

Abstract
Background
Although coffee consumption is often reported as a trigger for atrial fibrillation (AF) among patients with paroxysmal AF, prospective studies on the relation of coffee consumption with AF risk have been inconsistent. Hence, we sought to assess the association between coffee consumption and risk of AF in men.
Methods and Results
We prospectively studied men who participated in the Physicians’ Health Study (N=18 960). Coffee consumption was assessed through self‐reported food frequency questionnaires. The incidence of AF was assessed through annual questionnaires and validated through review of medical records in a subsample. Cox proportional hazard models were used to calculate hazard ratios and 95% CIs of AF. The average age was 66.1 years. A total of 2098 new cases of AF occurred during a mean follow‐up of 9 years. Hazard ratios (95% CI) of AF were 1.0 (reference), 0.85 (0.71‐1.02), 1.07 (0.88‐1.30), 0.93 (0.74‐1.17), 0.85 (0.74‐0.98), 0.86 (0.76‐0.97), and 0.96 (0.80‐1.14) for coffee consumption of rarely/never, ≤1 cup/week, 2 to 4 cups/week, 5 to 6 cups/week, 1 cup/day, 2 to 3 cups/day, and 4+ cups/day, respectively; adjusting for age, smoking, alcohol intake, and exercise (P for nonlinear trend=0.01). In a secondary analysis the multivariable adjusted hazard ratio (95% CI) of AF per standard deviation (149‐mg) change in caffeine intake was 0.97 (0.92‐1.02).
Conclusions
Our data suggest a lower risk of AF among men who reported coffee consumption of 1 to 3 cups/day.
Keywords: atrial fibrillation, caffeine, cardiovascular disease, coffee, epidemiology and Nutrition
Subject Categories: Cardiovascular Disease, Diet and Nutrition, Epidemiology, Lifestyle, Primary Prevention
Short abstract
See Editorial Aleong and Sandhu
Clinical Perspective
What Is New?
In this prospective long‐term cohort study, we found a lower risk of atrial fibrillation among men drinking 1 to 3 cups of coffee per day in the Physicians’ Health Study (N=18 960, mean follow‐up 9 years).
However, we did not find any significant association between caffeine intake and atrial fibrillation risk in Physicians’ Health Study participants.
What Are the Clinical Implications?
Our findings will guide physicians making recommendations on coffee intake, one of the most consumed beverages in the world, and its long‐term effect on atrial fibrillation risk, one of the most common types of arrythmia.
Atrial fibrillation (AF) is one of the most common types of serious arrhythmias, and its incidence has increased significantly during the past few years.1 According to the Centers for Disease Control and Prevention, ≈2% of people younger than 65 years, and 9% of people older than 65 years, are living with AF in the United States, and these numbers are expected to increase in coming years.2, 3 More than 750 000 hospitalizations and 130 000 deaths are associated with AF each year in the United States, and this costs around $6 billion each year.2, 4 Mortality and morbidity related to AF remain high5 despite advancement in AF management. Many risk factors have been identified for AF including high blood pressure,6 diabetes mellitus,7 heart failure,8 obesity,9 hyperthyroidism,10 and ischemic heart disease.6 However, only a few studies have examined the role of dietary habits on AF risk. Coffee is a major drink in the United States, and the trend has gone up during the past year.11 Coffee contains caffeine, polyphenols, and diterpenes, which have been shown to influence cardiovascular disease.12 Coffee promotes the vrelease of epinephrine, norepinephrine, and renin13 and increases the sensitivity of myocardium to calcium,14, 15 which can affect heart rhythm. Few large studies have assessed the association of coffee consumption with the risk of AF, and results have been inconsistent. The Women's Health Study showed an increased risk of AF with 2 to 3 cups/day of caffeinated coffee.16 On the other hand, a meta‐analysis showed a nonsignificant inverse association of coffee intake with AF among women and a nonsignificant positive association among men.17 Given the widespread use of coffee around the world and the inconsistent relation between coffee and AF, we sought to examine whether coffee intake is associated with AF risk in a cohort of men.
