

Abstract
Background
Vivax malaria reemerged in the Korean peninsula in 1990s beginning from the western border area and spread across both Koreas rapidly with its peak incidences reported on the early 2000s. There have been few reports on the malaria incidence in the Democratic People's Republic of Korea (North Korea) that provides detailed epidemiological features. The purpose of this study was to describe the time trends and spatial distribution of malaria in North Korea with comparison to those in South Korean regions across the border.
Methods
The incidence of malaria in each province of North Korea from 2004 to 2016 was estimated based on data from domestic and international health authorities. Consistency of the data was evaluated by calculating the ratio of malaria cases in each province to the total cases each year. We also compared the changes in malaria incidence over time in South and North Korea adjacent to the demilitarized zone.
Results
In North Korea, the incidence of malaria in the three provinces adjacent to the demilitarized zone was the highest (52.1−315.3 per 100,000), followed by Pyeonganbuk-do (14.7−113.5 per 100,000), where railways and road networks were connected to northern China. The incidence of malaria in each province of North Korea reported after 2011 was more consistent than when compared with previous annual data, and there was also a positive correlation between changes in incidence over time when compared with malaria incidence in South Korea (r = 0.855, r = 0.596).
Conclusion
The malaria report of North Korea was relatively consistent in its spatiotemporal tendency since 2011, suggesting improvement of the quality of the surveillance data. The strong correlation between North and South Korean malaria incidence at regional level suggests that collaboration between both sides are essential for the successful elimination of malaria in the Korean peninsula.
Keywords: Vivax Malaria, North Korea, South Korea, Demilitarized Zone, Cross-Border Transmission
Graphical Abstract
INTRODUCTION
Vivax malaria had been an indigenous disease in the Korean peninsula, with a first record appearing during the Goryeo Dynasty (918–1,392 CE).1 In the 1910s, malaria was widespread from the southern coast of Gyeongsangnam-do to the northernmost Hamgyeongbuk-do.2,3 In the 1930s, during the Japanese colonial period, the annual number of malaria cases reached almost 150,000 nationwide; malaria was an endemic disease occurring anywhere across the country.4 Although it had been declining for a while, malaria spread to all regions of the Korean peninsula after the Korean War.5 It disappeared in the 1980s by the efforts from the World Health Organization (WHO) and both the Korean government in parallel with environmental changes from rapid economic development in the 1960s and 1970s.6,7,8,9
Since the re-emergence of malaria in the northern part of the Republic of Korea (South Korea)'s northern Gyeonggi-do in July 1993, the epidemic has expanded.10 Malaria peaked in South Korea at approximately 4,100 in 2000 and now is reported approximately 600 cases each year.11 In Democratic People’s Republic of Korea (North Korea), malaria had been eradicated in the 1970s; however, it reemerged in 1997 and has been reported to be continuously prevalent, with a high incidence in regions adjacent to the demilitarized zone (DMZ).12 The malaria epidemic in North Korea has steadily been declining since it peaked with approximately 300,000 cases in 2001 (Fig. 1).13 In the early days of the malaria resurgence in North Korea, the rates of confirmation through laboratory tests were low, and infection cases in the military camps were missing from statistics.13,14 For this reason, the point has been raised that the exact size of the malaria epidemic in North Korea could have been underestimated.14
Fig. 1. Maps in the border region of South Korea and North Korea.

In North Korea, the national incidence of malaria was reported to the WHO annually; however, malaria incidence at the regional level was not publicly available. Thus, malaria incidence at the regional level in North Korea has been released in a fragmental way through cooperation meetings or has been obtained from reference tables in strategic reports. Based on these data, it was estimated that malaria in North Korea has been reported throughout the country, with low incidence of malaria having been reported in the three northern provinces of Jagang-do, Ryanggang-do, and Hamgyeongbuk-do; most cases have been reported in Gangwon-do, Hwanghaebuk-do, and Hwanghaenam-do, which are adjacent to the DMZ between South and North Korea.15 Previous epidemiological reports strongly suggest that Plasmodium vivax malaria in South Korea has been closely associated with malaria in the neighboring regions of North Korea; thus, the incidence of malaria in the North Korean provinces adjacent to the DMZ is essential to understand the malaria situation in both Koreas.16,17
This study aimed to describe and evaluate the spatial distribution of malaria incidence and its time trend over time in North Korea, based on the data of the malaria status at provincial level based on the data from domestic and international health authorities.
