

Abstract
Background
Dogs with immune‐mediated disease are often coadministered glucocorticoids and aspirin, but ulcerogenic effects of current protocols are unknown.
Objectives
To compare gastrointestinal changes among dogs administered aspirin, prednisone, and combination treatment.
Animals
Twenty‐four healthy research dogs.
Methods
Double‐blinded, placebo‐controlled randomized trial of dogs administered placebo, aspirin (2 mg/kg q24h), prednisone (2 mg/kg q24h), or combination treatment PO for 28 days. Clinical signs were recorded daily, with laboratory work performed at baseline and day 28. Gastrointestinal mucosal hemorrhages, erosions, and ulcers were numerated for endoscopic studies performed on days 0, 14, and 28; endoscopic mucosal lesion scores were calculated. Results were compared using mixed model repeated‐measures analyses of variance and generalized estimating equation proportional odds models. P < .05 was considered significant.
Results
Gastric mucosal lesion scores differed by treatment‐by‐time (F[6, 40] = 4.4, P = .002), treatment (F[3, 20] = 7.1, P = .002), and time (F[2, 40] = 18.9, P < .001). Post hoc analysis revealed increased scores in the aspirin (day 14 only), prednisone, and prednisone/aspirin groups during treatment. Ulcers were identified on 14 studies, representing 10 dogs. Dogs receiving prednisone and prednisone/aspirin had 11.1 times (95% CI, 1.7‐73.6) and 31.5 times (95% CI, 3.5‐288.0) higher odds, respectively, of having endoscopic mucosal lesion scores ≥4 than dogs receiving placebo (P ≤ .01).
Conclusions and Clinical Importance
Gastrointestinal bleeding occurs commonly in dogs administered aspirin, prednisone, or prednisone/aspirin treatment, with higher lesion scores for dogs receiving combination treatment. Even severe lesions are not accompanied by clinical signs.
Keywords: antiplatelet, corticosteroid, gastrointestinal bleeding, glucocorticoid, thromboprophylaxis, ulcer
Abbreviations
- GI
gastrointestinal
- IMHA
immune‐mediated hemolytic anemia
- MCS
muscle condition score
1. INTRODUCTION
Both sustained glucocorticoid and low‐dose aspirin treatment are associated with gastrointestinal (GI) bleeding in people.1, 2, 3, 4, 5 The use of other nonsteroidal medications in combination with prednisolone also causes GI bleeding in dogs.6, 7 A study using an aspirin dose of 0.5 mg/kg q24h finds no significant difference in endoscopically identified gastric mucosal lesions between healthy dogs administered prednisone alone and prednisone with aspirin.8 However, the use of an aspirin dose that achieves consistent antiplatelet effects might increase GI bleeding due to additive inhibition of prostaglandin formation and potential local effects on the gastric mucosa. Although dogs often are asymptomatic in the presence of aspirin‐induced GI bleeding,8, 9 GI bleeding could increase the risk of a negative outcome, as it has been associated with increased risk of thromboembolism and death in people.10
The purpose of this randomized‐controlled double‐blinded study was to characterize clinical, clinicopathologic, and endoscopic changes in healthy dogs receiving sustained placebo, aspirin (2 mg/kg q24h), prednisone (2 mg/kg q24h), or combination aspirin and prednisone treatment. Our hypothesis was that sustained administration of aspirin, used singly or in combination with prednisone (2 mg/kg q24h), would induce GI bleeding, and injury would be greater for dogs that receive combination treatment than for dogs receiving prednisone alone.
2. MATERIALS AND METHODS
2.1. Study population
Twenty‐four healthy dogs from the College's teaching and research colony were enrolled in the study. The study protocol was approved by the Institutional Animal Care and Use Committee at the University of Tennessee, College of Veterinary Medicine (protocol number 2283) and performed in compliance with “The Guide for the Care and Use of Laboratory Animals” in laboratory animal facilities that are AAALAC certified and exceed NIH standards of care.
Sample size calculation was performed using preliminary data.11, 12 In those studies, endoscopic mucosal lesion scores13 increased from 5 to 15 for dogs receiving 2 mg/kg q24h prednisone with 1 mg/kg q24h aspirin. Based on those results and assuming a standard deviation of 4.9, enrollment of 6 dogs per group was calculated to have 85% power to find endoscopic scores of 5 and 15 significantly different with an alpha of .05. In contrast to prior work,14 mucosal lesion scores also increased in dogs administered prednisone alone. Dogs in the prior report were substantially younger than dogs in our pilot evaluation, potentially suggesting increasing sensitivity to the ulcerogenic effects of glucocorticoids with age. Thus, dogs were stratified by age before randomization to 1 of 4 groups using a random number sequence generator (https://www.random.org, accessed May 16, 2017). Because gastric biopsies taken from all dogs at the conclusion of baseline were positive for urease producing bacteria (see below), stratification based on urease status was not necessary.
2.2. Treatment groups
The treatment groups were (1) placebo, (2) aspirin plus placebo, (3) prednisone plus placebo, and (4) prednisone plus aspirin. Dogs in the placebo group received 2 placebo capsules once daily, whereas dogs in groups 2 and 3 were administered 1 placebo capsule. Aspirin was administered at a dosage of 2 mg/kg q24h. Commercially available aspirin tablets (Rugby Laboratories, Livonia, Michigan) were compounded into capsules by the College's pharmacy using the standards for compounding provided by the United States Pharmacopeia. Prednisone was administered at a dosage of 2 mg/kg q24h using commercially available prednisone tablets (West‐Ward Pharmaceuticals Corp, Eatentown, New Jersey). Lactose‐containing gelatin capsules (LetCo Medical, Decatur, Alabama) were assembled by the College's pharmacy for use as placebos. All treatments were administered in small meatballs once daily before feeding by an individual blinded to the individual treatments and groups but not endoscopic findings.
2.3. Study periods
The study was comprised of 3 periods: acclimation (days −13 to −7), baseline (days −6 to 0), and treatment (days 1‐28). During the acclimation period, dogs were administered fenbendazole (50 mg/kg q24h, PO, days −13 to −9) and ivermectin (200 μg/kg SC once, day −13). As part of routine colony prophylaxis, dogs also received imidacloprid and moxidectin (Advantage Multi for dogs; Bayer HealthCare, LLC, Shawnee Mission, Kansas), dosed per manufacturer's instructions.
All dogs received water ad libitum and were fed a commercial kibble once daily in quantities sufficient to maintain ideal body condition. An observer not associated with the study and blinded to the treatment groups, medications, and all study‐related findings collected observations twice daily throughout the study (days −13 to 28). Attitude was characterized as normal or abnormal. Food intake was recorded to the nearest quartile consumed (0%, 25%, 50%, or 100%). The presence of vomiting, melena, or hematochezia was recorded, and feces were scored using a standard scale.15
2.4. Diagnostic testing
Dogs were confirmed to have negative fecal direct smears and fecal flotations (sugar and zinc sulfate) during the acclimation period (days −13 to −11). Clinicopathologic testing was performed at the conclusion of baseline and treatment by a commercial diagnostic laboratory (Antech Diagnostics, Fountain Valley, California). Testing included CBCs, serum biochemical profiles with lipase activity (PrecisionPSL; Antech Diagnostics), urinalyses, and urine protein:creatinine ratios.
Dogs were anesthetized on days 0, 14, and 28 for performance of esophagogastroduodenoscopy. Dogs were premedicated with acepromazine (.02 mg/kg SC) and butorphanol (.4 mg/kg SC) after which IV catheters were placed, and dogs were induced using propofol (3‐6 mg/kg IV to effect). Dogs were intubated, and general anesthesia was maintained with isoflurane administered in oxygen. Crystalloid fluids were administered at a rate of 10 mL/kg/h IV. Dogs then were positioned in left lateral recumbency.