Methods
All data and materials have been made publicly available at the Physician Health website.
Study Population
We used participants from the PHS (Physicians’ Health Study), which was divided into 2 phases, PHS I and PHS II. The PHS I was a randomized, double‐blinded, and placebo‐controlled trial of aspirin and β‐carotene among 22 071 US male physicians (1982‐1995). Detailed descriptions of PHS I have been published.18, 19 The PHS II evaluated the effect of different vitamin supplements on the prevention of cardiovascular disease, cancer, and age‐related eye disease among 14 641 participants (1997‐2007). Participants who replied to food frequency questionnaires from 1997 to 2001 were eligible for our study (N=21 082). We excluded a total of 2122 participants because of death before collection of data on coffee intake (n=7), history of AF (n=1962), and missing data on coffee consumption (n=153). The remaining 18 960 participants were used for current analyses. Each participant gave informed consent, and the study protocol was approved by the Institutional Review Board at the Brigham and Women's Hospital.
Assessment of Coffee Consumption/Caffeine Consumption
Participants provided dietary information through a food frequency questionnaire (1997‐2001). Each subject was asked about average use of coffee during the past year. Possible answers were never or <1 cup/month, 1 to 3 cups/month, 1 cup/week, 2 to 4 cups/week, 5 to 6 cups/week, 1 cup/day, 2 to 3 cups/day, 4 to 5 cups/day, and 6+ cups/day. We combined adjacent categories where data were sparse for stable estimates. Nutrients including dietary caffeine were derived using Harvard University nutrient databases supplemented by manufacturers’ information. The food frequency questionnaire has been validated in previous studies.20, 21
Ascertainment of AF in the PHS
Participants reported new AF diagnoses through follow‐up questionnaires. We performed a validation on 400 randomly selected AF cases. These participants were sent supplementary questionnaires to query about diagnosis and treatment of AF. In addition, we reviewed medical records for 225 new cases of AF. Self‐reported AF was confirmed 99% of the time. A detailed description of the AF validation in the PHS has been published.22
Other Variables
Each participant provided information on age, weight, height, smoking (never, former, and current smoker), exercise (none, <1 day/week, 1‐2 days/week, 3‐4 days/week, and 5‐7 days/week), and alcohol intake (never/rarely, monthly, weekly, daily, and >2+ cups/day), valvular heart disease, and parental history of myocardial infarction. We also obtained information on comorbidities including diabetes mellitus, blood pressure, hyperlipidemia, and heart failure at baseline and during follow‐up a through self‐reported questionnaire.
Statistical Analyses
We computed person‐time follow‐up from the food frequency questionnaire assessment until the first occurrence of atrial fibrillation, date of last follow up, death, or data‐cut date (March 2012). Within each category of coffee intake we calculated the crude incidence rate of AF by dividing AF cases by person‐time of follow‐up. We computed hazard ratio (HR) and 95% CI through the Cox proportional model. After the crude model we controlled for age, smoking, alcohol, and exercise. We adjusted our final model for age, smoking, alcohol, exercise, body mass index, systolic blood pressure, use of blood pressure medication, diabetes mellitus, high cholesterol, heart failure, and coronary heart disease. Because we did not know the shape of the relationship between coffee and AF (linear versus nonlinear), we used a restricted cubic spline to assess the nature and shape of the relationship.
In a secondary analysis we examined the association between dietary caffeine and AF using the Cox proportional hazard model.
All data were analyzed though SAS, version 9.4 (SAS Institute, Cary, NC).
Results
Baseline characteristics of participants according to coffee consumption are described in Table 1. Among the 18 960 participants, the mean age was 66.1 years, and the average follow‐up was 9 years. A total of 2098 new cases of AF occurred during follow‐up. Crude incidence rates of AF were 13.5, 11.9, 15.0, 13.5, 12.7, 11.4, and 10.6 per 1000 person‐years, from the lowest to highest category of coffee consumption, respectively.
Table 1.