METHODS
Data sources: malaria incidence in the North Korea
The number of reported malaria and microscopy examined data in North Korea from 1998 to 2016, was obtained from the WHO's annual World Malaria Report. Data on the cases of malaria in each province in North Korea have been scarce in previous literature. The data used in the study were obtained from WHO documents, the documents on the report of an international malaria conference prepared by the Korea Centers for Disease Control and Prevention (KCDC), the press release from KCDC, and articles of newspaper on the malaria situation in North Korea. The data for 2004 were obtained from the KCDC's press release dated on February 11, 2005, which is kept in the National Assembly Library.18 Data from 2005 to 2008 were obtained in the report on the “Technical Consultative Meeting on Malaria in South and North Korea and Related Countries,” held in India from April 21–26, 2009.19 The data for 2009 were derived from a newspaper article that reported on the “2009 malaria control activity in North Korea by the WHO”.20 Data from 2011 to 2016 were obtained from the review report for malaria control in North Korea, located on the WHO South East Asia Regional Office (SEARO) website.21 Among the data from 2004 to 2016, the data for 2010 were not available. Given that population data in North Korea have not been recorded since the 2008 population census, the population by the province in 2008 was applied to calculate the annual incidence for each year.22 The incidence of malaria per 100,000 population in North Korea was calculated for the Hwanghaenam-do, Hwanghaebuk-do, and Gangwon-do adjacent to the DMZ for comparison with the basic local governments of South Korea in the southern region of the DMZ (Fig. 1).
Data sources: malaria incidence in the South Korea
Malaria cases for each local government in South Korea were obtained from the Infectious Disease Portal, operated by the KCDC.23 In South Korea, malaria is designated as a Group 3 notifiable infectious disease, and the malaria statistic was based on epidemiological data, which reflects the actual number of malaria cases. Population data by region for each year in South Korea were used for annual population statistics based on resident registration. The incidence of malaria per 100,000 population in South Korean localities adjacent to the DMZ was calculated as the average incidence in three regions (Gimpo-si, Paju-si, Yeoncheon-gun) of Gyeonggi-do, five regions (Cheorwon-gun, Hwacheon-gun, Yanggu-gun, Inje-gun, Goseong-gun) of Gangwon-do, and Ganghwa-gun of Incheon Metropolitan City (Fig. 1).
Data analysis
Data from 1998 to 2016 were reviewed to identify the relationship between the number of reported malaria cases versus the number of cases undergoing the microscopic exam. From the total malaria cases in North Korea from 2004 to 2016, the proportion of malaria cases in each province was calculated. The incidence of malaria in South and North Korea in the regions adjacent to each other in the DMZ was calculated and compared. Because the large-scale international support for North Korean malaria control has been supported by the Global Fund to Fight AIDS, tuberculosis, and malaria (the Global Fund) since 2010, we evaluated the correlations with incidence data of South Korea in order to conduct the qualitative assessment of the North Korean's incidence data before and after the year of 2010.24
RESULTS
According to reports from the North Korean authorities, malaria was reemerged in 1998 in North Korea and peaked with about 300,000 cases in 2001. Since then, the number has been on a steady decline with a report of 5,113 cases in 2016 (Fig. 2). The number of reported cases from 2001 to 2003 was 186%-209% of the cases in whom microscopic examinations were conducted (Supplementary Table 1). It reached 100% in 2006. After that, the number of cases undergoing microscopic examinations increased gradually. From 2013 to 2016, the above ratio is in the 20% range.
Fig. 2. Status of malaria data in North Korea, 1998–2016.

