

Abstract
Introduction
In this study, we assessed the adequacy of the two echocardiographic parameters representing the longitudinal systolic function of the ventricles, MAPSE & TAPSE, in perioperative monitoring.
Aims
1. The assessment of MAPSE and TAPSE during the early (4 weeks) postoperative period after surgical correction of congenital heart defects in infants, performed with CPB. 2. The verification of the hypothesis, that the significant decline of TAPSE observed in this period is not related to the global RV systolic dysfunction. For this reason, systolic function of the RV was additionally assessed with another echocardiographic parameter: RVFAC.
Material and methods
Prospective study with 51 infants operated due to ASDII, VSD, AVSD and TOF. Four measurements of MAPSE,TAPSE and RVFAC were performed in the apical four-chamber projection. TAPSE and MAPSE were expressed as metric values and z-score; RV FAC values were expressed in percentages.
Results
TAPSE uniformly declined in the first postoperative day down to 34.5% of the initial value (p <0.00001), then gradually increased: up to 42.9% and 52% respectively, remaining significantly lower than preoperatively (p <0.001). RV FAC: increased by 21% (p <0.01), then remained stable in consecutive examinations. MAPSE declined by 21% during the first postoperative day, but with promptly normalized completely.
Conclusions
The movement of both AV valve annuli is subjected to different, not fully understood influences. The relatively slight decline of MAPSE makes this parameter suitable for the assessment of the postoperative LV systolic function. Deep, long-lasting decline of TAPSE, uniform in the whole group, does not permit to use this parameter and suggests the choice of another one, e.g. RVFAC.
Keywords: tricuspid annular plane systolic excursion, mitral annular plane systolic excursion, right ventricular fractional area change, postoperative intensive care
Introduction
The evaluation of post-operative heart function is crucial in the selection of adequate pharmacological therapy, prevention of heart dysfunction, planning of possible reoperations and in long-term prognosis. The study presented here evaluated the usefulness of two echocardiographic parameters: MAPSE and TAPSE (mitral and tricuspid annular plane systolic excursion), which determine the range of the tricuspid annular plane systolic excursion by means of M-mode measurement in the apical four-chamber projection(1,2). Both of these parameters demonstrate a well-documented correlation with the ventricular ejection fraction(3–5), and, owing to the simplicity of performance and reproducibility of the results, are widely used.
The aim of the study
The aim of the study was to: 1) to assess MAPSE and TAPSE after surgical correction of selected congenital heart defects in infants, conducted under cardiopulmonary bypass, in the immediate postoperative period (up to 4 weeks after surgery); 2) verification of the hypothesis that a significant decrease in the value of TAPSE observed in this period is not an expression of global right ventricular systolic dysfunction; 3) creating a basis for long-term observation of the variability of MAPSE and TAPSE in patients after correction of congenital heart disease.
The impulse to conduct the study was the observation of a sharp drop in the value of TAPSE during tests routinely performed in the postoperative therapy unit, which suggested a deep impairment of the right ventricular systolic function. At the same time, however, neither the clinical picture nor the entire echocardiographic study indicated the occurrence of severe right ventricular failure. Due to this fact, it was decided to evaluate the RV systolic function with another echocardiographic parameter, including in the analysis the function of a greater section of the right ventricular muscle than in the case of TAPSE. RV FAC (right ventricular fractional area change) was selected, which consists in calculating the percentage change in the surface area of this part of the right ventricle, which is visible in the apical four-chamber projection(5,6). This parameter is also characterized by the simplicity and repeatability of measurements.
Method
The study was prospective. 51 subsequently operated patients were involved in the study, aged 1–12 months, qualified for the correction of the tetralogy of Fallot (ToF), atrioventricular septal defect (AVSD), ventricular septal defect (VSD) and ostium secundum atrial septal defect, (ASDII). The operations were performed by the same surgeon with the use of CPB, cannulation of both superior and inferior caval veins right atrial access and moderate hypothermia. In the apical four-chamber projection, the area of the right ventricle was measured in the late systolic and late diastolic stage to calculate RV FAC and, using M-mode, TAPSE and MAPSE. The study was performed by one echocardiographer, the values of TAPSE and MAPSE were expressed in millimeters and as z-score, while RV FAC values were expressed in percentages.
Each patient underwent four examinations: pre-operative, immediately after surgery (1st–3rd day), in the 7th postoperative day (without catecholamines, respiratory support, chest drains) and during the outpatient treatment – in the 22nd postoperative day.
