

Abstract
Background/Purpose:
Providing powered mobility technology to people with disabilities is a common rehabilitation practice. However, the relationship between powered mobility introduction and identity development, when considered in the context of lived experiences of children with disabilities and their families, is not well understood. Investigating this relationship is timely given the emergence of alternative, community-based early mobility opportunities using adapted mobility toys whose impact may contrast experiences using powered wheelchairs typically provided in rehabilitation settings.
Method:
Using a qualitative, ethnographic case study approach, in-depth interview and field observation data were collected with two children and families, one who received a traditional powered wheelchair and the other who received an adapted mobility toy. A grounded theory approach guided the data analysis, and emerging themes were discussed until consensus was reached between the author and families.
Results:
Findings revealed four themes: 1) Dys/Function of Mobility Technology; 2) Daily Life, Play, and Participation; 3) Emerging Self/Advocacy; and Complex Family/Industry Interplay.
Conclusion:
Similarities and differences were present within the situated experiences of each family. Experiences were foregrounded by instances of emerging identity development throughout provision processes that were influenced by caregiver perceptions of disability (positive vs. negative), aesthetics and function (medical vs. adventure), and perceived intent of the devices (an opportunity for freedom vs. prolonging need for undesired mobility equipment). These findings highlight the varied dynamics and spheres of influence this transaction may have on the developing identity of children with disabilities, which may ultimately help inform future models of provision and rehabilitation practices.
Keywords: children with disabilities, mobility technology, identity, qualitative research, case study
Introduction
Providing powered mobility technology to people with disabilities is a common rehabilitation practice. However, the relationship between powered mobility introduction and identity development, when considered in the context of lived experiences of children with disabilities and their families, is not well understood. Investigating this relationship is timely given the emergence of alternative, community-based early mobility opportunities using adapted mobility toys whose impact may contrast experiences using powered wheelchairs typically provided in rehabilitation settings. To provide context for this study, which examines this impact in two children and families using different mobility devices, it is important to briefly highlight four key areas: the basis for powered mobility provision for children; the re-emergence of toy-based powered mobility opportunities; previous work on identity development in children with disabilities; and gaps in understanding of how these elements may intersect to impact the trajectory of identity development in children with disabilities as powered mobility is introduced.
Powered Mobility Provision for Children
In 2016, over six percent of children in the US were reported to have some type of disability, with just under one percent of children ages 5–17 categorized as having an ambulatory disability (Kraus et al., 2018). However, an accurate picture of young mobility device users is challenging to describe, since ambulatory disability statistics are not routinely collected for children under the age of five (Kraus et al., 2018). Only one older report notes that nearly 100,000 community dwelling children with disabilities under the age of 18 used powered wheelchairs or scooters as their primary means of mobility (Kaye et al., 2000). Nonetheless, scholarship and advocacy surrounding mobility technology has underscored the biopsychosocial importance of mobility intervention, recognizing mobility in any form as a basic human right.
For example, language within the United Nations Convention on the Rights of the Child (CRC), the United Nations Convention on the Rights of Persons with Disabilities (CRPD), and the Assistive Technology Act specifically address children’s rights to personal mobility and participation, which for many children with disabilities is facilitated via mobility technology1 (HR 4278, 2004; Lansdown, 2009; Parette et al., 2005; United Nations, 1989, 2006). These policies ensure a philosophical alignment to the ideal that mobility, and the technology that facilitates it, is a right of citizenship for children with disabilities (Borg et al., 2011). Similarly, developmental research suggests that self-directed mobility, defined as moving oneself by using the body or using a mobility device, leads to a cascade of changes in domains of cognition and communication, psychosocial development, other motor skills, play and exploration, and improved self-efficacy (Anderson et al., 2013; Bottos & Gericke, 2003; Butler et al., 1984; Campos et al., 2000; Casey et al., 2013; Feldner et al., 2016; Livingstone & Paleg, 2014; Paulsson & Christofferson, 1984; Rosen et al., 2009; Uchiyama et al., 2008).
However, recognition of these benefits has not translated to an associated increase in access to or use of powered mobility devices for children with disabilities. (Guerette et al., 2005; Livingstone & Paleg, 2014; Rodby-Bousquet & Hägglund, 2010). The literature has suggested that factors such as the stigma of wheelchairs as a major signifier of disability, social and rehabilitative perceptions of walking as the ideal or most ‘normal’ means of mobility, beliefs that powered mobility will interfere with other motor skills, size and weight of available devices, lack of choice, and lack of environmental accessibility have contributed to this trend (Bickenbach & Cieza, 2011; Daudji et al., 2011; Feldner et al., 2016; Østensjø et al., 2005; Wiart et al., 2004). Historically, provision of powered mobility has been situated within a medical or rehabilitation model, which philosophically views disability as an individual deficit to be remediated, rather than a more contemporary social model, which views disability as a social construct resulting from inaccessible environments, ableist attitudes, and discrimination (Abberley, 1995; Davis, 1995; Linton, 1998; Oliver, 1992). Thus, powered mobility has been traditionally characterized as an individual ‘fix’ or ‘compensation’, rather than a key means of access and participation in social and physical spaces that disable children (Ripat & Woodgate, 2011).
Alternative Models of Powered Mobility Provision
In the 1980’s and 90’s, rehabilitation researchers and clinicians pioneered novel mobility technology solutions in response to the lack of children’s powered mobility options for children with disabilities younger than five years old (Chiulli et al., 1988; Cooper et al., 1992; Jaffe et al., 1986; Wright-Ott, 1999; Zazula & Foulds, 1983). However, some of this work took place outside the US, were ‘one-off’ solutions or did not achieve widespread uptake in the community despite their benefits (Feldner et al., 2016). These innovations set the stage for the Go Baby Go mobility and socialization program, an alternative model of early powered mobility provision that re-emerged in 2010 to fill the same gap in availability of early mobility technology that remains over three decades later. The Go Baby Go program adapts commercially available, battery powered toy ride-on cars that have become ubiquitous in toy stores and are used by young children across the US and beyond. Developed in collaboration with rehabilitation professionals and engineers, adaptations typically include safety and accessibility features like an emergency on/off switch, custom seating supports, and a large, easily depressed switch to facilitate driving access by children with limited mobility (Huang & Galloway, 2012). Adaptations typically occur in community-based settings with volunteers, are completed in a few hours using materials available at hardware stores and have been used with children as young as 12 months of age within environments that are inaccessible to larger and heavier traditional powered mobility devices (Huang & Galloway, 2012; Huang et al., 2014; Ragonesi et al., 2010). Ongoing research is examining the developmental benefits, facilitators, and barriers to use for ride-on cars. Given the apparent contrasts between adapted ride-on cars and traditional powered wheelchairs in aesthetic, provision processes, and intent, a deeper examination of the respective roles of these devices in the developing identities of children with disabilities is important.
Identity Development in Children with Disabilities
Early childhood experiences are pivotal in identity development in all children, highly contextualized by age and culture, and significantly influenced by the presence, beliefs, and reciprocal influence of caregivers (Phillips & Shonkoff, 2000). Less attention, however, has been given to disability as an important contextual or cultural factor in children’s identity development (Davis et al., 2000; Priestley et al., 1999; Watson, 2012). Notably, the literature suggests that children tend to internalize society’s predominantly negative views of disability as their identity develops, thus achieving a positive disability identity is challenging (Connors & Stalker, 2007; Giangreco, 1995; Gill, 1997; Kielhofner, 2005; McMaugh, 2011). Caregivers have also been noted to play a significant role in either promoting or diminishing disability as a part of children’s developing identity (Priestley et al., 1999; Watson, 2012).
Watson (2012) highlights the importance of further examining identity within research frameworks to learn the lives of children with disabilities, citing the need to discover children’s own perspectives and connections between mobility, technology, and quality of life as a fundamental part of rehabilitation and assistive technology research. More work has been done in this area with adults with disabilities, notably Papadimitriou’s (2008) conceptualization of ‘becoming en-wheeled’ in adult spinal cord injury survivors. Papadimitriou notes that a re-embodiment occurs as new users incorporate their wheeled mobility device into their functional body. This becomes a salient piece of ‘en-wheeled’ identity formation, with technology creating a ‘newly abled’ experience for the user in both physical and social interactions (Papadimitriou,2008). Though the work is adult-focused, the concepts may be extended to children and families, with an additional acknowledgment of the key reciprocal influences of both caregiver and child in relation to identity and the assimilation of powered mobility.
Specifically within the context of powered mobility provision for children, noted influences on identity are mixed. Many researchers and caregivers suggest that the introduction of powered mobility has a positive influence on identity, as children with disabilities see themselves as capable, independent individuals who can make their own choices (Everard, 1984; Jaffe et al., 1986; Gibson et al., 2009; Gibson et al., 2012; Paulsson & Christofferson, 1984; Wiart & Darrah, 2002; Wiart et al., 2004). Children may view their devices as not only functional, but social, incorporating them into imaginative play (Holt, 2007; Gudgeon & Kirk, 2015). In some cases, children view their devices as extensions of their bodies; children who have received positive messages about their bodies and disability also communicate a positive self-identity, which includes their device as a central part of that identity (Gibson et al., 2011; Gibson et al., 2012; Wiart & Darrah, 2002). Community-based peer mentor programs have been cited as a means to establish positive disability identity and offer younger children positive older role models, especially in valuing their bodies and mode of mobility (Gibson et al., 2009).
However, depending on the messages children have received about disability and technology, negative or incongruent perceptions of identity may also occur (Huang et al., 2009; Gibson et al., 2011; Gudgeon & Kirk, 2015; McMaugh, 2011). Children understand their bodies as being ‘different’ or ‘not normal’ in having to use mobility devices when other children do not (Huang et al., 2009; Priestly et al., 1999). This points to recognition of difference as well as internalized ableism, where negative social associations and perceptions that have been projected onto the children about their difference become intrinsically acknowledged (Gibson et al., 2012). Children also recognize negative aspects about their technology itself, such as not being able to access certain physical environments, producing stress in navigating large crowds, or unwanted contact with their device and physical aggression resulting in wheelchair damage or threats to safety for the user and others in the user’s vicinity (Gudgeon & Kirk, 2015; McMaugh, 2011).
