending placebos. PAIN 2016;157:1590–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Colloca L, Jonas WB, Killen J, Miller FG, Shurtleff D. Reevaluating the placebo effect in medical practice. Z Psychol 2014;222:124–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Colloca L, Lopiano L, Lanotte M, Benedetti F. Overt versus covert treatment for pain, anxiety, and Parkinson's disease. Lancet Neurol 2004;3:679–84. [DOI] [PubMed] [Google Scholar]
- [37].Colloca L, Miller FG. How placebo responses are formed: a learning perspective. Philos Trans R Soc Lond B Biol Sci 2011;366:1859–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Colloca L, Miller FG. Role of expectations in health. Curr Opin Psychiatry 2011;24:149–55. [DOI] [PubMed] [Google Scholar]
- [39].Crawford CL, Boller J, Jadalla A, Cuenca E. An integrative review of pain resource nurse programs. Crit Care Nurs Q 2016;39:64–82. [DOI] [PubMed] [Google Scholar]
- [40].Darnall BD, Colloca L. Optimizing placebo and minimizing nocebo to reduce pain, catastrophizing, and opioid use: a review of the science and an evidence-informed clinical toolkit. Int Rev Neurobiol 2018;139:129–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet 2001;357:757–62. [DOI] [PubMed] [Google Scholar]
- [42].Dijkstra K, Pieterse M, Pruyn A. Physical environmental stimuli that turn healthcare facilities into healing environments through psychologically mediated effects: systematic review. J Adv Nurs 2006;56:166–81. [DOI] [PubMed] [Google Scholar]
- [43].Dinç L, Gastmans C. Trust in nurse-patient relationships: a literature review. Nurs Ethics 2013;20:501–16. [DOI] [PubMed] [Google Scholar]
- [44].Doyle K, Hungerford C, Cruickshank M. Reviewing Tribunal cases and nurse behaviour: putting empathy back into nurse education with Bloom's taxonomy. Nurse Educ Today 2014;34:1069–73. [DOI] [PubMed] [Google Scholar]
- [45].Drake G, de C Williams AC. Nursing education interventions for managing acute pain in hospital settings: a systematic review of clinical outcomes and teaching methods. Pain Manag Nurs 2017;18:3–15. [DOI] [PubMed] [Google Scholar]
- [46].Duong N, Davis H, Robinson PD, Oberoi S, Cataudella D, Culos-Reed SN, Gibson F, Götte M, Hinds P, Nijhof SL, Tomlinson D, van der Torre P, Ladas E, Cabral S, Dupuis LL, Sung L. Mind and body practices for fatigue reduction in patients with cancer and hematopoietic stem cell transplant recipients: a systematic review and meta-analysis. Crit Rev Oncol Hematol 2017;120:210–6. [DOI] [PubMed] [Google Scholar]
- [47].Enck P, Bingel U, Schedlowski M, Rief W. The placebo response in medicine: minimize, maximize or personalize? Nat Rev Drug Discov 2013;12:191–204. [DOI] [PubMed] [Google Scholar]
- [48].Finniss DG, Kaptchuk TJ, Miller F, Benedetti F. Biological, clinical, and ethical advances of placebo effects. Lancet 2010;375:686–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Froneman K, Du Plessis E, Koen MP. Effective educator-student relationships in nursing education to strengthen nursing students' resilience. Curationis 2016;39:1595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Garcia S. The effects of education on anxiety levels in patients receiving chemotherapy for the first time: an integrative review. Clin J Oncol Nurs 2014;18:516–21. [DOI] [PubMed] [Google Scholar]
- [51].Geerse OP, Stegmann ME, Kerstjens HAM, Hiltermann TJN, Bakitas M, Zimmermann C, Deal AM, Brandenbarg D, Berger MY, Berendsen AJ. Effects of shared decision making on distress and health care utilization among patients with lung cancer: a systematic review. J Pain Symptom Manage 2018;56:975–87. [DOI] [PubMed] [Google Scholar]
- [52].Geuter S, Koban L, Wager TD. The cognitive neuroscience of placebo effects: concepts, predictions, and physiology. Annu Rev Neurosci 2017;40:167–88. [DOI] [PubMed] [Google Scholar]
- [53].Gibson E, Sabo MT. Can pain catastrophizing be changed in surgical patients? A scoping review. Can J Surg 2018;61:311–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Glowacki D. Effective pain management and improvements in patients' outcomes and satisfaction. Crit Care Nurse 2015;35:33–41. [DOI] [PubMed] [Google Scholar]