The distribution of malaria cases in each province of North Korea from 2004 to 2008, the number of cases in Hwanghaebuk-do accounted for 22.0%, 50.8%, 16.0%, 19.5%, and 23.5%, respectively, of total cases and showed inconsistent distribution (Table 1). During the same period, Hwanghaenam-do and Gangwon-do, which are adjacent to the DMZ, also showed jagged distribution. Pyeongannam-do, which is adjacent to Pyongyang, the capital of North Korea, accounted for 18.0% of total malaria cases in 2004 but fell sharply to 6.8% in 2005. In the following year, however, it increased sharply to 18.2%, and further to 20.2% in 2007, then sharply decreased in 2008 to 9.7%. The proportion of malaria cases in the three provinces adjacent to the DMZ from 2004 to 2008 was reported as 45.9–78.2%, showing a significant difference in each year, whereas the proportion of malaria cases from 2011 to 2016 was 23.2%–25.6% in Hwanghaenam-do, 22.0%–29.1% in Hwanghaebuk-do province, and 15.1%–23.7% in Gangwon-do. The proportion of malaria in these three provinces from 2011 to 2016 was 64.3%–72.4%, narrowing the range of variability compared with 2004–2008.
Table 1. Numbers of malaria cases in the province of North Korea, 2004–2016.
| Year | Hwanghaenam-do | Hwanghaebuk-do | Gangwon-do | Pyeongannam-do | Pyeonganbuk-do | Pyongyang | Ryanggang-do | Jagang-do | Hamgyeongnam-do | Hamgyeongbuk-do | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2004 | 5,605 (16.6) | 7,415 (22.0) | 4,154 (12.3) | 6,064 (18.0) | 5,949 (17.7) | 1,041 (3.1) | 8 (0.0) | 51 (0.2) | 2,140 (6.4) | 1,250 (3.7) | 33,677 |
| 2005 | 1,906 (16.6) | 5,844 (50.8) | 1,244 (10.8) | 781 (6.8) | 747 (6.5) | 135 (1.2) | 3 (0.0) | 25 (0.2) | 574 (5.0) | 248 (2.2) | 11,507 |
| 2006 | 2,303 (24.6) | 1,498 (16.0) | 1,925 (20.6) | 1,703 (18.2) | 1,439 (15.4) | 105 (1.1) | 7 (0.1) | 18 (0.2) | 267 (2.9) | 88 (0.9) | 9,353 |
| 2007 | 814 (10.9) | 1,453 (19.5) | 1,143 (15.4) | 1,500 (20.2) | 1,803 (24.2) | 253 (3.4) | 5 (0.1) | 73 (1.0) | 273 (3.7) | 119 (1.6) | 7,436 |
| 2008 | 5,120 (21.9) | 5,493 (23.5) | 3,720 (15.9) | 2,282 (9.7) | 3,458 (14.8) | 533 (2.3) | 67 (0.3) | 193 (0.8) | 1,101 (4.7) | 338 (1.4) | 23,409 |
| 2009 | 4,123 (22.1) | 4,069 (21.8) | 3,557 (19.0) | - | - | - | - | - | - | - | 18,679 |
| 2010 | - | - | - | - | - | - | - | - | - | - | 15,392 |
| 2011 | 4,283 (24.4) | 4,327 (24.7) | 2,651 (15.1) | 1,556 (8.9) | 2,694 (15.4) | 527 (3.0) | - | - | 716 (4.1) | - | 17,518 |
| 2012 | 5,584 (24.4) | 6,665 (29.1) | 3,539 (15.4) | 1,852 (8.1) | 3,098 (13.5) | 575 (2.5) | - | - | 792 (3.5) | - | 22,918 |
| 2013 | 3,911 (25.6) | 3,363 (22.0) | 3,059 (20.0) | 1,249 (8.2) | 2,043 (13.4) | 525 (3.4) | - | - | 566 (3.7) | - | 15,259 |
| 2014 | 2,711 (24.7) | 2,461 (22.4) | 2,249 (20.5) | 897 (8.2) | 1,387 (12.6) | 431 (3.9) | - | - | 469 (4.3) | - | 10,970 |
| 2015 | 1,674 (23.2) | 1,871 (26.0) | 1,581 (21.9) | 609 (8.5) | 542 (7.5) | 379 (5.3) | - | - | 359 (5.0) | - | 7,204 |
| 2016 | 1,204 (23.8) | 1,255 (24.8) | 1,200 (23.7) | 389 (7.7) | 402 (8.0) | 228 (4.5) | 9 (0.2) | 1 (0.0) | 236 (4.7) | 49 (1.0) | 5,054 |
Data are presented as number (%).
