

Abstract
Background
This article summarizes the ERA-EDTA Registry’s 2016 Annual Report, by describing the epidemiology of renal replacement therapy (RRT) for end-stage renal disease (ESRD) in 2016 within 36 countries.
Methods
In 2017 and 2018, the ERA-EDTA Registry received data on patients undergoing RRT for ESRD in 2016 from 52 national or regional renal registries. In all, 32 registries provided individual patient data and 20 provided aggregated data. The incidence and prevalence of RRT and the survival probabilities of these patients were determined.
Results
In 2016, the incidence of RRT for ESRD was 121 per million population (pmp), ranging from 29 pmp in Ukraine to 251 pmp in Greece. Almost two-thirds of patients were men, over half were aged ≥65 years and almost a quarter had diabetes mellitus as their primary renal diagnosis. Treatment modality at the start of RRT was haemodialysis for 84% of patients. On 31 December 2016, the prevalence of RRT was 823 pmp, ranging from 188 pmp in Ukraine to 1906 pmp in Portugal. In 2016, the transplant rate was 32 pmp, varying from 3 pmp in Ukraine to 94 pmp in the Spanish region of Catalonia. For patients commencing RRT during 2007–11, the 5-year unadjusted patient survival probability on all RRT modalities combined was 50.5%. For 2016, the incidence and prevalence of RRT were higher among men (187 and 1381 pmp) than women (101 and 827 pmp), and men had a higher rate of kidney transplantation (59 pmp) compared with women (33 pmp). For patients starting dialysis and for patients receiving a kidney transplant during 2007–11, the adjusted patient survival probabilities appeared to be higher for women than for men.
Keywords: dialysis, end-stage renal disease, epidemiology, kidney transplantation, survival analysis
INTRODUCTION
The European Renal Association – European Dialysis and Transplant Association (ERA-EDTA) Registry’s Annual Report describes the epidemiology of renal replacement therapy (RRT) for end-stage renal disease (ESRD) within Europe and countries bordering the Mediterranean Sea, based on the data collected via national and regional renal registries [1]. The summary of the ERA-EDTA Registry Annual Report, which is published on an annual basis, is intended to provide an overview of the current status of RRT for ESRD in Europe [2–4]. In 2017 and 2018, data for the year 2016 were received from 52 national or regional renal registries in 36 countries covering a general population of 686.9 million people. When leaving out Israel and Tunisia, the remaining countries cover a general population of 677.3 million people, representing 80.5% of the 2016 European general population, which was similar to 2015 (80.3%). A total of 32 national or regional renal registries from 17 countries provided individual patient data, whereas 20 countries or regions provided aggregated data (see Appendix A1). Compared to the 2015 ERA-EDTA Registry Annual Report, there were no differences in country participation.
This summary presents the 2016 incidence and prevalence of RRT, kidney transplantation activity, and the patient and graft survival. A description of the methods used to analyse the data, along with the full results, can be found in the ERA-EDTA Registry 2016 Annual Report [1].
On the occasion of the 2018 global focus on kidneys and women’s health, this year’s annual report contains additional analyses on sex comparisons, a summary of which is also presented in this article.
RESULTS
Incidence of RRT
In 2016, 83 311 individuals commenced RRT for ESRD, which equated to an overall unadjusted incidence of 121 per million population (pmp; Table 1). The unadjusted incidence was highest in Greece (251 pmp), Czech Republic (243 pmp) and Portugal (236 pmp), whereas it was lowest in Ukraine (29 pmp) and Russia (59 pmp; Table 1 and Figures 1 and 2). Of the patients commencing RRT, 62% were men, 52% were aged ≥65 years and 23% had diabetes mellitus (DM) as their primary renal diagnosis (Figure 3). The median age of the patients commencing RRT in all countries and regions combined was 65.8 years, ranging from 51.0 years in Ukraine to 73.8 years in the Dutch-speaking part of Belgium (Table 1). The majority of patients started RRT with haemodialysis (HD; 84%), while 12% of patients started with peritoneal dialysis (PD) and 4% received a pre-emptive kidney transplant (Figure 4). However, the initial treatment modality varied considerably between age groups, as the proportion of patients receiving either PD or a pre-emptive transplant decreased with increasing age. Furthermore, patients with a primary renal diagnosis of DM were less likely to receive a pre-emptive kidney transplant compared with non-diabetic patients (2% versus 6%). Of the incident patients receiving RRT at Day 91 after the start of treatment, the majority (82%) were receiving HD, 13% were receiving PD and 5% were living with a kidney transplant (Figure 5). In the first 90 days of treatment, the percentage of patients receiving HD decreased, and this was particularly evident in the younger age groups.
Table 1.
Incidence of RRT in 2016 at Day 1, by country/region, for all primary renal diseases combined and DM types 1 and 2, as count (n) and unadjusted rate pmp, and the mean and median age at the start of RRT
|
Country/region |
General population covered by the registry in thousands | Incidence of RRT in 2016, at Day 1 |
|||||
|---|---|---|---|---|---|---|---|
| All (n) | All (pmp) | Mean age (years) | Median age (years) | DM (n) | DM (pmp) | ||
| Albania | 2860 | 252 | 88 | 52.6 | 52.2 | 50 | 17 |
| Austria | 8700 | 1155 | 133 | 64.4 | 67.3 | 305 | 35 |
| Belarus | 8172 | 504 | 62 | 53.0 | 54.0 | 92 | 11 |
| Belgium, Dutch-speakinga | 6509 | 1214 | 187 | 71.0 | 73.8 | 256 | 39 |
| Belgium, French-speakinga | 4822 | 906 | 188 | 67.3 | 69.3 | 202 | 42 |
| Bosnia and Herzegovina | 3531 | 397 | 112 | 62.2 | 63.9 | 131 | 37 |
| Bulgaria | 7102 | 1109 | 156 | 309 | 44 | ||
| Croatia | 3755 | 675 | 180 | 64.9 | 66.0 | 181 | 48 |
| Cyprus | 857 | 165 | 193 | 66.7 | 69.0 | 47 | 55 |
| Czech Republicb | 10 262 | 2496 | 243 | ||||
| Denmark | 5784 | 740 | 128 | 63.3 | 67.4 | 192 | 33 |
| Estonia | 1316 | 112 | 85 | 59.7 | 61.6 | 19 | 14 |
| Finland | 5495 | 560 | 102 | 60.9 | 63.8 | 189 | 34 |
| France | 66 860 | 11 033 | 165 | 67.9 | 70.6 | 2566 | 38 |
| Georgia | 3720 | 754 | 203 | 60.4 | 61.9 | 187 | 50 |
| Greece | 10 776 | 2702 | 251 | 70.8 | 73.6 | 710 | 66 |
| Iceland | 335 | 30 | 89 | 61.7 | 65.1 | 5 | 15 |
| Israel | 8545 | 1612 | 189 | 65.1 | 68.0 | 805 | 94 |
| Italy (6 of 20 regions) | 20 921 | 3023 | 144 | 68.8 | 71.8 | 522 | 25 |
| Latvia | 1560 | 171 | 110 | 60.3 | 63.0 | 26 | 17 |
| Lithuania | 2888 | 310 | 107 | 61.8 | 62.5 | 52 | 18 |
| Macedonia | 2022 | 332 | 164 | 63.7 | 65.0 | 84 | 42 |
| Norway | 5235 | 556 | 106 | 63.1 | 66.5 | 88 | 17 |
| Polandb | 38 362 | 5716 | 149 | 2098 | 55 | ||
| Portugal | 10 358 | 2446 | 236 | 757 | 73 | ||
| Romania | 19 505 | 3454 | 177 | 62.4 | 64.5 | 356 | 18 |
| Russiab | 143 869 | 8521 | 59 | 54.3 | 57.0 | 1491 | 10 |
| Serbiac | 7058 | 618 | 88 | 62.0 | 64.6 | 139 | 20 |
| Slovakiab | 5435 | 835 | 154 | 64.6 | 66.0 | 316 | 58 |
| Spain (All regions) | 46 558 | 6600 | 142 | 63.0 | 67.5 | 1610 | 35 |
| Spain, Andalusia | 8406 | 1133 | 135 | 63.5 | 66.0 | 294 | 35 |
| Spain, Aragon | 1317 | 165 | 125 | 63.5 | 67.3 | 39 | 30 |
| Spain, Asturias | 1041 | 188 | 181 | 64.8 | 66.6 | 41 | 39 |
| Spain, Basque country | 2166 | 284 | 131 | 63.4 | 65.4 | 57 | 26 |
| Spain, Cantabriaa | 582 | 59 | 101 | 63.1 | 67.7 | 12 | 21 |
| Spain, Castile and Leóna | 2445 | 308 | 126 | 68.1 | 71.3 | 85 | 35 |
| Spain, Castile-La Manchaa | 2045 | 287 | 140 | 66.1 | 69.1 | 67 | 33 |
| Spain, Catalonia | 7523 | 1260 | 167 | 65.9 | 68.7 | 261 | 35 |
| Spain, Extremadura | 1088 | 120 | 110 | 65.6 | 66.6 | 34 | 31 |
| Spain, Galicia | 2715 | 399 | 147 | 66.0 | 68.7 | 102 | 38 |
| Spain, Community of Madrid | 6467 | 870 | 135 | 64.9 | 67.7 | 227 | 35 |
| Spain, Region of Murcia | 1465 | 202 | 138 | 63.3 | 65.3 | 47 | 32 |
| Spain, Navarrea | 639 | 82 | 128 | 64.7 | 67.2 | 21 | 33 |
| Spain, Valencian region | 4960 | 858 | 173 | 65.8 | 68.9 | 178 | 36 |
| Sweden | 9923 | 1204 | 121 | 64.0 | 67.9 | 324 | 33 |
| Switzerland | 8373 | 844 | 101 | 63.8 | 66.6 | 181 | 22 |
| The Netherlands | 16 349 | 1906 | 117 | 64.2 | 67.4 | 368 | 23 |
| Tunisia, Sfax regionb | 1213 | 193 | 159 | 60.5 | 63.0 | 62 | 51 |
| Turkeyd | 79 815 | 11 169 | 140 | 787 | 10 | ||
| UK, Englanda,e | 55 268 | 6454 | 117 | 62.3 | 64.4 | 1618 | 29 |
| UK, Northern Irelanda | 1862 | 225 | 121 | 62.8 | 66.4 | 55 | 30 |
| UK, Scotland | 5405 | 571 | 106 | 59.2 | 61.6 | 171 | 32 |
| UK, Walesa | 3113 | 370 | 119 | 64.9 | 66.5 | 92 | 30 |
| Ukraine | 42 590 | 1246 | 29 | 49.7 | 51.0 | 303 | 7 |
| All countries | 687 084 | 83 311 | 121 | 63.1 | 65.8 | 17 757 | 29 |
When cells are left empty, the data are unavailable and could not be used for the calculation of the summary data.