- [55].Gordon J, Sheppard LA, Anaf S. The patient experience in the emergency department: a systematic synthesis of qualitative research. Int Emerg Nurs 2010;18:80–8. [DOI] [PubMed] [Google Scholar]
- [56].Grace PJ. The clinical use of placebos. Is it ethical? Not when it involves deceiving patients. Am J Nurs 2006;106:58–61. [DOI] [PubMed] [Google Scholar]
- [57].Greenlee H, Balneaves LG, Carlson LE, Cohen M, Deng G, Hershman D, Mumber M, Perlmutter J, Seely D, Sen A, Zick SM, Tripathy D; Society for Integrative Oncology. Clinical practice guidelines on the use of integrative therapies as supportive care in patients treated for breast cancer. J Natl Cancer Inst Monogr 2014;2014:346–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [58].Griffiths P, Jones S, Maben J. State of the art metric for nursing: A rapid appraisal. London: King's College London, University of London, 2008. [Google Scholar]
- [59].Gulwadi GB, Joseph A, Keller AB. Exploring the impact of the physical environment on patient outcomes in ambulatory care settings. HERD 2009;2:21–41. [DOI] [PubMed] [Google Scholar]
- [60].Guo P. Preoperative education interventions to reduce anxiety and improve recovery among cardiac surgery patients: a review of randomised controlled trials. J Clin Nurs 2015;24:34–46. [DOI] [PubMed] [Google Scholar]
- [61].Hall KT, Loscalzo J, Kaptchuk TJ. Genetics and the placebo effect: the placebome. Trends Mol Med 2015;21:285–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [62].Hansen BS, Rortveit K, Leiknes I, Morken I, Testad I, Joa I, Severinsson E. Patient experiences of uncertainty—a synthesis to guide nursing practice and research. J Nurs Manag 2012;20:266–77. [DOI] [PubMed] [Google Scholar]
- [63].Hardman DI, Geraghty AW, Lewith G, Lown M, Viecelli C, Bishop FL. From substance to process: a meta-ethnographic review of how healthcare professionals and patients understand placebos and their effects in primary care. Health (London) 2018:1363459318800169. [DOI] [PubMed] [Google Scholar]
- [64].Hatfield LA, Pearce M, Del Guidice M, Cassidy C, Samoyan J, Polomano RC. The professional appearance of registered nurses: an integrative review of peer-refereed studies. J Nurs Adm 2013;43:108–12. [DOI] [PubMed] [Google Scholar]
- [65].Hessels AJ, Flynn L, Cimiotti JP, Cadmus E, Gershon RRM. The impact of the nursing practice environment on missed nursing care. Clin Nurs Stud 2015;3:60–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [66].Horing B, Weimer K, Muth ER, Enck P. Prediction of placebo responses: a systematic review of the literature. Front Psychol 2014;5:1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Iyendo TO, Uwajeh PC, Ikenna ES. The therapeutic impacts of environmental design interventions on wellness in clinical settings: a narrative review. Complement Ther Clin Pract 2016;24:174–88. [DOI] [PubMed] [Google Scholar]
- [68].Jakimowicz S, Stirling C, Duddle M. An investigation of factors that impact patients' subjective experience of nurse-led clinics: a qualitative systematic review. J Clin Nurs 2015;24:19–33. [DOI] [PubMed] [Google Scholar]
- [69].Jellinek EM. Rôle of the placebo in tests for drug discrimination. Fed Proc 1946;5:184. [PubMed] [Google Scholar]
- [70].Johansson P, Oléni M, Fridlund B. Patient satisfaction with nursing care in the context of health care: a literature study. Scand J Caring Sci 2002;16:337–44. [DOI] [PubMed] [Google Scholar]
- [71].Kaptchuk TJ. Placebo studies and ritual theory: a comparative analysis of Navajo, acupuncture and biomedical healing. Philos Trans R Soc Lond B Biol Sci 2011;366:1849–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].Klinger R, Blasini M, Schmitz J, Colloca L. Nocebo effects in clinical studies: hints for pain therapy. Pain Rep 2017;2:e586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].LaSala KB, Nelson J. What contributes to professionalism? Medsurg Nurs 2005;14:63–7. [PubMed] [Google Scholar]