Two provinces, Hwanghaebuk-do and Hwanghaenam-do, located in the western region of the North Korean DMZ, showed a strong correlation with malaria incidence from 2004 to 2016 (r = 0.81) (Supplementary Fig. 1). However, it was significantly different from the incidence of malaria in South Korea (3 counties of Gyeonggi-do and Ganghwa-gun of Incheon metropolitan city), which is facing Hwanghaebuk-do and Hwanghaenam-do across the western region of the DMZ (Fig. 3). The incidence of malaria in Hwanghaenam-do of North Korea and Ganghwa-gun of South Korea near the western region of the DMZ showed a strong negative correlation (r = −0.872) between 2004 and 2009, but there was a strong positive correlation (r = 0.855) in the period from 2011 to 2016. Similarly, the incidence of malaria in Hwanghaebuk-do of North Korea and Gyeonggi-do of South Korea near the central region of the DMZ showed a strong negative correlation (r = −0.826) between 2004 and 2009, but in the period between 2011 and 2016, there was a positive correlation (r = 0.596). Gangwon-do of North Korea and Gangwon-do of South Korea, located north and south of the eastern region of the DMZ facing each other, had no correlation with malaria incidence from 2004 to 2009, as well as from 2011 to 2016 (r = 0.064, r = 0.079).
Fig. 3. Correlation of malaria incidence in the border region of South and North Korea, 2004–2016. Data of Gyeonggi-do is the average malaria incidence per 100,000 in Gimpo, Paju, and Yeoncheon regions. Data of Gangwon-do (South Korea) is the average malaria incidence per 100,000 in Cheorwon, Hwacheon, Yanggu, Inje, and Goseong regions.

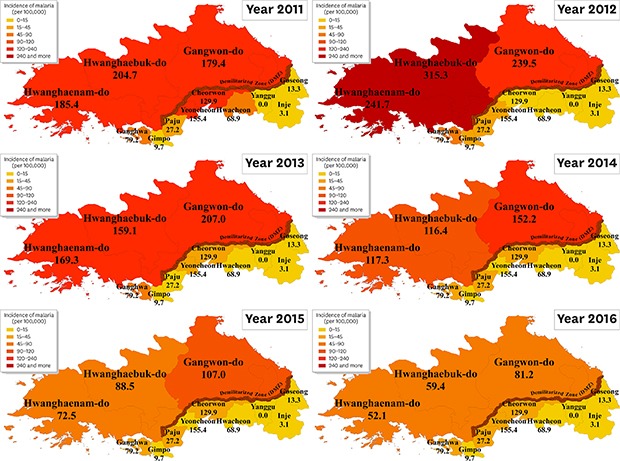
The incidence of malaria in each North Korean province in 2011 was higher than 15 per 100,000 persons in all provinces except for Jagang-do, Ryanggang-do, and Hamgyeongbuk-do (Fig. 4). In particular, the incidence of malaria in the three provinces adjacent to the DMZ was high, reaching over 150 persons per 100,000. Although the incidence of malaria per 100,000 persons in North Korea is declining, the incidence of malaria in these three provinces adjacent to the DMZ was still high in 2016, exceeding 50 persons per 100,000. Excluding provinces adjacent to the DMZ, Pyeonganbuk-do, which is bordered by China and is connected by roads and railways, has consistently had fourth-highest incidence of malaria. Northern three regions (Jagang-do, Ryanggang-do, and Hamgyeongbuk-do) of North Korea bordered by the Jilin province in Northern China had less than 5% of total malaria cases each year, making them the lowest incidence of malaria in North Korea.
Fig. 4. Malaria incidence in province of North Korea and adjacent to the DMZ, 2011–2016.