The demographic data characterizing the examined group of patients are presented in Tab. 1.
Tab. 1.
Data characterizing the study group
| Age (months) | 4.58 ± 2.56 |
| Boys – N (%) | 26 (50.98) |
| Girls – N (%) | 25 (49.02) |
| Weight (g) | 5685.45 ± 1506.89 |
| CBP time (min) | 77.82 ± 29.16 |
| AoCC time (min) | 40.70 ± 16.30 |
| Down syndrome – W (%) | 5 (9.80) |
| Type of heart defect | |
| ASD – N (%) | 4 (7.84) |
| VSD – N (%) | 26 (50.98) |
| AVSD – N (%) | 12 (23.52) |
| ToF – N (%) | 9 (17.64) |
ASD – atrial septal defect; ToF – tetralogy of Fallot; VSD – ventricular septal defect; AVSD – atrioventricular septal defect; N – group size; mean ± standard deviation
The statistical analysis of the results was performed in the Statistica 12.0 PL program. Due to the distribution of data, in order to assess the significance of the changes taking place in the values of TAPSE and MAPSE and RV FAC parameters, the non-parametric Wilcoxon test was used before and after the surgery. The Spearman correlation test was used to assess the correlation of individual variables. The values of p <0.05 were considered statistically significant.
Results
The values of the parameters assessed in subsequent tests are presented in Tab. 2.
Tab. 2.
Detailed values of TAPSE, RV FAC and MAPSE parameters in individual measurements before surgery (measurement 0) and after surgery (measurement 1, 2, 3) – median and quartile distribution
| Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
|---|---|---|---|---|
| TAPSE (mm) | 15.2 (13.26–18.5) | 4.82 (4.10–5.97) | 6.37 (5.40–7.31) | 7.88 (6.62–8.76) |
| RV FAC (%) | 43.07 (35.71–51.06) | 53.57 (44.04–60.99) | 54.16 (48.48–60.00) | 54.54 (46.66–60.86) |
| MAPSE (mm) | 7.67 (6.92–8.94) | 5.88 (5.27–6.92) | 6.80 (6.00–8.09) | 7.66 (7.06–9.00) |
Fig. 1, Fig. 2, Fig. 3 graphically present the results of the study.
Fig. 1.
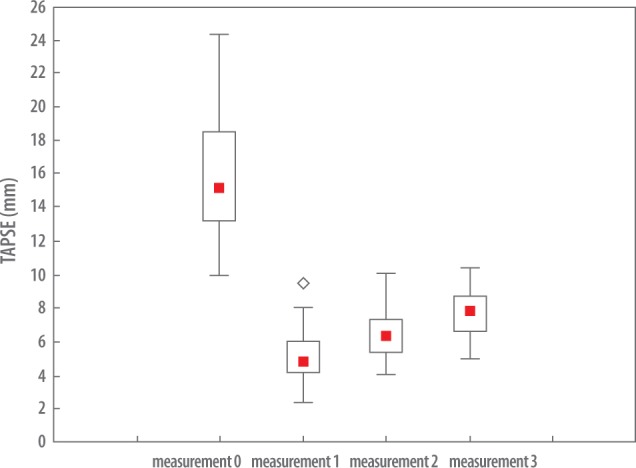
Temporary change of the TAPSE parameter during the study period: measurement 0 – before surgery, measurement 1, 2, 3 – after surgery. The red point in the square corresponds to the median, the upper and lower edge of the quadrangle – quartile spacing, the arms of the graph – values 1–99% of TAPSE measurements, and free points – outliers
Fig. 2.
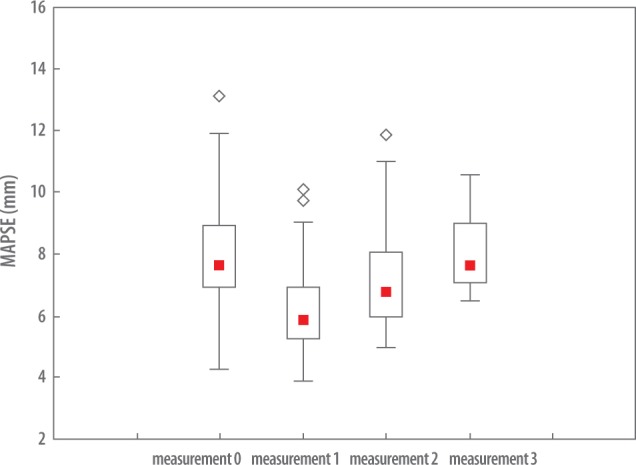
Temporary change of the MAPSE parameter during the study period: measurement 0 – before surgery, measurements 1, 2, 3 – after surgery
Fig. 3.
