

The temporomandibular joints (TMJs) play crucial roles in mastication and jaw mobility, and in verbal and emotional expression. Temporomandibular disorders (TMDs) include several disorders that can lead to orofacial pain symptoms. Box 1 presents a TMD taxonomic classification adopted from a publication by a panel of experts developing the diagnostic criteria for TMD (DC/TMD) for the most common TMDs,1 and the expanded TMD taxonomy for the more uncommon TMDs.2 It has been reported that about 5% to 12% of the United States population is affected by TMD, and the annual cost of managing TMD, excluding cost related to imaging, is about $4 billion.1 Plesh and colleagues3 reported that in the 2000 to 2005 US National Health Interview Survey (NHIS) that included a total of 189,977 people, 4.6% (n = 8964) people had experienced temporomandibular joint and muscle disorder (TMJD).
Box 1. Taxonomy of temporomandibular joint disorders.
| I.Temporomandibular disorders |
| a. Joint pain |
| b. Joint disorders |
| i. Disc disorders |
| ii. Hypomobility disorders other than disc disorders |
| iii. Hypermobility disorders |
| c. Joint diseases |
| i. Degenerative joint disease |
| ii. Systemic arthritides |
| iii. Condylysis/idiopathic condylar resorption |
| iv. Osteochondritis dissecans |
| v. Osteonecrosis |
| vi. Neoplasm |
| vii. Synovial chondromatosis |
| d. Fractures |
| e. Congenital/developmental disorders |
| II. Masticatory muscle disorders |
| a. Muscle pain |
| i. Myalgia |
| ii. Tendonitis |
| iii. Myositis |
| iv. Spasm |
| b. Contracture |
| c. Hypertrophy |
| d. Neoplasm |
| e. Movement disorders |
| f. Masticatory muscle pain attributed to systemic/central pain disorders |
| III. Headache |
| a. Headache attributed to TMD |
| IV. Associated structures |
| a. Coronoid hyperplasia |
Progress in cross-sectional imaging using computed tomography (CT), MRI, and cone-beam CT (CBCT) has allowed better evaluation of the TMJ. Traditionally TMJ radiographic examinations included 2-dimensional images, such as transcranial, transmaxillary, and transpharyngeal projections, and submentovertex, lateral, and posteroanterior cephalometric radiographs.4 Conventional and panoramic tomography has also been used in TMD diagnosis but has limited use in assessing the TMJs.5
The following sections provide a brief overview of the most common TMJ-related disorders and most appropriate imaging techniques. The latest recommendation from the panel of experts who developed the DC/TMD concluded that imaging should not be obtained routinely, but should be based on the clinical needs of the patient.1
DISC DISPLACEMENT
Disc displacement of the TMJ is a condition whereby the articular disc is displaced from its normal functional relationship with the condylar head and the articular fossa of the temporal bone (Fig. 1). Disc displacement is considered to have 4 clinical stages.6
Fig. 1.
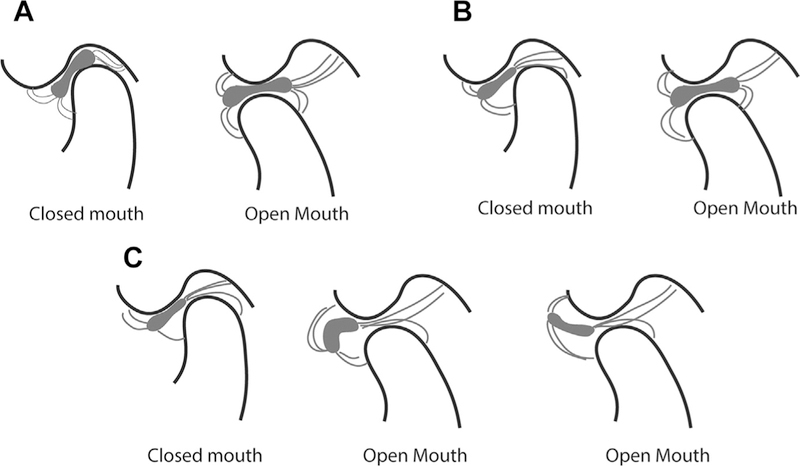
Relationship between bone and articular disc of the temporomandibular joint. (A) Normal disc location in closed- and open-mouth position. In the closed-mouth position, the posterior band of the articular disc is located between 11:30 and 12:30 of a clock face. The central narrow zone of the disc is in contact with the condylar surface and the articular fossa. In the open-mouth position, the central narrow zone of the disc remains in contact with the condylar head and the articular eminence. (B) Disc displacement with reduction. In the closed-mouth position, the posterior band of the articular disc is displaced anterior to 11:30. The central narrow zone of the disc is not in contact with the condyle or the articular fossa. In the open-mouth position, the central narrow zone of the disc is in contact with the condylar head and articular eminence. (C) Disc displacement without reduction. In the closed-mouth position, the posterior band of the articular disc is displaced anterior to 11:30. The central narrow zone of the disc is not in contact with the condyle or the articular fossa. In the open-mouth position, the disc is anteriorly displaced, and may assume a normal biconcave shape or become deformed.
Stage I (disc displacement with reduction): the articular disc is displaced in closed-mouth position, and reduces to normal relationship, that is, the central narrow zone of the disc is in contact with the condylar head and articular eminence, in open-mouth position
Stage II (disc displacement with reduction with intermittent locking): the disc is displaced in closed-mouth position, and intermittently locks in open-mouth position
Stage III (disc displacement without reduction): the disc is displaced in closed- mouth position, and does not reduce to normal contact in open-mouth position (also referred to as closed lock)
Stage IV (disc displacement without reduction): the disc is displaced and does not reduce, with perforation of the disc or posterior attachment tissues.
A commonly used classification of TMJ disc displacement, referred to as internal derangement, was described by Wilkes.7 This classification (Table 1) described clinical and radiographic findings, the latter being based on MRI and tomography.
Table 1.
Wilkes classification of disc displacement and degenerative joint disease
| Early stage (stage I) | Slight forward displacement and good anatomic contour of the disc. No osseous changes |
| Early/intermediate stage (stage II) | Slight forward displacement, and slight thickening of posterior edge or beginning anatomic deformity of disc. No osseous changes |
| Intermediate stage (stage III) | Anterior displacement with significant anatomic deformity/prolapse of disc (moderate to marked thickening of posterior edge). No osseous changes |
| Intermediate/late stage (stage IV) | Increase in severity over intermediate stage. Early to moderate degenerative osseous changes |
| Late stage (stage V) | Anterior disc displacement, nonreducing with perforation, gross anatomic deformity of the disc and hard tissues. Severe degenerative osseous changes |
From Wilkes CH. Internal derangements of the temporomandibular joint. Pathological variations. Arch Otolaryngol Head Neck Surg 1989;115(4):470; with permission.