DISCUSSION
The incidences of malaria in the regions of South and North Korea, which face each other across the DMZ, have been very different in the past in terms of the scale of infected cases. After the re-emergence of malaria in South Korea in 1993, North Korea experienced what is termed the “Arduous March” due to a series of disasters and famine in the mid-1990s.25,26 North Korea reported reemergence of malaria in 1998, which soon exploded, with an estimated 300,000 cases in 2001. Mass primaquine preventive treatment, which began in 2002 with the aid of the international community, has contributed to reducing the incidence of malaria in North Korea; and the support of the Global Fund, which began in 2010, has enabled stable financial support for malaria control.13 From 2008 to 2011, South Korea's provincial government (Gyeonggi-do) and the North Korean authorities have implemented a joint malaria control project in North Korea's Kaesong region as a part of activities to control high malaria incidence in areas near the DMZ. However, the joint malaria control project in South and North Korea lasted for only four years and was stopped due to the deterioration of South and North Korean relations, which did not prove its effectiveness.27,28
For the malaria surveillance system to function properly, the number of microscopic examinations must exceed the number of confirmed cases. However, until 2006, many cases were diagnosed clinically without being confirmed by microscopic examination in North Korea. From 2007, the number of microscopic examinations has exceeded the number reported, and from 2013, about 20%–30% of the microscopic examinations were confirmed as malaria. To ensure the credibility of national statistical data, the sum of cases collected from each province should be similar to the statistics of the central government. However, there were more than 1,000 differences in North Korea according to the data sources before 2011.
The percentage of malaria cases in each province among North Korea's total malaria cases has fluctuated significantly every year until 2009; however, there has been a tendency for those fluctuations to be reduced and stabilized since 2011. The Hwanghaebuk-do accounted for 22.0% of total cases in 2004, but it accounted for approximately half (50.8%) of total cases in 2005, then dropped to 16.0% in the next year. Hwanghaenam-do accounted for 16.6% of total cases in 2005, up sharply from 24.6% in 2006, and down more than 10% the following year to 10.9% in 2007. The reason malaria surveillance data for each province reported before 2010 fluctuates significantly from one year to the next, and why the stability in terms of the data is greatly reduced, is related to the collapse of the overall health care system in North Korea.29,30,31 This phenomenon appears to be related to the effects of famine and natural disasters that persisted from the 1990s to the early 2000s.32,33 As an example that reflects this fact well, national immunization coverage in North Korea had been steadily increasing since the 1980s, with vaccination coverage reaching 98% in 1990. However, in the course of famine and natural disasters, the health care system collapsed and vaccination coverage fell sharply. The collapsed health care system has gradually been restored with the support of international aid. Diphtheria-tetanus-pertussis (DTP3) immunization coverage, which had reached 98% in 1990, dropped to less than 40% in 1998 due to this collapse.29 DTP3 immunization coverage has since recovered to 90% in 2007, and other immunization coverage has also reached over 90% by 2007–2008 as the health care system has been rebuilt with the support of the international community and the North Korean government.34 The process of collapse and recovery of these health care systems has been reflected in the stability of the infectious disease surveillance system. In particular, since 2011, when the Global Fund was implemented, supplying solar panels to power computer network systems and replenish scarce energy resources, malaria incidence data in all provinces have become more stabilized.
The impact of the collapse and recovery of the socioeconomic system in North Korea mentioned above is also confirmed in the comparison of the malaria incidence in the South and North Korea regions adjacent to the DMZ. The incidence of malaria in Hwanghaenam-do and Ganghwa-gun areas in the western part of the DMZ showed a strong negative correlation from 2004 to 2009. However, there was a strong positive correlation in malaria incidence from 2011 to 2016. Because the two areas are adjacent to each other across the DMZ, which is 4 km wide, a high positive correlation between the incidence of malaria in North and South Korea in the western part of the DMZ suggests that malaria vectors and protozoa are circulating in that region. However, it is difficult to explain the difference in trends between these two regions only by differences in weather factors or mosquito vector density. Even in areas adjacent to the DMZ, it was difficult to directly compare the incidence of malaria due to differences in economic levels and differences in the capabilities of the health care systems between South and North Korea. South Korea has a national health insurance system and malaria cases are reported as a legal infectious disease. For this reason, it is difficult to miss out the malaria case in the surveillance system. On the other hand, when the North Korean health care system had not yet fully recovered from the economic crisis, it is possible that the malaria reporting system in North Korea did not function properly. These geographical and socio-economic characteristics are also similar in Hwanghaebuk-do and Northern Gyeonggi-do areas, which are adjacent to each other in the central part of the DMZ. Located in the eastern part of the DMZ, South Korea's Gangwon-do and North Korea's Gangwon-do have consistently failed to show a clear correlation from 2004 to 2016. In North Korea, Gangwon-do is known to be inaccessible due to mountainous terrain. Therefore, this accessibility issue may be the cause of malaria incidence reporting system being difficult to operate normally.