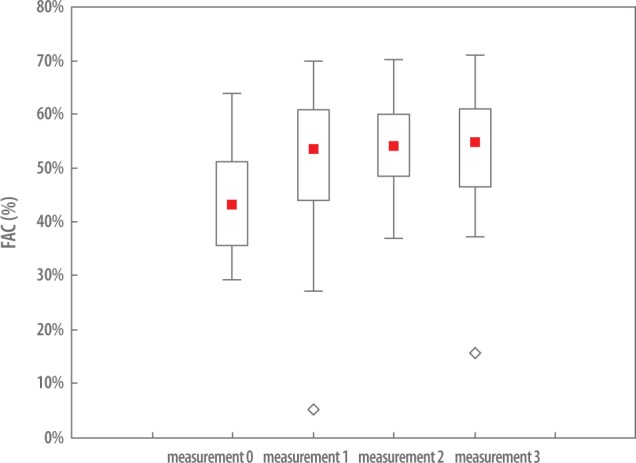
Temporary change of the RV FAC parameter during the test period: measurement 0 – before surgery, measurements 1, 2, 3 – after surgery
Analyzing the change in TAPSE parameter, a statistically significant (assuming p <0.05) difference between the preoperative measurement (measurement 0) and all the measurements performed during the post-operative care period (measurement 1, 2, 3) (p <0.001) was observed (Tab. 2, Fig. 1).
In the postoperative period, the MAPSE values from the measurements 1 and 2 showed a statistically significant variation in relation to the pre-operative study (measurement 0). There was no statistically significant difference noted in the measurement 3 (p <0.955), which indicates that the MAPSE values significantly approached the preoperative level.
The change in the RV FAC parameter after the surgery (measurement 1, 2, 3) was statistically significantly increased (p <0.001) in relation to the initial test (measurement 1).
There was no statistically significant (assuming p <0.05) correlation of the TAPSE parameter with the RV FAC parameter in the measurements performed: TAPSE measurement 0 – RV FAC measurement 0 (r = –0.29, p <0.109); TAPSE measurement 1 – RV FAC measurement 1 (r = 0.11, p <0.564); TAPSE measurement 2 – RV FAC measurement 2 (r = –0.29, p <0.116); TAPSE measurement 3 – RV FAC measurement 3 (r = 0.13, p <0.501).
Table 3 contains the assessed parameters measurement results subdivided by particular heart defects.
Tab. 3.
Detailed changes in TAPSE, RV FAC and MAPSE parameters according to heart defects in particular measurements before the surgery (measurement 0) and after surgery (measurement 1, 2, 3) – median and quartile distribution
| ASD N = 4 | Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
| TAPSE (mm) | 16.60 (14.97–21.22) | 7.00 (3.72–9.46) | 7.77 (6.74–8.67) | 7.68 (6.62–8.75) | |
| MAPSE (mm) | 6.95 (6.46–10.99) | 6.12 (4.98–7.99) | 6.88 (6.56–8.99) | 11.71 (8.57–14.85) | |
| RV FAC (%) | 32.66 (0.00–52.11) | 48.75 (39.28–51.31) | 50.66 (44.06–70.12) | 39.11 (37.21–41.02) | |
| VSD N = 26 | Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
| TAPSE (mm) | 15.17 (12.62–18.28) | 4.98 (4.18–5.98) | 6.11 (5.40–7.31) | 7.44 (6.80–8.25) | |
| MAPSE (mm) | 8.04 (7.02–9.30) | 6.07 (5.47–6.70) | 6.59 (5.69–7.55) | 7.20 (7.02–8.41) | |
| RV FAC (%) | 43.94 (37.50–52.00) | 59.25 (48.15–61.90) | 52.83 (48.48–58.33) | 54.65 (52.33–59.31) | |
| ToF N = 9 | Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
| TAPSE (mm) | 15.20 (14.63–17.50) | 4.60 (3.60–5.65) | 6.55 (5.97–7.07) | 8.17 (6.49–9.21) | |
| MAPSE (mm) | 8.27 (6.66–9.27) | 5.66 (5.10–8.27) | 7.73 (6.31–9.39) | 9.01 (8.95–9.72) | |
| RV FAC (%) | 39.39 (35.08–46.66) | 49.31 (34.84–59.54) | 54.17 (50.75–59.57) | 55.17 (39.39–61.53) | |
| AVSD N = 12 | Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
| TAPSE (mm) | 15.47 (13.28–18.98) | 4.82 (3.97–5.71) | 6.2 (5.11–7.02) | 8.47 (6.57–8.78) | |
| MAPSE (mm) | 7.21 (6.74–8.29) | 5.78 (5.46–6.92) | 7.33 (6.14–8.25) | 7.91 (7.15–9.00) | |
| RV FAC (%) | 42.11 (30.76–43.85) | 53.97 (42.32–59.58) | 54.97 (50.00–60.00) | 56.01 (50.00–68.86) |
Discussion
Both TAPSE and MAPSE showed a statistically significant decrease in the first 24 hours after the surgery, however, there was a much greater decrease in TAPSE, whose value in the first study decreased by nearly 70% of the baseline value; the MAPSE value decreased in the first day of the follow-up by only about 23%. In the first postoperative study, a statistically significant increase in RV FAC was determined (about 24% of the baseline value), which contradicts severe global impairment of the right ventricular systolic function, which such a significant decrease in TAPSE would suggest.