Baseline Characteristics of 18 960 Male Physicians According to Coffee Consumption
| Variables | Categories of Coffee Consumption | |||||||
|---|---|---|---|---|---|---|---|---|
| Almost Never (N=3946) | ≤1 cup/wk (N=1419) | 2 to 4 cups/wk (N=1036) | 5 to 6 cups/wk (N=766) | 1 cup/d (N=3453) | 2 to 3 cups/d (N=6432) | 4+ cups/d (N=1908) | P for Difference | |
| Age, ya | 66.6±9.5 | 66.9±9.0 | 66.9±8.8 | 67.7±9.1 | 67.9±9.4 | 65.3±8.8 | 62.7±8.2 | <0.0001 |
| Body mass index, kg/m2 a | 25.5±3.3 | 25.6±3.4 | 25.7±3.5 | 25.9±3.3 | 25.5±3.2 | 26.0±3.3 | 26.3±3.5 | <0.0001 |
| Exercise, % | 0.22 | |||||||
| None | 34.3 | 34.5 | 33.3 | 34.5 | 37.3 | 34.5 | 34.9 | |
| <1 d/wk | 3.2 | 2.5 | 3.2 | 1.9 | 3.0 | 2.8 | 3.4 | |
| 1 to 2 d /wk | 16.1 | 17.0 | 16.7 | 16.8 | 16.4 | 16.8 | 16.5 | |
| 3 to 4 d/wk | 29.2 | 29.7 | 30.6 | 31.8 | 28.9 | 30.6 | 29.1 | |
| 5 to 7 d/wk | 17.2 | 16.3 | 16.3 | 15.1 | 14.6 | 15.3 | 16.1 | |
| Alcohol use, % | <0.0001 | |||||||
| Never | 33.5 | 20.1 | 18.9 | 16.5 | 15.8 | 12.5 | 16.2 | |
| Monthly | 8.4 | 8.3 | 8.4 | 6.6 | 5.7 | 5.5 | 6.0 | |
| Weekly | 35.3 | 43.4 | 42.4 | 47.2 | 38.4 | 36.3 | 34.8 | |
| Daily | 11.2 | 15.5 | 16.3 | 15.8 | 21.2 | 20.3 | 16.8 | |
| ≥2 cups/d | 11.6 | 12.7 | 14.0 | 14.0 | 19.0 | 25.5 | 26.2 | |
| Smoking, % | <0.0001 | |||||||
| Never | 66.3 | 61.5 | 59.0 | 55.6 | 52.5 | 49.8 | 45.2 | |
| Past | 31.9 | 36.2 | 39.0 | 41.3 | 44.7 | 46.2 | 46.4 | |
| Current | 1.8 | 2.3 | 2.0 | 3.1 | 2.8 | 4.0 | 8.4 | |
| Heart failure, % | 1.8 | 1.7 | 1.2 | 1.2 | 1.6 | 0.8 | 0.6 | <0.0001 |
| Valvular heart disease, % | 1.5 | 2.1 | 0.9 | 2.1 | 1.3 | 1.1 | 0.6 | 0.0007 |
| Parental history of myocardial infarction, % | 10.7 | 9.6 | 12.1 | 9.3 | 9.9 | 10.6 | 11.7 | 0.16 |
| High cholesterol, % | 42.1 | 45.8 | 44.6 | 47.5 | 44.2 | 41.1 | 38.3 | <0.0001 |
| Diabetes mellitus, % | 7.3 | 8.6 | 8.7 | 10.1 | 7.9 | 6.5 | 5.7 | <0.0001 |
| Hypertension medication, % | 35.9 | 37.5 | 37.5 | 39.8 | 38.2 | 32.8 | 27.7 | <0.0001 |
| Coronary heart disease, % | 14.2 | 14.2 | 12.6 | 15.9 | 13.3 | 9.7 | 8.0 | <0.0001 |
| Energy intake, kcala | 1674±522 | 1669±532 | 1659±509 | 1541±472 | 1669±515 | 1688±510 | 1780±558 | <0.0001 |
| Caffeine intake, mga | 55±65 | 64±60 | 90±51 | 120±47 | 138±48 | 281±53 | 496±97 | <0.0001 |
| Systolic blood pressure, mm Hga | 129±29 | 129±22 | 129±25 | 131±36 | 131±35 | 129±30 | 127±20 | 0.0041 |
Missing numbers according to variables: body mass index (n=26), systolic blood pressure (n=1759), alcohol intake (n=44), exercise (n=340), smoking (n=12), history of hypercholesterolemia (n=464), taking hypertension medications (n=581), parenteral history of myocardial infraction (1316).