Based on the results of these analyses, it can be confirmed that the reported malaria data at the regional level in North Korea since 2011, improved more objectively than the data of the previous year in reliability and validity. In North Korea's province data from 2011 to 2016, the three provinces close to the DMZ have consistently shown the highest malaria incidence. Meanwhile, the Pyeonganbuk-do, adjacent to Liaoning Provence in northeastern China, marks the fourth-highest incidence of malaria in North Korea. This is the highest incidence, except for the three provinces near the DMZ. Given that Pyeonganbuk-do is approximately 300 km away from the DMZ, it is not affected much by malaria high-risk areas. Rather, it could have been affected by the influx of malaria from outside the country because it is a logistics hub that connects China with roads and railways and is frequented by people crossing the border.
The malaria data from 2004 to 2009 presented in this study are limited in that they are not official statistics of the North Korean authorities. It also has limitations in that it is not possible to assess the actual reporting rate for malaria incidence in each province. However, since the data for each province from 2011 to 2016 are included in the report submitted to WHO, the reliability of the data can be expected. Considering the number of microscopic examination exceeding the reported cases, the consistency of the number of malaria cases in different data sources, and the correlation of malaria incidence between the South-North Korea regions adjacent to the DMZ, North Korea's regional data since 2011 show that reliability and validity than previous data. In addition to excluding the assessment of the reporting rate of malaria cases in North Korea, it is meaningful that the malaria cases for each province and each year are evaluated in terms of data stability and regional trend.
The incidence of malaria in North Korea is high in the southern region closer to the DMZ, malaria cases in South Korea occur only in the region adjacent to the DMZ. Because the DMZ is only 4 kilometers wide and actual distance is much less in most of the areas, Anopheles sinensis, a major mosquito species associated with malaria infection on the Korean Peninsula, is known to be able to fly across the DMZ during its life cycle.35 Until now, only annual data of malaria surveillance in North Korea have officially been released, making it difficult to develop strategies for controlling malaria on the Korean peninsula, especially in the border regions near the DMZ. As observed from other successful international cases, malaria issues occurring across the border between countries can be solved only by active cooperation between the neighboring countries. Malaria incidence data by the province of North Korea since 2010, after Global Fund support began, show a more consistent regional distribution when compared with the previous annual data, and correlate with the province data of neighboring South Korea. The securement of stability and the increase in the reliability of malaria surveillance data produced by the North Korean authorities are good sources for understanding the epidemiological characteristics of malaria in North Korea. These data can be a valuable resource for conducting malaria eradication projects in the border region of the DMZ.
In conclusion, the malaria report of North Korea was relatively consistent in its spatiotemporal tendency since 2011, suggesting improvement of the quality of the surveillance data. The strong correlation between North and South Korean malaria incidence at regional level suggests that collaboration between both sides are essential for the successful elimination of malaria in the Korean peninsula.
Footnotes
Funding: This study was supported by the Government-wide R&D Fund project for infectious disease research (HG18C0025), Republic of Korea.
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Kim JH.
- Data curation: Lim AY, Kim JH.
- Formal analysis: Lim AY, Kim JH.
- Methodology: Kim JH, Cheong HK.
- Writing - original draft: Kim JH.
- Writing - review & editing: Kim JH, Cheong HK.
SUPPLEMENTARY MATERIALS
Qualitative status of malaria data in North Korea through the World Malaria Report and province data, 1998–2016
Comparison of malaria incidence in the border region of South Korea and North Korea, 2004–2016.