In subsequent measurements, a gradual increase in TAPSE was observed towards the normal values. However, even in the fourth measurement, all the values were below the value of z-score = –2 SD (mean = –3.32 SD) (Tab. 4). Small dispersion of the measurement values is also worth noting, as it indicates the surgery performed had a homogeneous effect on TAPSE in the entire examined group. The increasing trend in MAPSE was parallel to the trend in TAPSE. However, due to a relatively small reduction in the baseline value, total normalization took place in the fourth measurement values and all the mean values of MAPSE, including the ones obtained in the first post-operative measurement, were within the normal limits (mean z-score ≥–1). Relatively smallest decrease in TAPSE and MAPSE was observed in the group of ASDII patients. However, this may have been an expression of the small size of this subgroup. In the case of other types of defects, the measurement results did not differ significantly.
Tab. 4.
Change in the TAPSE z-score value for individual measurements
| Measurement 0 | Measurement 1 | Measurement 2 | Measurement 3 | |
|---|---|---|---|---|
| Z-score TAPSE | 2.15 ± 2.22 | −4.99 ± 1.33 | −4.16 ± 1.12 | −3.32 ± 0.98 |
The RV FAC values remained at the same level in the subsequent measurements, slightly exceeding the baseline values.
TAPSE and MAPSE is the distance which the AV valve annuli cover between their highest point reached at the peak of atrial contraction and the lowest one – at the maximum ventricular contraction(1,2,6). Its assessment consists in the M-mode measurement of the extent of the motion of the plane of the atrioventricular annuli in the apical four-chamber projection (Fig. 4). The diastolic phase of the upward (directed towards the base of the heart) motion of the AV annuli consists of two sub-periods: ventricular relaxation and atrial contraction (atrial ascent). The range of the excursion of the plane of the atrioventricular annuli during the contraction period depends on the initial position achieved as a result of the atrial contraction, and thus both the systolic and diastolic functions not only of the chambers, but also of the atria. In normal conditions, there are significant differences between the range and the dynamics of the atrioventricular annuli:
Fig. 4.

Scatter plot of the TAPSE and RV FAC parameter in particular measurements
TAPSE is significantly higher than MAPSE;
The mean amplitude of the tricuspid annulus during the period of atrial systole is significantly greater than the one of the mitral annulus;
MAPSE lasts longer than TAPSE;
The duration of the mitral annulus ascent phase is shorter than the one of the tricuspid annulus.
The reasons for these differences are not obvious and may result from the conditions described below(6). The left ventricle (LV) has a number of spirally oriented fibers (subendocardial and subepicardial ones) responsible for the presence of the torsional LV systolic movement component, which is just an important component of LV mechanics as the longitudinal component is – the dimensions of the chamber decrease in all directions in the systolic period. The right ventricular muscle fibers have a different orientation (virtually no spiral fibers), which makes the longitudinal component dominate in the systolic motion of the RV walls, increasing the extent of the excursion of the tricuspid annulus towards the apex. Furthermore, the range of the elevation of the plane of the tricuspid annulus during the period of atrial systole is greater than the one of the mitral annulus. This can be explained by the different construction of atrial walls, in particular their appendages. In this aspect, the content and distribution of the pectinate muscles seem the most significant. The right atrial appendage is adjacent to the external part of the tricuspid annulus and the fibers of the pectinate muscles are oriented in the cephalocaudal axis in the direction perpendicular to the plane of the tricuspid valve annulus. Therefore, their contraction exerts a significant influence on its range of motion – especially, of its lateral part. The pectinate muscles of the left atrial appendage, less numerous and less prominent, have no direct relation to the mitral annulus, which results in their contraction having less impact of on MAPSE range and dynamics. Also the much greater susceptibility of the right ventricular wall to stretching than of the thick wall of the left ventricle seems not without significance(6).