Individuals with disc displacement can be asymptomatic.8 Persons who have disc displacement with reduction may have a normal range of jaw movement or limitations because of pain. Clinical examination may reveal joint sounds (eg, clicking and popping) during jaw movements. Individuals with disc displacement without reduction with limited opening may have deviation during opening toward the involved joint, and limited contralateral movements accompanied by pain and functional limitations, including compromised ability to eat.
Imaging
MRI of the TMJ in both closed and open positions is necessary for diagnosing stages of disc displacement (Fig. 2). Other radiographic examinations, such as panoramic radiography or CT, are not useful in determining the location of the disc. In some individuals with a history of trauma, fluid effusion may be present. Effusion can be identified with T2-weighted MRI, whereby effusion has high signal intensity (see Fig. 2E2, Table 2). The authors have updated the previous diagnostic criteria for disc displacement developed by their team (see Table 2).5
Fig. 2.
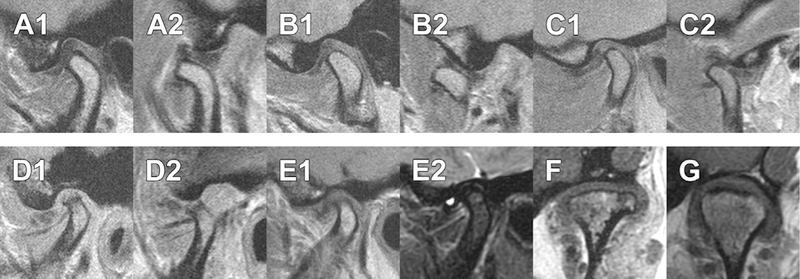
MRI of the temporomandibular joints. A1 and A2 are from the same patient, in closed (A1) and open (A2) mouth position, showing normal disc relationship with the condylar head and articular fossa/eminence. B1 and B2 are from the same patient, in closed (B1) and open (B2) mouth position, showing anteriorly displaced intermediate zone of the disc (B1) and normal disc relationship with condylar head and articular eminence (B2). C1 and C2 are from the same patient, in closed (C1) and open (C2) mouth position, showing disc displacement with reduction. D1 and D2 are from the same patient, in closed (D1) and open (D2) mouth position, showing disc displacement without reduction. E1 and E2 are from the same patient in closed-mouth position. E2, which is a T2-weighted image, shows presence of effusion as a region of bright intensity. (F, G) Axially corrected coronal views from different patients, of (F) normal disc position and (G) laterally displaced disc. All images are proton density except E2.
Table 2.
Image analysis criteria for disc position based on MRI
| Image Type | Mouth Position | Diagnosis | Posterior Band of the Disc | Intermediate Zone of the Disc |
|---|---|---|---|---|
| T1 or proton-density MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Normal disc position | Relative to the superior aspect of the condyle, the border between the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | Located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence |
| Indeterminant disc position | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The condyle contacts the intermediate zone located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence | ||
| Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | The intermediate zone of the disc is not in contact with the condyle | |||
| Displaced disc | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The intermediate zone of the disc is located anterior to the condyle | ||
| Disc not visible | Neither signal intensity nor outlines make it possible to define a structure as the disc | |||
| Open mouth | Disc with reduction | Location of posterior band of the disc is not critical | The intermediate zone is located between the condyle and the articular eminence | |
| Disc without reduction | The intermediate zone is located anterior to the condylar head | |||
| T2 MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Effusion present | A bright signal in either joint space that extends beyond the osseous contours of the fossa/ articular eminence and/or condyle and has a convex configuration in the anterior or posterior recesses | |
| Effusion absent | No bright signal in either joint space, or a bright signal in either joint space that conforms to the contours of the disc, fossa/articular eminence, and/or condyle | |||
INFLAMMATORY DISTURBANCES OF THE TEMPOROMANDIBULAR JOINT
Arthralgia refers to joint pain, common causes of which include mechanical, metabolic, infectious, neuropathic, or inflammatory factors. When inflammation is present, this is referred to as arthritis,2 one of the most prevalent chronic diseases. The TMJ may be affected by any form of arthritis. Tanaka and colleagues9 classified arthritis as low-inflammatory or high-inflammatory disorder. Low-inflammatory arthritic disorders include degenerative joint disease or osteoarthritis, and posttraumatic arthritis. High-inflammatory arthritic disorders include infectious arthritis, adult and juvenile rheumatic arthritic conditions, and metabolic arthritic conditions, for example, gouty arthritis, psoriatic arthritis, lupus erythematosus, ankylosis spondylitis, Reiter syndrome, and arthritis associated with ulcerative colitis.
DEGENERATIVE JOINT DISEASE
The terms degenerative joint disease (DJD), osteoarthritis, and osteoarthrosis are often used interchangeably.1,5,9,10 Peck and colleagues2 suggested that DJD be subdivided into osteoarthritis and osteoarthrosis, with both having the same diagnostic criteria but with the added feature of osteoarthritis denoting individuals with joint pain, whereas individuals with osteoarthrosis have DJD but no joint pain. Although its etiology is largely unknown, DJD is a disease often associated with trauma and the aging process. The joints first involved are those that bear the weight of the body and thus are subjected to continued stress and strain: the joints of the knees, hips, and spine. In the case of TMJs, primary DJD is by definition idiopathic. Secondary DJD is assumed to typically occur after the disc is displaced and bony contact exists between the condyle and articular fossa. However, there are reports that DJD can precede disc displacement. Clinical signs and symptoms of DJD are often remarkably absent even in the face of severe histologic or radiographic joint changes (i.e., osteoarthrosis).
RADIOGRAPHIC DIAGNOSTIC CRITERIA
DJD is diagnosed radiographically, as the clinical signs and symptoms have poor validity.1 In an in-depth review, Larheim and colleagues10 concluded that CBCT and CT are the reliable examinations to diagnose degenerative changes, and the diagnostic accuracy of CBCT for DJD is similar to that of CT. MRI and panoramic radiographs have limited value in diagnosing early degenerative changes.5,11
Three cardinal radiographic features that lead to a diagnosis of DJD are osteophyte, surface erosion, and subcortical pseudocyst.5 These features are shown in Fig. 3 and are defined as follows:
Fig. 3.