Knowledge gaps and purpose
Despite the growing body of literature connecting mobility technology and identity development, several gaps in knowledge remain. First, previous literature about the importance of children’s perspectives have been theoretical in nature or conducted retrospectively, well after mobility technology introduction has occurred. Second, methods that involve child wheelchair users as co-researchers to explore psychosocial aspects of powered mobility provision have not been widely undertaken. Third, further understanding of how design and provision of traditional powered wheelchairs and alternative mobility toys may uniquely mediate caregiver and child experiences and acceptance is needed. Fourth, examination of preexisting caregiver perceptions of disability, technology, and their changes across time has been limited; more attention is deserved in exploring how these perceptions are either challenged or reinforced during powered mobility provision. Finally, while some literature has explored the connection between wheeled embodiment and identity in adults, no work specifically addressing the child-caregiver dynamic within this process has been published.
The purpose of this study was to understand the perceptions and experiences of children with disabilities and their families as they engaged in the introduction of different forms of powered mobility technology. The research questions were: What are the similarities and differences in perception and experience of two distinct models of powered mobility provision? How do these perceptions shift over time? What external and internal influences shape these experiences? What role do these experiences have in shaping emerging identities of children with disabilities? Answers to these questions may contribute to improved understanding of powered mobility introduction from the child and family’s point of view and its role in identity development of children with disabilities to ultimately inform clinical best practices in rehabilitation and mobility technology provision.
Methods
This study was conducted as part of a larger, overarching study using qualitative and participatory research methods to describe the experiences of children and families during early powered mobility introduction. An ethnographic case study approach was chosen for its utility in obtaining longitudinal information from participants in natural settings and in everyday life experiences, specifically focused on the culturally-situated use of powered mobility introduction (Ellenbogen, 2003; Gallant, 2008; Merriam, 2009). Researchers across multiple disciplines have utilized an ethnographic case study approach in learning the experiences of their participants, but its application in rehabilitation has been limited (Andrews et al., 2005; Storesund & McMurray, 2009). In-depth data collection processes including semi-structured interviews and field observations were used to become intensively engaged with the participants, evaluate and triangulate their experiences and produce rich descriptions of their introduction to powered mobility technology (Merriam, 2009). All study procedures were approved by the author’s institutional review board. The author adhered to ethical guidelines for human subjects research including the consent and/or parent permission of adults and verbal assent of children. Pseudonyms are used throughout this paper to protect the identity of all participants.
Partcipants
Two children and families and their rehabilitation clinicians in [city removed for blinded review] metropolitan area were recruited to participate in this study. Sampling was targeted to include one child and family about to pursue a powered wheelchair, and another age and diagnosis-matched child and family about to pursue an adapted ride-on car. To be eligible for the study, children were between the ages of 3–7 years; pursuing powered mobility for the first time; and able to communicate proficiently in English. Clinicians, vendors and/or ride-on car build volunteers were actively employed in a seating clinic or engaged as a therapist or other volunteer who assists families in procuring and modifying ride-on cars; willing to assist in the recruitment of a child and family receiving one of the specified powered mobility devices; willing to allow the researcher to be present for field observations during critical events of the provision process; and able to communicate proficiently in English. Potential participants were excluded if they were unable to communicate proficiently in English or had any documented cognitive impairment that would have impacted consent, assent, or communication. Recruitment was discontinued once two age and diagnosis-matched families agreed to participate in the study.
Sam, age 5 at the time of the study, was Caucasian, one of triplets all diagnosed with quadriplegic cerebral palsy, and had an accessible home and transportation. Sam’s primary means of mobility at the time was a manual stroller. He and his family lived in an upper-middle class suburb of [city removed for blinded review]. Sam communicated using verbal language and an eye-gaze computer but chose to participate in all interviews using verbal language. Sam and his siblings attended public preschool and a private conductive education center. Sam’s mom, Teresa, worked as an allied health professional. Sam and his family had recently chosen to pursue a powered wheelchair for the first time through a local seating and mobility clinic at a pediatric rehabilitation facility.
Jamie, age 4 at the time of the study, was the adopted African-American son of Caucasian parents, one of twins both diagnosed with quadriplegic cerebral palsy, and did not have an accessible home or transportation. Jamie’s primary means of mobility was crawling or walking holding on to furniture. He and his family lived in a different upper-middle class suburb of [city removed for blinded review]. Jamie communicated using verbal language. Jamie and his brother attended public preschool. Jamie’s mom, Linda, worked as a nurse. Jamie and his family had recently chosen to pursue a Go Baby Go adapted ride-on car through his school therapists and a group of local engineering and rehab volunteers with adaptation experience.
The six clinicians, vendors, and volunteers that participated in the study with the families had a mean of 27.4 (SD 8.2) years of experience as occupational or physical therapists, durable medical equipment suppliers, and engineers. All were Caucasian and were employed in the [city removed for blinded review] metropolitan region. One occupational therapist and engineer had previous experience adapting cars and served as volunteers to assist in building Jamie’s car.
Role and Background of the researcher
The author, a pediatric physical therapist and disability researcher with experience in seating clinic practices and the Go Baby Go adapted ride-on car program, had no prior relationship to the participating families. Researcher reflexivity was essential, as prior knowledge and experience within both models of powered mobility provision allowed for some recognition of ‘insider’ status by participants, but also could have led to undue influence or bias as well as a power imbalance between researcher and child/family participants (Ulin et al.,2005). To minimize bias, children and families were recruited to participate in the study only after selecting their preferred device, but prior to its implementation. Additionally, the author consciously acted as an ‘observer as participant’ during field observations, where the researcher and the researcher’s activities were known to the participants, however participation was secondary to gathering information for the study (Merriam, 2009).
Study Procedures
This study took place across a 12-month span from February 2015 to February 2016. Clinicians were contacted directly via email flyers, who then assisted in identifying potential child and family participants. Interested families contacted the researcher directly to express interest in study participation. Sustained engagement with the families and their clinicians or build volunteers took place across six months, from September 2015 to February 2016. During field observations, raw field notes were hand recorded according to a researcher-developed field guide, which included details about timeframes, the physical environments (including hand drawn maps of physical spaces), people within each environment, activities and interactions that took place, conversations, symbolic or non-verbal engagement, and the researcher’s own reactions and assumptions about the event and its dynamic (Merriam, 2009). In-depth, semi-structured interviews were conducted using a researcher-developed interview guide for children and families. Sample questions from the interviews are included in Table I. A participatory photo narrative project was also completed by each family for the overarching study (see [citation removed for blinded review] for findings).
TABLE I.
SAMPLE INTERVIEW GUIDE QUESTIONS FOR CHILDREN AND FAMILIES
| Question Type and Audience | Example Question from Interview Guide |
|---|---|
| Experience and Behavior Question, Child | When you go places with your family, what do you like to do? |
| Opinion and Values Question, Caregiver | What is your opinion about the knowledge and roles of professionals in obtaining the (wheelchair/ride-on car)? |
| Feelings Question, Child | When you drove your (wheelchair/ride-on car) for the first time, how did it make you feel? |
| Knowledge Question, Child | Tell me about how you drive your (wheelchair/ride-on car)? |
| Sensory Question, Caregiver | Describe what you saw/heard when your child first used their (wheelchair/ride-on car)? |
| Devil’s Advocate Question, Caregiver | Some people think that powered mobility should happen early, others think it should wait until after a child focuses on standing and walking. What do you think? |
Three sequential events triggered data collection with the families. For Sam, the first event was the initial seating clinic appointment and wheelchair order. Field observations took place at the pediatric rehabilitation clinic, followed by a 120-minute interview at the family’s home approximately one week later. The second event was the wheelchair delivery appointment. Field observations took place at the home delivery, and a 120-minute interview took place approximately two weeks later at the family home. The final event was a three-month follow up field observation in a setting of the family’s choosing, in this case, outside in Sam’s neighborhood. This was immediately followed by the final 120-minute interview, after which the family assisted in co-creating and refining themes for the study.
For Jamie, the first event entailed the ride-on car selection process. Field observations were conducted at the toy store where the ride-on car was purchased, and a 120-minute interview took place approximately two weeks later at the family home. The second event was the ride-on car modification build session, which took place after hours in a conference room at a volunteer’s place of work. Field observations were conducted at the build, and a 120-minute interview took place approximately one week later at the family home. The final event was a two-month follow up field observation at a location of the family’s choosing, in this case, Jamie’s school. This was immediately followed by a final 120-minute interview, after which the family assisted in co-creating and refining themes for the study.
The clinicians, vendors, and volunteers for the powered wheelchair and ride-on car provision participated in the field observations at the first two events for each child and family, for a total of 5–6 hours. Participation time for each child and family was approximately 20 hours. Each child received a $25 gift card incentive at the completion of the study, and the clinicians did not receive compensation.
Data Analysis and Rigor
Data analysis was grounded in participant experience and perceptions, and was ongoing throughout the study, using constant comparison to search for emerging themes and generate hypotheses (Merriam, 2009). All interviews were audio recorded and transcribed verbatim by the researcher and a transcription assistant using Express Scribe transcription software (NCH Software, www.nch.com.au/scribe). Raw field notes taken during field observations were immediately ‘bracketed’ with researcher observations, assumptions, and reflections, then typed into expanded field note transcriptions by the researcher. Coding was emergent from multiple line-by-line hand-coded reviews of the transcripts by the author. Twenty-two open codes were condensed into 14 focused codes, then ultimately grouped into four preliminary themes, or core categories that emerged from the data (Charmaz, 2014). Three broader constructs, or patterns that connected the data to broader psychosocial experiences, were generated with the families.
Triangulation between the interviews and expanded field observation notes was conducted to ensure credibility from multiple sources (Merriam, 2009). Each family engaged in member-checking, reviewing excerpts from transcripts, coding processes, and a concept map of preliminary themes with the author to ensure appropriate interpretation and grouping of themes and allow for discussion and revision (Charmaz, 2014). Review of these materials was also conducted by members of the author’s doctoral advisory committee to ensure data saturation. Discussion easily resolved minor disagreements to achieve full consensus on the final themes and higher order constructs (Charmaz, 2014). To ensure consistency, an audit trail describing detailed data analysis procedures was created (see Figure 1).