Esophagogastroduodenoscopy was performed by a single individual (J.C.W.), blinded to each dog's treatment group, using a standardized technique to avoid creation of iatrogenic lesions.8, 13 Briefly, endoscopic exploration was performed under continuous visual guidance from the upper esophageal sphincter through the duodenum. Within the stomach, the gastric body, antrum/pylorus, angularis incisura, and cardia were individually interrogated before pyloric intubation for duodenal evaluation. Endoscopic explorations were recorded using a digital capture system, with still images collected of the lower esophageal sphincter, gastric body, angularis incisura, antrum and pylorus, cardia, and duodenum. Supplementary images of focal abnormalities also were collected. Endoscopic evaluations were anonymized after data collection to blind investigators to dog, treatment group, and time point. Gastric biopsies taken on day 0 were incubated in urease media to assess for the presence of potential Helicobacter spp.
2.5. Endoscopic scoring
Two investigators (J.T., J.C.W.) independently evaluated each endoscopic study. Hemorrhages, punctate erosions, invasive erosions, and ulcers were numerated for the esophagus, each region of the stomach (gastric body, pyloric antrum, angularis incisura, and cardia), and duodenum.6, 8 Hemorrhages were defined as reddened areas with intact mucosa. Pinhead‐sized or smaller discontinuations in the mucosa were classified as punctate erosions, whereas discontinuations greater than a pinhead in size or with detectable depth were classified as invasive erosions. Lesions with wide mucosal defects and craterous centers were classified as ulcers. If >25 lesions were identified in an anatomic region, lesions were recorded as 26‐50, 51‐100, 100‐200, or >200 to avoid erroneous quantitation. For statistical analysis, lesions >25 but ≤200 were entered according to the midpoint of the categorical range (eg, 26‐50 was entered as 37.5, and so on). When >200 lesions were identified, a value of 201 was assigned.
To optimize consistency in endoscopic evaluation given high reported interindividual variation in endoscopic interpretation,16 investigators independently evaluated 10 videos and still images of 10 GI endoscopies unrelated to this study 4 months after completion of data collection. Studies were selected to represent a range of GI disease, from normal to severe GI bleeding, by 1 investigator (J.C.W.) before the start of the study. After datasheets from the individual investigators were merged, the combined database was reviewed for areas of discordance. Each investigator then independently reevaluated studies with discordant scores and corrected any self‐identified errors in scoring or data entry. Finally, the 2 investigators reviewed the studies together to address areas of disagreement and reach consensus in differentiation among lesion types.
Anonymized endoscopic evaluations for this study were independently scored thereafter (approximately 6 months after completion of data collection). After datasheets from the individual investigators were merged, the combined database was reviewed for areas of discordance. Each investigator then independently reevaluated studies with discordant scores and corrected any self‐identified errors in scoring or data entry. Results of these studies were not reviewed together to achieve consensus. Instead, the mean of lesions numerated by each of the 2 investigators was used for analyses. Total gastric mucosal endoscopic lesion scores were calculated based on mean lesion counts using the Forsyth scoring system.6
2.6. Statistical and data analysis
Descriptive statistics were generated for relevant clinical, clinicopathologic, and endoscopic variables. Samples were analyzed for normality using the Shapiro‐Wilk test and for the presence of outliers using box‐and‐whisker plots.
Mean food intake, days of vomiting, and mean fecal score were determined for each study period. Clinicopathologic variables recorded were hematocrit and platelet count; albumin and blood urea nitrogen (BUN) concentrations; BUN:creatinine and urine protein:creatinine ratios; activities of alkaline phosphatase (ALP), gamma‐glutamyl transferase (GGT), amylase, and lipase; and urine‐specific gravity.
Selected clinical, clinicopathologic, and endoscopic data were compared between treatment groups using mixed model, split‐plot repeated‐measures analyses of variance that included fixed effects of treatment, time, and treatment‐by‐time interaction. The repeated measure of time was accounted for in a repeated statement. Dog nested within treatment group was included as a random effect. Fisher's least significant difference was used to perform post hoc analyses. The Shapiro‐Wilk test of normality and QQ plots of the residuals were evaluated for each marker to confirm the assumption of normally distributed residuals had been met. Model assumptions regarding equality of variances were verified with Levene's Test for equality of variances. Differences in marginal means were determined for markers with significant main effects or interaction terms. Non‐normally distributed data were logarithmically or rank‐transformed, as necessary, to meet underlying statistical assumptions. If logarithmic transformation was required, 0.05 was added to all values. Due its infrequent occurrence, mixed model analysis could not be performed for ulceration. The relative odds of having a total endoscopic mucosal lesion score ≥4 (eg, >25 hemorrhages or punctate erosions, ≥1 invasive erosion, and/or ≥1 ulcer) was determined using a repeated‐measures generalized estimating equation proportional odds model with a binomial distribution and a logit link function. After data analysis revealed a lack of association between hemorrhages and group or time point (see Results), hemorrhages were excluded from lesion scores in order to increase precision of the results.
Commercial statistical software packages (MedCalc 15.8 MedCalc Software, Ostend, Belgium; SAS 9.4 release TS1M5, SAS Institute Inc, Cary, North Carolina) were used for all analyses. P < .05 was considered significant.
3. RESULTS
3.1. Study population
Baseline demographics of the 4 treatment groups are summarized in Table 1. Attitude was categorized as normal on all days for all dogs. There was no significant difference in food intake or body condition score among groups over time. All but 3 dogs had a muscle condition score (MCS) of 3 at all time points. One dog in the aspirin group had an MCS of 2 at all time points. Two dogs (aspirin, 1; prednisone, 1) had MCSs of 3 at baseline but 2 on day 28. Six dogs vomited at least once during the study, representing 2 dogs each in the placebo, aspirin, and prednisone/aspirin groups. No dog in the prednisone group experienced vomiting. Vomiting was noted once during baseline for 3 dogs (1, placebo; 2, prednisone/aspirin). During the treatment period, vomiting was recorded on 1 day for 3 dogs (1, aspirin; 2, prednisone/aspirin), on 2 days for 1 dog (aspirin), and on 3 days for 1 dog (placebo). Neither hematemesis or melena nor hematochezia occurred during the study. No dog developed diarrhea, and fecal scores did not differ among groups over time.
Table 1.
Baseline demographics of dogs stratified by age then randomized to receive placebo, aspirin with placebo, prednisone with placebo, or a combination of prednisone and aspirin for 28 days
| Placebo | Aspirin | Prednisone | Prednisone and aspirin | |
|---|---|---|---|---|
| Age (y) | 3.5 (2‐6) | 3.5 (2‐7) | 3.0 (2‐6) | 3.5 (2‐7) |
| Sex | ||||
| Intact female | 3 | 2 | 2 | 2 |
| Female spayed | 0 | 0 | 0 | 0 |
| Intact male | 1 | 2 | 2 | 3 |
| Male castrated | 2 | 2 | 2 | 1 |
| Breed | 3 Beagles, 3 Hounds | 4 Beagles, 2 Hounds | 4 Beagles, 2 Hounds | 4 Beagles, 2 Hounds |
| Weight (kg) | 14.2 ± 3.1 | 15.8 ± 7.1 | 15.2 ± 6.1 | 20.9 ± 9.9 |
| Body condition score | 6 (5‐8) | 6 (4–8) | 6 (5–9) | 7 (5‐8) |
| Muscle condition score | 3 (NA) | 3 (2–3) | 3 (NA) | 3 (NA) |
Age, body condition score, and muscle condition score are presented as median (range). Weight is presented as mean ± SD.