Mean and standard deviation.
In our primary analysis multivariable adjusted HR (95% CI) showed a lower risk of AF only among participants who reported coffee consumption of 1 to 3 cups/day (Table 2, P for nonlinear trend=0.01). The fitted spline curve suggested a J‐shaped association between coffee consumption and AF risk with inverse association up to 3 cups/day (Figure). Inclusion of body mass index, systolic blood pressure, use of blood pressure medication, diabetes mellitus, high cholesterol, heart failure, and coronary heart disease did not alter the results (HR [95% CI] 0.84 [0.69‐1.02], 1.05 [0.86‐1.29], 0.88 [0.69‐1.13], 0.87 [0.75‐1.00], 0.85 [0.75‐0.97], and 0.93 [0.77‐1.12], for increasing categories of coffee intake, respectively).
Table 2.
Incidence Rate and HR (95% CI) of AF According to Coffee Consumption Categories (N=18 960)
| Coffee Consumption | Cases | Incidence Rate | Crude HR (95% CI) | Model 1 HR (95% CI) | Model 2 HR (95% CI) | Model 3 HR (95% CI) |
|---|---|---|---|---|---|---|
| Almost never | 472 | 13.5 | 1.0 | 1.0 | 1.0 | 1.0 |
| ≤1 cup/wk | 151 | 11.9 | 0.88 (0.74‐1.06) | 0.86 (0.71‐1.03) | 0.85 (0.71‐1.02) | 0.84 (0.69‐1.02) |
| 2 to 4 cups/wk | 137 | 15.0 | 1.11 (0.92‐1.34) | 1.09 (0.90‐1.32) | 1.07 (0.88‐1.30) | 1.05 (0.86‐1.29) |
| 5 to 6 cups/wk | 89 | 13.5 | 1.00 (0.80‐1.26) | 0.95 (0.76‐1.19) | 0.93 (0.74‐1.17) | 0.88 (0.69‐1.13) |
| 1 cup/d | 383 | 12.7 | 0.94 (0.82‐1.08) | 0.87 (0.76‐0.99) | 0.85 (0.74‐0.98) | 0.87 (0.75‐1.00) |
| 2 to 3 cups/d | 675 | 11.4 | 0.84 (0.75‐0.94) | 0.91 (0.81‐1.03) | 0.86 (0.76‐0.97) | 0.85 (0.75‐0.97) |
| 4+ cups/d | 191 | 10.6 | 0.78 (0.66‐0.92) | 1.02 (0.86‐1.21) | 0.96 (0.80‐1.14) | 0.93 (0.77‐1.12) |
| P for linear trend | 0.0006 | 0.28 | 0.05 | 0.04 |
Incidence rate, cases/1000 person‐years. Model 1: Adjusted for age. Model 2: Adjusted for age, smoking, alcohol intake (never, rarely, monthly, weekly, daily, >2 cups/d), and exercise (none, <1 d/wk, 1‐2 d/wk, 3‐4 d/wk, 5‐7 d/wk). Model 3: Adjusted for variables in Model 2 plus BMI, systolic blood pressure, taking blood pressure medication, diabetes mellitus, high cholesterol, heart failure, and coronary heart disease. AF indicates atrial fibrillation; BMI, body mass index; HR, hazard ratio.
Figure 1.