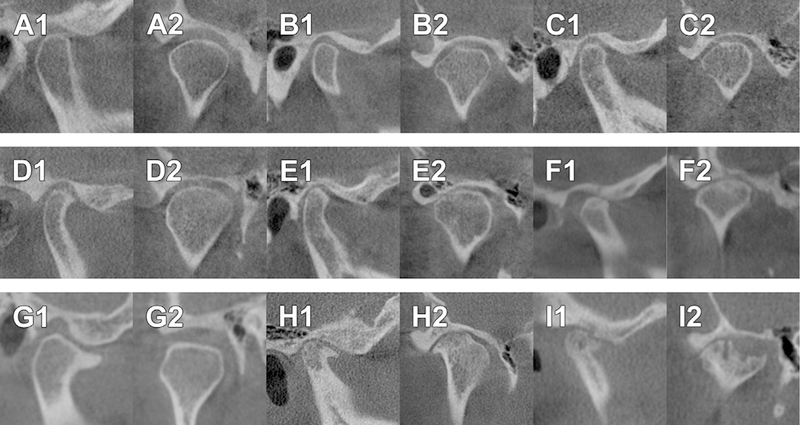
CBCT findings of normal and different representations of degenerative joint disease. A1 and A2 are from the same patient, in corrected sagittal (A1) and corrected coronal (A2) orientations, showing a normal temporomandibular joint, which has smooth, rounded, and well-defined cortical margin of the condyle and the fossa. B1 and B2 are from the same patient, in corrected sagittal (B1) and corrected coronal (B2) orientations, showing flattening of the anterior and lateral slopes of the condylar head, indicating remodeling of the joint. C1 and C2 are from the same patient, in corrected sagittal (C1) and corrected coronal (C2) orientations, showing localized subcortical sclerosis of the condylar head, which indicates remodeling of the joint. The middle panel shows examples of grade 1 DJD. D1 and D2 are from the same patient, in corrected sagittal (D1) and corrected coronal (D2) orientations, showing an osteophyte at the anterior aspect of the condyle. E1 and E2 are from the same patient, in corrected sagittal (E1) and corrected coronal (E2) orientations, showing flattening and subcortical sclerosis of the anterior slope (E1) and localized erosion of the condyle (E2). F1 and F2 are from the same patient, in corrected sagittal (F1) and corrected coronal (F2) orientations, show the presence of a single subcortical pseudocyst. The lower panel shows examples of grade 2 DJD. G1 and G2 are from the same patient, in corrected sagittal (G1) and corrected coronal (G2) orientations, showing an anterior osteophyte larger than 2 mm (G1) and flattening of the superior and lateral slopes of the condyle (G2). H1 and H2 are from the same patient, in corrected sagittal (H1) and corrected coronal (H2) orientations, showing the presence of osteophytes and multiple subcortical pseudocysts. I1 and 12 are from the same patient, in corrected sagittal (I1) and corrected coronal (I2) orientations, showing the presence of osteophytes and multiple areas of erosion, one of which is wider than 2 mm.
An osteophyte is a marginal hypertrophy with sclerotic borders and exophytic angular formation of osseous tissue arising from the surface.
Surface erosion is loss of continuity of articular cortex of the condyle or the fossa.
A subcortical pseudocyst is defined as a cavity below the articular surface that deviates from normal marrow pattern. It is not a true cyst but rather the loss of trabeculation.
Other radiographic findings related to possible osseous remodeling are articular surface flattening and subcortical sclerosis. Flattening and subcortical sclerosis may be indeterminate for degenerative joint disease as they may represent aging, functional remodeling of the joints, or a precursor to DJD.10 Longitudinally, flattening and sclerosis may progress to DJD; as such it would represent regressive remodeling, whereas if it does not progress would represent adaptive remodeling.
A surface flattening is defined as a loss of rounded contour of the surface of the condyle or the articular eminence; this can be present in normal joints and be a variation of normal.
A subcortical sclerosis is defined as any increased thickness of the cortical plate in the load-bearing areas related to the adjacent non-load-bearing areas; this likely results from increased loading, or from normal loading when the disc is displaced.
In evaluating the TMJ, it is necessary to describe the extent of DJD. Although this is a diagnostic challenge, grading of DJD is important in evaluating progress or stability of the disorder.10 Tanaka and colleagues9 have developed a classification of the extent of DJD. In this classification the investigators have considered clinical signs, symptoms, imaging features, and management options to arrive at a grading of the DJD. The diagnostic criteria based on imaging are: stage I, early disease: mild to moderate erosive changes of the condyle/fossa/eminence; stage II, arrested disease: flattened condyle/eminence; and stage III, gross erosive changes, loss of condyle and eminence height, ankylosis, and/or hypertrophy of coronoid process. In another classification of the severity of the arthritis, Koos and colleagues12 categorized the joints as class A (no form change), class B (deformation), and class C (destruction). The primary classes were subclassified as mild, moderate, and severe for flattening and erosion, and yes/no for osteophytes. These 2 classifications use the terminologies of mild, moderate, and gross/severe changes. Such terminologies are likely to be subjective during image interpretation. The reliability of these classification schemes is largely unknown.
To reduce the subjectivity of image interpretation, in unpublished work related to the DC/TMD Validation Project, the authors have developed the following image analysis criteria in grading the extent of DJD.5 These diagnostic criteria can be used to interpret CT, CBCT, or MRI.
DJD is classified as grade 1 (see Fig. 3D1–F2) if the joint displays any 1 of the following features:
Osteophyte (the greatest length of the osteophyte is <2 mm when measured from tip of osteophyte to expected contour of condyle as viewed on the corrected sagittal section), or
Erosion (the greatest dimension of the erosion is <2 mm in depth and width), and the erosion is limited to a single occurrence only, or
Subcortical pseudocyst (the greatest dimension of the pseudocyst is <2 mm in depth and width) and the pseudocyst is limited to a single occurrence only
A DJD is classified as grade 2 (see Fig. 3G1–I2) if the joint displays 1 or more of the following features:
Osteophyte (the greatest length of the osteophyte is ≥2 mm measured from tip of osteophyte to expected contour of condyle as viewed on the corrected sagittal section), and/or
Erosion (the greatest dimension of the erosion is ≥2 mm in depth and width), or more than 1 erosion of any size, and/or
Subcortical pseudocyst (the greatest dimension of the pseudocyst is ≥), or more than 1 pseudocyst of any size, and/or
Two or more imaging signs of grade 1 DJD
For grading DJD, the authors adopted the following 2 principles:
Most advanced finding in all views will be used to arrive at the diagnosis of DJD. The most advanced finding should be visible in 2 image orientations.
If erosion and cyst are continuous, it is called erosion.
RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is a chronic inflammatory disease of unknown etiology, characterized by joint swelling, joint tenderness, and destruction of the synovial joints, leading to severe disability and premature mortality.13 The distribution of joint involvement is nearly always polyarticular and frequently symmetrically bilateral. Patients usually manifest chronic episodic exacerbations and remissions. TMJ involvement in cases of RA is not particularly common despite this being a polyarticular disease.
Juvenile idiopathic arthritis (JIA) (juvenile RA or Still disease) is a pediatric rheumatic disease. TMJ involvement in JIA patients may be as high as 87%. Some studies indicate that TMJ can be the only joint involved with JIA. The patient may be asymptomatic, without any clinical signs and symptoms. The first clinical signs may be limited range of motion and asymmetry of the mandible, and class II malocclusion attributable to irreversible condylar resorption.