Abbreviation: NA, not applicable.
3.2. Clinicopathologic data
Selected baseline and post‐treatment clinicopathologic results are presented in Table 2. One dog in the prednisone group had a mildly low platelet count (143,000 platelets/μL) at baseline, but platelet clumping was noted. Both manual review and a repeat platelet count the next day yielded platelet counts within the reference interval. Results of CBCs otherwise were unremarkable for all dogs. Results for biochemical analytes also were within reference intervals at both time points for the majority of dogs. Logarithmic transformation was required before statistical analysis for ALP and lipase activity, creatinine concentration, and urine protein:creatinine ratio, whereas rank transformation was required before analysis of GGT activity and BUN concentration.
Table 2.
Selected clinicopathologic results for 24 healthy research dogs administered placebo, aspirin with placebo, prednisone with placebo, or a combination of prednisone and aspirin for 28 days
| RI | Placebo | Aspirin | Prednisone | Prednisone and aspirin | |||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Day 28 | Baseline | Day 28 | Baseline | Day 28 | Baseline | Day 28 | ||
| Amylase (IU/L) | 290‐1125 | 435ABC (316‐762) | 544A (363‐852) | 476AB (355‐854) | 391ABC (326‐708) | 409AB (310‐950) | 245C (225‐509) | 524A (395‐848) | 354BC (264‐458) |
| Albumin (g/dL) | 2.7‐4.4 | 3.8ABC (3.3‐4.2) | 3.7ABC (3.5‐4.1) | 3.8ABC (3.1‐3.9) | 3.6ABC (3.4‐3.7) | 3.5BD (3.3‐3.9) | 4AC (3.3‐4.2) | 3.6CD (3.2‐3.9) | 4.1AB (3.4‐4.1) |
| ALP (IU/L) | 5‐131 | 24B (18‐34) | 26B (19‐42) | 32B (20‐34) | 40B (23‐67) | 32B (26‐91) | 103A (48‐161) | 25B (15‐47) | 124A (42‐509) |
| GGT (IU/L) | 1‐12 | 5* (4‐8) | 7* (5‐7) | 6* (4‐7) | 5* (1‐7) | 5* (5‐7) | 8* (6‐10) | 5* (3‐12) | 9* (4‐24) |
| BUN (mg/dL) | 6‐31 | 12 (8‐36) | 14.5 (9‐20) | 12 (10‐21) | 13.5 (11‐23) | 18 (10‐20) | 17.5 (13‐22) | 13 (11‐14) | 15 (11‐19) |
| Creatinine (mg/dL) | 0.5‐1.6 | 0.8ABC (0.7‐1.4) | 0.7CDE (0.6‐0.9) | 0.8ADC (0.7‐1.1) | 0.8BCD (0.6‐1.1) | 1A (0.8‐1.4) | 0.7DE (0.6‐0.7) | 0.9AB (0.6‐1.5) | 0.6E (0.5‐0.7) |
| BUN:creatinine ratio | 4‐27 | 16BC (11‐26) | 20.5B (13‐27) | 16BC (13‐19) | 18BC (14‐28) | 15.5A (13‐19) | 27BC (22‐31) | 15C (7‐20) | 27A (22‐28) |
| Hematocrit (%) | 36‐60 | 55* (46‐63) | 53* (48‐62) | 54* (48‐59) | 53* (44‐59) | 54* (48‐57) | 49* (43‐54) | 48* (42‐64) | 44* (37‐56) |
| Lipase (U/L) | 24‐140 | 40.5* (16‐100) | 51.5* (18‐346) | 42* (20‐88) | 40.5* (27‐170) | 45.5* (29‐120) | 95.5* (38‐177) | 35.5* (16‐114) | 114* (21‐254) |
| Platelet count (×103/μL) | 170‐400 | 291 (192‐417) | 240 (183‐339) | 304 (194‐348) | 262 (218‐419) | 238 (143‐317) | 256 (173‐421) | 275 (199‐414) | 292 (200‐461) |
| Urine‐specific gravity | 1.015‐1.050 | 1.023 (1.004‐1.050) | 1.026 (1.014‐1.041) | 1.029 (1.011‐1.041) | 1.035 (1.015‐1.050) | 1.028 (1.005‐1.038) | 1.019 (1.002‐1.026) | 1.029 (1.012‐1.042) | 1.020 (1.004‐1.028) |
| Urine protein:creatinine ratio | <0.5 | 0.1C (0.1‐0.4) | 0.2C (0.1‐0.5) | 0.3BC (0.1‐0.6) | 0.2C (0.1‐0.4) | 0.3C (0.1‐1.5) | 0.6AB (0.2‐4.1) | 0.3BC (0.1‐0.6) | 1.7A (0.1‐2.8) |
Results are presented as median (range). Superscript letters and asterisks highlight values with significant treatment‐by‐time, treatment, or time interactions. Values that do not share a common superscript letter differed significantly (P < .05) based on post hoc analysis. * indicates values that differed significantly (P < .05) over time independent of treatment.
Abbreviations: ALP, alkaline phosphatase; BUN, blood urea nitrogen; GGT, gamma‐glutamyl transferase; RI, reference interval.
Serum ALP activities increased over time in the prednisone and prednisone/aspirin groups, resulting in a significant treatment‐by‐time interaction (F[3, 20] = 10.8, P < .001) and significant corresponding post‐hoc tests (P < .001 for each). Both GGT (F[1, 20] = 10.5, P = .004) and lipase (F[1, 20] = 10.3, P = .004) activityes increased significantly over time due to increased activities in the prednisone‐receiving groups although the treatment‐by‐time interactions were not significant. Amylase activities decreased over time for the prednisone and prednisone/aspirin groups, resulting in a treatment‐by‐time interaction (F[3, 20] = 5.8, P = .006) and significant corresponding post hoc tests (P ≤ .002 for each).
Although neither BUN concentration nor urine‐specific gravity differed among treatments or over time, BUN:creatinine ratios significantly differed by treatment‐by‐time (F[3, 20] = 5.6, P = .006) and time (F[3, 20] = 5.8, P < .001). Post hoc tests revealed significant increases in BUN:creatinine ratios over time for prednisone and prednisone/aspirin treatment groups compared to baseline values (P < .001 for each). Significant changes over time were not observed in BUN:creatinine ratios for dogs treated with aspirin or placebo. Differences in BUN:creatinine ratios over time among groups reflected significant decreases in creatinine concentrations (F[3, 20] = 6.48, P = .003). Post hoc tests revealed that creatinine concentrations in dogs treated with prednisone or prednisone/aspirin significantly decreased over time (P ≤ .001 for each), while similar decreases were not observed for dogs treated with aspirin or placebo. Finally, urine protein:creatinine ratios were significantly higher after treatment for the prednisone and prednisone/aspirin groups compared to baseline values and results for the other 2 groups, as demonstrated by both significant treatment‐by‐time interactions (F[3, 20] = 5.9, P = .005) and corresponding post hoc tests (P ≤ .01 for each).
3.3. Endoscopic findings
Gastric biopsies taken at baseline from all dogs were positive for urease‐producing bacteria.
