

To the Editor: We report the case of a 32‐year‐old Caucasian female patient with fistulizing Crohn's disease complicated by diversion colitis.
Due to therapy‐refractory perianal fistulae, diverting sigmoidostomy had been performed in early 2016. Initially, the patient reported good general condition under vedolizumab therapy, although the fistulae persisted. In late 2016, she noticed looser stools, progressive lower abdominal pain, and passage of mucus and blood via the anus.
Suspecting a manifestation of Crohn's disease, treatment was switched to ustekinumab and, due to non‐response, intermittent topical hydrocortisone application was needed. Subsequently, combination therapy with infliximab and 6‐mercaptopurin was initiated. Again, there were no signs of therapeutic efficacy as clinical disease activity persisted.
Endoscopically, mucosal inflammation was evident in the distal ostomy branch (Fig. 1a), while the proximal branch was unaffected. Histological evaluation revealed edematous mucosa with lymphoplasmocytic lamina propria infiltration and hyperplasia of local lymphatic tissue (Fig. 1b). Together, these findings indicated the presence of diversion colitis [1].
Fig. 1.
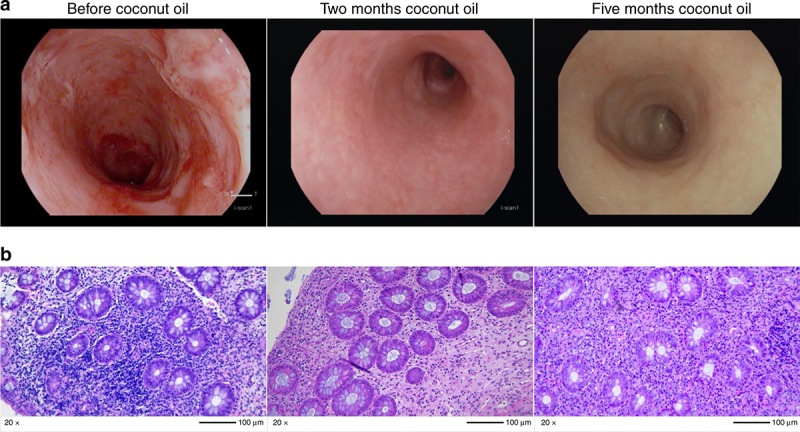
Endoscopic and histopathological findings of diversion colitis. a Representative endoscopic images of the rectum prior (left) and after two (middle) and five (right) months of local coconut oil therapy. Before therapy, spontaneous bleeding, erosions, and fibrin indicated moderate mucosal inflammation. Follow‐up endoscopies under treatment with coconut oil demonstrated only low‐grade inflammation indicated by reduced vasculature and diffuse erythema. b Representative H/E‐stained microscopic images from the histopathological evaluation of sigmoid colon biopsies from the same areas obtained prior (left), after two (right) and five (right) months of therapy with topical coconut oil. Before therapy, acute and chronic inflammation with lymphoplasmocytic aggregates, focal crypt abscesses, superficial defects, and crypt architectural abnormalities (modified Riley score: 10) indicated moderate inflammation. After 2 months of therapy, only mild signs of acute and chronic inflammation with reduced lymphoplasmocytic aggregates, focal crypt abscesses, and superficial defects (modified Riley score: 5) remained and demonstrated low‐grade inflammation. This was maintained after 5 months (modified Riley score: 6)
Reversal of sigmoidostomy was not a therapeutic option due to the persisting fistulae. Local therapy with 5‐ASA and glucocorticoids had been ineffective. Intended local therapy with short‐chain fatty acid (SCFA) enemas [2, 3] was not possible, as—to our knowledge—no pharmacological formulation of SCFAs is available [2] and we did not find any compounding pharmacy.
Therefore, and in view of the deteriorating condition of the patient, proctectomy was recommended, which was refused by the patient, who instead asked for an alternative conservative therapy. Thus, in agreement with the patient, daily local administration of 100 mL prewarmed coconut oil as a rectal enema was initiated.
This was based on the rationale that coconut oil contains fatty acids with comparatively short chain length [4]. Although these are not identical with the SCFAs established in diversion colitis therapy, they are commensally produced and reduced in the inflamed mucosa [5] suggesting a positive impact on epithelial metabolism as postulated for SCFAs [2]. Indeed, cell death studies with the colon epithelial cell line HT29 demonstrated that coconut oil, but not other oils exclusively consisting of fatty acids with long chain length [4], substantially decreased epithelial cell necrosis (Fig. 2).
Fig. 2.