Imaging
Radiographic examination (Fig. 4) of RA of the TMJ includes panoramic radiography,14 CT,15 and MRI.16 Erosion of the condylar head is the most common finding of RA on a panoramic radiograph.14 Goupille and colleagues15 reported that characteristic findings of RA in CT are erosion, subcortical pseudocyst, flattening of the articular eminence, erosion of the glenoid fossa, and decreased joint space. Using MRI, Kretapirom and colleagues16 classified 4 types of osseous changes in the condyle: type I, abnormal signal intensity of the condylar bone marrow without erosion or resorption; type II, surface erosion of the condylar cortex; type III, bone resorption extending within half of the condylar head; and type IV, bone resorption involving more than half of the condylar head. Unlike the findings in DJD, the disc in RA can be in the normal position despite significant osseous changes. Disc displacement may be a late phenomenon in RA. In contrast to DJD, in RA osteophyte formation is not a frequent finding. Effusion is significantly more frequent in RA patients than in patients with DJD.
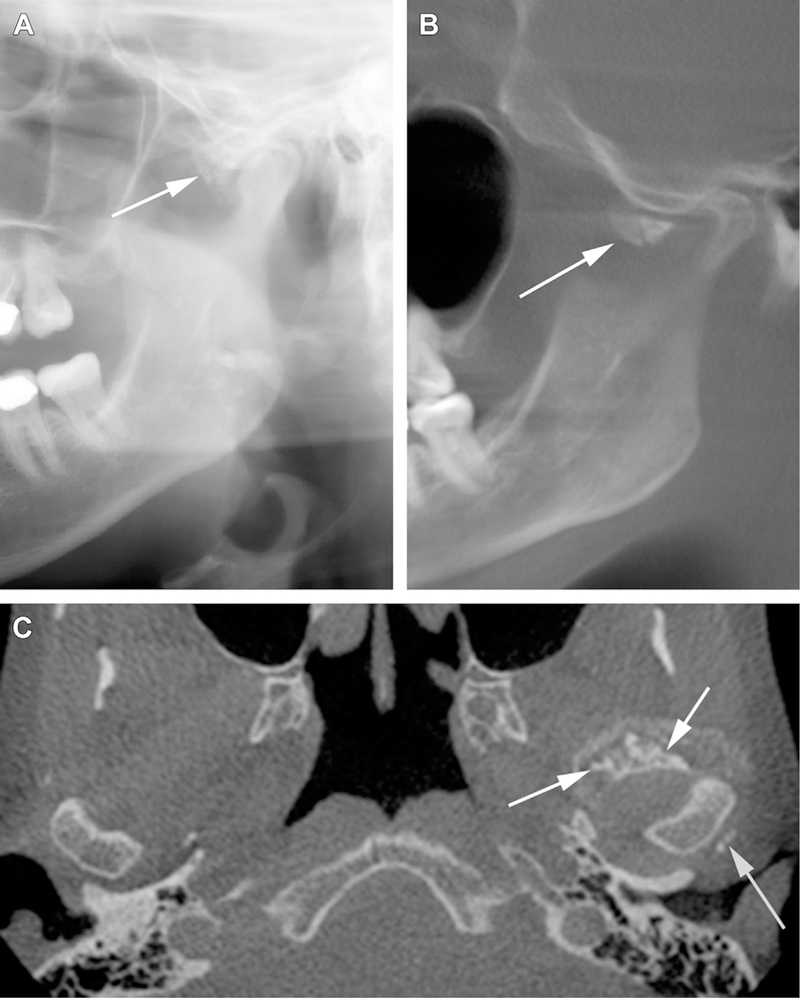
Fig. 4.
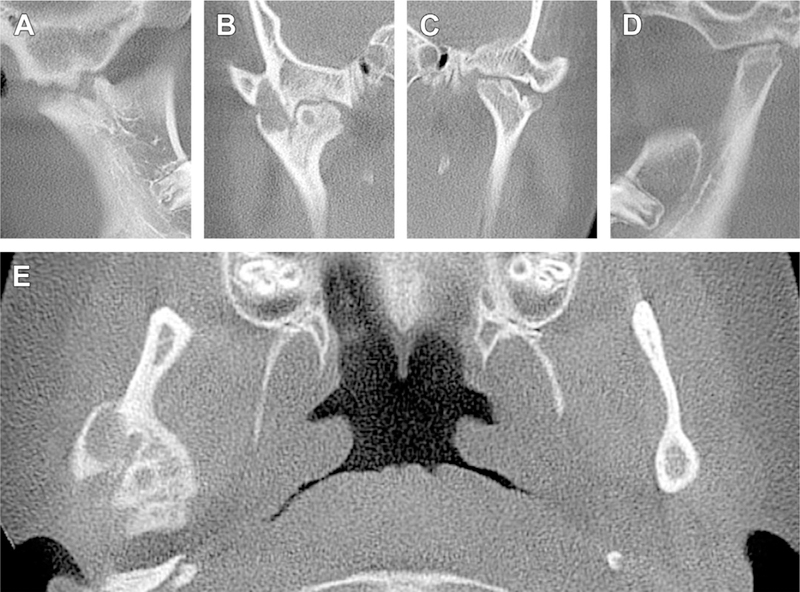
Cone-beam computed tomography of a patient with bilateral involvement with rheumatoid arthritis. (A) Corrected sagittal view of the right joint. Superior margin of the condylar head is irregular. (B) Axially corrected coronal view of the right joint, which shows interdigitation of bony projections that lead to ankylosis of the joint. A subcortical pseudocyst is present in the condylar head. (C, D) Sagittal and coronal sections of the left joint. Superior margin of the left condylar head is irregularly flat and has prominent notching. The articular fossa is also flat. (E) Axial section of the same patient at the level of the right condylar head. Note the excessive enlargement of the right condylar head with subcortical pseudocysts and irregular margins.
SEPTIC (INFECTIOUS) ARTHRITIS
The incidence of arthritis resulting from a specific infection is low when compared with the occurrence of DJD and RA. Until recently, about 40 cases had been reported in the English literature. Leighty and colleagues17 reviewed the existing literature, which showed that most common organism is Staphylococcus aureus. The spread of infection is either directly from a penetrating wound or from hematogenous origin. Cai and colleagues18 reported another 40 patients who were treated in a hospital in China, most of whom had a hematogenous source of infection.
Patients suffering from acute septic arthritis complain chiefly of sudden severe TMJ pain with extreme tenderness on palpation over the joint area or with jaw manipulation. The severe pain typically restricts the motion of the jaw. During the healing process of septic arthritis the joint may undergo osseous or fibrous ankylosis, resulting in severe limitation of motion.
Imaging
Diagnosis of the condition is usually achieved by clinical examination, radiographic evaluation, and aspiration of the fluid in the joint area. A recent study by Gayle and colleagues19 suggested that MRI and contrast-enhanced CT should be acquired to assess for joint effusion, cortical destruction, signs of inflammatory changes, and ankylosis of the joint. These investigators also recommend that a contrast-enhanced CT scan be acquired before joint aspiration.