Median (range) numbers of gastric mucosal lesions are summarized in Table 3. Hemorrhages, punctate erosions, and invasive erosions required logarithmic transformation before statistical analysis in order to meet underlying statistical assumptions. Total mucosal hemorrhages did not differ among treatment groups or over time (P > .2). Total gastric punctate erosions had significant treatment‐by‐time (F [6, 40] = 3.0, P = .02), treatment (F[3, 20] = 10.0, P < .001), and time (F[2, 40] = 14.4, P < .001) effects. Additionally, total gastric invasive erosions had significant treatment‐by‐time (F[6, 40] = 5.8, P < .001), treatment (F[3, 20] = 11.7, P < .001), and time (F[2, 40] = 27.2, P < .001) effects. Post hoc analysis revealed that differences were due to greater numbers of lesions during treatment for dogs in the aspirin (invasive erosions, day 14 only), prednisone (days 14 and 28), and prednisone/aspirin groups (days 14 and 28; P ≤ .008 for all comparisons). Erosion often was marked and multifocal (Figure 1), although primarily concentrated in the antrum. Ulceration was noted in 14 studies, representing 10 dogs over the course of the study (Table 3, Figure 2). Ulcers were generally limited in size and depth, but severe ulceration was noted in 2 dogs (Video S1). One dog in the placebo group had 1 small ulcer identified on day 28. One dog in the aspirin group had 22 ulcers identified at day 14. The same dog had 4 ulcers at day 28. It was not possible to determine whether these were persistent or new ulcers due to the severity of ulceration on day 14. Three dogs in the prednisone group each developed 1 ulcer (day 14, 1 dog; day 28, 2 dogs). Finally, 5 dogs in the prednisone/aspirin group had between 1 and 25 ulcers identified at day 14; 2 of the same dogs had 1 and 3 new ulcers identified on day 28, respectively. Residual gastric contents were noted in the majority of dogs with GI bleeding. Duodenal lesions were rare, limited to hemorrhages (maximum score, 3) and invasive erosions (maximum score, 2) in 5 dogs each.
Table 3.
Median (range) for gastric mucosal lesions identified on endoscopy for 24 healthy research dogs administered placebo, aspirin with placebo, prednisone with placebo, or a combination of prednisone and aspirin for 28 days
| Baseline | Day 14 | Day 28 | |
|---|---|---|---|
| Placebo | |||
| Hemorrhages | 0 (0–29) | 3 (0‐132) | 1 (0‐10) |
| Punctate erosions | 0 (0‐14)D | 0 (0‐1)D | 0 (0‐36)CD |
| Invasive erosions | 0 (0‐4)E | 0 (0‐1)E | 0 (0–11)E |
| Ulcersa | 0 (0–0) | 0 (0‐0) | 0 (0‐1) |
| Aspirin | |||
| Hemorrhages | 0 (0‐60) | 16 (0‐31) | 0 (0‐16) |
| Punctate erosions | 0 (0‐7)CD | 14 (0‐37)BC | 0 (0‐227)CD |
| Invasive erosions | 0 (0‐1)E | 3 (0‐36)CD | 0 (0‐41)DE |
| Ulcersa | 0 (0–0) | 0 (0–22) | 0 (0–4) |
| Prednisone | |||
| Hemorrhages | 0 (0‐17) | 1 (0–10) | 7 (0‐105) |
| Punctate erosions | 0 (0‐2)D | 37 (0‐303)AB | 55 (7‐261)AB |
| Invasive erosions | 0 (0‐0)E | 10 (0‐45)BC | 33 (3‐211)AB |
| Ulcersa | 0 (0–0) | 0 (0‐1) | 0 (0‐1) |
| Prednisone and aspirin | |||
| Hemorrhages | 5 (0‐64) | 0 (0–2) | 0 (0–5) |
| Punctate Erosions | 0 (0‐237)CD | 214 (10‐540)A | 164 (1‐220)A |
| Invasive Erosions | 0 (0–16)E | 85 (16‐220)A | 13 (5‐100)AB |
| Ulcersa | 0 (0–0) | 3 (0‐25) | 1 (0‐3) |
Values that do not share a common superscript letter differed significantly (P < .05) among groups over time based on post hoc analysis.
Statistical comparisons were not performed due to limited occurrences.
Figure 1.
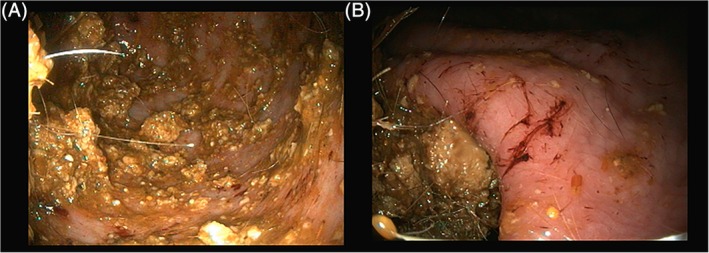
Diffuse punctate and invasive erosions in the antrum (A) and angularis incisura (B) of a healthy dog administered prednisone (2 mg/kg q24h) and aspirin (2 mg/kg q24h) PO for 14 days. Residual gastric contents in the antrum (A) likely resulted in underestimation of number and depth of some lesions
Figure 2.
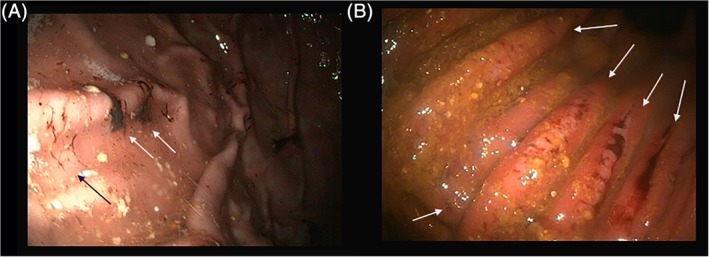
Healing (black arrow) and active ulceration with adherent clots (white arrows) in the gastric body of healthy dogs administered (A) prednisone (2 mg/kg q24h) and aspirin (2 mg/kg q24h) PO for 28 days and (B) aspirin (2 mg/kg q24h) PO for 14 days
As shown in Figure 3, total gastric endoscopic mucosal lesion scores13 differed significantly by treatment‐by‐time (F[6, 40] = 4.4, P = .002), treatment (F[3, 20] = 7.1, P = .002), and time (F[2, 40] = 18.9, P < .001). Post hoc analysis revealed significantly higher lesion scores during treatment over time for dogs in the aspirin (day 14 only), prednisone (days 14 and 28), and prednisone/aspirin groups (days 14 and 28) (P ≤ .02 for all comparisons). Scores for dogs in the prednisone/aspirin group on day 14 were significantly higher than those for any other time point or in any other group (P ≤ .05).
Figure 3.