Figure 1.
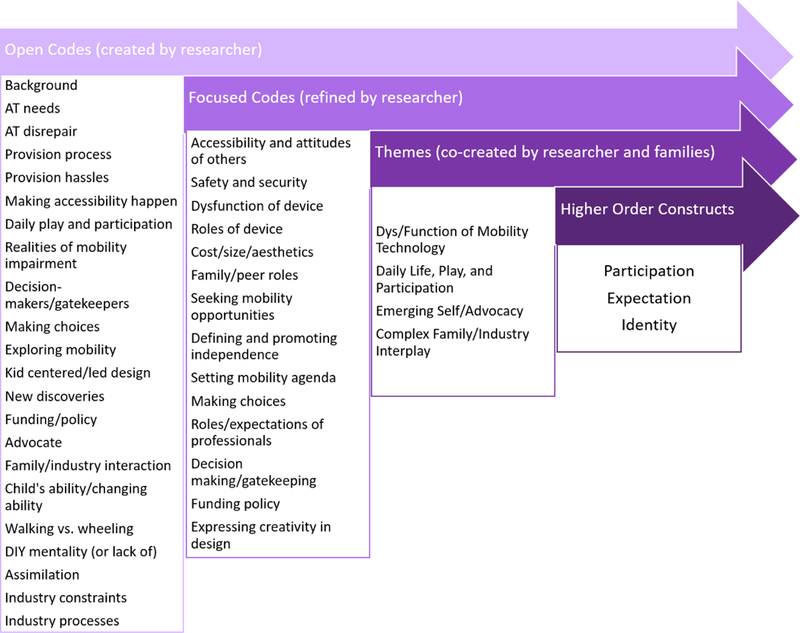
Visual representation of data analysis process.
Findings
Four major themes emerged from the data as findings: 1) Dys/Function of Mobility Technology; 2) Daily Life, Play, and Participation; 3) Emerging Self/Advocacy; and 4) Complex Family/Industry Interplay. These themes served to inform three higher order constructs that connect each family’s data to broader psychosocial experiences of children with disabilities: Participation, Expectation, and Identity.
Theme One: Dys/Function of Mobility Technology
This theme was defined from experiences with device disrepair or provision hassles, perceptions of the practical and abstract functions or roles of the device, concerns about safety and security, and concerns about the size and weight footprint of the device. For example, Teresa and Sam looked especially forward to the powered seating functions that would allow access to countertops or eye level communication. Sam was excited and nervous about this function,
S. squeals and giggles as he slowly rises up to what would be equivalent to the standing height of a small adult. At his highest, S. initially expresses a look of uncertainty…Excitement quickly takes over for S., however. “Now I’m way up high” he says. “I am a GIANT!” (Expanded field notes, November 2015)
The seat elevator function remains a salient feature for Sam and his family throughout all subsequent research visits. Teresa also discusses the function of the powered wheelchair as a means for Sam to control his body and environment. Prior to receiving the wheelchair she notes,
“You know, before we got the chair, his brother did something and ran off and he said, “You wait till I get my chair!” so he is very excited about the independence. It is exciting for him to think about being able to control his body. I can’t wait for him to be able to interact with the kids on the playground…and with his sisters and his brother.it will open up his world. You know? To not have to depend on either another child or an adult to take them from point A to point B.” (Interview one, September 2015)
Conversely, Linda’s perception of the ride-on car function was directly linked with her perception of the dysfunction of a wheelchair. She described her initial reaction upon hearing from her therapists that a wheelchair might be a possibility for Jamie’s mobility in the future,
“So I was at physical therapy with the boys and the physical therapist said something about a wheelchair and I went ‘Why do I need a wheelchair?’ And she looked at me and she said, ‘Well, uh, he’s not going to be a community walker’…It felt like I had been hit in the stomach. It was…a bad conversation. It was very hard to digest.” (Interview one, November 2015)
After being encouraged by her therapists to “Put it in the back of your mind for a while” (Interview one, November 2015), Linda and Jamie’s school physical therapist, Susan, decided to pursue an adapted ride-on car for Jamie to use at school. The ride-on car served a desirable function in prolonging the need for a wheelchair. Revisiting these perceptions after Jamie was successfully driving his car, Linda noted,
“[The car] just encourages me to keep him out of a wheelchair. That’s what it does. It’s a way to make sure that I know that there are other ways out there, and we’ll figure it out…If you can keep a kid out of a wheelchair for years, that’s awesome.” (Interview three, February 2016)
Practically, however, Linda recognized the potential for independence for Jamie in the car,
“He’ll go on grass a little bit more and have some independence and catch up with his brother…he’ll be able to keep up with and it’ll be huge. We really think it’ll be a fun thing for him. We think it’ll make him happy. So there will be less frustration and screaming and there will be more laughing.” (Interview one, November 2015)
Here, Linda also sees function from a more emotional standpoint, potentially with the car potentially mediating a shift in Jamie’s mobility experiences from frustration to fun and happiness. As for Jamie’s own perception of the ride-on car, he has one focus: speed. Field notes from the build session note,
As they pack up to leave, J. comes over to say thank you. I give him a high five and ask him what his favorite part of driving was. He replies without missing a beat, “Going FAST!” (Expanded field notes, January 2016)
Each family’s perspectives within this theme reinforce the view that self-directed mobility is pivotal for everyone and that a powered wheelchair or ride-on car may function as an important means of enacting mobility and self-efficacy, even when traditional wheelchairs may be negatively perceived.
Theme Two: Daily Life, Play, and Participation
The second theme was defined from perceptions of participation with and without mobility technology, daily activity, interaction and attitudes of others, and environmental accessibility. For example, Sam associates his new power chair with the chance to be spontaneously mischievous- participating in life with his siblings in ways that differ from being pushed in a wheelchair by his parents,
H: And how are you going to drive your chair?
S: I don’t know.
T: What are you going to use?
S: My head!
H: Your head? That’s going to be pretty awesome.
S: Yes.
H: Are you going to be able to drive by yourself using your head?
S: Yes.
T: So what happens when your sisters or your brother leave you somewhere- like in the basement?
S: I’m going to chase them!
T: You’re going to chase them! Are you going to run them over?
S: Yes.
T and H: (laughing simultaneously) What???
S: (laughing) Nooooo (Interview one, September 2015).
In later research visits, Sam continued to demonstrate more direct participation with his siblings as well as independent play using his wheelchair, as this field note excerpt indicates,
He beelines over to me, at the other end of the driveway, then turns left and heads down the driveway into the grass. “My wheelchair is dirty, so it’s getting a mudbath!” he tells me. A few minutes later, S.’s sister rides up on her bike and taps the armrest of the wheelchair. “Gotcha” she says, then laughs and turns her bike around, taking off. S. tells us he is going to catch his sister and asks his mom to turn his speed up. “I’m going to get you!” he yells, and starts off down the sidewalk. She rides up, turns her bike to the side, and S. promptly drives forward, gently tapping her bike with his footrests. “Tag- you’re it!” he calls out. (Expanded field notes, February 2016)
While Teresa occasionally helps with chair navigation, she notes how empowering it is for Sam to participate on his own in more naturally paced play. However, Teresa also anticipates the external limitations of Sam’s participation in his powered wheelchair, as a function of inaccessible spaces,
“The other fear that I have is like, is this going to make it harder for him to go on the playground?…When they get into kindergarten, it’s not accessible. The playground is not accessible at all. So…will this just make him more excluded? So, that is one big fear of mine…If you have one curb, that’s it.” (Interview one, September 2015)
Teresa understands that Sam’s successful participation with his powered wheelchair depends on the accessibility of these environments in addition to the attitudes of others. She also discusses the assumptions they’ve encountered about Sam’s abilities related to his wheelchair,
“Everyone seems a little surprised…They look at it and are like “Wow, it’s a big chair!” And then we say, well, it’s a power chair and he can control it, and everyone is like “WOW!” So, because you don’t see a lot of people with head controls, I think that everybody just assumed he wouldn’t be able to control a chair…So I think it’s opening up some people’s perspectives a little bit, which is good.” (Interview two, December 2015)
Even with his ability to control his powered mobility device, Sam is, to some extent, at the mercy of others’ attitudes and dedication to facilitating driving opportunities.
Linda also considers how the ride-on car will affect Jamie’s participation at school, noting,
“Well, for Jamie it allows him not to be in the way at school. He can propel himself around…so when they have library time or when they go to other classrooms or they go outside or go to the gym he can go to and from…He’s still expected to use his walker at school and get up and walk and do all the things he’s supposed to, but it will allow him instead of being…different than his classmates he’ll be different in a different way. He won’t be different needing people, he’ll be different with something cool that people want to have too.” (Interview one, November 2015)
At Jamie’s school the ride-on car is still a novelty, but serves to mediate independent and peer play and participation opportunities for Jamie, as evidenced by this field note excerpt,
J. explores the open field for a while, zigging and zagging back and forth between the grass and the paved pathway. He eventually makes his way back to the playground enclosure. As soon as he is through the gate, two classmates jog next to him as he drives through the woodchips and around the equipment. One child tells him not to get too close to the swings. Another takes a pile of leaves and throws them up in the air as J. drives through them, laughing. This same child asks S. if he can have a turn on the ATV. “I didn’t realize he would be IN the playground with the car and the other kids,” L. comments, smiling. (Expanded field notes, February 2016)
Like Teresa, Linda also acknowledges barriers to Jamie’s participation using the ride-on car,
“It’s huge! It’s too big, too unwieldy in the classroom. It could fit into the main corridor of the classroom, but trying to get around… It’s not a huge classroom…and it’s not a little ATV, it’s a big ATV, so it’s not like you could you quietly maneuver through a small space.” (Interview two, February 2016)
Linda notes that Jamie has two walkers inside his classroom, indicating that she and Jamie’s therapists feel strongly about promoting walking as his primary mode of mobility and participation in class, despite their excitement about the ride-on car outside of the classroom.
Within this theme Sam and Jamie experience mixed attitudes of others during the early stages of driving proficiency. However, both boys recognize a shift in their own participation as mediated by their devices, and both mothers see powered mobility technology as a means to shift others’ perspectives in how they may view each child’s abilities and their readiness to explore their worlds.