Patients <20 years of age are not reported. The true incidence counts are, therefore, slightly higher than the counts reported here.
Data on incidence include dialysis patients only.
The incidence is underestimated by ∼29% due to centres not submitting complete data for 2016.
Data on incidence of primary renal disease (DM) is based on 2078 dialysis patients (18.6% of total).
The incidence is underestimated by ∼2% due to a small number of centres not submitting complete data for 2016.
DM, diabetes mellitus as primary renal disease.
FIGURE 1.

Incidence of RRT pmp in 2016, at Day 1, by country/region, unadjusted. The incidence for Czech Republic, Poland, Russia, Slovakia and Tunisia (Sfax region) only includes patients receiving dialysis. For Serbia and England (UK), the incidence is underestimated by, respectively, ∼26% and ∼2% (see Table 1).
FIGURE 2.

Unadjusted (left panel) and adjusted (right panel) incidence of RRT pmp in 2016, at Day 1, by country/region. Registries providing individual patient data are shown as dark bars, and registries providing aggregated data as light bars. Adjustment of incidence was performed by standardizing the rates to the age and gender distribution of the EU27 population [5]. The incidence for Czech Republic, Poland, Russia, Slovakia and Tunisia (Sfax region) only includes patients receiving dialysis. For Serbia and England (UK), the incidence is underestimated by, respectively, ∼26% and ∼2% (see Table 1).
FIGURE 3.
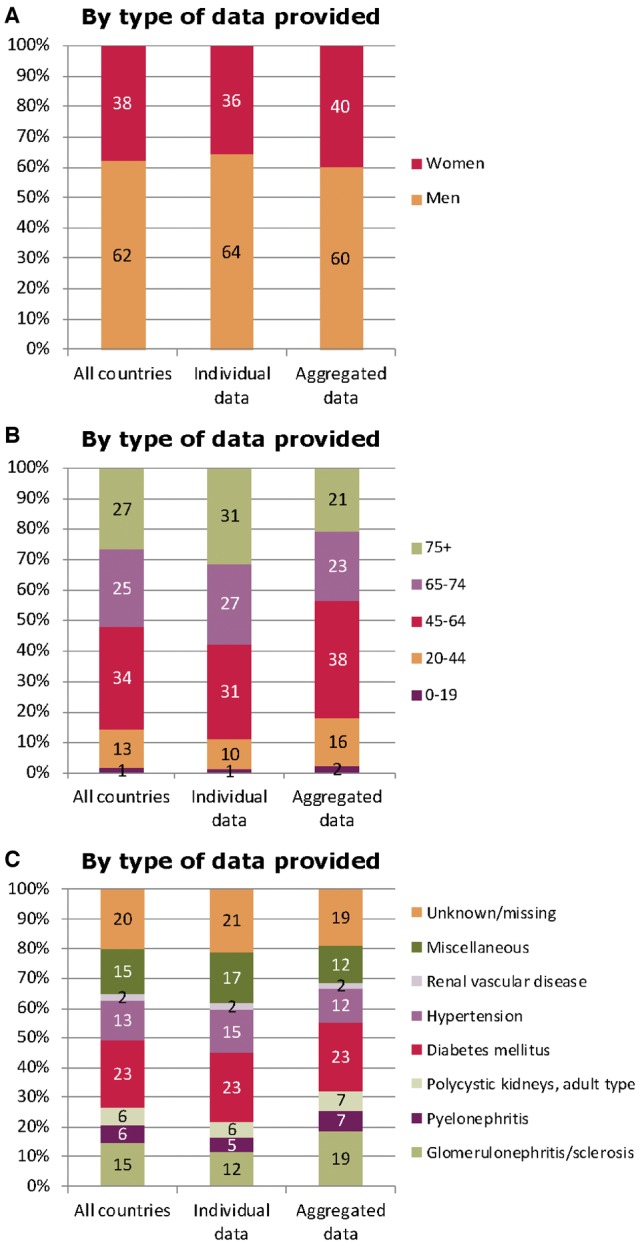
(A) Sex, (B) age and (C) primary renal disease distribution by type of data provided for incident patients accepted for RRT in 2016, at Day 1. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data.
FIGURE 4.
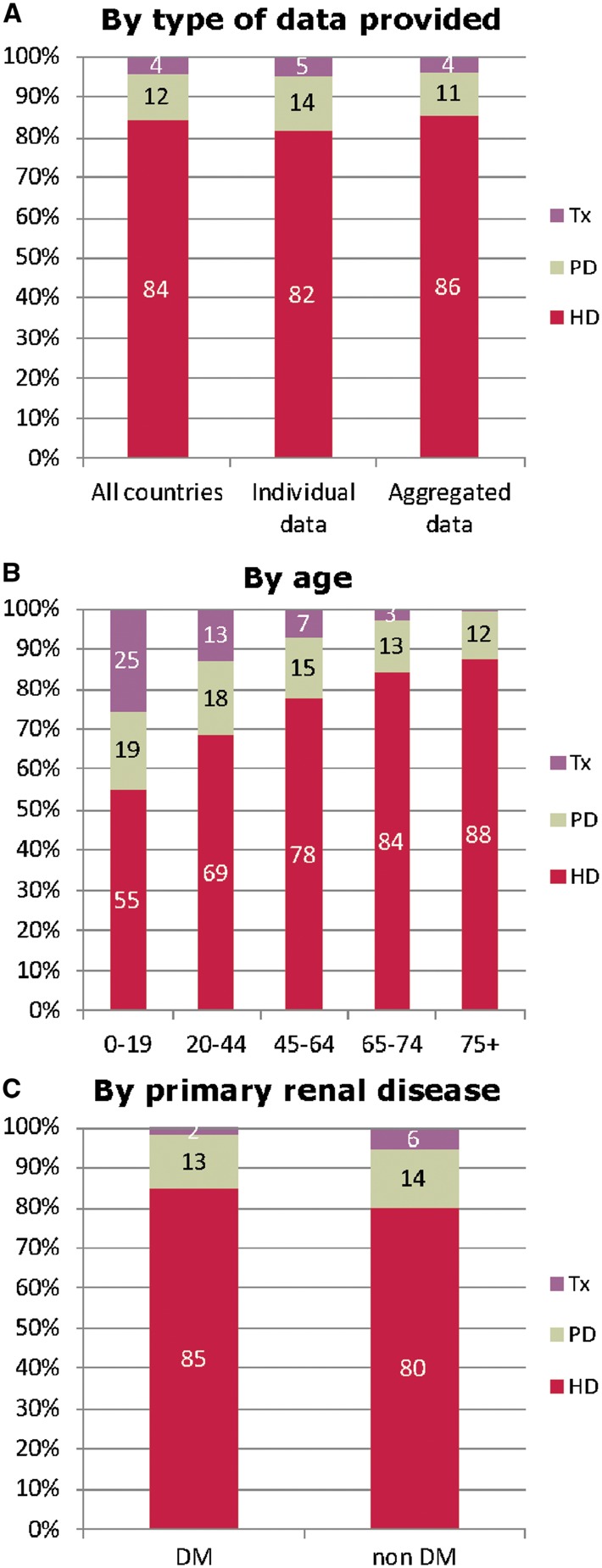
Treatment modality distribution, at Day 1, by (A) type of data provided (B) age and (C) primary renal diagnosis (DM and non-DM) for incident patients accepted for RRT in 2016. Parts (B) and (C) are only based on the data from registries providing individual patient data. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data. Tx, kidney transplant.
FIGURE 5.