A high degree of correlation was found between TAPSE and MAPSE, as well as EF RV (and RV FAC) and EF LV, both in healthy subjects and those suffering from various diseases impairing ventricular function(3–13). TAPSE and MAPSE have a well-established application in the monitoring of ventricular systolic function and doubtlessly could be a very useful instrument for hemodynamic monitoring immediately after surgery. However, as it has already been mentioned, daily observations resulting from early postoperative measurements pointed to intense reduction in TAPSE values, calling into question the possibility of using these parameters. A systematic study whose results are presented in this publication, confirmed this observation – immediately after the surgery, a decrease in TAPSE of almost 70% was observed in all patients of the study group, which did not normalize during a 3-week postoperative follow-up. Simultaneously, a decrease in MAPSE was also observed, but it was much smaller (on average 23% of the baseline value), and there was a return to the baseline values during the follow-up period. Simultaneous assessment of the right ventricular systolic function with the use of a different parameter (one showing strong correlation with TAPSE in normal conditions) – RV FAC – did not demonstrate global impairment of right ventricular systolic function, but its small, statistically significant increase.
In the opinion of the authors, it is possible to identify the reasons for the observed disproportion of TAPSE and MAPSE decreases. These reasons seem to be primarily related to the technical aspects of the operation performed. The direct observation of the heart during the cardiosurgical procedure casts a lot of light on this issue. Following the surgical exposure of the heart it is easy to follow the movement of the right atrioventricular groove, which is the external equivalent of the tricuspid annulus. With reference to the assessment of the motion of the groove, the following stages of the operation can be distinguished:
Opening of the pericardium – no visible change in the motion of the groove was observed.
Aortic cannulation – also without any noticeable effect.
The cannulation of the caval veins, especially the inferior vena cava – a moderate decrease in mobility.
Probably the greatest influence on the dynamics of the tricuspid annulus motion is exerted by the dissection of the right atrium (RA) front wall in order to gain access to the interior of the heart, and its subsequent suturing. The suture, covering the at least 2/3 of the appendage wall impairs both the contraction and relaxation of the pectinate muscles of the right atrium (RA) appendage. The mobility of the AV groove after aortic cross-clamp removal and the restoration of spontaneous cardiac function is evidently lower than immediately after cannulation, before the atrium is dissected, irrespective of the impression RV muscle contraction makes (no significant differences were observed between patients with right ventricular hypertrophy and hypokinesis). The decanulation of the caval veins at the next stage does not visibly improve the dynamics of the AV groove motion. The observation of the heart during the procedure of coming off cardiopulmonary bypass and the actions completing the surgery suggests that the maximum reduction of TAPSE occurs already during the coming off the extracorporeal circulation, certainly before the chest is closed. Therefore, extracardiac causes (adhesions, the presence of intravascular cannulas, drains, fluid in serous cavities or other mechanical factors) seem to exert less influence on the observed impairment of TAPSE. An argument for the significant impact of the atrial wall dissection on the decrease of TAPSE may be a very weakly expressed component of atrial systole (atrial ascent) of the tricuspid annulus motion curve.
A similar course of TAPSE and MAPSE trends suggests that, in addition to the factors described above, both chambers are subject to similar influences – most likely metabolic ones (stun), which relatively quickly subside (full MAPSE normalization and the increase in the TAPSE values determined in the fourth measurement). The longitudinal RV systolic function is subjected to additional influences, which do not subside despite the hemodynamic normalization.