- [74].Laursen J, Danielsen A, Rosenberg J. Effects of environmental design on patient outcome: a systematic review. HERD 2014;7:108–19. [DOI] [PubMed] [Google Scholar]
- [75].Leder D, Krucoff MW. The touch that heals: the uses and meanings of touch in the clinical encounter. J Altern Complement Med 2008;14:321–7. [DOI] [PubMed] [Google Scholar]
- [76].Lee JH. The effects of music on pain: a meta-analysis. J Music Ther 2016;53:430–77. [DOI] [PubMed] [Google Scholar]
- [77].Lee SE, Scott LD. Hospital nurses work environment characteristics and patient safety outcomes: a literature review. West J Nurs Res 2018;40:121–45. [DOI] [PubMed] [Google Scholar]
- [78].Leslie JL, Lonneman W. Promoting trust in the registered nurse-patient relationship. Home Healthc Now 2016;34:38–42. [DOI] [PubMed] [Google Scholar]
- [79].MacAllister L, Zimring C, Ryherd E. Environmental variables that influence patient satisfaction: a review of the literature. HERD 2016;10:155–69. [DOI] [PubMed] [Google Scholar]
- [80].Machiels M, Metzelthin SF, Hamers JPH, Zwakhalen SMG. Interventions to improve communication between people with dementia and nursing staff during daily nursing care: a systematic review. Int J Nurs Stud 2017;66:37–46. [DOI] [PubMed] [Google Scholar]
- [81].MacMillan K. The hidden curriculum: what are we actually teaching about the fundamentals of care? Nurs Leadersh (Tor Ont) 2016;29:37–46. [DOI] [PubMed] [Google Scholar]
- [82].Martin LC, Arenas-Montoya NM, Barnett TO. Impact of nurse certification rates on patient satisfaction and outcomes: a literature review. J Contin Educ Nurs 2015;46:549–54. [DOI] [PubMed] [Google Scholar]
- [83].Miller FG, Colloca L, Kaptchuk TJ. The placebo effect: illness and interpersonal healing. Perspect Biol Med 2009;52:518–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [84].Miller FG, Kaptchuk TJ. The power of context: reconceptualizing the placebo effect. J R Soc Med 2008;101:222–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [85].Miller LR, Miller FG. Understanding placebo effects: implications for nursing practice. Nurs Outlook 2015;63:601–6. [DOI] [PubMed] [Google Scholar]
- [86].Moerman DE, Jonas WB. Deconstructing the placebo effect and finding the meaning response. Ann Intern Med 2002;136:471–6. [DOI] [PubMed] [Google Scholar]
- [87].Morrison SM, Symes L. An integrative review of expert nursing practice. J Nurs Scholarsh 2011;43:163–70. [DOI] [PubMed] [Google Scholar]
- [88].Müller-Schwefe G, Jaksch W, Morlion B, Kalso E, Schäfer M, Coluzzi F, Huygen F, Kocot-Kepska M, Mangas AC, Margarit C, Ahlbeck K, Mavrocordatos P, Alon E, Collett B, Aldington D, Nicolaou A, Pergolizzi J, Varrassi G. Make a CHANGE: optimising communication and pain management decisions. Curr Med Res Opin 2011;27:481–8. [DOI] [PubMed] [Google Scholar]
- [89].Nemcová J, Hlinková E. The efficacy of diabetic foot care education. J Clin Nurs 2014;23:877–82. [DOI] [PubMed] [Google Scholar]
- [90].O'Gara PE, Fairhurst W. Therapeutic communication part 1: general approaches that enhance the quality of the consultation. Accid Emerg Nurs 2004;12:166–72. [DOI] [PubMed] [Google Scholar]
- [91].Ozsoy SA, Ozgür G, Durmaz Akyol A. Patient expectation and satisfaction with nursing care in Turkey: a literature review. Int Nurs Rev 2007;54:249–55. [DOI] [PubMed] [Google Scholar]
- [92].Paniagua-Collado M, Cauli O. Non-pharmacological interventions in patients with spinal cord compression: a systematic review. J Neurooncol 2018;136:423–34. [DOI] [PubMed] [Google Scholar]
- [93].Papastavrou E, Efstathiou G, Charalambous A. Nurses' and patients' perceptions of caring behaviours: quantitative systematic review of comparative studies. J Adv Nurs 2011;67:1191–205. [DOI] [PubMed] [Google Scholar]
- [94].Park M, Giap TT, Lee M, Jeong H, Jeong M, Go Y. Patient- and family-centered care interventions for improving the quality of health care: a review of systematic reviews. Int J Nurs Stud 2018;87:69–83. [DOI] [PubMed] [Google Scholar]