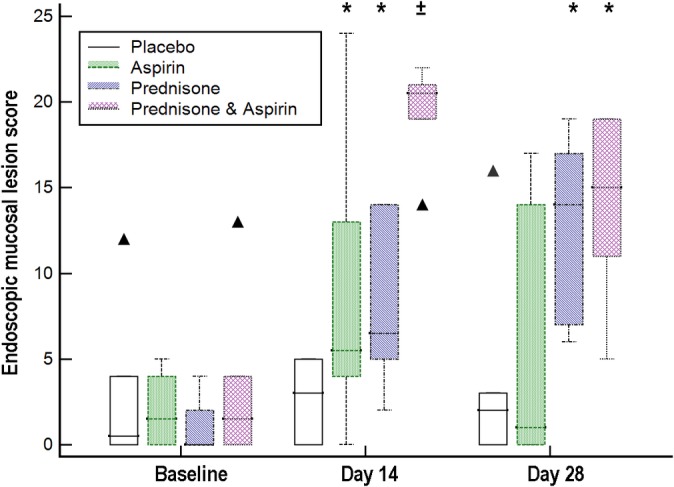
Box and whisker plots of total gastric endoscopic mucosal lesion scores6 for 24 healthy dogs randomized to receive placebo, aspirin with placebo, prednisone with placebo, or a combination of prednisone and aspirin for 28 days. ▲ = outliers, * = significantly higher than scores without overlying symbols, ± = significantly higher than all other scores
Forty studies had endoscopic mucosal lesion scores ≥4, with significant differences among treatment groups (χ2 [3] = 18.05, P < .001). Dogs receiving prednisone and prednisone/aspirin had 5.1 times (95% CI, 1.4‐18.1) and 11.2 times (95% CI, 3.4‐37.0) higher odds of developing total lesion scores ≥4 over time than dogs administered placebos (P ≤ .01), respectively. When hemorrhages were excluded from scoring of endoscopic mucosal lesions, odds of total lesions scores ≥4 occurring were 11.1 times (95% CI, 1.7‐73.6) and 31.5 times (95% CI, 3.5‐288.0) times higher for dogs receiving prednisone or prednisone/aspirin, respectively, than placebo (P ≤ .01). In contrast, dogs receiving aspirin were not more likely to have lesion scores ≥4 over time than dogs administered placebo.
4. DISCUSSION
Total gastric endoscopic mucosal lesion scores increased significantly in dogs administered aspirin (day 14 only), prednisone, and prednisone/aspirin combination treatment in this study. Increases were primarily due to increased numbers of punctate and invasive erosions, although ulcers developed in 10 dogs over the course of the study. Both numbers of lesions and endoscopic lesion scores were higher on day 14 than 28, with significantly higher values in the aspirin and prednisone/aspirin group on day 14 compared to day 28. However, a number of dogs had new lesions, such as ulcers, identified on day 28, suggesting ongoing primary disease. Dogs receiving prednisone and prednisone/aspirin combination treatment had 11.1 times and 31.5 times higher odds to have endoscopic lesions scores ≥4 (eg, >25 punctate erosions, ≥1 invasive erosion, ≥1 ulcer, or all) than dogs administered placebo.
Although gastric mucosal damage was marked and often severe, it was not accompanied by changes in food intake, vomiting, fecal score, or weight. Furthermore, many clinicopathologic changes associated with GI bleeding were not identified, potentially due to offsetting effects of glucocorticoids. For example, permissive effects of steroids on erythropoiesis could have blunted development of anemia secondary to GI blood loss. Lack of hypoalbuminemia could reflect increased albumin synthesis secondary to steroid administration, as occurs in both experimental models and people with hepatic and non‐hepatic disease.14, 17, 18, 19, 20, 21 Other glucocorticoid‐associated changes identified in this study included decreased amylase activity; increased ALP, GGT, and lipase activity; and increased urine protein:creatinine ratio compared to baseline. Though results for these analytes changed significantly over time and differed from those for other groups, results uncommonly were out of the reference interval in spite of an extended duration of glucocorticoid administration. The exception was urine protein:creatinine ratios, for which median values were above the reference interval at day 28 for dogs in the prednisone and prednisone/aspirin groups.
The BUN:creatinine ratio detects changes consistent with GI bleeding in absence of increases in BUN concentration, given the latter's poor sensitivity for bleeding. Ten percent of people experiencing acute GI blood loss of ≥1.1 L have BUN concentrations <24 mg/dL.22 Furthermore, only 66% of subjects with massive GI hemorrhage have BUN concentrations ≥31 mg/dL—the upper limit of the reference interval for BUN in this study. Less marked increases are anticipated in cases with chronic compensated blood loss,23 like that identified in our study. The median BUN:creatinine ratio for dogs with overt upper GI bleeding is 28,23 with no difference in BUN:creatinine ratios between dogs that have received steroids versus those that have not. Although BUN concentrations did not change in this study, median BUN:creatinine ratios increased by 1.8‐fold to 27 in the prednisone‐containing groups—almost identical to median ratios for dogs in the prior report. Given the lack of changes in MCS in spite of decreased creatinine concentrations in the prednisone‐receiving groups, it is reasonable to surmise that glucocorticoid‐induced polydipsia offset GI bleeding‐associated increases in BUN concentrations. Unfortunately, this hypothesis cannot be confirmed because neither urine output nor water intake was quantitated. Although urine‐specific gravity did not differ significantly among groups, first morning voided urine samples could not be collected because the majority of the dogs urinated at will in their runs.
Glucocorticoids remain the mainstay of treatment for IMHA24 due to their rapid onset of action, proven efficacy, and low cost. Glucocorticoids have complex and competing effects on the GI tract. Basal concentrations help maintain GI mucosal integrity, and stress‐related increases in endogenous glucocorticoid concentrations are gastroprotective due to maintenance of local glucose homeostasis.1, 2 Sustained glucocorticoid excess, however, inhibits endogenous peroxidase,25 which scavenges endogenous hydrogen peroxide in the gastric mucosa.26 Peroxidase is rich in the parietal cell and also plays a role in the control of acid secretion.27 Inactivation of peroxidase leads to increased free radical damage, decreased synthesis of prostaglandin, hyperacidity, and altered vascular permeability, ultimately resulting in GI ulceration.1, 2, 26, 27, 28, 29, 30, 31, 32, 33
Short‐term injectable corticosteroid administration can cause GI bleeding and ulceration in healthy dogs.34, 35, 36 Almost all (90%‐100%) dogs administered high‐dose methylprednisolone IV for 48 hours in 2 studies develop severe GI bleeding, with disease primarily located in the antrum.34, 35 The first34 of these studies finds GI bleeding associated with residual gastric contents, consistent with results of our study. Lack of an association between bleeding and gastric contents in the second study likely reflects an increased fasting period before anesthesia.35 Healthy dogs administered high‐dose twice daily dexamethasone SC for 8 days also develop severe GI bleeding with lesions primarily located in the antrum and minimal difference in the severity of lesions between days 2 and 8.36 Additionally, dogs receiving dexamethasone develop anemia and loose dark feces, neither of which is reported in dogs administered methylprednisolone. Fecal occult blood tests are positive in the majority of dogs with GI bleeding.34, 35, 36 Finally, GI bleeding increases significantly for middle‐aged healthy research dogs administered high‐dose prednisolone for 3 days, with vomiting at least once during treatment occurring in 83% of dogs.37 In contrast to these 4 studies, sustained oral administration of prednisone is not associated with an increase in the incidence or severity of GI bleeding in healthy dogs in another randomized trial.8
Potential explanations for conflicting findings among the prior studies, as well as ours, include differences in the drugs administered, dosages used, routes of administration, and durations of treatment. However, none of these possibilities explains the discordance between the results of our study and another study using the same corticosteroid, dosage, and duration of treatment. 8 Furthermore, all dogs in both studies had positive test results for Helicobacter spp. Commercial prednisone tablets were used for this study versus being compounded into gelatin capsules.8 In this study, aspirin similarly was repackaged into capsules due to its instability in liquid formulations38 versus being suspended in almond oil.6 Discordance in findings regarding the impact of aspirin administration on GI bleeding, thus, could reflect differences in aspirin dose, differences in drug reformulation, or both. It is possible, though exceedingly unlikely, that differences in drug formulation contributed to the discordant association between prednisone administration and GI bleeding between the 2 studies. A more likely explanation is that the discordance between studies reflects differences in subject age. Although 3 prior studies do not provide subject age,34, 35, 36 median age of the dogs administered prednisone without associated GI bleeding is substantially younger (14 months)8 than that of the dogs in our pilot evaluation (48 months) or the study that provides age (58 months),37 potentially suggesting an increasing sensitivity to the ulcerogenic effects of glucocorticoids with age. To prevent age from potentially confounding our results, dogs with a wide range of ages were used, and subjects were stratified by age before group randomization. Covariate testing revealed a lack of association between age and development of bleeding, but the lack of an age‐related association must be interpreted with care given small group sizes.