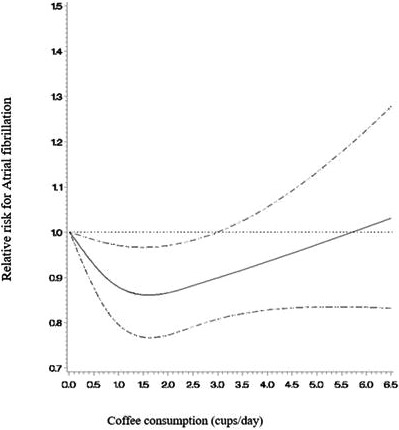
Spline curve assessing the relationship between coffee consumption and atrial fibrillation risk. (Dashed curves indicate 95% CI band.) Adjusted for age, smoking, alcohol, and exercise (P for nonlinear trend=0.01).
In a secondary analysis we did not find any significant relationship between dietary caffeine intake and risk of AF (HR [95% CI] of AF per standard deviation [149‐mg] change in caffeine intake was 0.96 [0.91‐1.01] in a model adjusted for age, smoking, alcohol, exercise, body mass index, systolic blood pressure, use of blood pressure medication, diabetes mellitus, high cholesterol, heart failure, and coronary heart disease).
Discussion
In this cohort of US male physicians we found a lower risk of AF only among participants drinking 1 to 3 cups of coffee per day; consumption below 1 cup/day or above 3 cups/day was not associated with AF risk.
Our findings are consistent with the NCCHC (Northern California Comprehensive Health Care Study),23 which reported a lower risk of AF‐related hospitalization among people drinking ≥4 cups of coffee per day (HR [95% CI] 0.81 [0.69‐0.96]). The Northern California Comprehensive cohort assessed AF risk among hospitalized patients only, so it could have missed out‐of‐hospital AF cases. Furthermore, the Danish Diet Cancer and Health Study24 also found a lower risk of AF among people consuming 6 to 7 cups of coffee per day (HR [95% CI] 0.79 [0.64‐0.98]).
Contrary to our results, a study by Wilhelmsen et al25 (N=7495, mean follow‐up 25 years) reported a 24% higher risk of AF with coffee intake of 1 to 4 cups/day compared with participants who did not drink coffee (OR [95% CI] 1.24 [1.00‐1.54], adjusting for age only). Of note is that Wilhelmsen et al enrolled participants at higher risk for AF than our cohort (subjects enrolled for intervention trial against smoking, blood pressure, and hypercholesterolemia). The Women's Health Study16 also showed a 36% higher risk of AF with caffeinated coffee intake of 2 to 3 cups/day among women in a multivariable model (HR [95% CI] 1.36 [1.12‐1.65]). The difference in outcomes between the Women's Health Study and our study could be due to gender difference and/or to a higher percentage of current smokers in the Women's Health Study (12.3% versus 3.5% in our study).
A study by Larsson et al did not find any significant association between coffee consumption and risk of AF among a Swedish cohort.17 In addition, a meta‐analysis by Larsson et al, including 6 studies,17 did not find any significant association between coffee intake and AF risk, comparing the highest versus the lowest category of coffee consumption (RR [95% CI] 0.96 [0.80‐1.08]).
We did not find any significant association between dietary caffeine intake and AF risk in our secondary analysis. The observed effect in the primary analysis could be due to other components of coffee. Coffee contains a high number of antioxidants including polyphenol, cafestol, polyphenol, trigonelline, chlorogenic acid, and quinine, which could reduce cardiovascular events through anti‐inflammatory effect. Previous studies have reported an inverse association between polyphenols and cardiovascular disease.26 Additionally, antioxidants have been reported to be protective against AF.27 Furthermore, perioperative antioxidant supplementation has been reported to prevent AF after cardiac surgery in a meta‐analysis.28
Our study has some limitations. First, our cohort consisted of male physicians, who usually are more health conscious than the general population, which could limit the generalizability of our findings. However, a significant proportion of participants used alcohol and tobacco and were not exercising. Second, we did not have data on coffee preparation methods including boiled, filtered versus unfiltered, and types of brewing; and we were unable to differentiate caffeinated versus decaffeinated coffee use in our cohort. Third, we lacked repeated measures of coffee intake over time for further analyses. However, our study has some strengths including a large sample size, long‐term follow‐up, prospective study design, and standard method of ascertainment of AF.