- [95].Peiris N, Blasini M, Wright T, Colloca L. The placebo phenomenon: a narrow focus on psychological models. Perspect Biol Med 2018;61:388–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Porr C, Dawe D, Lewis N, Meadus RJ, Snow N, Didham P. Patient perception of contemporary nurse attire: a pilot study. Int J Nurs Pract 2014;20:149–55. [DOI] [PubMed] [Google Scholar]
- [97].Price DD, Finniss DG, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought. Annu Rev Psychol 2008;59:565–90. [DOI] [PubMed] [Google Scholar]
- [98].Refai M, Andolfi M, Gentili P, Pelusi G, Manzotti F, Sabbatini A. Enhanced recovery after thoracic surgery: patient information and care-plans. J Thorac Dis 2018;10:S512–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [99].Rehman SA, Ali PA. A review of factors affecting patient satisfaction with nurse led triage in emergency departments. Int Emerg Nurs 2016;29:38–44. [DOI] [PubMed] [Google Scholar]
- [100].Rossettini G, Carlino E, Testa M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet Disord 2018;19:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [101].Schedlowski M, Enck P, Rief W, Bingel U. Neuro-bio-behavioral mechanisms of placebo and nocebo responses: implications for clinical trials and clinical practice. Pharmacol Rev 2015;67:697–730. [DOI] [PubMed] [Google Scholar]
- [102].Schenk LA, Krimmel SR, Colloca L. Observe to get pain relief: current evidence and potential mechanisms of socially learned pain modulation. PAIN 2017;158:2077–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [103].Schenk PW. “Just breathe normally”: word choices that trigger nocebo responses in patients. Am J Nurs 2008;108:52–7. [DOI] [PubMed] [Google Scholar]
- [104].Schmitz J, Kamping S, Wiegratz J, Müller M, Stork J, Colloca L, Flor H, Klinger R. Impact of patient information leaflets on pain medication intake behavior: a pilot study. Pain Rep 2017;2:e620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [105].Schofield P, Gough K, Lotfi-Jam K, Bergin R, Ugalde A, Dudgeon P, Crellin W, Schubach K, Foroudi F, Tai KH, Duchesne G, Sanson-Fisher R, Aranda S. Nurse-led group consultation intervention reduces depressive symptoms in men with localised prostate cancer: a cluster randomised controlled trial. BMC Cancer 2016;16:637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [106].See MTA, Kowitlawakul Y, Tan AJQ, Liaw SY. Expectations and experiences of patients with osteoarthritis undergoing total joint arthroplasty: an integrative review. Int J Nurs Pract 2018;24:e12621. [DOI] [PubMed] [Google Scholar]
- [107].Sibanda A, Carnes D, Visentin D, Cleary M. A systematic review of the use of music interventions to improve outcomes for patients undergoing hip or knee surgery. J Adv Nurs 2018. 10.1111/jan.13860. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- [108].Sirch L, Salvador L, Palese A. Communication difficulties experienced by deaf male patients during their in-hospital stay: findings from a qualitative descriptive study. Scand J Caring Sci 2017;31:368–77. [DOI] [PubMed] [Google Scholar]
- [109].Smith MY, DuHamel KN, Egert J, Winkel G. Impact of a brief intervention on patient communication and barriers to pain management: results from a randomized controlled trial. Patient Educ Couns 2010;81:79–86. [DOI] [PubMed] [Google Scholar]
- [110].Song M, Li N, Zhang X, Shang Y, Yan L, Chu J, Sun R, Xu Y. Music for reducing the anxiety and pain of patients undergoing a biopsy: a meta-analysis. J Adv Nurs 2018;74:1016–29. [DOI] [PubMed] [Google Scholar]
- [111].Stalpers D, de Brouwer BJM, Kaljouw MJ, Schuurmans MJ. Associations between characteristics of the nurse work environment and five nurse-sensitive patient outcomes in hospitals: a systematic review of literature. Int J Nurs Stud 2015;52:817–35. [DOI] [PubMed] [Google Scholar]
- [112].Symon A, Williams B, Adelasoye QA, Cheyne H. Nocebo and the potential harm of “high risk” labelling: a scoping review. J Adv Nurs 2015;71:1518–29. [DOI] [PubMed] [Google Scholar]
- [113].Tabatabaee A, Tafreshi MZ, Rassouli M, Aledavood SA, AlaviMajd H, Farahmand SK. Effect of therapeutic touch in patients with cancer: a literature review. Med Arch 2016;70:142–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [114].Testa M, Rossettini G. Enhance placebo, avoid nocebo: how contextual factors affect physiotherapy outcomes. Man Ther 2016;24:65–74. [DOI] [PubMed] [Google Scholar]