Survival rates in dogs with immune‐mediated hemolytic anemia (IMHA) historically are low (30%‐50%),39 primarily due to fatal thromboembolism. As such, current recommendations for IMHA include the immediate initiation of thromboprophylactic treatment.24, 40 Thromboprophylaxis should continue until the resolution of the hypercoagulable state because premature cessation of thromboprophylaxis is associated with an increased risk of thrombosis.24 Because glucocorticoids independently increase thrombotic risk,40, 41, 42 ACVIM guidelines for dogs with IMHA recommend thromboprophylaxis continue until dogs are weaned off prednisone.24 Given the need for prolonged treatment and in the absence of objective data showing superiority of 1 thromboprophylactic agent for management of canine IMHA, drug selection often is influenced by financial and lifestyle constraints of owners. Given its low cost, oral route of administration, once daily dosing interval, and long‐term efficacy in decreasing mortality in 1 retrospective report of dogs with IMHA,39 aspirin continues to be widely prescribed for IMHA. The ideal dose, however, remains unclear. The dosage of aspirin shown to decrease mortality in the aforementioned retrospective study does not result in reliable platelet inhibition based on platelet function tests.43, 44 Reliable inhibition requires an aspirin dosage of 2 mg/kg q24h.44
Aspirin exerts its antiplatelet effects through irreversible acetylation of the COX active site in platelets and megakaryocytes, decreasing thromboxane production and impairing platelet response.3 Due to non‐selective COX inhibition, aspirin administration can cause gastric ulceration and intestinal lesions in dogs in a dose‐dependent manner.6, 9, 45 Aspirin also increases intestinal permeability and decreases recovery of barrier function after ischemic insult.46 These effects are particularly concerning in dogs with IMHA, because of the local ischemic effects of marked anemia. Occult GI bleeding is the major negative side effect of low‐dose aspirin treatment in people.3, 4, 5 Systematic reviews find no association between the type of aspirin formulation (plain, enterically coated, buffered) and relative risk of GI bleeding in people.47 As such, minimizing the aspirin dose is the best way to decrease the risk of bleeding. Although 1 prior report finds no association between administering low‐dose aspirin with prednisone and GI bleeding in healthy dogs,8 the aspirin dosage used in that study is much lower (.5 mg/kg q24h) than the currently recommended dosage for antiplatelet effects (2 mg/kg q24h).44 In this study, aspirin administration significantly increased gastric mucosal lesions on day 14, with development of profound and sustained ulceration in 1 dog (Figure 4, Video S1). Furthermore, the administration of combination of prednisone/aspirin treatment more than doubled the risk of having endoscopic mucosal lesion scores ≥4 compared to that for dogs administered prednisone alone.
Unfortunately, neither misoprostol, omeprazole, or sucralfate nor cimetidine administration decreases the incidence or severity of GI bleeding due to short‐term glucocorticoid treatment in healthy dogs or dogs with intervertebral disk disease.35, 48, 49 Omeprazole is ineffective in decreasing GI bleeding in dogs due to sustained glucocorticoid and low‐dose aspirin treatment based on 1 preliminary report,11 although the omeprazole dosage used was less than that currently recommended for treatment of GI ulceration.50 Thus, prophylactic administration of these gastroprotectants is not recommended given their lack of efficacy.50 In contrast, mosapride decreases both GI bleeding and the occurrence of vomiting due to short‐term administration of high‐dose prednisolone.37 Further evaluation is warranted to determine whether similar prophylactic benefits occur in dogs administered sustained oral glucocorticoid treatment. In cases where GI bleeding is confirmed, management using twice daily proton pump inhibitor treatment is warranted to improve healing.50 Based on the results of this study, however, the primary focus should be on reducing or eliminating glucocorticoid treatment.
Results of this study cannot be extrapolated to the use of prednisone with other thromboprophylactic agents. Although clopidogrel, heparin, and direct oral anticoagulants increase the risk of GI bleeding in people,4, 51, 52, 53, 54 the underlying etiopathology for each differs from that of prednisone‐induced bleeding, aspirin‐induced bleeding, or both. Furthermore, results for people might not accurately predict their effects in dogs. Fecal occult blood testing was not performed in this study, which might have enhanced detection of occult GI bleeding. However, false positives occur due to differences in diet,55 potentially limiting application of test results in client‐owned animals. Other limitations of our study include the use of healthy research dogs and the relatively short study duration. Although dogs ranged in age and were older than dogs in 1 prior report, they all were either Beagles or Hound dogs, and none had underlying disease. Results might differ in dogs with underlying disease or receiving additional medications. Subtle changes in attitude, appetite, and fecal quality might have been overlooked given the lack of 24‐hour surveillance and owner‐pet pair bonding. Although GI lesion scores were equivalent to or higher for dogs administered prednisone/aspirin combination treatment versus prednisone alone, hematocrit did not differ significantly between those groups. In fact, anemia was not noted in any dog, despite the occurrence of multifocal punctate erosions, invasive erosions, and ulceration (Table 3). The short study duration could have contributed to a lack of difference in hematocrit, because anemia due to chronic GI bleeding can take months to manifest in an animal with normal iron stores. Gastrointestinal bleeding significantly decreased between days 14 and 28 for dogs receiving aspirin and prednisone/aspirin combination treatment. It is possible that prednisone‐associated GI bleeding could have resolved with ongoing administration, although this seems unlikely given the development of new lesions, including ulcers, by day 28 in several dogs. Finally, the impact of these findings on managing dogs with immune‐mediated diseases is unknown. Further evaluation in dogs receiving sustained treatment for naturally occurring diseases will be necessary to determine the impact of GI bleeding on disease management, thromboembolic risk, and long‐term survival.
In conclusion, oral administration of prednisone and prednisone/aspirin combination treatment increased the risk of having endoscopic lesions scores ≥4 (eg, >25 punctate erosions, ≥1 invasive erosion, ≥1 ulcer, or all) 11.1‐ and 31.5‐fold, respectively, in this study. Lesions were most severe on day 14 for dogs receiving prednisone/aspirin combination treatment, with no significant difference in the amount or severity of lesions on day 28 between dogs receiving prednisone versus combination treatment. Even when severe, GI bleeding was not accompanied by changes in attitude, food intake, vomiting, fecal score, hematocrit, or BUN concentration in dogs. Neither hematemesis nor melena was noted. Clinicians must maintain a heightened suspicion for GI bleeding; changes in the BUN:creatinine ratio might be helpful in identifying dogs experiencing occult bleeding without classical biochemical changes, such as increased BUN concentration or anemia. When possible, glucocorticoids should be weaned before other immunomodulators to minimize occult GI blood loss and facilitate discontinuation of thromboprophylactic treatment.
CONFLICT OF INTEREST DECLARATION
The funder, University of Tennessee, Knoxville, through the Acree Research Chair of Medicine endowment had no involvement in the design or performance of the study, writing of the manuscript, or the decision to submit the manuscript for publication.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
The study protocol was approved by the IACUC of the University of Tennessee, Knoxville (protocol number 2283) and performed in compliance with “The Guide for the Care and Use of Laboratory Animals” in laboratory animal facilities that are AAALAC certified and exceed NIH standards of care.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
Supporting information
Video S1 Diffuse ulceration in the stomach of a healthy dog administered aspirin (2 mg/kg q24h) PO for 14 days.