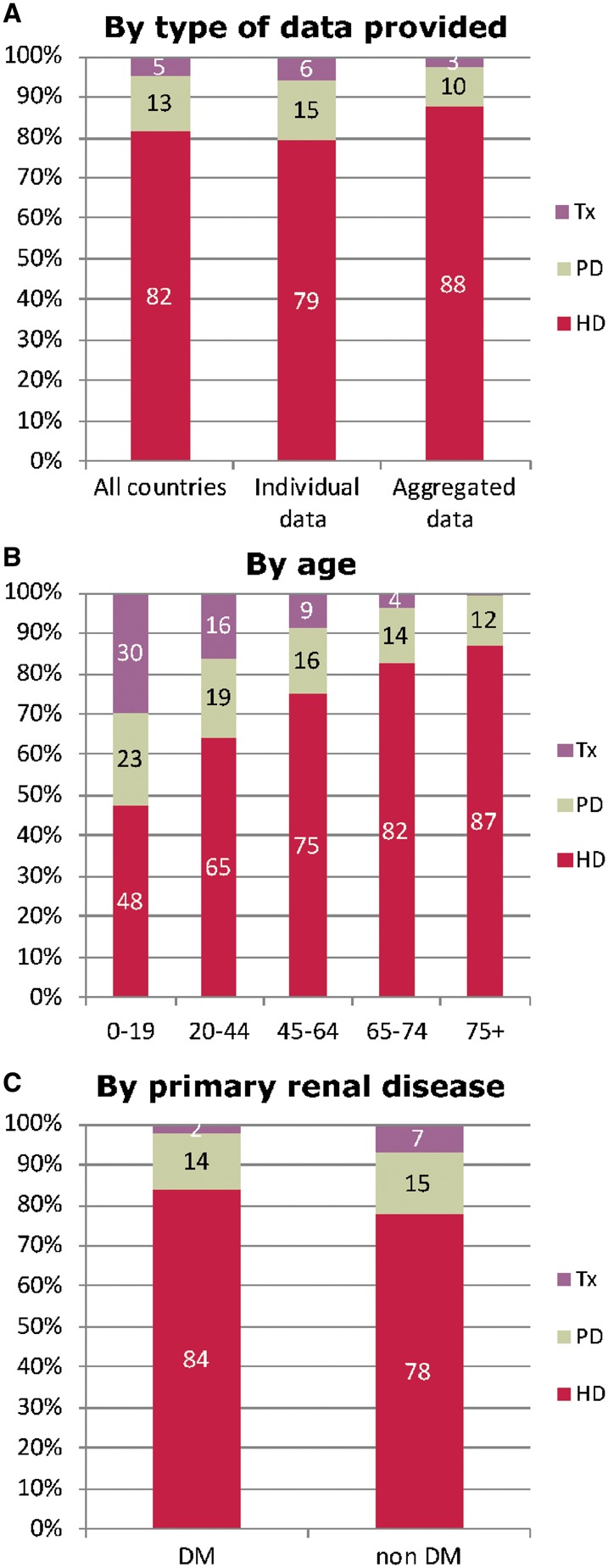
Treatment modality distribution, at Day 91, by (A) type of data provided, (B) age and (C) primary renal diagnosis (DM and non-DM) for incident patients accepted for RRT in 2016. Parts (B) and (C) are only based on the data from registries providing individual patient data. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data. Tx, kidney transplant.
Prevalence of RRT
On 31 December 2016, 564 638 individuals were receiving RRT for ESRD (Table 2), corresponding to an overall unadjusted prevalence of 823 pmp. Again, there was considerable variation between countries, with the highest unadjusted prevalence seen in Portugal (1906 pmp) and the Spanish regions of Catalonia (1399 pmp) and Valencia (1388 pmp; Table 2 and Figures 6 and 7). The unadjusted prevalence of RRT was considerably lower in Ukraine (188 pmp) and Belarus (289 pmp). The top five countries with the highest prevalence of RRT have remained the same since 2014. Of the prevalent patients, 60% were men, 42% were aged ≥65 years and 17% had DM as their primary renal diagnosis (Figure 8). The median age of prevalent patients receiving RRT in all countries and regions combined was 62.4 years, ranging from 50.7 years in Albania to 68.0 years in Israel (Table 2). The majority of prevalent patients (58%) were receiving HD, 37% of patients were living with a kidney transplant and only 5% were receiving PD (Figure 9). Once again the modality of RRT varied considerably between age groups as the proportion of patients with a kidney transplant decreased with increasing age. For those aged 20–44 years, 66% were living with a kidney transplant, whereas this was only 42% for patients aged 65–74 years. Prevalent patients with a primary renal diagnosis of DM were much less likely to be living with a kidney transplant compared with the patients without DM (28% versus 50%).
Table 2.
Prevalence of RRT on 31 December 2016, by country/region, for all primary renal diseases combined and DM types 1 and 2, as count (n) and unadjusted rate pmp, and the mean and median age on 31 December 2016
|
Country/region |
General population covered by the registry in thousands | Prevalent patients on RRT in 2016 |
|||||
|---|---|---|---|---|---|---|---|
| All (n) | All (pmp) | Mean age (years) | Median age (years) | DM (n) | DM (pmp) | ||
| Albania | 2860 | 1450 | 507 | 49.6 | 50.7 | 230 | 80 |
| Austria | 8700 | 9397 | 1080 | 61.2 | 62.7 | 1848 | 212 |
| Belarus | 8172 | 2360 | 289 | 51.6 | 53.0 | 295 | 36 |
| Belgium, Dutch-speakinga | 6509 | 8257 | 1269 | 66.1 | 67.9 | 1426 | 219 |
| Belgium, French-speakinga | 4822 | 6317 | 1310 | 64.9 | 66.5 | 1109 | 230 |
| Bosnia and Herzegovina | 3531 | 2679 | 759 | 59.7 | 61.7 | 548 | 155 |
| Bulgaria | 7102 | 4333 | 610 | ||||
| Croatia | 3755 | 3908 | 1041 | 65.7 | 67.0 | 710 | 189 |
| Cyprus | 857 | ||||||
| Czech Republic | 10 262 | 11 265 | 1098 | ||||
| Denmark | 5784 | 5433 | 939 | 58.8 | 60.4 | 929 | 161 |
| Estonia | 1316 | 919 | 698 | 57.9 | 58.6 | 168 | 128 |
| Finland | 5495 | 4861 | 885 | 59.2 | 61.5 | 1231 | 224 |
| France | 66 860 | 85 471 | 1278 | 62.8 | 64.6 | 13 833 | 207 |
| Georgia | 3720 | 2652 | 713 | 60.1 | 61.2 | 539 | 145 |
| Greece | 10 776 | 13 841 | 1284 | 64.6 | 66.8 | 2637 | 245 |
| Iceland | 335 | 224 | 668 | 54.9 | 56.3 | 26 | 78 |
| Israelb | 8545 | 6566 | 768 | 66.0 | 68.0 | 3035 | 355 |
| Italy (6 of 20 regions) | 20 921 | 24 035 | 1149 | 62.0 | 64.1 | 2654 | 127 |
| Latvia | 1560 | 1038 | 665 | 56.3 | 57.0 | 98 | 63 |
| Lithuania | 2888 | 2193 | 759 | ||||
| Macedonia | 2022 | 1665 | 823 | 58.6 | 60.0 | 273 | 135 |
| Norway | 5235 | 4974 | 950 | 59.4 | 61.5 | 654 | 125 |
| Poland | 38 362 | 31 144 | 812 | 6132 | 160 | ||
| Portugal | 10 358 | 19 738 | 1906 | 66.9 | 67.9 | 3435 | 332 |
| Romaniac | 19 505 | 20 445 | 1048 | 61.2 | 63.0 | 2051 | 105 |
| Russia | 1 43 869 | 44 544 | 310 | 55.5 | 57.0 | 5340 | 37 |
| Serbiad | 7058 | 3833 | 543 | 59.5 | 62.0 | 640 | 91 |
| Slovakiab | 5435 | 3370 | 620 | 63.8 | 66.0 | 1140 | 210 |
| Spain (All regions) | 46 558 | 57 433 | 1234 | 60.0 | 63.2 | 9031 | 194 |
| Spain, Andalusia | 8406 | 10 019 | 1192 | 60.5 | 61.9 | 1548 | 184 |
| Spain, Aragon | 1317 | 1588 | 1205 | 62.9 | 64.0 | 274 | 208 |
| Spain, Asturias | 1041 | 1325 | 1273 | 63.0 | 63.5 | 215 | 207 |
| Spain, Basque country | 2166 | 2704 | 1249 | 62.0 | 63.8 | 304 | 140 |
| Spain, Cantabriaa | 582 | 686 | 1179 | 62.6 | 64.0 | 91 | 156 |
| Spain, Castile and Leóna | 2445 | 2858 | 1169 | 64.8 | 65.8 | 505 | 207 |
| Spain, Castile-La Manchaa | 2045 | 2357 | 1153 | 62.5 | 63.3 | 373 | 182 |
| Spain, Catalonia | 7523 | 10 523 | 1399 | 63.0 | 64.8 | 1499 | 199 |
| Spain, Community of Madrid | 6467 | 7450 | 1152 | 61.9 | 63.2 | 1323 | 205 |
| Spain, Extremadura | 1088 | 1263 | 1161 | 62.0 | 62.3 | 191 | 176 |
| Spain, Galicia | 2715 | 3619 | 1333 | 62.5 | 64.0 | 598 | 220 |
| Spain, Navarrea | 639 | 837 | 1310 | 62.5 | 64.0 | 128 | 200 |
| Spain, Region of Murcia | 1465 | 1949 | 1331 | 62.1 | 63.3 | 274 | 187 |
| Spain, Valencian region | 4960 | 6883 | 1388 | 63.3 | 65.2 | 933 | 188 |
| Sweden | 9923 | 9718 | 979 | 59.9 | 62.0 | 1742 | 176 |
| Switzerlande | 8373 | 7503 | 896 | 62.1 | 63.9 | 1159 | 138 |
| The Netherlands | 16 349 | 17 117 | 1047 | 60.5 | 62.4 | 2229 | 136 |
| Tunisia, Sfax regionb | 1213 | 946 | 780 | 58.2 | 59.0 | 200 | 165 |
| Turkeyf | 79 815 | 74 475 | 933 | 2719 | 34 | ||
| UK, Englanda,g | 55 268 | 52 641 | 952 | 58.8 | 59.2 | 8884 | 161 |
| UK, Northern Irelanda | 1862 | 1784 | 958 | 58.7 | 58.4 | 280 | 150 |
| UK, Scotland | 5405 | 5028 | 930 | 56.8 | 57.7 | 826 | 153 |
| UK, Walesa | 3113 | 3062 | 984 | 59.5 | 60.3 | 503 | 162 |
| Ukraine | 42 590 | 8019 | 188 | 49.5 | 51.0 | 1280 | 30 |
| All countries | 687 084 | 564 638 | 823 | 60.6 | 62.4 | 79 834 | 134 |
When cells are left empty, the data are unavailable and could not be used for the calculation of the summary data.
Patients <20 years of age are not reported. The true prevalent counts are therefore slightly higher than the counts reported here.
Data on prevalence include dialysis patients only.