- [115].Thomas CM, Ehret A, Ellis B, Colon-Shoop S, Linton J, Metz S. Perception of nurse caring, skills, and knowledge based on appearance. J Nurs Adm 2010;40:489–97. [DOI] [PubMed] [Google Scholar]
- [116].Tobiano G, Marshall A, Bucknall T, Chaboyer W. Patient participation in nursing care on medical wards: an integrative review. Int J Nurs Stud 2015;52:1107–20. [DOI] [PubMed] [Google Scholar]
- [117].Van der Elst E, Dierckx de Casterle B, Gastmans C. Elderly patients' and residents' perceptions of “the good nurse”: a literature review. J Med Ethics 2012;38:93–7. [DOI] [PubMed] [Google Scholar]
- [118].Varelmann D, Pancaro C, Cappiello EC, Camann WR. Nocebo-induced hyperalgesia during local anesthetic injection. Anesth Analg 2010;110:868–70. [DOI] [PubMed] [Google Scholar]
- [119].Vase L, Amanzio M, Price DD. Nocebo vs. placebo: the challenges of trial design in analgesia research. Clin Pharmacol Ther 2015;97:143–50. [DOI] [PubMed] [Google Scholar]
- [120].Verschueren M, Kips J, Euwema M. A review on leadership of head nurses and patient safety and quality of care. Adv Health Care Manag 2013;14:3–34. [DOI] [PubMed] [Google Scholar]
- [121].Wager TD, Atlas LY. The neuroscience of placebo effects: connecting context, learning and health. Nat Rev Neurosci 2015;16:403–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [122].Walike BC, Meyer B. Relation between placebo reactivity and selected personality factors. An exploratory study. Nurs Res 1966;15:119–23. [PubMed] [Google Scholar]
- [123].Watson J. Nursing: The philosophy and science of caring. Revised ed Boulder: University Press of Colorado, 2008. [Google Scholar]
- [124].Webster RK, Weinman J, Rubin GJ. A systematic review of factors that contribute to nocebo effects. Health Psychol 2016;35:1334–55. [DOI] [PubMed] [Google Scholar]
- [125].Wiechula R, Conroy T, Kitson AL, Marshall RJ, Whitaker N, Rasmussen P. Umbrella review of the evidence: what factors influence the caring relationship between a nurse and patient? J Adv Nurs 2016;72:723–34. [DOI] [PubMed] [Google Scholar]
- [126].Wiles R, Cott C, Gibson BE. Hope, expectations and recovery from illness: a narrative synthesis of qualitative research. J Adv Nurs 2008;64:564–73. [DOI] [PubMed] [Google Scholar]
- [127].Wilson C, Bungay H, Munn-Giddings C, Boyce M. Healthcare professionals' perceptions of the value and impact of the arts in healthcare settings: a critical review of the literature. Int J Nurs Stud 2016;56:90–101. [DOI] [PubMed] [Google Scholar]
- [128].Wong CA, Cummings GG. The relationship between nursing leadership and patient outcomes: a systematic review. J Nurs Manag 2007;15:508–21. [DOI] [PubMed] [Google Scholar]
- [129].Wong CA, Cummings GG. The relationship between nursing leadership and patient outcomes: a systematic review update. J Nurs Manag 2013;21:709–24. [DOI] [PubMed] [Google Scholar]
- [130].Woo BFY, Lee JXY, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: a systematic review. Hum Resour Health 2017;15:63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [131].Woo KY. Unravelling nocebo effect: the mediating effect of anxiety between anticipation and pain at wound dressing change. J Clin Nurs 2015;24:1975–84. [DOI] [PubMed] [Google Scholar]
- [132].You E, Kim D, Harris R, D'Alonzo K. Effects of auricular acupressure on pain management: a systematic review. Pain Manag Nurs 2018;S1524–9042:30380–6. [DOI] [PubMed] [Google Scholar]
- [133].Zhang JM, Wang P, Yao JX, Zhao L, Davis MP, Walsh D, Yue GH. Music interventions for psychological and physical outcomes in cancer: a systematic review and meta-analysis. Support Care Cancer 2012;20:3043–53. [DOI] [PubMed] [Google Scholar]
- [134].Zhou L, Liu XL, Tan JY, Yu HP, Pratt J, Peng YQ. Nurse-led educational interventions on cancer pain outcomes for oncology outpatients: a systematic review. Int Nurs Rev 2015;62:218–30. [DOI] [PubMed] [Google Scholar]