Theme Three: Emerging Self/Advocacy
The third theme was defined from instances of independence and interdependence, making choices about mobility, discovering positive role models, and creative mobility design ideas. For example, Teresa recognizes the importance of interdependence for Sam. Interdependence, through understanding his equipment and asking others to help him with what he needs, will be an important facet of teaching Sam to self-advocate,
“Because we talk to him about [his equipment], his level of understanding is there. And that’s why I think he will be so successful. He knows if something’s not on right, he knows if something’s hurting, …one of the first things when he started talking was- the first words I want him to learn are “I need help.” Because, he needs to be able to advocate for himself.” (Interview one, September 2015)
Teresa also feels that having positive disability role models and peers will help teach Sam to advocate for himself and his mobility needs, noting,
“There’s something to be said about learning from same, like peers…To have him be motivated by somebody else who’s using a chair, I think that’s so much more powerful than mom saying, ‘Come on, let’s go’….because I’m not sitting in it.” (Interview two, December 2015)
Part of Teresa’s motivation is to advocate for Sam in setting and achieving his goals, actively counteracting some of the negative self-perceptions that have already entered Sam’s mind,
“He wants to be a weather man right now. But the other day he said he can’t be, because he doesn’t see any other weather people using wheelchairs. .So, I want him to see that adult side of things too. Because you can see other kids…but then, it’s, “But Mommy, I don’t see anybody on TV,” so that must mean that they don’t exist.” (Interview three, February 2016)
Sam’s self-advocacy related to mobility emerges at the delivery appointment and continues to evolve throughout the first months of his wheelchair use. He asks and answers questions about his chair and his body and immediately begins activating switches with his head and learning the display, despite adult expectations of him to wait. After driving for only a few weeks, his pride and agency are evident,
Sam makes a beeline for center court, spins in a few circles before giggling and happily exclaiming, “I’m coming to get you Mommy!” His mom, Teresa, beams as she shows the videotape Sam driving, his head gently pushing on switches in his headrest where he knows his head movements will control where he wants to go. “Why are you coming to me, Sam?” asks Teresa on the recording. “Because I want to be by you,” Sam replies. (Interview two, December 2015)
Linda has similar visions of independence for Jamie, and therapies are an especially salient component of doing everything she can to “make life easier” for Jamie (Interview one, November 2015). Walking, as a major goal of his therapies, holds particular importance for Linda, even after the ride-on car build. As she notes,
L: He got put into [positioning straps] for the first time yesterday. But like 30 minutes in he’s like, ‘Take these things off! ‘ And I’m like, ‘Nope… ‘ ‘Jamie, do you want to walk better? Do you want to walk?’ ‘Yes’. ‘Ok, keep the [positioning straps] on.’ So he, we use the term ‘walking man’. Are you a walking man or are you a crawling man?
J: Walking man
L: Are you a walking man or a crawling man?
J: Walking man
L: So we say that a lot. You are a walking man, you are not a crawling man.
Which means, you gotta move. So, that’s in his vocabulary. Where as other kids, it’s not. And ours, its .it’s there. So we’ll get him there as much as we can. (Interview two, February 2016)
Walking is of such importance to Linda, that Jamie has already incorporated the notion of himself as a ‘walking man’ into his identity. However, she continues to fiercely advocate for multiple modes of mobility for Jamie in addition to walking, including hippotherapy, bicycling, swimming, and the car.
Jamie, like Sam, demonstrates moments of his own emerging agency throughout the provision process and use of his modified ride-on car. He also asks questions and explores the components of his device, as noted in this field note excerpt.
J. drops down to his hands and knees and begins exploring the car. J presses the horn and calls out ‘Beep beep!’ and makes motor sounds. He pushes on the bright green fenders of the ATV, and explores a small silver toggle switch along the back of the bumper…Investigating further, J. is grabbing the wheels with his hands. He is curious about all the moving parts- flipping switches, turning the handlebars, and now rolling the wheels (Expanded field notes, January 2016)
During the car trial at the end of the build session, he tells his therapist, “I want to do it by myself’, and when she turns the safety switch off to stop the car, he turns to look at her, saying, ““Why is it off? Why am I stopped? I want to go.” (Expanded field notes, January 2016). Like Sam, his confidence in making mobility decisions and setting his own agenda grows with practice. At the final research visit, he listens patiently to his therapist tell him instructions about his path to the playground, and when the car is turned on, he immediately veers in the exact opposite direction with a huge smile on his face.
Both Sam and Jamie also exercise their emerging self-advocacy by describing imagined details of mobility devices they would each create. (Features listed in Table II). Both boys’ narratives offer a vivid description of device aesthetics as well as the logistics involved in obtaining and operating it. The ways in which the boys communicate these details exemplify a moment of child-led design that could serve a useful purpose for both mobility toy and wheelchair manufacturers.
TABLE II.
THEMATIC COMPARISON OF CHILDREN’S PERCEPTION AND EXPERIENCE OF MOBILITY TECHNOLOGY PROVISION AND USE
| Overarching Theme | Thematic Instance |
Sam | Jamie |
|---|---|---|---|
|
EMERGING SELF/ADVOCACY |
Child Led Design: | ||
| Looks like | “Mickey Mouse” | “A Motorcycle” | |
| Colors | “Mickey Colors- Red and Black” | “Gray and Black” | |
| Be made of | “Marshmallows, no, a pillow” | “Play-doh, no, metal. All metal” | |
| How it drives | “Mickey’s Hand” | “Stand up, like me” | |
| Cost | “One Dollar” | “Five Dollars” | |
| Where it comes from | “The wheelchair store” | “The grocery store” | |
Instances within this theme highlight the interconnection between elements of device design, parental perception of disability, and a continuum of independence. These devices may mediate, even in a relatively short time, changes in agency that will contribute to ongoing identity development for users.
Theme Four: Complex Family/Industry Interplay
The fourth theme was defined from each family’s experiences with decision-making and consumer choice, knowledge and expectations of the volunteers or providers, funding policies, and costs within each provision model. For example, Sam was unable to trial the powered wheelchair he eventually ordered, because a trial of the head switch drive control was considered more important than a trial of his preferred seating system and wheelchair base at the evaluation. As Teresa points out, Sam was evaluated briefly, by people unfamiliar to him, in an unfamiliar environment. Yet, that evaluation time is standard for the assessment of driving abilities and needs for such costly equipment,
“Because they didn’t have one to show me what it looked like in person, I had to look online…And [we discussed] the supports. I know my son, and as a therapist, I’m like, “OK, he needs the laterals, he needs an abductor.” and they were trying to say, “Well, no.” and I was like, “Right now in this chair, that’s not the chair we are ordering, in this chair he looks fine, but in his chair, you know,” I was like, “I need the foot plates, I need the foot pieces that his feet can actually sit in and strap down.” (Interview one, September 2015)
Teresa also discussed preparing for her appointment but feeling limited by her therapists and vendors, noting how her background as an allied health professional helped mitigate some of the overwhelmed feelings that others might experience,
“I have a large community of friends with kids in push chairs, you know manual chairs, power chairs…so I was asking ideas, looking up online and stuff like that. So, when I came to the appointment, they had never really heard of a couple of the chairs, so they didn’t really have any input .I feel like you’re limited to their knowledge or their biases in that way. I felt like I was involved because I would ask questions and I came prepared, but if I didn’t have my background and knowledge, it would have probably been just left up to whatever was suggested and gone from there.” (Interview one, September 2015)
Teresa’s experiences point to limited consumer options within the medical mobility industry that are situated in contrast to other retail technology markets. It is unlikely that a consumer would be expected to, or be satisfied with, purchasing another type of expensive motor vehicle- like a car-sight unseen.
Teresa and Sam’s experiences were directly impacted by current funding policies and regulatory oversight. The funding approval process resulted in a nearly three-month delay between the evaluation and the delivery of his powered wheelchair, and although their insurance paid for most of the $42,000 cost, some features, like the seat elevator so important to Sam and his family, was an over $4000 out of pocket expense as it was not considered medically necessary. This was frustrating for her as a consumer,
“It’s really hard to contact an insurance company when you don’t know all the codes for each piece. You call them up and say ‘Is the power chair covered?’ ‘Yes!’ and I’m like ‘OK!’ but then they’re like ‘Oh, but not this and not this and not this,’…I’m hoping insurance will pay for [the seat elevator], I guess a lot of times they don’t. And we want the little joystick in the back and they said they probably won’t cover that. Really? For a kid?” (Interview one, September 2015)
Teresa classified her experience with the seating clinic and vendor as a distinct business transaction. Being valued as a consumer was important, which meant being timely with responses and repairs, even though she had the background and skills to attend to these herself,
“I have an engineering undergrad degree, I have friends with tools, so yeah, I do it myself. I am happy that I can, but I would rather not have to. I tried to call the vendor and it took them a week to even get back to me to schedule a time to come and fix it, and I was like, ‘It’s already done’. I don’t have time to wait for that.” (Interview one, September 2015)
Throughout the study, Teresa dealt with ongoing consumer frustrations and a lack of responsiveness and delays in part orders and repairs soon after delivery, noting,
“In December, we found out one of the motors had burned out, we don’t know why. But it took them til the first week of February to get it back to us. When they finally ordered the right motor.” (Interview three, February 2016)
A more rapid response and further education from vendors was perceived to help demonstrate that Sam’s mode of mobility identity as a powered wheelchair user and consumer was valued as well.
Jamie and his family had a distinctly different interaction with the individuals who volunteered to build his ride-on car. For example, Linda was grateful for the knowledge and guidance of her school therapist, Susan, as a key decision-maker in the ride-on car process. Susan assumed a leadership role in orchestrating the build, and Linda credited her for making the ride-on car opportunity happen, noting,
“I told her what I’d seen at the toy store and she said, “That’s the one you’re going to go get.” So I pretty much just got what Susan had measured. So Susan was huge. She measured everything and she made a mock up at school of, like, the width he’d be, so she’d know that he could do it. So she was very, because I don’t, I really don’t know if we would have [done this otherwise].” (Interview one, November 2016)
Somewhat ironically, Jamie also noted Susan’s decision-making role related to his driving, recognizing the adult-imposed parameters of his ride-on car use,
H: So Jamie, can you remind me how you drive your car? What do you have to do?