The prevalence is underestimated by ∼3% due to an estimated 30% under-reporting of patients living with a functioning graft.
The prevalence is underestimated by ∼29% due to centres not submitting complete data for 2016.
The prevalence is underestimated by ∼6% due to an estimated 11% under-reporting of patients living with a functioning graft.
Data on the prevalence of primary renal disease (DM) is based on 8043 dialysis patients (10.8% of total)
The prevalence is underestimated by ∼1% due to a small number of centres not submitting complete data for 2016.
DM, diabetes mellitus as primary renal disease.
FIGURE 6.

Prevalence of RRT pmp on 31 December 2016 by country/region. The prevalence for Israel only includes patients receiving dialysis. For Romania, Serbia, Switzerland and England (UK), the prevalence is underestimated by, respectively, ∼30, ∼29, ∼6 and ∼1% (see Table 2).
FIGURE 7.

Unadjusted (left panel) and adjusted (right panel) prevalence of RRT pmp on 31 December 2016 by country/region. Registries providing individual patient data are shown as dark bars, and registries providing aggregated data as light bars. Adjustment of the prevalence was performed by standardizing the prevalence to the age and gender distribution of the EU27 population [5]. The prevalence for Israel only includes patients receiving dialysis. For Romania, Serbia, Switzerland and England (UK), the prevalence is underestimated by, respectively, ∼30, ∼29, ∼6 and ∼1% (see Table 2).
FIGURE 8.
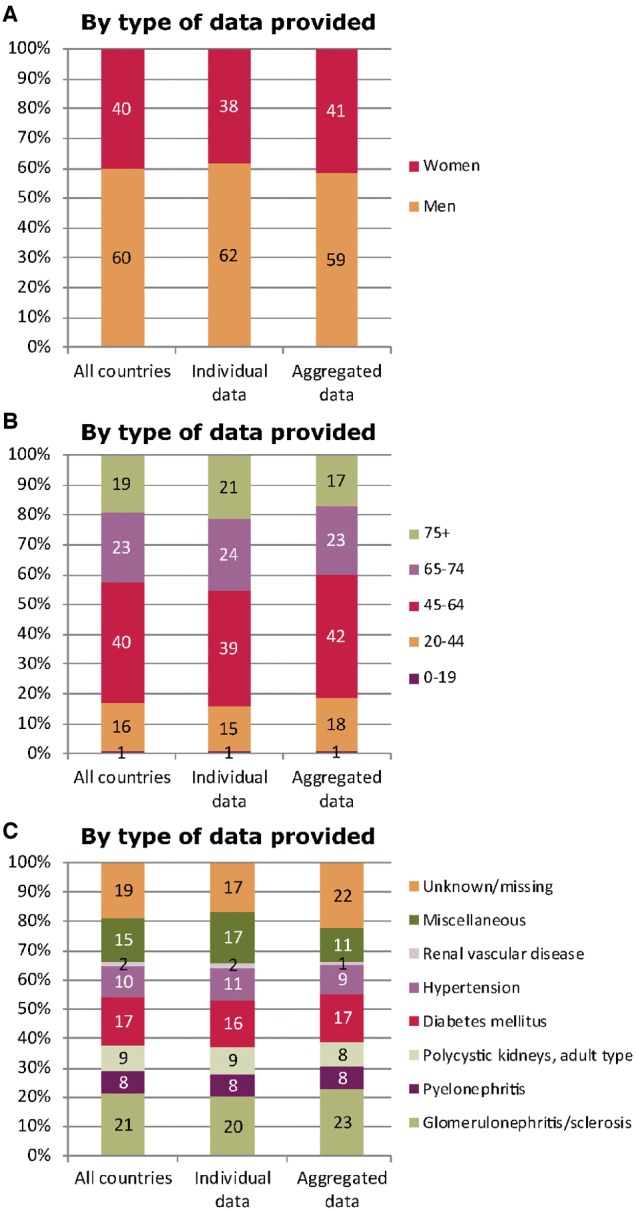
(A) Sex, (B) age and (C) primary renal disease distribution by type of data provided for prevalent patients on RRT on 31 December 2016. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data.
FIGURE 9.
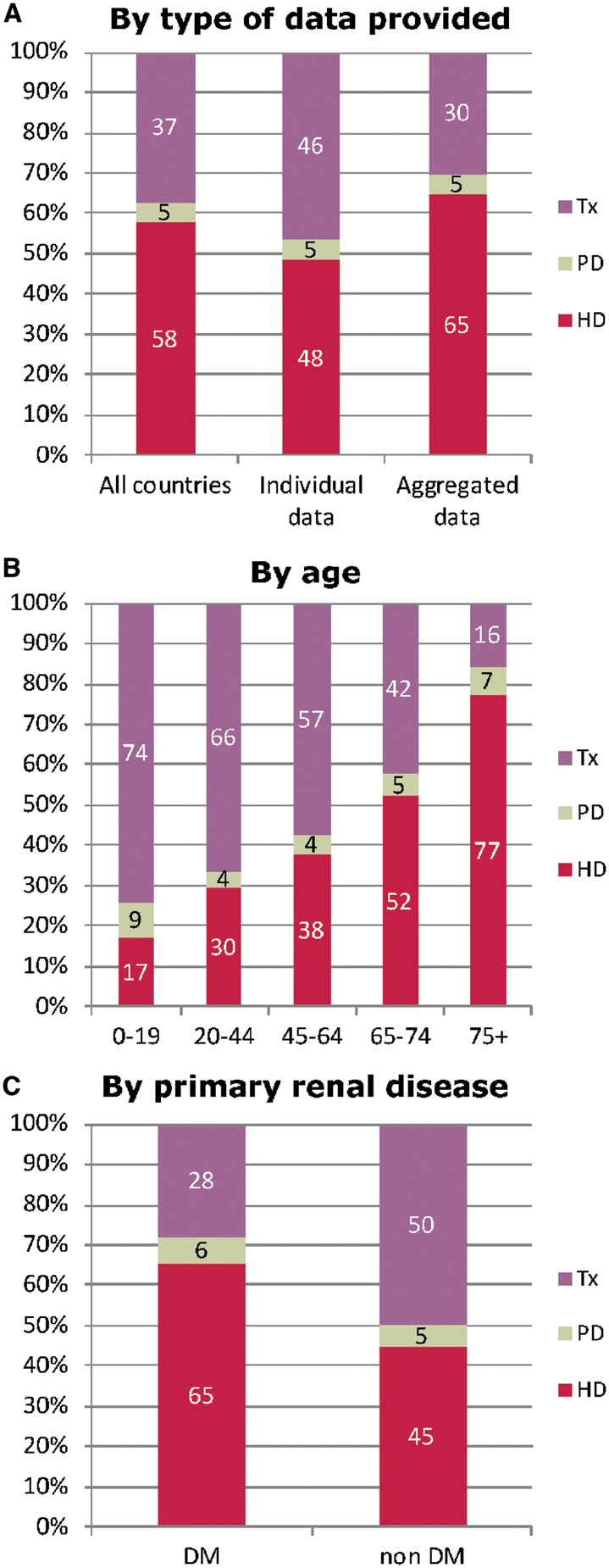
Treatment modality distribution by (A) type of data provided (B) age and (C) primary renal diagnosis (DM and non-DM) for prevalent patients on RRT on 31 December 2016. Parts (B) and (C) are only based on the data from registries providing individual patient data. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data. Tx, kidney transplant.
Kidney transplantation
In 2016, 22 046 kidney transplantations were performed, which equated to an overall unadjusted transplant rate of 32 pmp (Figure 10). Again there was considerable variation between countries/regions with unadjusted kidney transplant rates well over 70 pmp in several Spanish regions, and very low unadjusted kidney transplant rates in Ukraine (3 pmp) and Macedonia (3 pmp). Overall, the unadjusted deceased donor kidney transplant rate was more than twice that of the unadjusted living donor transplant rate (22 pmp versus 9 pmp; 70% versus 30%; Figure 11). The highest unadjusted rates of deceased donor kidney transplants were seen in some Spanish regions (>70 pmp; Figure 12), whereas the highest unadjusted rate of living donor transplants was seen in Northern Ireland (38 pmp), the Netherlands (33 pmp) and Turkey (33 pmp; Figure 12).
FIGURE 10.

Kidney transplants performed in 2016, as counts and pmp (unadjusted) by country/region. Registries providing individual patient data are shown as dark bars, and registries providing aggregated data as light bars. Data based on patients aged ≥20 years in Dutch-speaking Belgium, French-speaking Belgium, the Spanish regions of Cantabria, Castile and León, Castile-La Mancha and Navarre and UK: England, Northern Ireland and Wales. The total count for Austria is based on residents and non-residents. For Romania, Serbia, Switzerland and England (UK), the overall kidney transplant rate is underestimated by, respectively, ∼30, ∼36, ∼6 and ∼7%.
FIGURE 11.
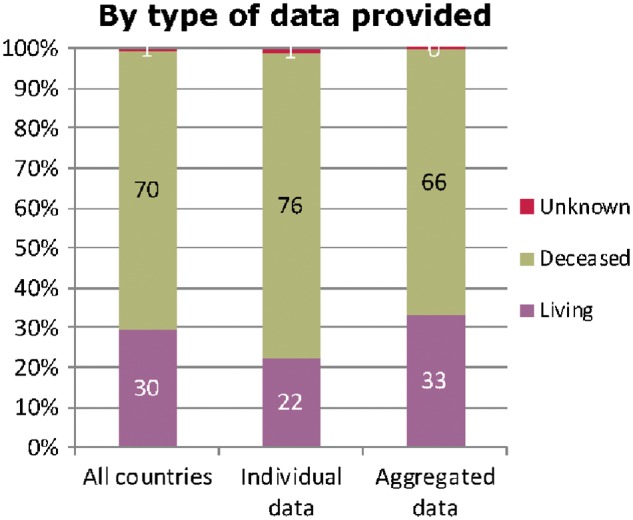
Donor-type distribution for kidney transplants performed in 2016, by type of data provided. See Appendix A1 for a list of countries and regions supplying individual patient data or aggregated data.