References
- 1.Shin DH, Seo M, Hong JH, Lee E. Paleopathological considerations on malaria infection in Korea before the 20th century. BioMed Res Int. 2018;2018:8516785. doi: 10.1155/2018/8516785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hasegawa Y. Malaria in Korea. J Chosun Med Soc. 1913;4(4):53–69. [Google Scholar]
- 3.Himeno K. Malaria occurring at Kangnung area, Kangwon-do. Mansen no Ikai. 1926;62(62):59–66. [Google Scholar]
- 4.Yeo I. A history of malaria in modern Korea 1876–1945. Korean J Med Hist. 2011;20(1):53–82. [PubMed] [Google Scholar]
- 5.Ree HI. Unstable vivax malaria in Korea. Korean J Parasitol. 2000;38(3):119–138. doi: 10.3347/kjp.2000.38.3.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.National Malaria Eradication Service, Ministry of Health and Social Affairs. Malaria Pre-eradication Programme in Korea, 1961–1965 Progress Report. Seoul: Ministry of Health and Social Affairs; 1966. pp. 44–75. [Google Scholar]
- 7.Paik YH, Tsai FC. A note on the epidemiology of Korean vivax malaria. New Med J. 1963;6(2):37–43. [Google Scholar]
- 8.World Health Organization. Synopsis of the world malaria situation, 1979. Wkly Epidemiol Rec. 1981;56(19):145–149. [Google Scholar]
- 9.Paik YH, Ree HI, Shim JC. Malaria in Korea. Jpn J Exp Med. 1988;58(2):55–66. [PubMed] [Google Scholar]
- 10.Cho SY, Kong Y, Park SM, Lee JS, Lim YA, Chae SL, et al. Two vivax malaria cases detected in Korea. Korean J Parasitol. 1994;32(4):281–284. doi: 10.3347/kjp.1994.32.4.281. [DOI] [PubMed] [Google Scholar]
- 11.The Korea Centers for Disease Control and Prevention. Infectious Diseases Surveillance Yearbook 2017. Cheongju: The Korea Centers for Disease Control and Prevention; 2018. [Google Scholar]
- 12.Chol PT, Suwannapong N, Howteerakul N. Evaluation of a malaria control project in DPR Korea, 2001–2003. Southeast Asian J Trop Med Public Health. 2005;36(3):565–571. [PubMed] [Google Scholar]
- 13.Pant SD, Chol KY, Tegegn Y, Mandal PP, Chol RK. Mass primaquine preventive treatment for control of Plasmodium vivax malaria in the Democratic People's Republic of Korea: a country success story. WHO South-East Asia J Public Health. 2014;3(1):75–80. doi: 10.4103/2224-3151.206889. [DOI] [PubMed] [Google Scholar]
- 14.Mercado CE, Ekapirat N, Dondorp AM, Maude RJ. An assessment of national surveillance systems for malaria elimination in the Asia Pacific. Malar J. 2017;16(1):127. doi: 10.1186/s12936-017-1774-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.National Malaria Programme, Ministry of Public Health. National Malaria Elimination Strategy 2018–2022: Democratic People's Republic of Korea. Pyongyang: World Health Organization, Country Office for DPR Korea; 2017. [Google Scholar]
- 16.Ree HI. Can malaria be endemic in South Korea? Korean J Infect Dis. 1998;30(4):397–400. [Google Scholar]
- 17.Lee JS, Lee WJ, Cho SH, Ree HI. Outbreak of vivax malaria in areas adjacent to the demilitarized zone, South Korea, 1998. Am J Trop Med Hyg. 2002;66(1):13–17. doi: 10.4269/ajtmh.2002.66.13. [DOI] [PubMed] [Google Scholar]
- 18.The Korea Centers for Disease Control and Prevention. The government's report on malaria infection in North Korea [Internet] [Accessed March 15, 2019]. http://dl.nanet.go.kr/SearchDetailView.do?cn=NONB1200638195_1.