J: Stop.
H: You have to stop when you drive your car?
J: Yeah.
H: And why do you have to stop?
J: Cause Susan told me to stop. (Interview two, February 2016)
Linda described several benefits and drawbacks of the adapted ride-on car provision process. First, the ride-on car is a toy, not a medical device. While positive in terms of aesthetic and accessibility, because there is no Food and Drug Administration approval codes for toys, they are not considered reimbursable items under insurance plans2. Thus, car costs were out of pocket for Jamie’s family, and considered a significant expense given the relatively short time Jamie could use the car. As Linda stated,
“For the little kids I think they’re reasonable. They’re 50 bucks. This one we got was $260 but it was the only one that fit him. Now because of the [volunteers], we’re not paying for it to be modified. I don’t know if it would be cost prohibitive if we did a modification because I don’t know how much that would cost. And yeah…he’s going to outgrow it but we’ll just donate it to the school.” (Interview one, November 2015)
Despite these cost concerns Linda appreciated the “cool” aesthetic meant to inspire adventure, exploration, and movement, all with an extremely high fun factor that would draw other children in. Jamie chimed in too, saying, “Especially, my ATV is cool. Beep beep!” (Interview two, February 2016).
While having a greater amount of community flexibility and consumer choice in a mainstream, child-centric environment could be viewed as welcome, for Linda, the process of choosing a car was daunting. Both she and Susan went separately to look at the store, but Linda did not take Jamie with her to try out any of the cars. As she explains,
“I can’t take him to a toy store and have him sit on these things because he’s not going to process. I can’t have him dissolving every time he sees something because, ‘Here, now I have to try this [other] one on you’. He doesn’t understand. It’s just devastating. And as mom it’s really hard. I wasn’t going to do it.” (Interview one, November 2015)
Additionally, Linda admits that she would prefer to leave the modifications to others,
My brain just doesn’t work that way. If you’re mechanically inclined with stuff it’s nothing. It’s just PVC pipes and somebody who knows how to do the switching, which I don’t…If you had a buddy who could do the electric and somebody who could do all the PVC then it’s really nothing. It’s just the pieces. It’s just you have to have somebody with that knowledge…which we don’t have.” (Interview one, November 2015)
The community based, decentralized process was also frustrating at times for Linda, who indicated that she would have liked more organization and logistical detail throughout the provision process,
“Just let the person know.a) timing, and b) where do you drop the thing off. It’s just too expensive to just bring it and be like, who am I bringing this to? That’s why when Brian was like, ‘Well, you can call me and arrange to bring it to me,’ and I was like, perfect, now I have my person…instead of giving 12 contacts on the email, cause you don’t know which of the 12 you’re supposed to reach out to…Brian kind of took the lead at the end. I don’t know who was taking the lead in the beginning.” (Interview two, February 2016)
Linda also noted that the build, at four hours total, was too long for the children to be expected to wait, then be expected to drive the ride-on car at the end of the session.
Despite these frustrations, Linda praised the informal community dynamic, education and hands-on experience she and her therapists received from the build volunteers. She perceived the after-hours build as a distinctly personal transaction, continuing to speak to Jamie about the build team and acknowledge their expertise and contribution of time and energy after the build, noting,
“So I just thought they were phenomenal people, and they were so generous with their time. I still haven’t figured out what I’m doing for everybody. I said to Susan, ‘I don’t know what I’m supposed to get you guys for this’, and she’s like ‘Nothing!’ and I’m like, oh no, you guys are all getting something”. (Interview two, February 2016)
Having a toy-based mobility option that could be adapted for Jamie’s specific needs provided a valued option for independence that simultaneously prolonged the need for a wheelchair and promoted a differently conceptualized identity for Jamie in the eyes of his mother. These interactions and industry or organizational factors could indirectly impact identity development through the implicit and explicit messages received during provision processes.
Discussion
The experiences and perceptions offered by Sam, Jamie, and their mothers are nuanced and many times distinct, however four core categories emerged as themes within the above findings. Three higher order constructs, or patterns, connected their data to broader psychosocial experiences of children with disabilities: Participation, Expectation, and Identity. These patterns can be drawn from each theme in unique ways but remain omnipresent as the families navigate their respective experiences (Charmaz, 2014). For example, consider the first two constructs and how they reflect each theme, before a deeper examination of the primary construct of identity. Participation is facilitated or hindered by dys/function of the mobility device (Theme 1), others’ attitudes and perceptions (Theme 2), the confidence of the child in setting a mobility agenda (Theme 3), or the choices and aesthetics offered by the mobility industry for consumers (Theme 4). Similarly, expectation relates to a caregiver’s expectation of the mobility device itself (Theme 1), the child’s expectations in exploring play and participation (Theme 2), a caregiver’s expectations of their child (Theme 3), or caregiver expectations of industry knowledge or support (Theme 4). The collective experiences within the themes, as well as device design and intent, are not neutral and will help shape the identities of Sam and Jamie into the future. The subsequent discussion focuses on the primary construct of identity as mediated by powered mobility introduction across six key areas.
First, Jamie and Sam experience similar new experiences using their respective powered mobility devices, however the underlying assumptions about each device are distinct. Teresa proactively seeks out a powered wheelchair for Sam and discusses the positive roles and function of the chair, which mirrors existing literature suggesting that therapists and other industry professionals recognize the efficacy of early powered mobility experiences for children to foster independence, promote socialization with peers, and augment participation in family and community life (Butler et al., 1984; Casey et al., 2013; Jones et al., 2012; Rosen et al., 2009). Teresa’s professional background as a therapist may have a significant impact on how she values the role of a wheelchair and communicates this directly and indirectly with Sam. Their perceptions contrast findings in the literature that reflect initial caregiver reluctance to pursue powered mobility for reasons including stigma, beliefs that powered mobility will interfere with other motor skills, size and weight of devices, lack of appropriate environmental accessibility, or perceptions of a powered wheelchair as a failure or last resort (Feldner et al., 2016).
For Linda, this negative perception of wheelchairs persists throughout the study, as evidenced by her shared perceptions about mobility and walking. In fact, the ride-on car strengthens her resolve to forestall Jamie’s potential need for a wheelchair as long as possible. In the literature, caregivers have also been shown to highly value walking and mobility aids that support walking, because of their symbolic value in affording their children an upright position regardless of physiological gain (McKeever et al., 2013). Gibson and Teachman (2012) posit that this focus on upright mobility and walking results from a dominant social viewpoint of walking as ‘normal’, which affects both caregiver perceptions as well as children’s self-concept. Indeed, even Jamie’s operation of the car in a standing position is aimed to promote strength and balance that will aid in walking and other upright activities. Linda and her therapists have valorized, and Jamie has already internalized, his role as a ‘walking man’, which may undermine his ability to positively identify as a person with a disability should walking remain as a secondary means of mobility (Giangreco, 1995; Gill, 1997; Kielhofner, 2005). Connors and Stalker (2007) identify the above issues as common ‘barriers of being’ for children with disabilities.
Second, Sam and Jamie demonstrate and verbalize recognition of how their participation changes using their respective devices. This awareness exists at four and five years old, a younger age than has been identified in previous work that has examined children’s own perspectives of their assistive technologies (Huang et al., 2009; Gibson et al., 2012; Gudgeon & Kirk, 2015; Skar, 2002). After receiving their technologies, both boys incorporate them into real and imaginary play. The literature describes the incorporation of assistive devices into the active shaping of play worlds and peer interactions as an important aspect of participation and identity development for children with disabilities (Burke, 2012; Holt 2007; Kramer & Hammel, 2011; Sapey et al., 2005). This includes new conceptualizations of self-initiated risk and exploration of terrain, heights, and driving away when called, which are behaviors reflected in literature that examines the development of self and identity, body awareness, and environmental awareness in young children without disabilities (Sandseter, 2007; 2009). For adults with disabilities, self-selecting exploratory activities that might be deemed by others as ‘risky’ was noted as a meaningful part of how they define themselves and their participation (Hammel et al., 2008). Thus, Sam and Jamie’s self-selected activities now will likely impact their sense of competence and developing identity as they mature (Connors & Stalker, 2007; Gill, 1997; Watson, 2012).
Third, through observations of Sam and Jamie in their community and school, respectively, it is evident how their powered mobility devices change the trajectory of how peers and adults enter their worlds, as well as how their developing agency is projected. Friends who are curious, who want a turn, or who want to help direct play with the boys and their new devices approach both Sam and Jamie. Adults express praise, surprise, and in the case of Jamie, even jealousy, in regard to the devices and their mobility. Both their siblings engage in new and different ways. Many authors corroborate these observations, noting that powered mobility devices mediate a shift in how others approach the device user (Everard, 1984; Jaffe et al., 1986; Paulsson & Christofferson, 1984; Wiart et al., 2004). Paulsson and Christofferson (1984) specifically noted how sibling interaction is more spontaneous and playful when the sibling with a disability was using a powered mobility device. However, within the boys’ peer interactions, it was much less about the device itself and more about the play and participation, whereas with adults, the device itself became the primary subject of interaction. Literature to date has not captured or addressed this key difference, and this shift in focus from peers to adults may have implications on the developing self-concept of the children as powered mobility users if/when attention to technology supersedes attention to self.
Both Sam and Jamie demonstrate a similar trajectory of agency development as a result of powered mobility introduction. Existing literature speaks to the importance of this trajectory in the development of self-concept and identity of children with disabilities, noting that part of self-advocacy skill development involves experiencing agency over one’s body and world in concert with technology (Everard, 1984; Gibson et al., 2011; Gudgeon & Kirk, 2015; Holt, 2007; McMaugh, 2011). Agency is further exercised when Sam and Jamie describe their ideal powered mobility design. Although this method of child-led design is touched on in the literature, it has not, to date, been put into practice in meaningful or consistent ways. As such, scholars have called for an increase in child-led research and powered mobility design opportunities, citing the need for already marginalized voices of disabled children to inform adult driven ideas of what mobility technology should look like, how it should function and be built (Allsop et al., 2010; Allsop et al., 2011; Durkin, 2002; Rigby et al., 1996). Jamie takes the idea of designing his own ride-on car a step further, utilizing his agency in creating sameness, by telling the researcher to stand and ride ‘like him’. Sameness, as Gill (1997) describes, is one key facet of connecting with both disability and mainstream culture. For Jamie, this hints at a more positive self-concept that may be developing because of his engagement with the ride-on car, although this is difficult to discern, as the car also reproduces a socially and developmentally desired position of standing (Gibson & Teachman, 2012; Gill, 1997; McKeever et al., 2013).