Surgical treatment of a range of congenital heart defects requires interference in the structure of the right ventricle – e.g. widening of a hypoplastic outflow tract with a pericardial patch or a compound vascular prosthesis in tetralogy of Fallot. Usually, early correction results are completely satisfactory, however, their long-term course is burdened with a large number of complications. A good example here are the consequences of the regurgitation of the deformed pulmonary valve, leading to progressive right ventricular insufficiency, failure requiring a reconstructive surgery or implantation of an artificial pulmonary valve as a result. Echocardiographic RV imaging and the assessment of its hemodynamics are fraught with significant technical difficulties even in healthy patients, due to the position of the right ventricle in the immediate vicinity of the sternum and the complex geometry of its cavity, which prevents the use of simple geometric models to calculate its volume. After a Fallot tetralogy repair operation, additional factors appear which disturb imaging: adhesions between the right ventricular free wall, frontal sections of the lungs and the chest wall, presence of post-surgery scars in cardiac walls, patches or vascular prostheses widening the right ventricular outflow tract (RVOT), inconsistent contractility of RV walls caused by the resection and intraventricular muscle structure dissection, and, finally, the intra-cellular conduction disturbances in these patients.
The imaging method which allows to bypass the limitations listed above and is the gold standard for the assessment of the RV function after ToF correction, especially in patients over 10, is MRI. Magnetic resonance allows for precise assessment of the volume of the chamber and its lesions, it also makes it possible to calculate RV ejection fraction and pulmonary regurgitation fraction. Its limited availability, inconvenience and potentially adverse impact on the health of the patients examined prevent it from being a method adequate for ongoing post-operative follow-up. Echocardiography, with its non-invasiveness and easy accessibility, remains the main monitoring tool, hence the search for the echocardiographic parameters reflecting the RV function, which could be assessed even in the difficult postoperative conditions and which would enable the patients to be qualified for MRI, is ongoing. High expectations are held of new techniques (Doppler tissue imaging – DTI, speckle tracking echocardiography – STE). However, they are also not free from the limitations resulting from the reduction of the acoustic window and the position of a significant part of the right ventricular wall too close to the head. The use of TAPSE and MAPSE, which require a relatively small acoustic window, is a very attractive alternative to calculating the ejection fraction or even RV FAC, which requires precise visualization of much larger sections of the right ventricle.
In studies concerning TAPSE, the correlations between TAPSE and RV EF / RVE DVI, as well as MAPSE, RV EF and RV EDVI were analyzed in patients after congenital heart disease surgeries. The results published are ambiguous, which seems to be related to inhomogeneous selection of patients and not fully clear effect of various postoperative abnormalities on ventricular systolic function. Some authors demonstrated a statistically significant relationship(14–19), which would justify the use of these parameters in making a decision on expectant management or qualifying patients for MRI; others(20) did not confirm a satisfactory correlation, concluding that, based on the parameters of the longitudinal component of the RV systolic function (also STE and DTI), EF RV cannot be estimated. Lower TAPSE values were observed in all operated patients than in the control group selected by age. There were also differences in this respect. In the analysis of the largest group of patients after surgical correction of tetralogy of Fallot(18,19) it was suggested that, in the immediate postoperative period, TAPSE values were normal, while during long-term follow-up they decreased. After seven years, they reached values below 2 SD of the control group. The MAPSE values showed a similar trend during the observations.
In the first published study(21) analyzing TAPSE and MAPSE in adults operated on CPB due to CAD and/or valve defects, a significant reduction in TAPSE was observed in the studies immediately after surgery and then a gradual increase in its value after six months, but without full normalization. MAPSE showed much less intense dynamics. RV and RA dysfunction was suggested to be the explanation, resulting from poorer cardioplegic protection, a greater influence of significant amounts of heat from surgical lamps on the frontally located right ventricle, flow of relatively warm blood to the right ventricle (the atrium was cannulated, not superior veni cavi), leading to right atrium stun and, finally, the presence of drains and cannulas in the chest and the accumulation of fluid in the pericardium and pleura in the earliest postoperative period and the formation of adhesions in the later one. Better MAPSE value is suggested to stem from the better cardioplegia perfusion on the left, better thermal insulation, lack of LA perfusion during surgery, as well as the continuity of the posterior pericardium, lack of tubing in immediate vicinity and non-interference in the structure of the left part of the heart at a slightly later period.