- 19.Division of Infectious Disease Control, The Korea Centers for Disease Control and Prevention. Report on the participation of the technical consultative meeting on malaria in South and North Korea and related countries, 2009 [Internet] [Accessed March 15, 2019]. https://btis.mpm.go.kr/cmm/main/mainPage.do, Report number=51352.
- 20.Voice of America. WHO says the number of malaria patients in North Korea is about 18,000 in 2009 [Internet] [Accessed March 15, 2019]. https://www.voakorea.com/a/malaria-north-korea-91917899/1333560.html.
- 21.Ejov M, Gunasekar A, Hii J. External malaria programme review: DPR Korea [Internet] [Accessed March 15, 2019]. http://www.searo.who.int/dprkorea/documents/dprk-malaria-propgramme/en/
- 22.Central Bureau of Statistics. DPR Korea 2008 Population Census National Report. Pyongyang: Central Bureau of Statistics; 2009. [Google Scholar]
- 23.The Korea Centers for Disease Control and Prevention. Infectious disease portal [Internet] [Accessed April 04, 2019]. http://www.cdc.go.kr/npt/biz/npp/nppMain.do.
- 24.Burki T. North Korea and the global fund. Lancet Infect Dis. 2018;18(5):501. doi: 10.1016/S1473-3099(18)30238-X. [DOI] [PubMed] [Google Scholar]
- 25.Bhatia R, Thorne-Lyman AL. Food shortages and nutrition in North Korea. Lancet. 2002;360(Suppl):s27–8. doi: 10.1016/s0140-6736(02)11809-5. [DOI] [PubMed] [Google Scholar]
- 26.Grundy J, Moodie R. An approach to health system strengthening in the Democratic Peoples Republic of Korea (North Korea) Int J Health Plann Manage. 2009;24(2):113–129. doi: 10.1002/hpm.958. [DOI] [PubMed] [Google Scholar]
- 27.Gyeonggi Research Institute. Gyeonggi Policy Research 2016-52. Inter-Korean Cooperation and Gyeonggi-Do. Suwon: Gyeonggi Research Institute; 2016. pp. 1–170. [Google Scholar]
- 28.Hwang JS. Malaria control project in the DPRK [Internet] [Accessed August 02, 2019]. https://vtncankor.files.wordpress.com/2011/09/malaria-control-project-in-the-dprk.pdf.
- 29.Schwekendiek D. Regional variations in living conditions during the North Korean food crisis of the 1990s. Asia Pac J Public Health. 2010;22(4):460–476. doi: 10.1177/1010539509337253. [DOI] [PubMed] [Google Scholar]
- 30.McCurry J. Aid workers warn of North Korea's forgotten health crisis. Lancet. 2005;365(9476):1997–1998. doi: 10.1016/S0140-6736(05)66680-9. [DOI] [PubMed] [Google Scholar]
- 31.Grundy J, Biggs BA, Hipgrave DB. Public health and international partnerships in the Democratic People's Republic of Korea. PLoS Med. 2015;12(12):e1001929. doi: 10.1371/journal.pmed.1001929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Owen-Davies J. North Korea's public health tragedy. Lancet. 2001;357(9256):628–630. doi: 10.1016/S0140-6736(00)04062-9. [DOI] [PubMed] [Google Scholar]
- 33.Centers for Disease Control and Prevention (CDC) Status of public health--Democratic People's Republic of Korea, April 1997. MMWR Morb Mortal Wkly Rep. 1997;46(24):561–565. [PubMed] [Google Scholar]
- 34.Ahmad K. Explosion in North Korea destroys health facilities. Lancet. 2004;363(9419):1447. doi: 10.1016/S0140-6736(04)16138-2. [DOI] [PubMed] [Google Scholar]
- 35.Cho SH, Lee HW, Shin EH, Lee HI, Lee WG, Kim CH, et al. A mark-release-recapture experiment with Anopheles sinensis in the northern part of Gyeonggi-do, Korea. Korean J Parasitol. 2002;40(3):139–148. doi: 10.3347/kjp.2002.40.3.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Qualitative status of malaria data in North Korea through the World Malaria Report and province data, 1998–2016
Comparison of malaria incidence in the border region of South Korea and North Korea, 2004–2016.