LOOSE JOINT BODIES
Synovial Chondromatosis
Synovial chondromatosis (Fig. 5) is a rare benign condition whereby nodular cartilaginous or osteocartilaginous entities proliferate in the joint synovium. These entities may become loose from the synovium and continue to grow in size in the joint space. Bilateral synovial chondromatosis is rare. The mean age of patients with synovial chondromatosis is about 45 years, and it is more common in women. Guarda-Nardini and colleagues20 have reported 3 clinical cardinal signs and symptoms of synovial chondromatosis:
Fig. 5.
Synovial chondromatosis of the left temporomandibular joint. (A) Sectional panoramic radiograph shows synovial chondromatosis (arrow) associated with the left temporomandibular joint. (B) Section of a reconstructed panoramic view of a CBCT of the same patient, showing presence of synovial chondromatosis (arrow) at the anterior aspect of the left condylar head. (C) Axial view at the level of the TMJs of the left TMJ. Synovial chondromatosis (arrows) is present at the anterior and posterior margins of the condylar head.
Pain in the preauricular area
Swelling, facial asymmetry, and joint deformity
Limited joint function
Additional signs and symptoms include occlusal changes, ipsilateral posterior open bite, headache, and joint sounds.
Imaging
Panoramic radiographs can demonstrate signs of synovial chondromatosis when the cartilage ossifies. CT and MRI are useful imaging examinations for diagnosis and treatment planning.2,21 MRI displays multiple nodular entities (cartilaginous or osseous), joint effusion, and isointense signal tissues within the joint spaces and capsule.22
Noyek and colleagues23 provided the following radiographic diagnostic criteria for synovial chondromatosis:
Widening of the joint space
Limitation of motion
Irregularity of joint surfaces
Presence of calcified loose bodies (cartilage)
Sclerosis of the glenoid fossa and mandibular condyle
TRAUMATIC DISTURBANCES OF TEMPOROMANDIBULAR JOINTS
Traumatic injuries to the TMJs can be broadly categorized into 3 types: (1) fracture of the TMJ complex, (2) dislocation of the condyle, and (3) ankylosis of the joint.
Fracture of the Temporomandibular Joint Complex
About 17% to 52% of mandibular fractures involve condylar fracture (Fig. 6).24 Condylar fractures may be classified according to the anatomic location: the condylar head (intracapsular), the condylar neck (extracapsular), and the subcondylar region. Condylar fractures may also be classified as nondisplaced, deviated, displaced (typically anterior, medial, or lateral), and dislocated. Another classification is based on the orientation of the fracture line, for example, horizontal, vertical, or compression type.
Fig. 6.

Fracture of the condylar heads. (A) Sectional panoramic radiograph of a fractured condylar head superimposed over the neck of the condyle. The displaced fractured fragment is either on the lateral or medial aspect of the neck. (B) Open-mouth Towne projection showing an example of horizontal fracture of the neck of the condyle that is displaced laterally. (C) Open-mouth Towne projection showing an example of horizontal fracture of the neck of the condyle that is displaced medially. (D) Coronal section from a CBCT, showing bilateral vertical fractures of the condylar heads. (E) Coronal section from a CBCT, showing a vertical and medially displaced fracture of the left condylar head.
Imaging
Initial imaging for screening a suspected trauma to the condylar region should be performed with panoramic radiography.25 A fractured condyle, which is not displaced, may be difficult to detect on a panoramic radiograph. Plain radiographs, such as open-mouth Towne or transorbital views, can provide limited information on the condylar fracture. Cross-sectional imaging with CT or CBCT and 3-dimensional (3D) reconstruction of the fractured region is the imaging modality of choice. To evaluate acute condylar trauma, bilateral sagittal and coronal MR images can provide additional information on disc position, capsular tear, and hemarthrosis.26
Dislocation of the Condyles
Condylar dislocation is primarily of 2 types: anterior or cranial dislocations. Cranial dislocation, whereby the condylar head is dislocated into the cranial fossa because of trauma, is rare. The causative trauma is typically motor vehicle or sports related. Trauma may also dislocate the condylar head posteriorly. Anterior dislocation of the TMJ, which is more common than cranial dislocation, when the head of the condyle moves anteriorly over the articular eminence into such a position that may be returned voluntarily to its normal position by the individual or with assistance. Dislocation of the condyle can be categorized as follows:
Cranial
-
Anterior
Subluxation (self-reducing by the patient)
Luxation (non-self-reducing by the patient; requires assistance)
Habitual
Fracture
Imaging
Panoramic radiography or CT/CBCT has limited diagnostic value for the hypermobility disorders of subluxation, luxation, or individual dislocation of the condylar head, except to identify the location of the condylar head.2 If the patient has chronic pain related to subluxation or luxation, MRI can be acquired to evaluate the status of the disc and the capsule. Cranial or anterior dislocation related to fracture requires CT or CBCT with 3D reconstruction. In addition, MRI should be obtained to evaluate the extent of injury to the brain tissues.
Ankylosis (Hypomobility)
Ankylosis of the TMJ is a disorder whereby adhesion of joint components takes place by fibrous or bony union, resulting in loss of function and movement. The most frequent causes of ankylosis of the TMJ are traumatic injuries, and local or systemic infections. Other causes of ankylosis include systemic disease such as ankylosing spondylitis, RA, psoriasis, or previous TMJ surgery. Bilateral ankylosis is often a result of RA.
In 1986 Sawheny classified ankylosis of the TMJ into 4 different types27:
Type I. The condylar head is flattened or deformed. Presence of fibrous adhesion makes movement impossible.
Type II. The condylar head is deformed and a small bony adhesion exists between the condyle and articular fossa. The articular surfaces are mostly well defined.
Type III. A bony bridge extends from the ramus to the zygomatic arch. On the medial aspect, atrophic and displaced condylar head is still present. The articular surface of the fossa is intact. The articular disc is also probably intact.
Type IV. The architecture of the joint is lost because of a bony bridge extending from the ramus to the temporal bone.
A simpler classification of TMJ ankylosis identifies 2 types: intra-articular ankylosis and extra-articular ankylosis. In intra-articular ankylosis, the joint undergoes progressive destruction of the meniscus with flattening of the mandibular fossa, thickening of the head of the condyle, and narrowing of the joint space. This type of ankylosis is basically fibrous, although ossification in the scar may result in a bony union. Extra-articular ankylosis results in a “splinting” of the TMJ by a fibrous or bony mass external to the joint proper, as in cases of infection in surrounding bone or extensive tissue destruction and scarring.