Conclusion
Our data suggest a lower risk of AF among men drinking 1 to 3 cups of coffee per day but no meaningful relationship with other frequencies of coffee intake.
Author Contributions
Bodar and Djoussé created the study design, and Chen did the statistical analysis. Gaziano, Albert, and Djoussé were responsible for the acquisition of data. Bodar drafted this article with critical review and editing by Djoussé, Chen, Gaziano, and Albert. Gaziano and Djoussé obtained funding for this study. All authors reviewed the article and have a responsibility for its final content.
Sources of Funding
This study is supported by grants R21HL088081 from the National Heart, Lung, and Blood Institute. The PHS was supported by grants CA‐34944, CA‐40360, CA‐097193, HL‐26490, and HL‐34595 from the National Institutes of Health, Bethesda, MD.
Disclosures
None.
Acknowledgments
We would like to thank the PHS participants for their valuable commitment and contribution. We are also grateful to the PHS team for their contribution to the current project.
(J Am Heart Assoc. 2019;8:e011346 DOI: 10.1161/JAHA.118.011346.)
References
- 1. Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton‐Cheh C, Lubitz SA, Magnani JW, Ellinor PT, Seshadri S, Wolf PA, Vasan RS, Benjamin EJ, Levy D. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Centers for Disease Control and Prevention; Division for Heart Disease and Stroke Prevention . Atrial fibrillation fact sheet. August 22, 2017. Available at: https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_atrial_fibrillation.htm. Accessed January 13, 2018.
- 3. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW; ACC/AHA Task Force Members . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. [DOI] [PubMed] [Google Scholar]
- 4. Gilligan AM, Gandhi P, Song X, Wang C, Henriques C, Sander S, Smith DM. All‐cause, stroke‐, and bleed‐specific healthcare costs: comparison among patients with non‐valvular atrial fibrillation (NVAF) newly treated with dabigatran or warfarin. Am J Cardiovasc Drugs. 2017;17:481–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Andersson T, Magnuson A, Bryngelsson IL, Frøbert O, Henriksson KM, Edvardsson N, Poçi D. All‐cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995–2008: a Swedish nationwide long‐term case‐control study. Eur Heart J. 2013;34:1061–1067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population‐based cohort. The Framingham Heart Study. JAMA. 1994;271:840–844. [PubMed] [Google Scholar]
- 7. Movahed MR, Hashemzadeh M, Jamal MM. Diabetes mellitus is a strong, independent risk for atrial fibrillation and flutter in addition to other cardiovascular disease. Int J Cardiol. 2005;105:315–318. [DOI] [PubMed] [Google Scholar]
- 8. Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91:2D–8D. [DOI] [PubMed] [Google Scholar]
- 9. Wang TJ, Parise H, Levy D, D'Agostino RB Sr, Wolf PA, Vasan RS, Benjamin EJ. Obesity and the risk of new‐onset atrial fibrillation. JAMA. 2004;292:2471–2477. [DOI] [PubMed] [Google Scholar]
- 10. Auer J, Scheibner P, Mische T, Langsteger W, Eber O, Eber B. Subclinical hyperthyroidism as a risk factor for atrial fibrillation. Am Heart J. 2001;142:838–842. [DOI] [PubMed] [Google Scholar]
- 11. Nick B. 2017 US Coffee Drinking Trends Include More Gourmet, More Youth. Daily Coffee News by Roast Magazine. August 31, 2017. Available at: https://dailycoffeenews.com/2017/03/27/2017-us-coffee-drinking-trends-include-more-gourmet-more-youth. Accessed January 14, 2018.