Authors of various studies(14–20,22) agreed that in long-term follow-up (15–20 years) of patients after surgical correction of tetralogy of Fallot with the use of a dilating RVOT patch, together with RV enlargement and decline in its systolic function due to severe pulmonary regurgitation, also gradual deterioration of the LV systolic function develops, which manifests itself in the decreasing parameters of the longitudinal component of the LV contraction (MAPSE). Therefore, monitoring TAPSE dynamics may also be useful in predicting the occurrence of left ventricular dysfunction. It has been assumed that in juveniles and adults the value of TAPSE below 1.5 cm is a bad prognosis(17–19). It seems that this late lowering of the TAPSE value is caused mainly by the insufficiency of the right ventricle secondary to its volume overload. The question arises, however, to what extent reducing the range of the systolic excursion of the tricuspid annulus remains a result of factors present in the immediate postoperative period, in which we did not observe global right ventricle contractile dysfunction (normal values of RV FAC), and whether the dynamics of TAPSE in patients with the tetralogy of Fallot should not be compared with patients after operations of other birth defects which do not cause significant damage to the structures of the right ventricle. Patients after ASD and VSD correction, who, in our study, demonstrated a similar degree of TAPSE reduction in measurements performed immediately after the surgery, could be used as a reference group.
Conclusions
-
1.
In the material presented, a uniform, statistically significant decrease in the value of TAPSE was determined in infants after congenital heart defects correction performed in CPB, with access through the right atrium. The values of TAPSE remained below normal values throughout the follow-up period.
-
2.
There was no simultaneous decrease in the RV FAC value. These results indicate the unsuitability of TAPSE in the assessment of right ventricular systolic function in the early postoperative period and dictate caution in the interpretation of results obtained in a long-term follow-up.
-
3.
The values of MAPSE demonstrated only a slight decrease and remained within the normal range during the follow-up. This proves that the motion of the atrioventricular valve annuli is subject to a different, not yet fully understood influence in the perioperative period. The swift MAPSE normalization allows for the use of this parameter to monitor left ventricular systolic function in the early postoperative period.
Footnotes
Conflict of interest
The authors do not report any financial or personal connections with other persons or organizations that could adversely affect the content of this publication and claim its rights.
References
- 1.Simonson JS, Schiller NB: Descent of the base of the left ventricle: an echocardiographic index of left ventricular function. J Am Soc Echocardiogr 1989; 2: 25–35. [DOI] [PubMed] [Google Scholar]
- 2.Hammarström E, Wranne B, Pinto FJ, Puryear J, Popp RL: Tricuspid annular motion. J Am Soc Echocardiogr 1991; 4: 131–139. [DOI] [PubMed] [Google Scholar]
- 3.Núñez-Gil IJ, Rubio MD, Cartón AJ, López-Romero P, Deiros L, García-Guereta L et al.: Determination of normalized values of the tricuspid annular plane systolic excursion (TAPSE) in 405 Spanish children and adolescents. Rev Esp Cardiol 2011; 64: 674–680. [DOI] [PubMed] [Google Scholar]
- 4.Koestenberger M, Nagel B, Ravekes W, Avian A, Heinzl B, Fritsch P et al. : Left ventricular long-axis function: reference values of the mitral annular plane systolic excursion in 558 healthychildren and calculation of z-score values. Am Heart J 2012; 164: 125–131. [DOI] [PubMed] [Google Scholar]
- 5.Miller D, Farah MG, Liner A, Fox K, Schluchter M, Hoit BD: The relation between quantitative right ventricular ejection fraction and indices of tricuspid annular motion and myocardial performance. J Am Soc Echocardiogr 2004; 17: 443–447. [DOI] [PubMed] [Google Scholar]
- 6.Bazaz R, Edelman K, Gulyasy B, López-Candales A: Evidence of robust coupling of atrioventricular mechanical function of the right side of the heart: insights from M-mode analysis of annular motion. Echocardiography 2008; 25: 557–561. [DOI] [PubMed] [Google Scholar]