Ankylosis of the joint occurs at any age, but most cases occur before the age of 10 years. Distribution is approximately equal between the genders. The individual may or may not be able to open the mouth to any appreciable extent, depending on the type of ankylosis. In complete ankylosis, bony fusions will absolutely limit movement. There is usually somewhat greater motion in fibrous ankylosis than in bony ankylosis.
Imaging
Panoramic radiography has a limited role in detecting ankylosis. Fibrous ankylosis is better evaluated using MRI. In fibrous ankylosis, the joint space is often limited. The articulating surfaces of the condyle and the fossa may be irregular. Irregular surfaces appear to interdigitate in a locking fashion. In bony ankylosis, a bony bridge exists from the condylar head to the articular fossa. CT or CBCT is the imaging modality of choice in detecting osseous ankylosis.2
DEVELOPMENT DISTURBANCES OF TEMPOROMANDIBULAR JOINT
At the time of birth, the TMJs are incompletely formed. Therefore, developmental disturbance to the TMJ can occur either before or after birth. Kaneyama and colleagues28 have classified developmental disturbances as follows:
- Hypoplasia or aplasia of the condyle
- Congenital or primary hypoplasia or aplasia
- Acquired or secondary hypoplasia or aplasia
Condylar hyperplasia
Bifid condyle
Condylar Hypoplasia or Aplasia
Condylar aplasia is failure of development of the mandibular condyle, and condylar hypoplasia is underdevelopment of the condyle. Aplasia or hypoplasia may be congenital or acquired, and may occur unilaterally or bilaterally (Fig. 7).
Fig. 7.
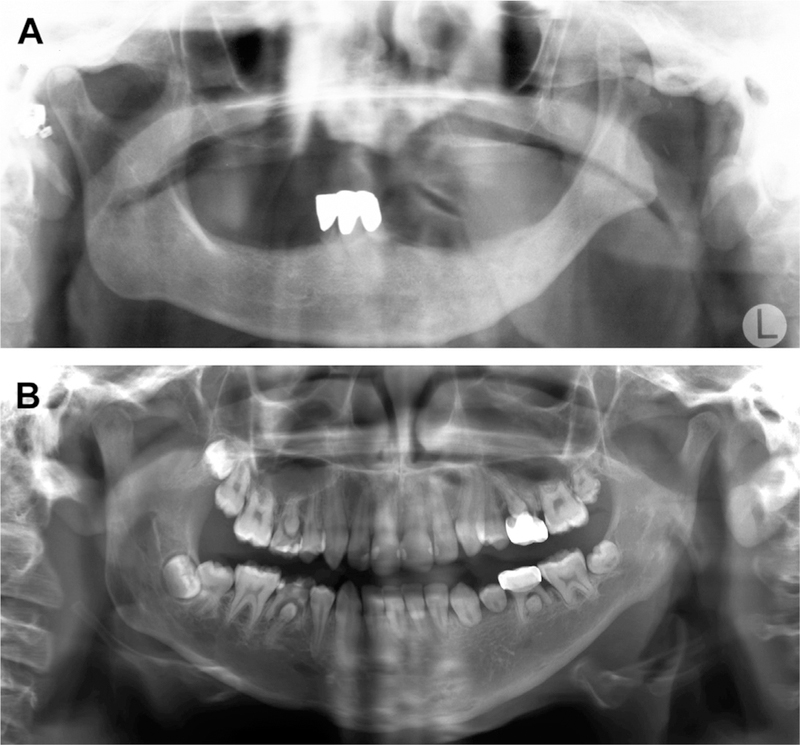
Aplasia or hypoplasia of the condyle. (A) An 85-year-old woman whose left condylar head and ramus are aplastic because of an osteomyelitis that had affected her left mandible when she was 10 years old. (B) Example of hypoplasia of the left condyle and ramus caused by childhood treatment with radiation therapy. Note multiple teeth with stunted roots as a result from the radiation therapy.
Congenital, or primary, hypoplasia or aplasia is characterized by unilateral or bilateral underdevelopment or absence of the condyle, usually caused by disturbances in the first or second branchial arches. Conditions that show congenital hypoplasia or aplasia include Treacher-Collins syndrome, oculo-auriculo-vertebral syndrome, hemifacial macrosomia, Pierre-Robin sequence, and Hurler syndrome. In congenital variety, both the joints are usually affected but the primary clinical finding may be unilateral.
The acquired or secondary form of hypoplasia may be due to any agent that interferes with the normal development of the condyle. Local causes that may initiate condylar hypoplasia include trauma, infection of the mandible or middle ear, and therapeutic doses of radiation.
Imaging
Initial imaging may be limited to plain films and panoramic radiography. Xi and colleagues29 demonstrated that CBCT and 3D reconstruction of the CBCT data provide an invaluable diagnostic advantage over conventional radiography for treatment planning and follow-up. A series of lateral cephalometric radiographs acquired over a period of time also provides information on the progression of the disease.2
Hyperplasia of Mandibular Condyle
Condylar hyperplasia or hyperactivity is a rare unilateral enlargement of the condyle. Although the cause of this condition is unknown, it has been suggested that mild chronic inflammation, resulting in a condition analogous to a proliferative osteomyelitis, stimulates the growth of the condyle or adjacent tissues. The unilateral occurrence strongly suggests a local phenomenon. Obewegeser and Makek30 have classified condylar hyperplasia into 3 categories.
Type A is hemimandibular hyperplasia, causing asymmetry in the vertical plane. In this type the growth is unilateral in the vertical plane, with minimal deviation of the chin. Typically the maxilla shows compensatory growth. In the absence of maxillary growth, an open bite may be present on the same side.
Type B is hemimandibular elongation causing asymmetry in the transverse plane. In this type the chin is deviated toward the contralateral side with no vertical asymmetry. Cross-bite may be present.
Type C is a combination of types A and B, and exhibits hyperplastic features unilaterally or bilaterally.
Imaging
Diagnosis of condylar hyperplasia is made by a combination of clinical and radiographic findings. The patients usually exhibit a unilateral, slowly progressive elongation of the face with deviation of the chin away from the affected side. The enlarged condyle may be clinically evident or, at least, palpated. Condylar hyperplasia presents a striking radiographic appearance in both coronal and sagittal views. Panoramic radiography31 may be used as an initial imaging method for identifying condylar hyperplasia, but for quantitative evaluation and follow-up, 3D imaging using CT or CBCT is necessary (Fig. 8).32 Differential diagnosis includes osteochondroma.
Fig. 8.