Fourth, both families’ narratives demonstrate the ways in which a continuum of independence exists in their family life. As Gibson et al. (2011) argue, this fluidity between dependence, independence, and interdependence is an important, and natural, part of ‘becoming’ for a young person using mobility technology. Teresa’s interpretation of interdependence as building a community, and perhaps more importantly, as building a disability-positive community for Sam, is reflected in Rousso’s (1996) work highlighting the importance of both peer and adult role models and mentors for youth with disabilities. Gill (1997) similarly refers to the importance of establishing a place within a disability community, describing it as ‘coming home’. Tsuda (2006) argues that interdependence is key for self/advocacy as it relies on the notion of building and maintaining relationships in community. Teresa recognizes that as a non-user, her knowledge is situated in a differently embodied experience, and encounters in community, especially with successful wheelchair users, are pivotal to the development of Sam’s self-concept, and a disability-positive identity (Papadimitriou, 2008; Stainback et al., 1994).
Again here, Linda has distinct and at times incongruent ways of advocating for her son’s independence, primarily through intensive rehabilitation and promoting multi-modal mobility (excluding a wheelchair). Both McKeever et al. (2013) and Gibson and Teachman (2012) have noted that a common way for caregivers to conceptualize their advocacy for their children with disabilities is through vigilance with therapies and focused attention on achieving walking. However, many authors also argue that in doing so, caregivers essentially reinforce dominant stigmatized views of disability and mobility other than walking, by intensively engaging in activities that serve to ‘normalize’ both movement and body, which have significant implications on identity development as a person with a disability who may move through the world differently (Giangreco, 1995; Gibson & Teachman, 2012; Gill, 1997; Kielhofner, 2005; McKeever et al., 2013). Sapey et al. (2005) and Oliver (1993) note from a disability studies perspective, that ‘not-walking’, when conceptualized as a natural aspect of diversity and not a deviation, can challenge the ‘ideology of normality’ and help develop a positive identity as a wheeled mobility user. Although Linda does not, at the time of the study, see Jamie’s disability as diversity rather than deviation, she does commit to advocating for his rights to use the ride-on car for access and fun. Longer term use of the ride-on car may shape or even shift the ways in which Linda advocates for Jamie and his mobility opportunities, and thus his identity development, in the future.
Fifth, the findings of this study also suggest that powered mobility and toy industry policies and practices are a direct influence on Sam and Jamie’s provision experiences, and thus may have an indirect influence on their developing identities as users of powered mobility technology. For example, availability of trial equipment has been explored to a lesser extent in the literature; only two studies and one position paper highlight the need for trial devices that may be accessed by families on short-term loan, rather than restricting the trial and subsequent equipment selection to the mobility evaluation alone (Mortenson & Miller, 2008; Nicholson & Bonsall, 2005; Rosen et al., 2009). Improved access to temporary or trial equipment may contribute to initial success and positive self-concept of children learning to drive independently.
Further, knowledge, bias, and power of the provision teams were acknowledged by both mothers, which was a barrier in Teresa’s view and a facilitator in Linda’s. Both perspectives are mirrored in the literature. For example, Long and Perry (2008) report that over half of the nearly 400 pediatric assistive technology clinicians they surveyed indicated that their competence and confidence in addressing the needs of families during the provision process was inadequate, citing gaps in both knowledge and hands-on skill across domains of device-specific expertise, training in assistive technology assessment, and education on funding policy. Mortenson and Miller (2008) note that while both consumers and professionals may bring distinct expertise to the wheelchair provision process, professionals enjoy “privileged positions…as equipment gatekeepers” (p. 173). Characterizations of this power dynamic have also been described by scholars in disability studies who critique the rehabilitation industry for perpetuating the marginalization of people with disabilities by restricting equipment choice, limiting input into decision-making processes, and taking credit for successes while attributing perceived failures to consumers (Abberley, 1995; Beaumont-White & Ham, 1997; Mortenson & Miller, 2008).
However, for Linda, the individuals involved in the build were an asset, in that some of the clinicians knew Jamie very well, and the build volunteers had needed expertise in the technical modification processes for the ride-on car. These perceptions coincide with assertions that professionals within pediatric rehabilitation are optimally positioned to provide technology recommendations because of their close regular contact with families (Carey & Long, 2012; Long & Perry, 2008). Her perspective also affirms Mortenson and Miller’s (2008) conceptualization of professional privilege, although in this case, in a way that Linda perceived as desirable and helpful in facilitating the provision of the ride-on car.
Finally, cost and choice were both important sources of tension for the families. Several authors address this tension within the industry between business interests and the altruistic aims to enable full participation in society for people with disabilities (Borisoff, 2010; Bühler & Barbera, 2011; Stack et al., 2009). Additionally, while authors have cited the aesthetics of a toy- based mobility device like the ride-on cars as a potential sea change for device acceptance, there remains a significant gap in the availability of universally designed toys to improve access for children of many abilities (Feldner et al., 2016; Hsieh, 2008; Lane & Mistrett, 2002). Thus, the ride-on cars are adapted after-market and are not eligible for reimbursement by third party payers, making availability even more limited by the need for technical expertise, comfort completing modification procedures, and financial resources (Hsieh, 2008; Lane & Mistrett, 2002). Additionally, the ride-on car program is a grassroots endeavor, therefore lack of commercialization and reliance on volunteers and private funding remains a potential concern for program sustainability (Feldner et al., 2016). While indirect, these industry-related factors send messages to children with disabilities and their families about the priorities of their needs and the value of their mobility and may contribute to internalized ableism and poor self-concept during identity development in childhood.
These findings and key areas of connection have several practice and policy implications for rehabilitation. These include a need to: Re-examine mobility hierarchies and consider alternative or multiple modes of mobility as equally valued means for a child to access his world; engage in more specific education and training in professional rehabilitation curricula, especially surrounding mobility technology provision and alternative ways of thinking about disability; promote an evolution of therapeutic practice out of the clinic to facilitate exploration of mobility in real world spaces with peers with and without disabilities; and lobby to change inefficient and outdated funding or justification policies for medical and non-medical mobility equipment alike.
Limitations and Future Directions
There are limitations to this study. First, the presence of a researcher in qualitatively capturing the lived experiences of children and families may be disruptive or cause an undue influence on the responses of the participants toward acquiescence or social desirability bias. Focusing on ‘point-of view’ questions and maintaining a demeanor of unconditional positive regard helped mitigate this limitation (Merriam, 2009). Despite engagement with each of the families across several months, the length of time spent, relative to the amount of time each child was able to use their new powered mobility device, was still rather limited and is only a representation of their very early use of the devices. Further, while the intent of this study was to characterize perceptions of families, most of the time spent with Sam, and all of the time spent with Jamie, was carried out in conjunction with only their mothers. Interpretations and findings may have differed or been strengthened by obtaining the co-parent’s perspective, both fathers in this case, to a greater extent. Third, the results of this qualitative study reflect the unique experiences and perceptions of the participants and may not be generalizable to other children or families, especially given the relatively homogenous participant sample, as more diverse participants with different disabilities or those with reduced access to rehabilitation resources were not included in this study. Future research work will focus on engagement with larger samples and more diverse participants and development of novel theoretical constructs from the data to further ground the experiences of children and families as they navigate the introduction of powered mobility.
Conclusion
The findings from this study highlight the complexity of powered mobility technology transactions, the similarities and differences in traditional powered wheelchair provision and alternative adapted ride-on toy car models, and the significant impacts that these processes may have on the developing identity of children with disabilities. Further, the findings from this study may inform adjustments in rehabilitation service delivery to include an explicit commitment to a paradigm of ‘right mode, right time’ decision-making, in which all modes of mobility are considered equally valuable, dependent on environmental contexts and needs of the child (Palisano et al., 2009). This includes further exploration of alternative mobility technologies like ride-on cars, given the perceived importance of aesthetics. Moreover, ensuring that the child himself, as well as the caregiver, is at the center of these modal decision-making processes, at the earliest possible opportunity, increases the likelihood that the child’s trajectory of identity development will be a positive one.
Impact:
This research highlights novel perspectives and experiences of very young children with disabilities and their families participating in early powered mobility provision, which offers a methodological framework for future work capturing young children’s voices along with caregiver perceptions by proxy.
This study applies a grounded theory framework and qualitative methodology to a rehabilitative process that has been skewed toward quantitative investigation of functional performance assessment and outcomes.
By foregrounding the situated knowledge of disability, mobility, and technology experienced by children and families as a central discourse during powered mobility provision processes, this study contributes to advocacy for children who use mobility technology, by questioning how current and future design and provision can improve to positively impact their developing identities.
This study helps to challenge traditional and often subconscious mobility hierarchies and advocate for the need for further education for rehabilitation professionals in areas of mobility technology provision and alternative models of disability.
This work contributes to strengthening the call among rehabilitation professionals and families to advocate for policy change regarding funding and equipment justification, to allow for a broader conceptualization of early powered mobility for children, and more successful engagement with underserved populations.
Acknowledgements
The author would like to thank Sam, Jamie, their families, and all the clinicians and volunteers involved in making this study a reality. Special thanks to Sam, Jamie, Teresa, and Linda for allowing the researcher into their lives and for helping to co-create the product of this research. Many thanks to [name redacted for blinded review] for transcription assistance, and to the author’s dissertation committee for their assistance in navigating the themes that emerged from Sam and Jamie’ story. The crafting of this work has been supported in part by the National Institutes of Health, National Centers for Advancing Translational Sciences, KL2 TR002317.
Funding source: The preparation of this manuscript was supported by the National Institutes of Health, National Center for Advancing Translational Health Sciences, KL2 TR002317.
Footnotes
The United States, although a signatory of both the UN and the UN CRPD, has not ratified either convention.
Ride-on cars are toys, so in the US, instead of the Food and Drug Administration, they are subject to safety testing and continual oversight by the Consumer Product Safety Commission (www.cpsc.gov/).