- 7.López-Candales A, Rajagopalan N, Gulyasy B, Edelman K, Bazaz R: Comparative echocardiographic analysis of mitral and tricuspid annular motion: differences explained with proposed anatomic-structural correlates. Echocardiography 2007; 24: 353–359. [DOI] [PubMed] [Google Scholar]
- 8.Cruz-Lemini M, Crispi F, Valenzuela-Alcaraz B, Figueras F, Sitges M, Gómez O et al.: Value of annular M-mode displacement vs tissue Doppler velocities to assess cardiac function in intrauterine growth restriction. Ultrasound Obstet Gynecol 2013; 42: 175–181. [DOI] [PubMed] [Google Scholar]
- 9.Winter MM, Bouma BJ, Hardziyenka M, De Bruin-Bon RH, Tan HL, Konings TC et al.: Echocardiographic determinants of the clinical condition in patients with a systemic right ventricle. Echocardiography 2010; 27: 1247–1255. [DOI] [PubMed] [Google Scholar]
- 10.Giovanardi P, Tincani E, Rossi R, Agnoletto V, Bondi M, Modena MG: Right ventricular function predicts cardiovascular events in outpatients with stable cardiovascular diseases: preliminary results. Intern Emerg Med 2012; 7: 251–256. [DOI] [PubMed] [Google Scholar]
- 11.Messing B, Gilboa Y, Lipschuetz M, Valsky DV, Cohen SM, Yagel S: Fetal tricuspid annular plane systolic excursion (f-TAPSE): evaluation of fetal right heart systolic function with conventional M-mode ultrasound and spatiotemporal image correlation (STIC) M-mode. Ultrasound Obstet Gynecol 2013; 42: 182–188. [DOI] [PubMed] [Google Scholar]
- 12.Ghio S, Recusani F, Klersy C, Sebastiani R, Laudisa M, Campana C et al.: Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am J Cardiol 2000; 85: 837–842. [DOI] [PubMed] [Google Scholar]
- 13.Lee CY, Chang SM, Hsiao SH, Tseng JC, Lin SK, Liu CP: Right heart function and scleroderma: insights from tricuspid annular pane systolic excursion. Echocardiography 2007; 24: 118–125. [DOI] [PubMed] [Google Scholar]
- 14.Vliegen HW, van Straten A, de Roos A, Roest AA, Schoof PH, Zwinderman AH et al.: Magnetic resonance imaging to assess the hemodynamic effects of pulmonary valve replacement in adults late after repair of tetralogy of fallot. Circulation 2002; 106: 1703–1707. [DOI] [PubMed] [Google Scholar]
- 15.Kempny A, Diller GP, Orwat S, Kaleschke G, Kerckhoff G, Bunck AC et al.: Right ventricular-left ventricular interaction in adults with Tetralogy of Fallot: a combined cardiac magnetic resonance and echocardiographic speckle tracking study. Int J Cardiol 2012; 154: 259–264. [DOI] [PubMed] [Google Scholar]
- 16.Morcos P, Vick GW, Sahn DJ, Jerosch-Herold M, Shurman A, Sheehan FH: Correlation of right ventricular ejection fraction and tricuspid annular plane systolic excursion in tetralogy of Fallot by magnetic resonance imaging. Int J Cardiovasc Imaging 2009; 25: 263–270. [DOI] [PubMed] [Google Scholar]
- 17.Koestenberger M, Nagel B, Ravekes W, Everett AD, Stueger HP, Heinzl B et al.: Systolic right ventricular function in pediatric and adolescent patients with tetralogy of Fallot: Echocardiography versus magnetic resonance imaging. J Am Soc Echocardiogr 2011; 24: 45–52. [DOI] [PubMed] [Google Scholar]
- 18.Koestenberger M, Ravekes W, Everett AD, Stueger HP, Heinzl B, Gamillscheg A et al.: Right ventricular function in infants, children and adolescents: reference values of the tricuspid annular plane systolic excursion (TAPSE) in 640 healthy patients and calculation of z-score values. Jam Soc Echocardiogr 2009; 22: 715–719. [DOI] [PubMed] [Google Scholar]
- 19.Koestenberger M, Ravekes W, Nagel B, Avian A, Heinzl B, Fritsch P et al. : Longitudinal systolic ventricular interaction in pediatric and young adult patients with TOF: A cardiac magnetic resonance and M-mode echocardiographic study. Int J Cardiovasc Imaging 2013; 29: 1707–1715. [DOI] [PubMed] [Google Scholar]
- 20.Bonnemains L, Stos B, Vaugrenard T, Marie PY, Odille F, Boudjemline Y: Echocardiographic right ventricle longitudinal contraction indices cannot predict ejection fraction in post-operative Fallot children. Eur Heart J Cardiovasc Imaging 2012; 13: 235–242. [DOI] [PubMed] [Google Scholar]
- 21.Wranne B, Pinto FJ, Hammarström E, St Goar F, Puryear J, Popp RL: Abnormal right heart filling after cardiac surgery: time course and mechanisms. Br Heart J 1991; 66: 435–442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ghai A, Silversides C, Harris L, Webb GD, Siu SC, Therrien J: Left ventricular dysfunction is a risk factor for sudden cardiac death in adults late after repair of tetralogy of Fallot. J Am Coll Cardiol 2002; 40: 1675–1680. [DOI] [PubMed] [Google Scholar]