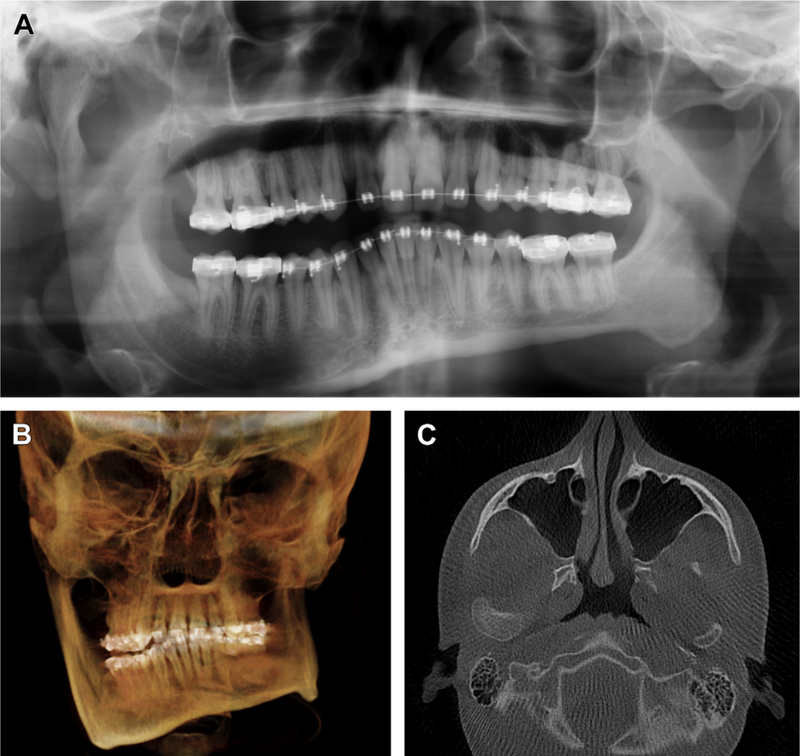
(A) Panoramic radiograph showing unilateral hyperplasia of the right condyle and right ramus. (B) Three-dimensional reconstruction of CBCT data of the same patient, showing significant facial asymmetry and right-sided posterior open bite. (C) Axial section of the same patient, showing significant hyperplasia of the right condyle in comparison with the left.
Bifid Condyle
Bifid condyle, which is usually an incidental finding on radiographic examination, is characterized by a varying depth of a groove or depression around the midline of the condylar head. A deep groove may result in an appearance of duplicity of the condylar head. Usually bifidity is unilateral, although bilateral bifid condyles, a rare condition that affects less than 1% of the population, have been reported.28 However, Miloglu and colleagues33 suspect that the incidence of bifid condyles is underreported. Even rarer are trifid condyles. The etiology of bifidity is controversial, although several theories have been proposed.34 One theory speculates that bifidity may originate in the embryo, where blood supply to the condylar head is limited. Another theory suggests microtrauma or trauma being the cause of bifidity, due to either birth trauma or transcoronal fracture of the condylar head. Others have suggested that radiotherapy, infection, or systemic factors such as endocrine disorders and genetic factors play a role in bifidity of the condyle.
Imaging
Although panoramic radiographs may be used to evaluate the presence of bifid condyle,33 such depression is better detected on CT coronal or sagittal orientation of a cross-sectional imaging and 3D reconstruction (Fig. 9).35
Fig. 9.
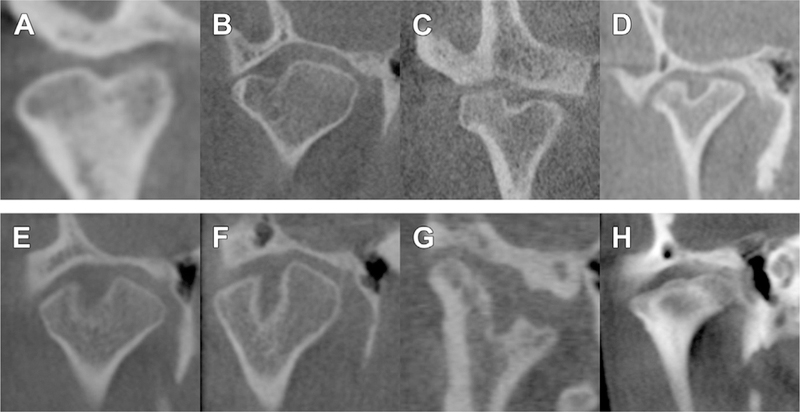
Axially corrected coronal views of condyles showing examples of bifidity. (A–G) Bifid condyles may have slight midline depression to almost a duplication of the condylar head. (H) Mild trifid appearance of the condylar head.
SUMMARY
TMD is the second most common chronic musculoskeletal condition after chronic low back pain.1 As pain-related TMD can affect an individual’s daily activities, psychosocial functioning, and quality of life, it is important to accurately diagnose these complex musculoskeletal disorders to provide the best clinical care. The new dual-axis DC/TMD offers an evidence-based assessment protocol for the clinician to use when screening patients for TMJ intra-articular disorders, although imaging is typically needed for a definitive diagnosis. Both clinical history and examination, augmented as indicated with imaging, are needed to render proper TMJ intra-articular diagnoses. As several imaging modalities recommended in this article use ionizing radiation, careful clinical assessment with due consideration of the benefit to the patient must be carried out before ordering any imaging.
KEY POINTS.
Temporomandibular disorder is the second most common chronic musculoskeletal condition after chronic low back pain. As pain-related TMD can affect an individual’s daily activities, psychosocial functioning, and quality of life, it is important to accurately diagnose these complex musculoskeletal disorders to provide the best clinical care.
The new dual-axis diagnostic criteria for TMD offers an evidence-based assessment protocol for the clinician to use when screening patients for temporomandibular joint (TMJ) intra-articular disorders, but imaging is typically needed for a definite diagnosis.
Both clinical history and examination, augmented as indicated with imaging, are needed to render proper tMj intra-articular diagnoses. As several imaging modalities recommended in this article use ionizing radiation, careful clinical assessment with due consideration of the benefit to the patient must be carried out before ordering any imaging.
ACKNOWLEDGMENTS
Research funded by NIH/NIDCR U01DE013331 and U01DE019784.