FIGURE 12.

Deceased donor (left panel) and living donor (right panel) kidney transplants performed in 2016 pmp, by country/region, unadjusted. Registries providing individual patient data are shown as dark bars, and registries providing aggregated data as light bars. Data based on patients aged ≥20 years in Dutch-speaking Belgium, French-speaking Belgium, the Spanish regions of Cantabria, Castile and León, Castile-La Mancha and Navarre and UK: England, Northern Ireland and Wales. The total count for Austria is based on residents and non-residents. For Romania, Switzerland and England (UK), the kidney transplant rate is underestimated by, respectively, ∼30, ∼6 and ∼7%. For Serbia, the transplant rate is underestimated by ∼29% for deceased donor transplants and by ∼39% for living donor transplants.
Survival of patients receiving RRT
For patients commencing RRT in the period 2007–11, the 5-year unadjusted patient survival probability for all RRT modalities combined was 50.5% [95% confidence interval (CI) 50.4–50.6]. For patients commencing RRT with dialysis between 2007 and 2011, the 5-year unadjusted patient survival probability was 42.1% (95% CI 42.0–42.3). Adjusted analyses for patient survival on HD and PD revealed higher survival probabilities in the first 3 years for patients receiving PD (Figure 13). For those with a kidney transplant, 5-year adjusted patient and graft survival were higher for living donor transplants compared with deceased donor transplants: 94.6% (95% CI 94.1–95.1) versus 91.9% (95% CI 91.6–92.3) for patient survival and 86.7% (95% CI 85.9–87.4) versus 80.9% (95% CI 80.4–81.4) for graft survival. See Table 3 for a description of the adjustments made and the countries/regions included in these analyses.
FIGURE 13.

Patient survival of patients starting HD and PD between 2007 and 2011 from Day 91 (left panel) and patients receiving a first kidney transplant from a living or deceased donor between 2007 and 2011 (right panel). Survival on dialysis was censored for transplantation, and adjusted using fixed values for age (67 years), gender (63% men) and primary renal disease (24% DM, 19% hypertension/renal vascular disease, 11% glomerulonephritis and 46% other causes). Survival after kidney transplantation was adjusted using fixed values for age (50 years), gender (63% men) and primary renal disease (14% DM, 10% hypertension/renal vascular disease, 23% glomerulonephritis and 53% other causes). These figures are based on the data from the following registries providing individual patient data: Austria, Belgium (Dutch-speaking), Belgium (French-speaking), Denmark, Finland, France, Greece, Iceland, Norway, Spain (Andalusia), Spain (Aragon), Spain (Asturias), Spain (Basque country), Spain (Cantabria), Spain (Castile and León), Spain (Castile-La Mancha), Spain (Catalonia), Spain (Extremadura), Spain (Galicia), Spain (Community of Madrid), Spain (Valencian region), Sweden, the Netherlands and the UK (all countries).
Table 3.
The survival probabilities at 1, 2 and 5 years by treatment modality and cohort, from Day 1 of the start of RRT/dialysis, or from the day of kidney transplantation
| Survival probabilities as percentage (95% CI) |
|||||
|---|---|---|---|---|---|
| Cohort: 2007–11 |
Cohort: 2010–14 |
||||
| Survival type | 1 year | 2 years | 5 years | 1 year | 2 years |
| Patient survival on RRT | |||||
| Unadjusted | 83.6 (83.4–83.7) | 73.2 (73.1–73.4) | 50.5 (50.4–50.6) | 84.6 (84.4–84.7) | 74.6 (74.5–74.8) |
| Adjusteda | 86.3 (86.1–86.4) | 76.6 (76.4–76.9) | 51.7 (51.5–52.0) | 87.1 (86.9–87.3) | 77.9 (77.7–78.1) |
| Patient survival on dialysis | |||||
| Unadjusted | 82.5 (82.4–82.7) | 70.8 (70.6–71.0) | 42.1 (42.0–42.3) | 83.5 (83.3–83.6) | 72.1 (71.9–72.2) |
| Adjusteda | 84.7 (84.5–84.9) | 74.0 (73.7–74.2) | 45.5 (45.2–45.8) | 85.9 (85.7–86.0) | 75.6 (75.4–75.8) |
| Patient survival after first kidney transplantation (deceased donor) | |||||
| Unadjusted | 96.3 (96.1–96.5) | 94.4 (94.1–94.6) | 87.7 (87.3–88.0) | 96.3 (96.1–96.5) | 94.3 (94.0–94.5) |
| Adjustedb | 97.7 (97.5–97.9) | 96.4 (96.2–96.6) | 91.9 (91.6–92.3) | 97.9 (97.8–98.1) | 96.7 (96.5–96.9) |
| Graft survival after first kidney transplantation (deceased donor) | |||||
| Unadjusted | 91.1 (90.7–91.4) | 88.2 (87.9–88.5) | 78.7 (78.3–79.1) | 91.0 (90.8–91.3) | 88.0 (87.7–88.3) |
| Adjustedb | 92.1 (91.8–92.4) | 89.6 (89.2–89.9) | 80.9 (80.4–81.4) | 92.6 (92.3–92.9) | 90.0 (89.7–90.4) |
| Patient survival after first kidney transplantation (living donor) | |||||
| Unadjusted | 98.7 (98.4–98.9) | 97.8 (97.4–98.0) | 94.1 (93.6–94.5) | 99.1 (98.9–99.2) | 98.1 (97.9–98.4) |
| Adjustedb | 98.8 (98.6–99.1) | 98.0 (97.7–98.3) | 94.6 (94.1–95.1) | 99.2 (99.1–99.4) | 98.5 (98.2–98.7) |
| Graft survival after first kidney transplantation (living donor) | |||||
| Unadjusted | 95.9 (95.5–96.3) | 94.1 (93.6–94.5) | 87.5 (86.9–88.0) | 96.8 (96.5–97.1) | 95.1 (94.7–95.4) |
| Adjustedb | 95.6 (95.2–96.1) | 93.7 (93.2–94.2) | 86.7 (85.9–87.4) | 96.6 (96.3–97.0) | 94.8 (94.4–95.2) |
This is based on the data from the following renal registries providing individual patient data: Austria, Belgium (Dutch-speaking), Belgium (French-speaking), Denmark, Finland, France, Greece, Iceland, Norway, Spain (Andalusia), Spain (Aragon), Spain (Asturias), Spain (Basque country), Spain (Cantabria), Spain (Castile and León), Spain (Castile-La Mancha), Spain (Catalonia), Spain (Extremadura), Spain (Galicia), Spain (Community of Madrid), Spain (Valencian region), Sweden, the Netherlands and the UK (all countries).
Analyses were adjusted using fixed values: age (67 years), gender (63% men) and primary renal disease (24% DM, 19% hypertension/renal vascular disease, 11% glomerulonephritis and 46% other causes).
Analyses were adjusted using fixed values: age (50 years), gender (63% men) and primary renal disease (14% DM, 10% hypertension/renal vascular disease, 23% glomerulonephritis and 53% other causes).
Expected remaining lifetime
There is still a substantial difference in the expected remaining lifetime between the general population and those receiving dialysis (Figure 14). Patients aged 20–44 years receiving dialysis are expected to live only one-third of the expected remaining lifetime of the age-matched general population, which is about 33 years less. The prospect is even worse for patients aged 45–64 years, as they are expected to live only a quarter as long as their age-matched counterparts in the general population (∼21 years less). Patients living with a kidney transplant fare better than those receiving dialysis. However, the life expectancy of the transplant recipients aged 20–44 years is still ∼30% less than that of the age-matched general population (∼15 years less). Thus, as the age of the transplant recipient increases, the relative difference in the expected remaining lifetime from that of the age-matched general population also increases although the absolute difference decreases.
FIGURE 14.

Expected remaining lifetimes of the general population (cohort 2012–16), and of prevalent dialysis and kidney transplant patients (cohort 2012–16), by age and gender. This figure is based on data from the following registries providing individual patient data: Austria, Belgium (Dutch-speaking), Belgium (French-speaking), Denmark, Finland, France, Greece, Iceland, Norway, Spain (Andalusia), Spain (Aragon), Spain (Asturias), Spain (Basque Country), Spain (Cantabria), Spain (Castile and León), Spain (Castile-La Mancha), Spain (Catalonia), Spain (Extremadura), Spain (Galicia), Spain (Community of Madrid), Spain (Valencian region), Sweden, the Netherlands and the UK (all countries).
Sex comparisons
Figures 15–31 showing comparisons of the sexes are based on the data from 32 national or regional renal registries from 17 countries that provided individual patient data, representing 33.8% of the 2016 European general population.
FIGURE 15.
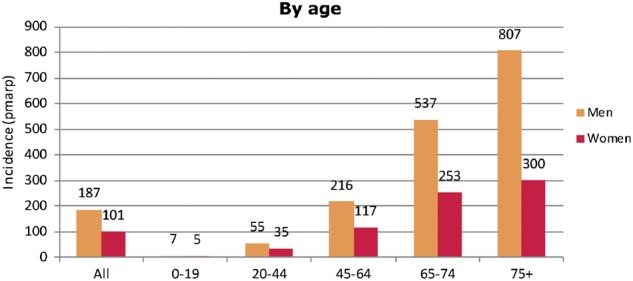
Incidence of RRT per million age-related population (pmarp) in 2016, at Day 1, by age and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
In 2016, 26 446 men and 14 820 women commenced RRT resulting in a higher unadjusted incidence among men (187 pmp) than women (101 pmp). This was the case for all age groups, with the incidence in men aged ≥75 years (807 pmp) being 2.7 times that of women aged ≥75 years (300 pmp; Figure 15). In men and women commencing RRT, the distribution of the age groups was very similar (Figure 16). About 36% of patients commencing RRT were female, decreasing from around 39% of patients <45 years at the start of RRT to about 36% of patients aged ≥45 years (Figure 17).