- 12. Bonita JS, Mandarano M, Shuta D, Vinson J. Coffee and cardiovascular disease: in vitro, cellular, animal, and human studies. Pharmacol Res. 2007;55:187–198. [DOI] [PubMed] [Google Scholar]
- 13. Robertson D, Frölich JC, Carr RK, Watson JT, Hollifield JW, Shand DG, Oates JA. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. N Engl J Med. 1978;298:181–186. [DOI] [PubMed] [Google Scholar]
- 14. Wendt IR, Stephenson DG. Effects of caffeine on Ca‐activated force production in skinned cardiac and skeletal muscle fibres of the rat. Pflugers Arch. 1983;398:210–216. [DOI] [PubMed] [Google Scholar]
- 15. Kong H, Jones PP, Koop A, Zhang L, Duff HJ, Wayne Chen SR. Caffeine induces Ca2+ release by reducing the threshold for luminal Ca2+ activation of the ryanodine receptor. Biochem J. 2008;414:441–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Conen D, Chiuve SE, Everett BM, Zhang SM, Buring JE, Albert CM. Caffeine consumption and incident atrial fibrillation in women. Am J Clin Nutr. 2010;92:509–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Larsson SC, Drca N, Jensen‐Urstad M, Wolk A. Coffee consumption is not associated with increased risk of atrial fibrillation: results from two prospective cohorts and a meta‐analysis. BMC Med. 2015;13:207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Steering Committee of the Physicians’ Health Study Research Group . Final report on the aspirin component of the ongoing Physicians’ Health Study. N Engl J Med. 1989;321:129–135. [DOI] [PubMed] [Google Scholar]
- 19. Christen WG, Gaziano JM, Hennekens CH. Design of Physicians’ Health Study II—a randomized trial of beta‐carotene, vitamins E and C, and multivitamins, in prevention of cancer, cardiovascular disease, and eye disease, and review of results of completed trials. Ann Epidemiol. 2000;10:125–134. [DOI] [PubMed] [Google Scholar]
- 20. Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C, Witschi J, Hennekens CH, Speizer FE. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol. 1985;122:51–65. [DOI] [PubMed] [Google Scholar]
- 21. Rimm EB, Giovannucci EL, Stampfer MJ, Colditz GA, Litin LB, Willett WC. Reproducibility and validity of an expanded self‐administered semiquantitative food frequency questionnaire among male health professionals. Am J Epidemiol. 1992;135:1114–1126. [DOI] [PubMed] [Google Scholar]
- 22. Aizer A, Gaziano J, Cook NR, Manson JE, Buring JE, Albert CM. Relation of vigorous exercise to risk of atrial fibrillation. Am J Cardiol. 2009;103:1572–1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Klatsky AL, Hasan AS, Armstrong MA, Udaltsova N, Morton C. Coffee, caffeine, and risk of hospitalization for arrhythmias. Perm J. 2011;15:19–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Mostofsky E, Johansen MB, Lundbye‐Christensen S, Tjønneland A, Mittleman MA, Overvad K. Risk of atrial fibrillation associated with coffee intake: findings from the Danish Diet, Cancer, and Health study. Eur J Prev Cardiol. 2016;23:922–930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Wilhelmsen L, Rosengren A, Lappas G. Hospitalizations for atrial fibrillation in the general male population: morbidity and risk factors. J Intern Med. 2001;250:382–389. [DOI] [PubMed] [Google Scholar]
- 26. Habauzit V, Morand C. Evidence for a protective effect of polyphenols‐containing foods on cardiovascular health: an update for clinicians. Ther Adv Chronic Dis. 2012;3:87–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Violi F, Pastori D, Pignatelli P, Loffredo L. Antioxidants for prevention of atrial fibrillation: a potentially useful future therapeutic approach? A review of the literature and meta‐analysis. Europace. 2014;16:1107–1116. [DOI] [PubMed] [Google Scholar]
- 28. Ali‐Hassan‐Sayegh S, Mirhosseini SJ, Rezaeisadrabadi M, Dehghan HR, Sedaghat‐Hamedani F, Kayvanpour E, Popov AF, Liakopoulos OJ. Antioxidant supplementations for prevention of atrial fibrillation after cardiac surgery: an updated comprehensive systematic review and meta‐analysis of 23 randomized controlled trials. Interact Cardiovasc Thorac Surg. 2014;18:646–654. [DOI] [PubMed] [Google Scholar]