References
- Abberley P (1995). Disabling ideology in health and welfare - the case of occupational therapy. Disability & Society, 10(2), 221–232. [Google Scholar]
- Allsop MJ, Holt RJ, Levesley MC, & Bhakta B (2010). The engagement of children with disabilities in health-related technology design processes: Identifying methodology. Disability and Rehabilitation: Assistive Technology, 5(1), 1. [DOI] [PubMed] [Google Scholar]
- Allsop M, Gallagher J, Holt R, Bhakta B, & Wilkie R (2011). Involving children in the development of assistive technology devices. Disability and rehabilitation: Assistive Technology, 6(2), 148–156. [DOI] [PubMed] [Google Scholar]
- Anderson DI, Campos JJ, Witherington DC, Dahl A, Rivera M, He M, . . . Barbu-Roth M. (2013). The role of locomotion in psychological development. Frontiers in Psychology, 4, 440, 1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews GJ, Sudwell MI, & Sparkes AC (2005). Towards a geography of fitness: an ethnographic case study of the gym in British bodybuilding culture. Social Science & Medicine, 60(4), 877–891. [DOI] [PubMed] [Google Scholar]
- Beaumont-White S, & Ham RO (1997). Powered wheelchairs: Are we enabling or disabling? Prosthetics and Orthotics International, 21(1), 62. [DOI] [PubMed] [Google Scholar]
- Berry ET, McLaurin SE, & Sparling JW (1996). Parent/Caregiver perspectives on the use of powered wheelchairs. Pediatric Physical Therapy, 8(4), 146–150. [Google Scholar]
- Bickenbach J, & Cieza A (2011). The prospects for universal disability law and social policy. Journal of Accessibility and Design for all, 1(1), 23–37. [Google Scholar]
- Borg J, Larsson S, Ostergren P (2011). The right to assistive technology: For whom, for what, and by whom? Disability & Society, 26(2), 151–167. [Google Scholar]
- Borisoff J (2010) Small markets in assistive technology: Obstacles and opportunities In Oishi M, Mitchell IM, & Van der Loos H (Eds) Design and Use of Assistive Technology, (pp. 105–113). Berlin: Springer. [Google Scholar]
- Bottos M, Gericke C (2003). Ambulatory capacity in cerebral palsy: prognostic criteria and consequences for intervention. Developmental Medicine & Child Neurology, 45(11), 786–790. [DOI] [PubMed] [Google Scholar]
- Bühler C, & Barbera R (2011). Assistive technology industry: A field for cooperation and networking. Technology and Disability,23(3), 115–130. [Google Scholar]
- Burke J (2012). “Some kids climb up; some kids climb down”: Culturally constructed play-worlds of children with impairments. Disability & Society, 27(7), 965–981. [Google Scholar]
- Butler C, Okamoto GA, & McKay TM (1984) Motorized wheelchair driving by disabled children. Archives of Physical Medicine and Rehabilitation, 65, 95–97. [PubMed] [Google Scholar]
- Campos JJ, Anderson DI, Barbu-Roth MA, Hubbard EM, Hertenstein MJ, & Witherington D (2000). Travel broadens the mind. Infancy, 1(2), 149–219. [DOI] [PubMed] [Google Scholar]
- Carey H, & Long T (2012). The pediatric physical therapist’s role in promoting and measuring participation in children with disabilities. Pediatric Physical Therapy, 24, 163–170. [DOI] [PubMed] [Google Scholar]
- Casey J, Paleg G, & Livingstone R (2013). Facilitating child participation through power mobility. The British Journal of Occupational Therapy, 76(3), 158–160. [Google Scholar]
- Charmaz K (2014). Constructing grounded theory. London: Sage. [Google Scholar]
- Chiulli C, Corradi-Scalise D, & Donatelli-Schultheiss L (1988). Powered mobility vehicles as aids in independent locomotion for young children: Suggestions from the field. Physical Therapy, 68(6), 997. [DOI] [PubMed] [Google Scholar]
- Connors C, & Stalker K (2007). Children’s experiences of disability: Pointers to a social model of childhood disability. Disability & Society, 22(1), 19–33. [Google Scholar]
- Cooper RJ, Gottlieb P, & Koeff BJ (1992) A new low-cost approach to early powered mobility-the CooperCar. Paper presented at the Computing Applications to Assist Persons with Disabilities . Proceedings of the Johns Hopkins National Search for Computing Applications to Assist Persons With Disabilities, February 1–5, 1992, Laurel, MD. [Google Scholar]
- Daudji A, Eby S, Foo T, Ladak F, Sinclair C, Landry MD, … & Gibson BE. (2011). Perceptions of disability among south Asian immigrant mothers of children with disabilities in Canada: implications for rehabilitation service delivery. Disability and rehabilitation, 33(6), 511–521. [DOI] [PubMed] [Google Scholar]
- Davis LJ (1995). Enforcing normalcy: Disability, deafness, and the body. New York, NY: Verso. [Google Scholar]
- Davis J, Watson N, Cunningham-Burley S (2000) Learning the lives of disabled children: Developing a reflexive approach In Christensen P & James A (Eds.), Research with children: Perspectives and practices (pp. 201–224). New York, NY: Falmer Press. [Google Scholar]
- Durkin J (2002). The need for the development of a child led assessment tool for powered mobility users. Technology and Disability, 14(4), 163–171. [Google Scholar]
- Ellenbogen KM (2003). Museums in family life: An ethnographic case study In: Learning conversations in museums, Leinhardt G, Crowley K., & Knutson K. (Eds.). Taylor & Francis; 81–101. [Google Scholar]
- Everard L (1984) The wheelchair toddler. Heath Visitor, 57(8), 241–242. [PubMed] [Google Scholar]
- Feldner HA, Logan SW, & Galloway JC (2018). Mobility in pictures: a participatory photovoice narrative study exploring powered mobility provision for children and families. Disability and Rehabilitation: Assistive Technology, 1–11. [DOI] [PubMed] [Google Scholar]
- Feldner HA, Logan SW, & Galloway JC (2016). Why the time is right for a radical paradigm shift in early powered mobility: the role of powered mobility technology devices, policy and stakeholders. Disability and Rehabilitation: Assistive Technology, 11(2), 89–102. [DOI] [PubMed] [Google Scholar]
- Furumasu J, Guerette P, & Tefft D (2004). Relevance of the pediatric powered wheelchair screening test for children with cerebral palsy. Developmental Medicine and Child Neurology, 46(7), 468–474. [DOI] [PubMed] [Google Scholar]
- Gallant M (2008). Using an ethnographic case study approach to identify socio-cultural discourse. Education, Business and Society: Contemporary Middle Eastern Issues, 1(4), 244–254. [Google Scholar]
- Giangreco M (1995). “The stairs don’t go anywhere! “ A self-advocate’s reflections on specialized services and their impact physical disabilities. Retrieved February 27, 2016, from http://www.dsamn.org/wp-content/uploads/2014/11/Stairs-to-nowhere-Readings-for-Jigsaw.pdf
- Gibson B, Darrah J, Cameron D, Hashemi G, Kingsnorth S, Lepage C, . . . Menna-Dack D. (2009). Revisiting therapy assumptions in children’s rehabilitation: Clinical and research implications. Disability and Rehabilitation, 31(17), 1446–53. [DOI] [PubMed] [Google Scholar]
- Gibson BE, Carnevale FA, & King G. (2012). “This is my way”: Reimagining disability, in/dependence and interconnectedness of persons and assistive technologies. Disability and Rehabilitation, 34(22), 1894–9. [DOI] [PubMed] [Google Scholar]
- Gibson BE, & Teachman G (2012). Critical approaches in physical therapy research: Investigating the symbolic value of walking. Physiotherapy Theory & Practice, 28(6), 474–484. [DOI] [PubMed] [Google Scholar]
- Gibson BE, Teachman G, Wright V, Fehlings D, Young NL, & McKeever P (2011). Children’s and parents’ beliefs regarding the value of walking: Rehabilitation implications for children with cerebral palsy. Child: Care, Health and Development, 38(1), 61–9. [DOI] [PubMed] [Google Scholar]
- Gill C (1997). Four types of integration in disability identity development. Journal of Vocational Rehabilitation, 9, 36–46 [Google Scholar]
- Gudgeon S, & Kirk S (2015). Living with a powered wheelchair: exploring children’s and young people’s experiences. Disability and Rehabilitation: Assistive Technology, 10(2), 118–125. [DOI] [PubMed] [Google Scholar]
- Guerette P, Tefft D, & Furumasu J (2005). Pediatric powered wheelchairs: results of a national survey of providers. Assistive Technology, 17(2), 144–158. [DOI] [PubMed] [Google Scholar]
- H.R. 4278−−108th Congress: Assistive Technology Act of 2004. (2004). In www.GovTrack.us. Retrieved September 19, 2014, from https://www.govtrack.us/congress/bills/108/hr4278
- Hammel J, Magasi S, Heinemann A, Whiteneck G, Bogner J, & Rodriguez E (2008). What does participation mean? an insider perspective from people with disabilities. Disability & Rehabilitation, 30(19), 1445–1460. [DOI] [PubMed] [Google Scholar]
- Holt L (2007). Children’s sociospatial (re)production of disability within primary school playgrounds. Environment and Planning D: Society and Space, 25(5), 783–802. [Google Scholar]
- Huang H, & Galloway JC (2012). Modified ride-on toy cars for early power mobility: A technical report. Pediatric Physical Therapy, 24(2), 149–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang HH, Ragonesi C, Stoner T, Peffley T, & Galloway JC (2014) Modified toy cars for mobility and socialization: A case report of a child with cerebral palsy. Pediatric Physical Therapy. [DOI] [PubMed] [Google Scholar]
- Huang I, Sugden D, & Beveridge S (2009). Children’s perceptions of their use of assistive devices in home and school settings. Disability and Rehabilitation: Assistive Technology, 4(2), 95–105. [DOI] [PubMed] [Google Scholar]
- Hsieh H (2008). Effects of ordinary and adaptive toys on pre-school children with developmental disabilities. Research in Developmental Disabilities, 29(5), 459–466. [DOI] [PubMed] [Google Scholar]
- Jaffe KM, Butler C, Hayes RM, & Everard DHS (1986). An innovative motorized wheelchair for young disabled children. Journal of Associated Prosthetic and Orthotic Clinics, 21, 46–51. [Google Scholar]