FIGURE 16.
Age distribution by sex for incident patients accepted for RRT in 2016, at Day 1. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 17.
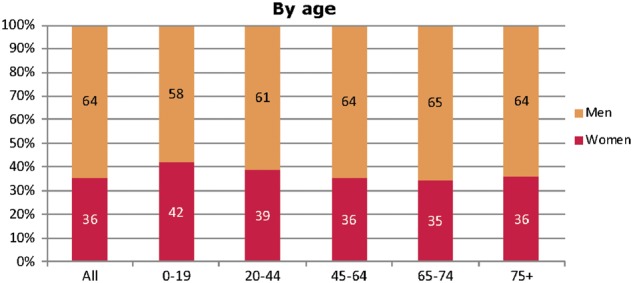
Sex distribution by age for incident patients accepted for RRT in 2016, at Day 1. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
Diabetes was the most frequent primary renal disease in both men and women starting RRT (Figure 18). The incidence of men starting RRT for ESRD due to glomerulonephritis/sclerosis (23 pmp) and hypertension (29 pmp) was more than double that of their female counterparts (10 and 13 pmp, respectively), while the incidence of polycystic kidney disease in men (9 pmp) was only about 30% higher than in women (7 pmp). When viewed by sex, the distribution of the primary renal disease was similar. Of the men commencing RRT, 16% had hypertension and 12% had glomerulonephritis/sclerosis, and for women this was 13 and 10%, respectively (Figure 19).
FIGURE 18.
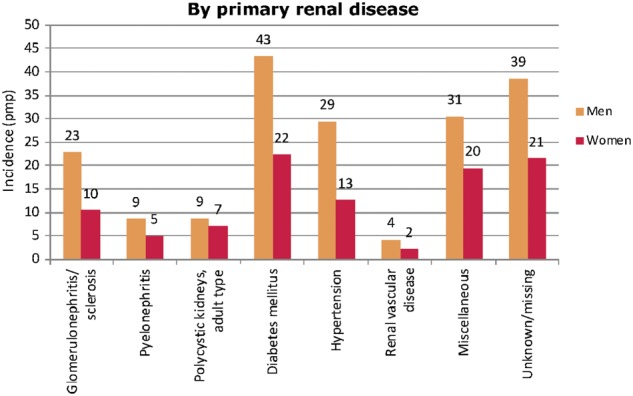
Incidence of RRT pmp in 2016, at Day 1, by primary renal disease and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 19.
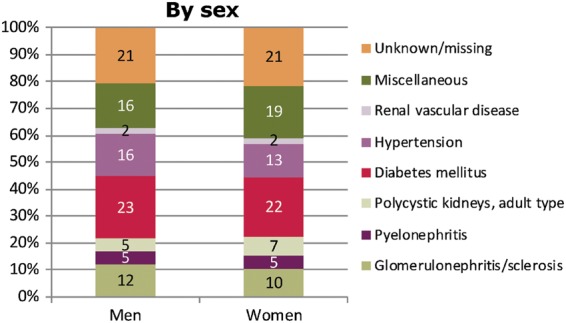
Primary renal disease distribution by sex for incident patients accepted for RRT in 2016, at Day 1. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
The incidence of all treatment modalities was higher among men than women (Figure 20). Of the men and women initiating RRT in 2016, the majority started with HD (82 and 81%, respectively; Figure 21). Although more men (8 pmp) than women (5 pmp) received a pre-emptive transplant, the percentage of patients starting RRT with a pre-emptive transplant was similar among men (4%) and women (5%).
FIGURE 20.
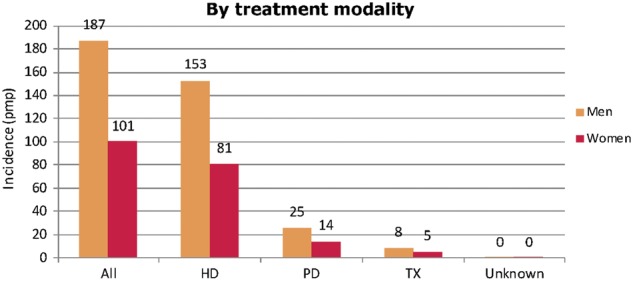
Incidence of RRT pmp in 2016, at Day 1, by treatment modality and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 21.
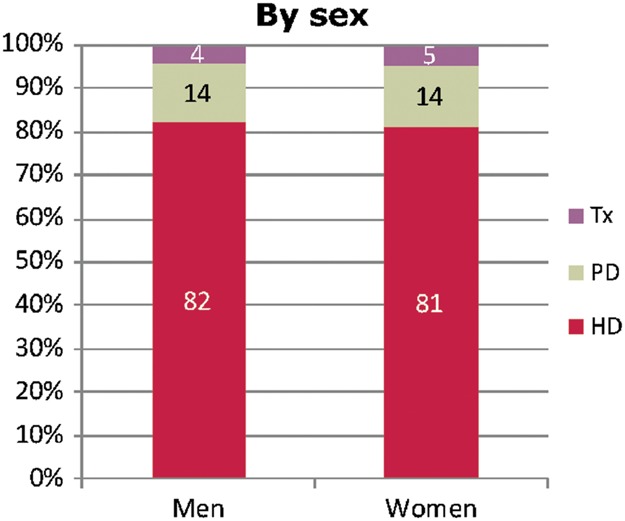
Treatment modality distribution by sex for incident patients accepted for RRT in 2016, at Day 1. Figure is only based on the data from registries providing individual patient data (see Appendix A1). Tx, kidney transplant.
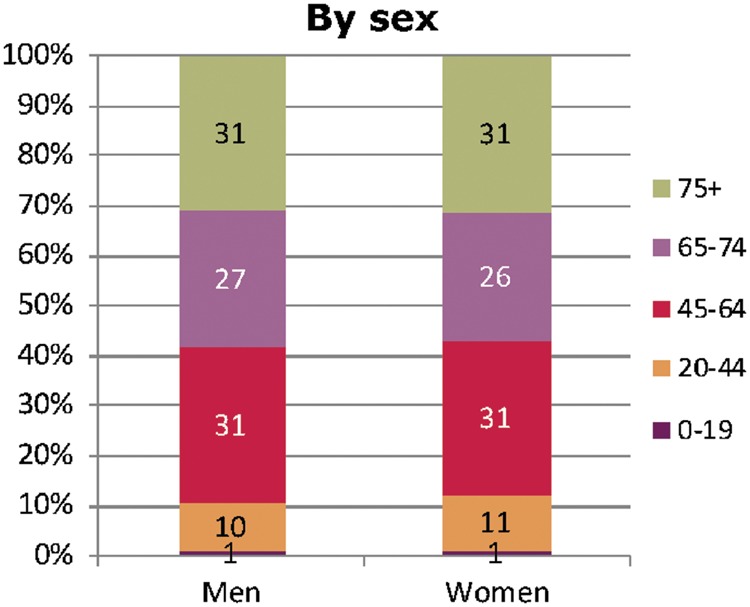
On 31 December 2016, 195 810 men and 121 755 women were receiving RRT for ESRD, resulting in a higher prevalence of RRT among men (1381 pmp) than women (827 pmp), which was the case for all age groups (Figure 22). In men, the highest prevalence was found in the group aged ≥75 years, whereas in women the highest prevalence was found in the group aged 65–74 years. The age distribution of patients receiving RRT was similar for both sexes, with most patients in the 45- to 64-year age group (39%; Figure 23). The percentage of women within the different age groups varied between 37% among patients aged 65–74 years and 40% among patients aged 0–19 years (Figure 24). The prevalence of men on RRT with glomerulonephritis/sclerosis and hypertension (301 and 167 pmp) was more than twice that of women (140 and 75 pmp; Figure 25). For men receiving RRT, the most frequent primary renal disease was glomerulonephritis/sclerosis (22%), while for women their most frequent primary renal disease category was ‘miscellaneous’ (Figure 26, Appendix 2). For both men and women, the majority of patients were receiving HD (668 and 399 pmp), and slightly fewer men and women were living with a kidney transplant (642 and 382 pmp, respectively; Figure 27). The distribution of treatment modalities was similar across the sexes (Figure 28).
FIGURE 22.
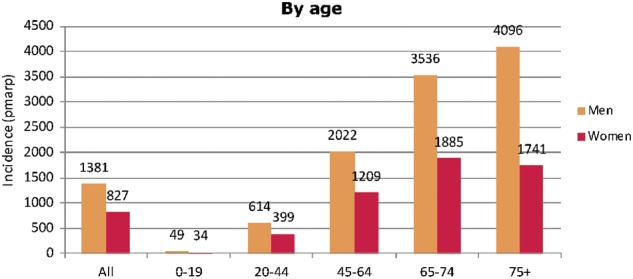
Prevalence of RRT pmarp on 31 December 2016, by age and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 23.
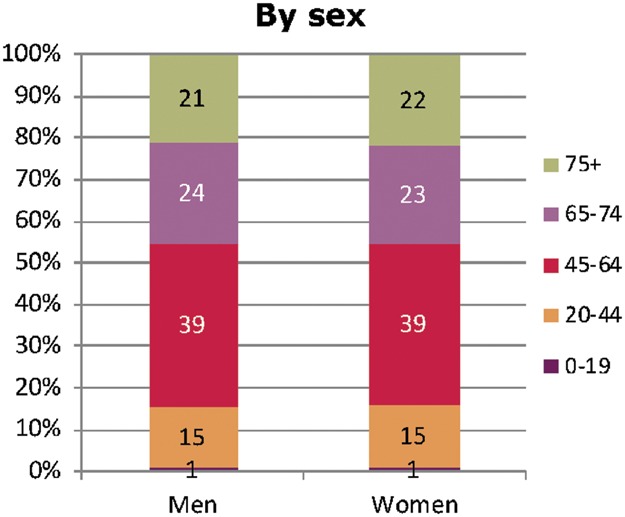
Age distribution by sex for prevalent patients on RRT on 31 December 2016. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 24.