Whittemore JC, Mooney AP, Price JM, Thomason J. Clinical, clinicopathologic, and gastrointestinal changes from aspirin, prednisone, or combination treatment in healthy research dogs: A double‐blind randomized trial. J Vet Intern Med. 2019;33:1977–1987. 10.1111/jvim.15577
Funding information University of Tennessee, Knoxville, Acree Research Chair of Medicine endowment.
REFERENCES
- 1. Filaretova L, Morozova O, Bagaeva T, et al. From gastroprotective to proulcerogenic action of glucocorticoids on the gastric mucosa. J Physiol Pharmacol. 2009;60(Suppl 7):79‐86. [PubMed] [Google Scholar]
- 2. Filaretova L, Podvigina T, Bagaeva T, Morozova O. Dual action of glucocorticoid hormones on the gastric mucosa: how the gastroprotective action can be transformed to the ulcerogenic one. Inflammopharmacology. 2009;17:15‐22. [DOI] [PubMed] [Google Scholar]
- 3. Floyd CN, Ferro A. Mechanisms of aspirin resistance. Pharmacol Ther. 2014;141:69‐78. [DOI] [PubMed] [Google Scholar]
- 4. Ibanez L, Vidal X, Vendrell L, et al. Upper gastrointestinal bleeding associated with antiplatelet drugs. Aliment Pharmacol Ther. 2006;23:235‐242. [DOI] [PubMed] [Google Scholar]
- 5. Lanas A, Garcia‐Rodriguez LA, Arroyo MT, et al. Effect of antisecretory drugs and nitrates on the risk of ulcer bleeding associated with nonsteroidal anti‐inflammatory drugs, antiplatelet agents, and anticoagulants. Am J Gastroenterol. 2007;102:507‐515. [DOI] [PubMed] [Google Scholar]
- 6. Forsyth SF, Guilford WG, Lawoko CR. Endoscopic evaluation of the gastroduodenal mucosa following non‐steroidal anti‐inflammatory drug administration in the dog. N Z Vet J. 1996;44:179‐181. [DOI] [PubMed] [Google Scholar]
- 7. Narita T, Sato R, Motoishi K, et al. The interaction between orally administered non‐steroidal anti‐inflammatory drugs and prednisolone in healthy dogs. J Vet Med Sci. 2007;69:353‐363. [DOI] [PubMed] [Google Scholar]
- 8. Heather Graham A, Leib MS. Effects of prednisone alone or prednisone with ultralow‐dose aspirin on the gastroduodenal mucosa of healthy dogs. J Vet Intern Med. 2009;23:482‐487. [DOI] [PubMed] [Google Scholar]
- 9. Reimer ME, Johnston SA, Leib MS, et al. The gastroduodenal effects of buffered aspirin, carprofen, and etodolac in healthy dogs. J Vet Intern Med. 1999;13:472‐477. [DOI] [PubMed] [Google Scholar]
- 10. Nagata N, Sakurai T, Shimbo T, et al. Acute severe gastrointestinal tract bleeding is associated with an increased risk of thromboembolism and death. Clin Gastroenterol Hepatol. 2017;15:1882‐1889. [DOI] [PubMed] [Google Scholar]
- 11. Whittemore JC, Gould E, Newman S. Gastrointestinal endoscopic mucosal lesion scores in healthy dogs receiving prednisone, aspirin, and omeprazole [abstract]. J Vet Intern Med. 2015;28:1152. [Google Scholar]
- 12. Whittemore JC, Mooney A, Mawby DI, Thomason J. Platelet function and endoscopic changes after clopidogrel, aspirin, prednisone, or combination treatment in dogs [abstract]. J Vet Intern Med. 2017;30:1282. [Google Scholar]
- 13. Wilson JE, Chandrasekharan NV, Westover KD, Eager KB, Simmons DL. Determination of expression of cyclooxygenase‐1 and ‐2 isozymes in canine tissues and their differential sensitivity to nonsteroidal anti‐inflammatory drugs. Am J Vet Res. 2004;65:810‐818. [DOI] [PubMed] [Google Scholar]
- 14. Wangh LJ. Glucocorticoids act together with estrogens and thyroid hormones in regulating the synthesis and secretion of Xenopus vitellogenin, serum albumin, and fibrinogen. Dev Biol. 1982;89:294‐298. [DOI] [PubMed] [Google Scholar]
- 15. Greco DS. Diagnosis and dietary management of gastrointestinal disease. https://www.purinaveterinarydiets.com/media/1202/gi_quick_reference_guide.pdf. 2011.
- 16. Slovak JE, Wang C, Sun Y, et al. Development and validation of an endoscopic activity score for canine inflammatory bowel disease. Vet J. 2015;203:290‐295. [DOI] [PubMed] [Google Scholar]
- 17. Brown PC, Papaconstantinou J. Coordinated modulation of albumin synthesis and mRNA levels in cultured hepatoma cells by hydrocortisone and cyclic AMP analogs. J Biol Chem. 1979;254:9379‐9384. [PubMed] [Google Scholar]
- 18. Okuyama S, Kakumu S, Kato Y, Inagaki T, Ito S. Albumin synthesis and effect of betamethasone on albumin synthesis in perfused liver of normal and CCL4‐intoxicated rats. Gastroenterol Jpn. 1975;10:271‐282. [DOI] [PubMed] [Google Scholar]
- 19. Nawa K, Nakamura T, Kumatori A, Noda C, Ichihara A. Glucocorticoid‐dependent expression of the albumin gene in adult rat hepatocytes. J Biol Chem. 1986;261:16883‐16888. [PubMed] [Google Scholar]
- 20. Schomerus H, Mayer G. Synthesis rates of fibrinogen and albumin in patients with rheumatoid arthritis. Acta Hepatogastroenterol (Stuttg). 1977;24:11‐14. [PubMed] [Google Scholar]
- 21. Cain GD, Mayer G, Jones EA. Augmentation of albumin but not fibrinogen synthesis by corticosteroids in patients with hepatocellular disease. J Clin Invest. 1970;49:2198‐2204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Pumphrey CW, Beck ER. Raised blood urea concentration indicates considerable blood loss in acute upper gastrointestinal haemorrhage. Br Med J. 1980;280:527‐528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Prause LC, Grauer GF. Association of gastrointestinal hemorrhage with increased blood urea nitrogen and BUN/creatinine ratio in dogs: a literature review and retrospective study. Vet Clin Pathol. 1998;27:107‐111. [DOI] [PubMed] [Google Scholar]
- 24. Swann JW, Garden OA, Fellman CL, et al. ACVIM consensus statement on the treatment of immune‐mediated hemolytic anemia in dogs. J Vet Intern Med. 2019;33:1141‐1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. De SK, Banerjee RK. Glucocorticoid effects on gastric peroxidase activity. Biochim Biophys Acta. 1984;800:233‐241. [DOI] [PubMed] [Google Scholar]
- 26. Das D, Banerjee RK. Effect of stress on the antioxidant enzymes and gastric ulceration. Mol Cell Biochem. 1993;125:115‐125. [DOI] [PubMed] [Google Scholar]
- 27. Bandyopadhyay U, Bhattacharyya DK, Chatterjee R, Banerjee RK. Localization of gastric peroxidase and its inhibition by mercaptomethylimidazole, an inducer of gastric acid secretion. Biochem J. 1992;284:305‐312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Das D, Bandyopadhyay D, Bhattacharjee M, Banerjee RK. Hydroxyl radical is the major causative factor in stress‐induced gastric ulceration. Free Radic Biol Med. 1997;23:8‐18. [DOI] [PubMed] [Google Scholar]