- Jones MA, McEwen IR, & Neas BR (2012). Effects of power wheelchairs on the development and function of young children with severe motor impairments. Pediatric Physical Therapy, 24(2), 131–140. [DOI] [PubMed] [Google Scholar]
- Kaye HS, Kang T and LaPlante MP (2000). Mobility Device Use in the United States Disability Statistics Report, (14). Washington, D.C: U.S. Department of Education, National Institute on Disability and Rehabilitation Research. [Google Scholar]
- Kielhofner G (2005). Rethinking disability and what to do about it: Disability studies and its implications for occupational therapy. American Journal of Occupational Therapy, 59(5), 487–496. [DOI] [PubMed] [Google Scholar]
- Kramer JM, & Hammel J (2011). “I do lots of things”: Children with cerebral palsy’s competence for everyday activities. International Journal of Disability, Development and Education, 58(2), 121–136. [Google Scholar]
- Kraus L, Lauer E, Coleman R, and Houtenville A (2018). 2017 Disability Statistics Annual Report. Durham, NH: University of New Hampshire. [Google Scholar]
- Lane SJ, & Mistrett S (2002). Let’s play: Assistive technology interventions for play. Young Exceptional Children, 5(2), 19–27. [Google Scholar]
- Lansdown G (2009) See Me Hear Me, a Guide to the CRPD for Children with Disabilities. Save the Children; London, UK. [Google Scholar]
- Linton S (1998). Disability studies/not disability studies. Disability & Society, 13(4), 525–540. [Google Scholar]
- Livingstone R (2010). A critical review of powered mobility assessment and training for children. Disability and Rehabilitation: Assistive Technology, 5(6), 392–400. [DOI] [PubMed] [Google Scholar]
- Livingstone R, & Paleg G (2014). Practice considerations for the introduction and use of power mobility for children. Developmental Medicine & Child Neurology, 56(3), 210–221. [DOI] [PubMed] [Google Scholar]
- Logan SW, Huang H, Stahlin K, & Galloway JC (2014). Modified ride-on car for mobility and socialization: Single-case study of an infant with down syndrome. Pediatric Physical Therapy, 26(4), 418. [DOI] [PubMed] [Google Scholar]
- Logan SW, Feldner HA, Galloway JC, & Huang HH (2016). Modified ride-on car Use by children with complex medical needs. Pediatric Physical Therapy, 28(1), 100–107. [DOI] [PubMed] [Google Scholar]
- Long TM, & Perry DF (2008). Pediatric physical therapists’ perceptions of their training in assistive technology. Physical Therapy, 88(5), 629–639. [DOI] [PubMed] [Google Scholar]
- McKeever P, Rossen BE, Scott H, Robinson-Vincent K, & Wright V (2013). The significance of uprightness: parents’ reflections on children’s responses to a hands-free walker for children. Disability & Society, 28(3), 380–392. [Google Scholar]
- McMaugh A (2011). En/countering disablement in school life in Australia: children talk about peer relations and living with illness and disability. Disability & Society, 26(7), 853–866. [Google Scholar]
- Merriam SB (2009). Qualitative research: A guide to design and implementation. San Francisco: Jossey-Bass. [Google Scholar]
- Mortenson WB, & Miller WC (2008). The wheelchair procurement process: Perspectives of clients and prescribers. Canadian Journal of Occupational Therapy. Revue Canadienne d’Ergotherapie, 75(3), 167–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicholson J, & Bonsall M. (2005). Powered mobility for children under five years of age in England. The British Journal of Occupational Therapy, 65(6), 291–293. [Google Scholar]
- Oliver M (1992). Changing the social relations of research production? Disability, Handicap & Society, 7(2), 101–114. [Google Scholar]
- Oliver M (1993). What’s so wonderful about walking? Inaugural lecture, London, University of Greenwich. [Google Scholar]
- Østensjø S, Carlberg EB, & Vøllestad NK. (2005). The use and impact of assistive devices and other environmental modifications on everyday activities and care in young children with cerebral palsy. Disability and Rehabilitation, 27(14), 849–861. [DOI] [PubMed] [Google Scholar]
- Palisano RJ, Shimmell LJ, Stewart D, Lawless JJ, Rosenbaum P, & Russell DJ (2009). Mobility experiences of adolescents with cerebral palsy. Physical & Occupational Therapy in Pediatrics, 29(2), 135–155. [DOI] [PubMed] [Google Scholar]
- Papadimitriou C (2008). Becoming en-wheeled: The situated accomplishment of re-embodiment as a wheelchair user after spinal cord injury. Disability & Society,23(7), 691–704. [Google Scholar]
- Parette P, Peterson-Karlan GR, & Wojcik BW (2005). The State of Assistive Technology Services Nationally and Implications for Future Development. Assistive Technology Outcomes and Benefits, 2(1), 13–24. [Google Scholar]
- Paulsson K, Christofferson M. (1984) Psychosocial aspects of technical aids - how does independent mobility affect the psychosocial and intellectual development of children with physical disability? In: Proceedings of the 2nd International Conference on Rehabilitation Engineering, Ottawa, Canada. Washington, DC: RESNA Press; p 282–6. [Google Scholar]
- Phillips DA, & Shonkoff JP (2000). From neurons to neighborhoods: The science of early childhood development: National Academies Press. [PubMed] [Google Scholar]
- Priestley M, Corker M, & Watson N (1999). Unfinished business: disabled children and disability identity. Disability Studies Quarterly, 19(2), 87–98. [Google Scholar]
- Ragonesi CB, Chen X, Agrawal S, & Galloway JC (2010). Power mobility and socialization in preschool: A case study of a child with cerebral palsy. Pediatric Physical Therapy, 22(3), 322–329. [DOI] [PubMed] [Google Scholar]
- Rigby P, Ryan S, From W, Walczak E, & Jutai J (1996). A client-centered approach to developing assistive technology for children. Occupational Therapy International. 3(1), 67–79. [Google Scholar]
- Ripat J, & Woodgate R (2011) Locating Assistive Technology within an emancipatory disability research framework. Technology and Disability, 23: 87–92. [Google Scholar]
- Rodby-Bousquet E, & Hagglund G (2010). Use of manual and powered wheelchair in children with cerebral palsy: A cross-sectional study. BMC Pediatrics, 10(59). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen L, Arva J, Furumasu J, Harris M, Lange ML, McCarthy E, … & Sabet A. (2009). RESNA position on the application of power wheelchairs for pediatric users. Assistive Technology, 21(4), 218–226. [DOI] [PubMed] [Google Scholar]
- Rousso H (1996). A positive sense of self for girls with disabilities. New Moon Network [Google Scholar]
- Sandseter EBH (2007). Risky play among four-and five-year-old children in preschool. Vision into practice: Making quality a reality in the lives of young children, 248–256. [Google Scholar]
- Sandseter EBH (2009). Affordances for risky play in preschool: The importance of features in the play environment. Early Childhood Education Journal, 36(5), 439–446. [Google Scholar]
- Sapey B, Stewart J, & Donaldson G (2005). Increases in wheelchair use and perceptions of disablement. Disability & Society, 20(5), 489–505. [Google Scholar]
- Skar L (2002). Disabled children’s perceptions of technical aids, assistance and peers in play situations. Scandinavian Journal of Caring Sciences, 16(1), 27–33. [DOI] [PubMed] [Google Scholar]
- Stainback S, Stainback W, East K, & Sapon-Shevin M (1994). A commentary on inclusion and the development of a positive self-identity by people with disabilities. Exceptional Children, 60(6),486. [Google Scholar]
- Storesund A, & McMurray A (2009). Quality of practice in an intensive care unit (ICU): a mini-ethnographic case study. Intensive and Critical Care Nursing, 25(3), 120–127. [DOI] [PubMed] [Google Scholar]
- Teachman G, & Gibson BE (2013). Children and youth with disabilities: Innovative methods for single qualitative interviews. Qualitative Health Research, 23, 264–274. [DOI] [PubMed] [Google Scholar]
- Thomas C (1999). Female Forms: Experiencing and Understanding Disability. McGraw-Hill Education; (UK: ). [Google Scholar]
- Tsuda E (2006). Japanese culture and the philosophy of self-advocacy: The importance of interdependence in community living. British Journal of Learning Disabilities, 34(3), 151–156. [Google Scholar]
- Uchiyama I, Anderson DI, Campos JJ, Witherington D, Frankel CB, Lejeune L, & Barbu-Roth M (2008). Locomotor experience affects self and emotion. Developmental Psychology, 44(5), 1225–1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ulin PR, Robinson ET, & Tolley EE (2005). Qualitative methods in public health: A field guide for applied research. San Francisco, CA: Jossey-Bass. [Google Scholar]
- United Nations. (1989). United Nations Convention on the Rights of the Child (UNCRC), Geneva: United Nations. [Google Scholar]
- United Nations. (2006). United Nations Convention on the Rights of Persons with Disabilities (UNCRPD), Geneva: United Nations. [Google Scholar]
- Watson N (2012). Theorising the lives of disabled children: How can disability theory help? Children & Society, 26(3), 192–202. [Google Scholar]
- Wiart L, & Darrah J (2002). Changing philosophical perspectives on the management of children with physical disabilities—their effect on the use of powered mobility. Disability & Rehabilitation, 24(9), 492–498. [DOI] [PubMed] [Google Scholar]
- Wiart L, Darrah J, Hollis V, Cook A, & May L (2004). Mothers’ perceptions of their children’s use of powered mobility. Physical and Occupational Therapy in Pediatrics, 24(4), 3–21. [DOI] [PubMed] [Google Scholar]
- Wright-Ott C (1999). The GOBOT: A transitional powered mobility aid for young children with physical disabilities. In International Conference on Rehabilitation Robotics, Stanford, CA, USA. [Google Scholar]
- Zazula JL, & Foulds RA (1983). Moblity device for a child with phocomelia. Archives of Physical Medicine and Rehabilitation, 64, 137–139. [PubMed] [Google Scholar]