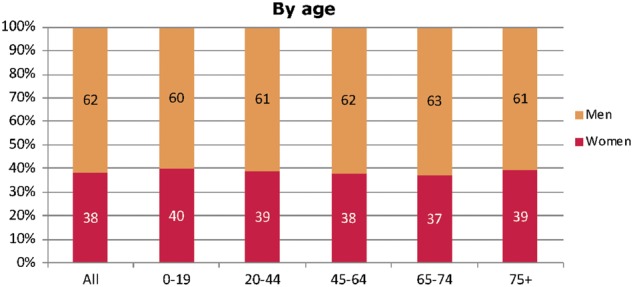
Sex distribution by age for prevalent patients on RRT on 31 December 2016. Figure is only based on data from registries providing individual patient data (see Appendix A1).
FIGURE 25.
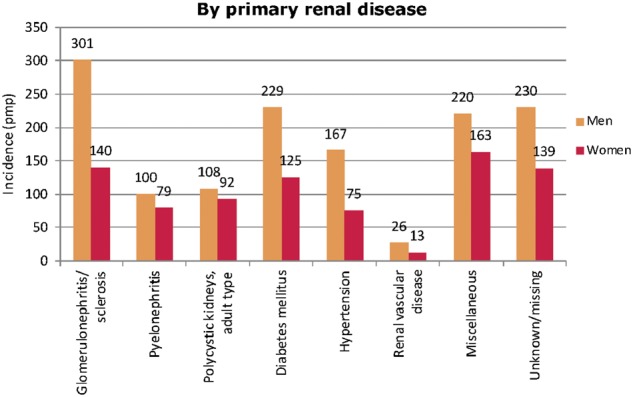
Prevalence of RRT pmp on 31 December 2016, by primary renal disease and sex. Figure is only based on data from registries providing individual patient data (see Appendix A1).
FIGURE 26.
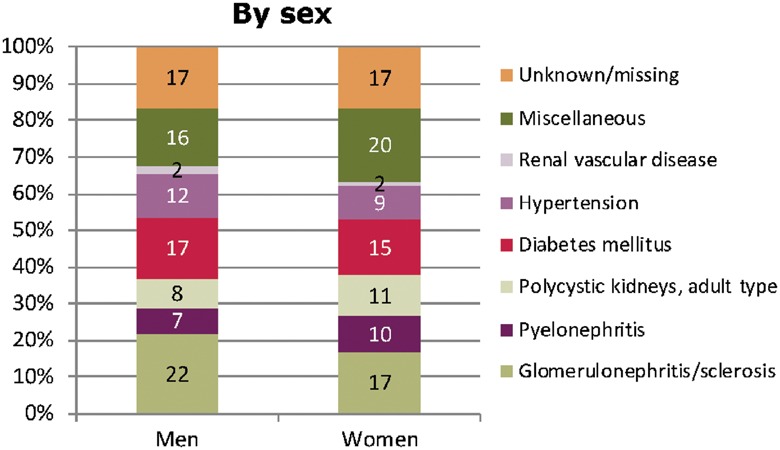
Primary renal disease distribution by sex for prevalent patients on RRT on 31 December 2016. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 27.
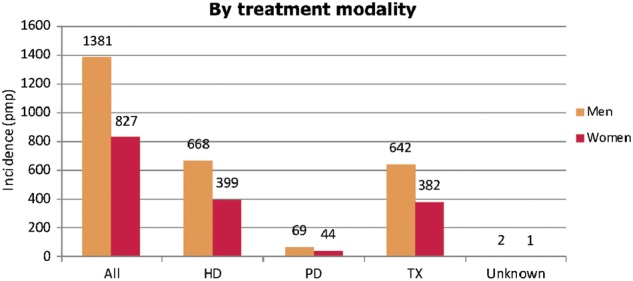
Prevalence of RRT pmp on 31 December 2016, by treatment modality and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 28.
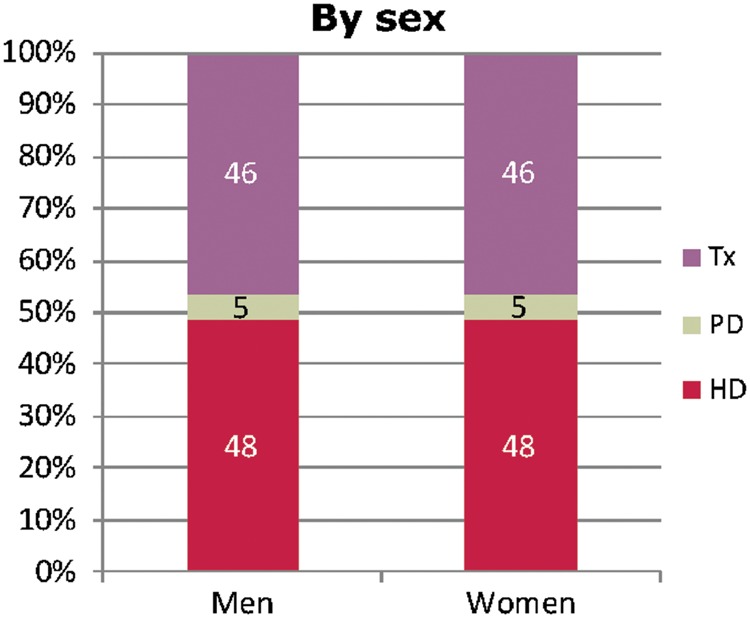
Treatment modality distribution by sex for prevalent patients on RRT on 31 December 2016. Figure is only based on the data from registries providing individual patient data (see Appendix A1). Tx, kidney transplant.
In 2016, 8355 kidney transplantations were performed in men, and 4827 in women, equating to transplant rates of 59 and 33 pmp, respectively (Figure 29). For men, 22% of the transplants came from living donors, and for women 24% (Figure 30).
FIGURE 29.
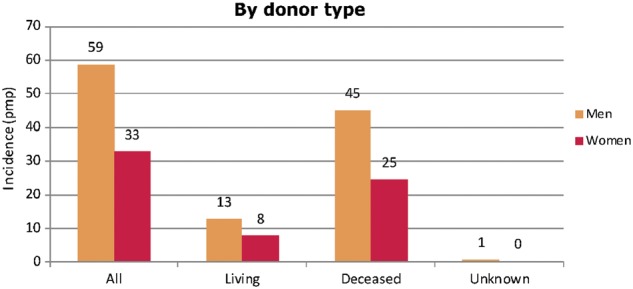
Kidney transplants performed pmp in 2016, by donor type and sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
FIGURE 30.
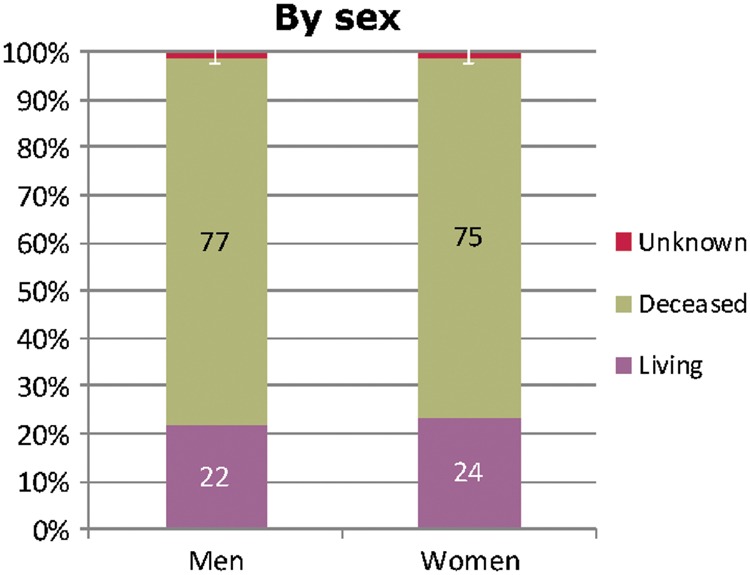
Donor-type distribution for kidney transplants performed in 2016, by sex. Figure is only based on the data from registries providing individual patient data (see Appendix A1).
For patients commencing RRT with dialysis in the period 2007–11, for both HD and PD, the adjusted patient survival probabilities were higher for women than for men (Figure 31). For both men and women receiving a kidney transplant in the period 2007–11, the adjusted patient survival was higher with a living donor transplant compared with a deceased donor transplant, and this difference was more prominent in men than in women.
FIGURE 31.

Patient survival of men and women starting HD and PD between 2007 and 2011 from Day 91 (left panel) and men and women receiving a first kidney transplant from a living or deceased donor between 2007 and 2011 (right panel). Survival on dialysis was adjusted using fixed values for age (67 years) and primary renal disease (24% diabetes mellitus, 19% hypertension/renal vascular disease, 11% glomerulonephritis and 46% other causes). Survival after kidney transplantation was adjusted using fixed values for age (50 years) and primary renal disease (14% diabetes mellitus, 10% hypertension/renal vascular disease, 23% glomerulonephritis and 53% other causes). These figures are based on the data from the following registries providing individual patient data: Austria, Belgium (Dutch-speaking), Belgium (French-speaking), Denmark, Finland, France, Greece, Iceland, Norway, Spain (Andalusia), Spain (Aragon), Spain (Asturias), Spain (Basque country), Spain (Cantabria), Spain (Castile and León), Spain (Castile-La Mancha), Spain (Catalonia), Spain (Extremadura), Spain (Galicia), Spain (Community of Madrid), Spain (Valencian region), Sweden, the Netherlands and the UK (all countries).