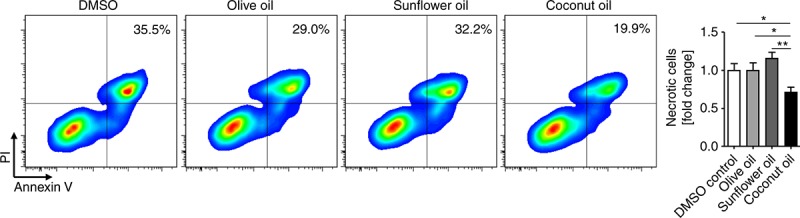
Assessment of epithelial cell death upon treatment with vegetable oils with distinct fatty acid composition. HT29 colon epithelial cells were grown in Dulbecco's modified Eagle's medium with 10% FCS and 1% Penicillin/Streptomycin until confluent and treated for 48 h with different oil formulations as indicated. Cells were then stained to assess epithelial cell death by anti‐EpCAM antibodies, Annexin V (both Biolegend), and propidium iodide (eBioscience) and immediately analyzed by flow cytometry. Representative pseudocolor plots (left) indicate the numbers of necrotic epithelial cells, which were identified as EpCAM+AnnexinV+PI+. Right: Quantitative flow cytometry (n = 6‐8 from three independent experiments). *p < 0.05, **p < 0.01
One week after initiation of daily coconut oil administrations, the patient reported decreasing abdominal pain and mucus secretion. After another 6 weeks of continuous therapy, hematochezia and mucus secretion had completely stopped. In a sigmoidoscopy performed after 8 weeks of daily therapy, clear improvement of endoscopic and histologic signs of inflammation could be observed. After 12 weeks of treatment, the patient was free of pain, back to work and physically active 3 to 4 times a week. Another follow‐up endoscopy after 5 months confirmed stable disease with only low‐grade inflammation. Similarly, histology verified maintained improvement. Daily coconut oil application has been continued by the patient for 6 months with continuous clinical response and without any adverse events. In the light of currently unavailable pharmacological formulations, local application of coconut oil can be considered as a treatment option in patients with severe refractory diversion colitis.
CONFLICT OF INTEREST
Guarantors of the article: Sebastian Zundler and Raja Atreya.
Specific author contributions: S.Z.: Outpatient care of the patient, collection, and interpretation of clinical, endoscopic, and experimental data, drafting of the manuscript; approved the final draft submitted. L.D.: Collection and interpretation of experimental data; approved the final draft submitted. K.M.: Outpatient care of the patient, collection, and interpretation of clinical data; approved the final draft submitted. E.B.: Collection and interpretation of experimental data; approved the final draft submitted. C.G.: Collection and interpretation of histopathological data and photography; approved the final draft submitted. T.R.: Collection and interpretation of endoscopic data; approved the final draft submitted. M.F.N.: Treatment supervision, interpretation of clinical and endoscopic data; approved the final draft submitted. R.A.: Outpatient care of the patient and treatment supervision, collection and interpretation of clinical, endoscopic and experimental data; approved the final draft submitted.
Financial support: German Research Foundation (DFG) ZU 377/3‐1 (SZ), DFG‐CRC1811 C02 (RA) and DFGSFB/TRR241 C02 (RA). The Heisenberg Professorship of RA is funded by the DFG.
Potential competing interests: None.
Informed consent: Informed patient consent for publication of this case report has been obtained.
Footnotes
Correspondence: R.A. (email: raja.atreya@uk‐erlangen.de)
REFERENCES
- 1.Haque S, Eisen RN, West AB. The morphologic features of diversion colitis: studies of a pediatric population with no other disease of the intestinal mucosa. Hum Pathol. 1993;24:211–9. [DOI] [PubMed] [Google Scholar]
- 2.Harig JM, Soergel KH, Komorowski RA, et al. Treatment of diversion colitis with short-chain-fatty acid irrigation. N Engl J Med. 1989;320:23–28. [DOI] [PubMed] [Google Scholar]
- 3.Vernia P, Cittadini M, Caprilli R, et al. Topical treatment of refractory distal ulcerative colitis with 5-ASA and sodium butyrate. Dig Dis Sci. 1995;40:305–7. [DOI] [PubMed] [Google Scholar]
- 4.Orsavova J, Misurcova L, Vavra Ambrozova J, et al. Fatty acids composition of vegetable oils and its contribution to dietary energy intake and dependence of cardiovascular mortality on dietary intake of fatty acids. Int J Mol Sci. 2015;16:12871–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Preter VD, Machiels K, Joossens M, et al. Faecal metabolite profiling identifies medium-chain fatty acids as discriminating compounds in IBD. Gut. 2015;64:447–58. [DOI] [PubMed] [Google Scholar]