REFERENCES
- 1.Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and orofacial pain special interest group†. J Oral Facial Pain Headache 2014;28(1):6–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Peck CC, Goulet JP, Lobbezoo F, et al. Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J Oral Rehabil 2014;41(1):2–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Plesh O, Adams SH, Gansky SA. Temporomandibular joint and muscle disordertype pain and comorbid pains in a national US sample. J Orofac Pain 2011;25(3): 190–8. [PMC free article] [PubMed] [Google Scholar]
- 4.Hunter A, Kalathingal S. Diagnostic imaging for temporomandibular disorders and orofacial pain. Dent Clin North Am 2013;57(3):405–18. [DOI] [PubMed] [Google Scholar]
- 5.Ahmad M, Hollender L, Anderson Q, et al. Research diagnostic criteria for temporomandibular disorders (RDC/TMD): development of image analysis criteria and examiner reliability for image analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107(6):844–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barkin S, Weinberg S. Internal derangements of the temporomandibular joint: the role of arthroscopic surgery and arthrocentesis. J Can Dent Assoc 2000;66(4): 199–203. [PubMed] [Google Scholar]
- 7.Wilkes CH. Internal derangements of the temporomandibular joint. Pathological variations. Arch Otolaryngol Head Neck Surg 1989;115(4):469–77. [DOI] [PubMed] [Google Scholar]
- 8.Haiter-Neto F, Hollender L, Barclay P, et al. Disk position and the bilaminar zone of the temporomandibular joint in asymptomatic young individuals by magnetic resonance imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 94(3):372–8. [DOI] [PubMed] [Google Scholar]
- 9.Tanaka E, Detamore MS, Mercuri LG. Degenerative disorders of the temporomandibular joint: etiology, diagnosis, and treatment. J Dent Res 2008;87(4):296–307. [DOI] [PubMed] [Google Scholar]
- 10.Larheim TA, Abrahamsson AK, Kristensen M, et al. Temporomandibular joint diagnostics using CBCT. Dentomaxillofac Radiol 2015;44(1):20140235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Alkhader M, Ohbayashi N, Tetsumura A, et al. Diagnostic performance of magnetic resonance imaging for detecting osseous abnormalities of the temporomandibular joint and its correlation with cone beam computed tomography. Dentomaxillofac Radiol 2010;39(5):270–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Koos B, Tzaribachev N, Bott S, et al. Classification of temporomandibular joint erosion, arthritis, and inflammation in patients with juvenile idiopathic arthritis. J Orofac Orthop 2013;74(6):506–19. [DOI] [PubMed] [Google Scholar]
- 13.Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010;62(9):2569–81. [DOI] [PubMed] [Google Scholar]
- 14.Helenius LM, Hallikainen D, Helenius I, et al. Clinical and radiographic findings of the temporomandibular joint in patients with various rheumatic diseases. A case-control study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99(4):455–63. [DOI] [PubMed] [Google Scholar]
- 15.Goupille P, Fouquet B, Valat JP. Computed tomography of the temporomandibular joint in rheumatoid arthritis. J Rheumatol 1992;19(8):1315–6. [PubMed] [Google Scholar]
- 16.Kretapirom K, Okochi K, Nakamura S, et al. MRI characteristics of rheumatoid arthritis in the temporomandibular joint. Dentomaxillofac Radiol 2013;42(4): 31627230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Leighty SM, Spach DH, Myall RW, et al. Septic arthritis of the temporomandibular joint: review of the literature and report of two cases in children. Int J Oral Maxillofac Surg 1993;22(5):292–7. [DOI] [PubMed] [Google Scholar]
- 18.Cai XY, Yang C, Zhang ZY, et al. Septic arthritis of the temporomandibular joint: a retrospective review of 40 cases. J Oral Maxillofac Surg 2010;68(4):731–8. [DOI] [PubMed] [Google Scholar]
- 19.Gayle EA, Young SM, McKenna SJ, et al. Septic arthritis of the temporomandibular joint: case reports and review of the literature. J Emerg Med 2013;45(5):674–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Guarda-Nardini L, Piccotti F, Ferronato G, et al. Synovial chondromatosis of the temporomandibular joint: a case description with systematic literature review. Int J Oral Maxillofac Surg 2010;39(8):745–55. [DOI] [PubMed] [Google Scholar]
- 21.Miyamoto H, Sakashita H, Wilson DF, et al. Synovial chondromatosis of the temporomandibular joint. Br J Oral Maxillofac Surg 2000;38(3):205–8. [DOI] [PubMed] [Google Scholar]
- 22.Wang P, Tian Z, Yang J, et al. Synovial chondromatosis of the temporomandibular joint: MRI findings with pathological comparison. Dentomaxillofac Radiol 2012; 41(2):110–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Noyek AM, Holgate RC, Fireman SM, et al. The radiologic findings in synovial chondromatosis (chondrometaplasia) of the temporomandibular joint. J Otolaryngol Suppl 1977;3:45–8. [PubMed] [Google Scholar]
- 24.Zachariades N, Mezitis M, Mourouzis C, et al. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment and proposals. J Craniomaxillofac Surg 2006;34(7):421–32. [DOI] [PubMed] [Google Scholar]
- 25.Chrcanovic BR. Open versus closed reduction: diacapitular fractures of the mandibular condyle. Oral Maxillofac Surg 2012;16(3):257–65. [DOI] [PubMed] [Google Scholar]
- 26.Gerhard S, Ennemoser T, Rudisch A, et al. Condylar injury: magnetic resonance imaging findings of temporomandibular joint soft-tissue changes. Int J Oral Maxillofac Surg 2007;36(3):214–8. [DOI] [PubMed] [Google Scholar]
- 27.Sawhney CP. Bony ankylosis of the temporomandibular joint: follow-up of 70 patients treated with arthroplasty and acrylic spacer interposition. Plast Reconstr Surg 1986;77(1):29–40. [PubMed] [Google Scholar]
- 28.Kaneyama K, Segami N, Hatta T. Congenital deformities and developmental abnormalities of the mandibular condyle in the temporomandibular joint. Congenit Anom (Kyoto) 2008;48(3):118–25. [DOI] [PubMed] [Google Scholar]
- 29.Xi T, Schreurs R, van Loon B, et al. 3D analysis of condylar remodelling and skeletal relapse following bilateral sagittal split advancement osteotomies. J Craniomaxillofac Surg 2015;43(4):462–8. [DOI] [PubMed] [Google Scholar]
- 30.Obwegeser HL, Makek MS. Hemimandibular hyperplasia-hemimandibular elongation. J Maxillofac Surg 1986;14(4):183–208. [DOI] [PubMed] [Google Scholar]
- 31.Kjellberg H, Ekestubbe A, Kiliaridis S, et al. Condylar height on panoramic radiographs. A methodologic study with a clinical application. Acta Odontol Scand 1994;52(1):43–50. [DOI] [PubMed] [Google Scholar]
- 32.Nolte JW, Karssemakers LH, Grootendorst DC, et al. Panoramic imaging is not suitable for quantitative evaluation, classification, and follow up in unilateral condylar hyperplasia. Br J Oral Maxillofac Surg 2015;53(5):446–50. [DOI] [PubMed] [Google Scholar]
- 33.Miloglu O, Yalcin E, Buyukkurt M, et al. The frequency of bifid mandibular condyle in a Turkish patient population. Dentomaxillofac Radiol 2010;39(1):42–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sala-Perez S, Vazquez-Delgado E, Rodriguez-Baeza A, et al. Bifid mandibular condyle: a disorder in its own right? J Am Dent Assoc 2010;141(9):1076–85. [DOI] [PubMed] [Google Scholar]
- 35.Tanner JM, Friedlander AH, Chang TI. Bilateral bifid mandibular condyles diagnosed with three-dimensional reconstruction. Dentomaxillofac Radiol 2012; 41(8):691–5. [DOI] [PMC free article] [PubMed] [Google Scholar]