AFFILIATED REGISTRIES
Albanian Renal Registry (M. Barbullushi, A. Idrizi and E. Bolleku Likaj); Austrian Dialysis and Transplant Registry [OEDTR] (R. Kramar); Belarus Renal Registry (K.S. Komissarov, K.S. Kamisarau and A.V. Kalachyk); Dutch-speaking Belgian Society of Nephrology [NBVN] (M. Couttenye, F. Schroven and J. De Meester); French-speaking Belgian Society of Nephrology [GNFB] (JM. des Grottes and F. Collart); Renal Registry Bosnia and Herzegovina (H. Resić, Z. Stipancic and N. Petkovic); Bulgaria (E.S. Vazelov and I. Velinova); Croatian Registry of renal replacement therapy [CRRRT] (I. Bubić and M. Knotek); Cyprus Renal Registry (K. Ioannou and all of the renal units providing data); Czech Republic: Registry of Dialysis Patients [RDP] (I. Rychlík, J. Potucek, and F. Lopot); Danish Nephrology Registry [DNS] (J.G. Heaf); Estonian Society of Nephrology (Ü. Pechter, K. Lilienthal and M. Rosenberg); Finnish Registry for Kidney Diseases (P. Finne, A. Pylsy and P.H. Groop); France: The Epidemiology and Information Network in Nephrology [REIN] (M. Lassalle and C. Couchoud); Georgian Renal Registry (N. Kantaria and Dialysis Nephrology and Transplantation Union of Georgia); Hellenic Renal Registry (N. Afentakis); Icelandic ESRD Registry (R. Palsson); Israel National Registry of Renal Replacement Therapy (R. Dichtiar, T. Shohat and E. Golan); Italian Registry of Dialysis and Transplantation [RIDT] (A. Limido, M. Nordio and M. Postorino); Latvian Renal Registry (H. Cernevskis, V. Kuzema and A. Silda); Lithuanian Renal Registry (I.A. Bumblyte, V. Vainauskas and E. Žiginskienė); Macedonian Renal Registry (M. Nedelkovska, N. Dimitriova and O. Stojceva-Taneva); Norwegian Renal Registry (T. Leivestad, A.V. Reisæter and A. Åsberg); Polish Renal Registry (G. Korejwo, A. Dębska-Ślizień and R. Gellert); Portuguese Renal Registry (F. Macário and A. Ferreira); Romanian Renal Registry [RRR] (G. Mircescu, L. Garneata and E. Podgoreanu); Russian Renal Registry (N. Tomilina, A. Andrusev and H. Zakharova); Renal Registry in Serbia (N. Maksimovic, R. Naumovic, all of the Serbian renal units, and the Serbian Society of Nephrology); Slovakian Renal Registry (V. Spustová, I. Lajdová and M. Karolyova); Spanish RRT National Registry at ONT, Spanish Regional Registries and Spanish Society of Nephrology (SEN) and the regional registries of Andalusia [SICATA] [P. Castro de la Nuez (on behalf of all users of SICATA)], Aragon (F. Arribas Monzón, J.M. Abad Diez and J.I. Sanchez Miret), Asturias (R. Alonso de la Torre, J.R. Quirós and RERCA Working Group), Basque country [UNIPAR] (Á. Magaz, J. Aranzabal, M. Rodrigo and I. Moina), Cantabria (J.C. Ruiz San Millán, O. Garcia Ruiz and C. Piñera Haces), Castile and León (M.A. Palencia García), Castile-La Mancha (G. Gutiérrez Ávila and I. Moreno Alía), Catalonia [RMRC] (E. Arcos, J. Comas and J. Tort), Extremadura (J.M. Ramos Aceitero and M.A. García Bazaga), Galicia (E. Bouzas-Caamaño), Community of Madrid (M.I. Aparicio de Madre), Renal Registry of the Region of Murcia (C. Santiuste de Pablos and I. Marín Sánchez), Navarre (M.F. Slon Roblero, J. Manrique Escola and J. Arteaga Coloma) and the Valencian region [REMRENAL] (M. Ferrer Alamar, N. Fuster Camarena and J. Pérez Penadés); Swedish Renal Registry [SNR] (K.G. Prütz, M. Stendahl, M. Evans, S. Schön, T. Lundgren and M. Segelmark); Swiss Dialysis Registry (P. Ambühl and R. Winzeler); Dutch Renal Registry [RENINE] (L. Heuveling, S. Vogelaar and M. Hemmelder); Tunisia, Sfax region (F. Jarraya and D. Zalila); Registry of the Nephrology, Dialysis and Transplantation in Turkey [TSNNR] (G. Süleymanlar, N. Seyahi and K. Ateş); Ukrainian Renal Data System [URDS] (M. Kolesnyk, S. Nikolaenko and O. Razvazhaieva); United Kingdom Renal Registry [UKRR] (all the staff of the UK Renal Registry and of the renal units submitting data); Scottish Renal Registry [SRR] (all of the Scottish renal units).
ERA-EDTA REGISTRY COMMITTEE MEMBERS
C. Zoccali, Italy (ERA-EDTA President); Z.A. Massy, France (Chairman); F.J. Caskey, UK; C. Couchoud, France; M. Evans, Sweden; P. Finne, Finland; J.W. Groothoff, The Netherlands; J. Harambat, France; J.G. Heaf, Denmark; F. Jarraya, Tunisia; M. Nordio, Italy; and I. Rychlik, Czech Republic.
ERA-EDTA REGISTRY OFFICE STAFF
K.J. Jager (Managing Director), M. Bonthuis (for the paediatric section), R. Cornet, G. Guggenheim, A. Kramer, M. Noordzij, M. Pippias, V.S. Stel and A.J. Weerstra.
ACKNOWLEDGEMENTS
The ERA-EDTA Registry would like to thank the patients and staff of all the dialysis and transplant units who have contributed data via their national and regional renal registries. In addition, we would like to thank the persons and organizations listed in the paragraph ‘Affiliated registries’ for their contribution to the work of the ERA-EDTA Registry.
FUNDING
The ERA-EDTA Registry is funded by the European Renal Association – European Dialysis and Transplant Association (ERA-EDTA). This article was written by Anneke Kramer et al. on behalf of the ERA-EDTA Registry, which is an official body of the ERA-EDTA. In addition, Dr. Caskey reports funding from the National Health Service during the conduct of the study. Dr. Finne reports personal fees from Baxter, outside the submitted work and Dr. Slon Roblero reports personal fees from NxStage, outside the submitted work.
CONFLICT OF INTEREST STATEMENT
None declared.
APPENDIX A1
Countries or regions providing individual patient data are: Austria, Dutch-speaking Belgium, French-speaking Belgium, Bosnia and Herzegovina, Denmark, Estonia, Finland, France, Greece, Iceland, Norway, Romania, Serbia, the Spanish regions of Andalusia, Aragon, Asturias, Basque country, Cantabria, Castile and León, Castile-La Mancha, Catalonia, Extremadura, Galicia, Community of Madrid, Murcia, Navarre, Valencian region, Sweden, Switzerland, the Netherlands, the UK, England/Northern Ireland/Wales and UK, Scotland.
Countries or regions providing aggregated data are: Albania, Belarus, Bulgaria, Croatia, Cyprus, Czech Republic, Georgia, Israel, Italy, Latvia, Lithuania, Macedonia, Poland, Portugal, Russia, Slovakia, Spain, Tunisia (Sfax region), Turkey, Ukraine.
APPENDIX A2
Miscellaneous primary renal diseases: Nephropathy (interstitial) due to analgesic drugs, nephropathy (interstitial) due to cis-platinum, nephropathy (interstitial) due to cyclosporin A, lead-induced nephropathy (interstitial), drug-induced nephropathy (interstitial) not mentioned above, cystic kidney disease—type unspecified, polycystic kidneys; infantile (recessive), medullary cystic disease; including nephronophtisis, cystic kidney disease—other specified type, hereditary/familial nephropathy—type unspecified, hereditary nephritis with nerve deafness (Alport’s Syndrome), cystinosis, primary oxalosis, Fabry’s disease, hereditary nephropathy—other specified type, renal hypoplasia (congenital)—type unspecified, oligomeganephronic hypoplasia, congenital renal dysplasia with or without urinary tract malformation, syndrome of agenesis of abdominal muscles (prune belly), renal vascular disease due to polyarteritis, Wegener’s granulomatosis, ischaemic renal disease/cholesterol embolism, glomerulonephritis related to liver cirrhosis, cryoglobulinemic glomerulonephritis, myelomatosis/light-chain deposit disease, amyloid, lupus erythematosus, Henoch–Schonlein purpura, Goodpasture’s Syndrome, systemic sclerosis (scleroderma), haemolytic uraemic syndrome (including Moschcowitz Syndrome), multi-system disease—other (not mentioned above), tubular necrosis (irreversible) or cortical necrosis (different from 88), tuberculosis, gout, nephrocalcinosis and hypercalcaemic nephropathy, Balkan nephropathy, kidney tumour, traumatic or surgical loss of kidney, other identified renal disorders.
REFERENCES
- 1.ERA-EDTA Registry. ERA-EDTA Registry Annual Report 2016. Amsterdam: Academic Medical Center, Department of Medical Informatics, 2018 [Google Scholar]
- 2. Kramer A, Pippias M, Stel VS. et al. Renal replacement therapy in Europe: a summary of the 2013 ERA-EDTA Registry Annual Report with a focus on diabetes mellitus. Clin Kidney J 2016; 9: 457–469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pippias M, Kramer A, Noordzij M. et al. The European Renal Association-European Dialysis and Transplant Association Registry Annual Report 2014: a summary. Clin Kidney J 2017; 10: 154–169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kramer A, Pippias M, Noordzij M. et al. The European Renal Association-European Dialysis and Transplant Association Registry Annual Report 2015: a summary. Clin Kidney J 2018; 11: 108–122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eurostat. http://ec.europa.eu/eurostat/data/database (21 February 2017, date last accessed)