- 29. Choquet A, Magous R, Bali JP. Gastric mucosal endogenous prostanoids are involved in the cellular regulation of acid secretion from isolated parietal cells. J Pharmacol Exp Ther. 1993;266:1306. [PubMed] [Google Scholar]
- 30. Bhattacharjee M, Chakraborty Y, Ganguly C, et al. Inhibition of gastric mucosal prostaglandin synthetase activity by mercaptomethylimidazole, an inducer of gastric acid secretion–plausible involvement of endogenous H2O2. Biochem Pharmacol. 1998;56:905‐913. [DOI] [PubMed] [Google Scholar]
- 31. Bandyopadhyay U, Chatterjee R, Chakraborty TK, Ganguly CK, Bhattacharyya DK, Banerjee RK. Activation of parietal cell by mercaptomethylimidazole: a novel inducer of gastric acid secretion. Biochem Pharmacol. 1997;54:241‐248. [DOI] [PubMed] [Google Scholar]
- 32. Bandyopadhyay U, Biswas K, Bandyopadhyay D, Ganguly C, Banerjee R. Dexamethasone makes the gastric mucosa susceptible to ulceration by inhibiting prostaglandin synthetase and peroxidase—two important gastroprotective enzymes. Mol Cell Biochem. 1999;202:31‐36. [DOI] [PubMed] [Google Scholar]
- 33. Das D, De PK, Banerjee RK. Thiocyanate, a plausible physiological electron donor of gastric peroxidase. Biochem J. 1995;305:59‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Rohrer CR, Fischer A, Fox LE, et al. Gastric hemorrhage in dogs given high doses of methylprednisolone sodium succinate. Am J Vet Res. 1999;60:977‐981. [PubMed] [Google Scholar]
- 35. Rohrer CR, Hill RC, Fischer A, et al. Efficacy of misoprostol in prevention of gastric hemorrhage in dogs treated with high doses of methylprednisolone sodium succinate. Am J Vet Res. 1999;60:982‐985. [PubMed] [Google Scholar]
- 36. Sorjonen DC, Dillon AR, Powers RD, Spano JS. Effects of dexamethasone and surgical hypotension on the stomach of dogs: clinical, endoscopic, and pathologic evaluations. Am J Vet Res. 1983;44:1233‐1237. [PubMed] [Google Scholar]
- 37. Tsukamoto A, Ohno K, Maeda S, et al. Effect of mosapride on prednisolone‐induced gastric mucosal injury and gastric‐emptying disorder in dog. J Vet Med Sci. 2012;74:1103‐1108. [DOI] [PubMed] [Google Scholar]
- 38. Bica K, Rijksen C, Nieuwenhuyzen M, Rogers RD. In search of pure liquid salt forms of aspirin: ionic liquid approaches with acetylsalicylic acid and salicylic acid. Phys Chem Chem Phys. 2010;12:2011‐2017. [DOI] [PubMed] [Google Scholar]
- 39. Weinkle TK, Center SA, Randolph JF, Warner KL, Barr SC, Erb HN. Evaluation of prognostic factors, survival rates, and treatment protocols for immune‐mediated hemolytic anemia in dogs: 151 cases (1993‐2002). J Am Vet Med Assoc. 2005;226:1869‐1880. [DOI] [PubMed] [Google Scholar]
- 40. deLaforcade A, Bacek L, Blais M‐C, Goggs R, Lynch A, Rozanski E. Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE): domain 1‐defining populations at risk. J Vet Emerg Crit Care. 2019;29:37‐48. [DOI] [PubMed] [Google Scholar]
- 41. Sharp CR, Goggs R, Blais M‐C, et al. Clinical application of the American College of Veterinary Emergency and Critical Care (ACVECC) Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE) guidelines to small animal cases. J Vet Emerg Crit Care. 2019;29:121‐131. [DOI] [PubMed] [Google Scholar]
- 42. Weiss DJ, Brazzell JL. Detection of activated platelets in dogs with primary immune‐mediated hemolytic anemia. J Vet Intern Med. 2006;20:682‐686. [DOI] [PubMed] [Google Scholar]
- 43. Dudley A, Thomason J, Fritz S, et al. Cyclooxygenase expression and platelet function in healthy dogs receiving low‐dose aspirin. J Vet Intern Med. 2013;27:141‐149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. McLewee N, Archer T, Wills R, Mackin A, Thomason J. Effects of aspirin dose escalation on platelet function and urinary thromboxane and prostacyclin levels in normal. J Vet Pharmacol Ther. 2018;41:60‐67. [DOI] [PubMed] [Google Scholar]
- 45. Ward DM, Leib MS, Johnston SA, Marini M. The effect of dosing interval on the efficacy of misoprostol in the prevention of aspirin‐induced gastric injury. J Vet Intern Med. 2003;17:282‐290. [DOI] [PubMed] [Google Scholar]
- 46. Little D, Jones SL, Blikslager AT. Cyclooxygenase (COX) inhibitors and the intestine. J Vet Intern Med. 2007;21:367‐377. [DOI] [PubMed] [Google Scholar]
- 47. García Rodríguez L, Hernández‐Díaz S, de Abajo FJ. Association between aspirin and upper gastrointestinal complications: systematic review of epidemiologic studies. Br J Clin Pharmacol. 2001;52:563‐571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Neiger R, Gaschen F, Jaggy A. Gastric mucosal lesions in dogs with acute intervertebral disc disease: characterization and effects of omeprazole or misoprostol. J Vet Intern Med. 2000;14:33‐36. [DOI] [PubMed] [Google Scholar]
- 49. Hanson SM, Bostwick DR, Twedt DC, Smith MO. Clinical evaluation of cimetidine, sucralfate, and misoprostol for prevention of gastrointestinal tract bleeding in dogs undergoing spinal surgery. Am J Vet Res. 1997;58:1320‐1323. [PubMed] [Google Scholar]
- 50. Marks SL, Kook PH, Papich MG, Tolbert MK, Willard MD. ACVIM consensus statement: support for rational administration of gastrointestinal protectants to dogs and cats. J Vet Intern Med. 2018;32:1823‐1840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Tsai TJ, Lai KH, Hsu PI, et al. Upper gastrointestinal lesions in patients receiving clopidogrel anti‐platelet therapy. J Formos Med Assoc. 2012;111:705‐710. [DOI] [PubMed] [Google Scholar]
- 52. Mistry DA, Chandratreya A, Lee PYF. A systematic review on the use of aspirin in the prevention of deep vein thrombosis in major elective lower limb orthopedic surgery: an update from the past 3 years. Surg J (N Y). 2017;3:e191‐e196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Jameson SS, Baker PN, Deehan DJ, Port A, Reed MR. Evidence‐base for aspirin as venous thromboembolic prophylaxis following joint replacement. Bone Joint Res. 2014;3:146‐149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Nielen JTH, Dagnelie PC, Emans PJ, et al. Safety and efficacy of new oral anticoagulants and low‐molecular‐weight heparins compared with aspirin in patients undergoing total knee and hip replacements. Pharmacoepidemiol Drug Saf. 2016;25:1245‐1252. [DOI] [PubMed] [Google Scholar]
- 55. Rice JE, Ihle SL. Effects of diet on fecal occult blood testing in healthy dogs. Can J Vet Res. 1994;58:134‐137. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video S1 Diffuse ulceration in the stomach of a healthy dog administered aspirin (2 mg/kg q24h) PO for 14 days.