

Abstract
Background
Key populations, including people who inject drugs (PWID), men who have sex with men (MSM), and female sex workers (FSW), are disproportionately affected by the HIV epidemic. Understanding the magnitude of, and informing the public health response to, the HIV epidemic among these populations requires accurate size estimates. However, low social visibility poses challenges to these efforts.
Objective
The objective of this study was to derive population size estimates of PWID, MSM, and FSW in Kampala using capture-recapture.
Methods
Between June and October 2017, unique objects were distributed to the PWID, MSM, and FSW populations in Kampala. PWID, MSM, and FSW were each sampled during 3 independent captures; unique objects were offered in captures 1 and 2. PWID, MSM, and FSW sampled during captures 2 and 3 were asked if they had received either or both of the distributed objects. All captures were completed 1 week apart. The numbers of PWID, MSM, and FSW receiving one or both objects were determined. Population size estimates were derived using the Lincoln-Petersen method for 2-source capture-recapture (PWID) and Bayesian nonparametric latent-class model for 3-source capture-recapture (MSM and FSW).
Results
We sampled 467 PWID in capture 1 and 450 in capture 2; a total of 54 PWID were captured in both. We sampled 542, 574, and 598 MSM in captures 1, 2, and 3, respectively. There were 70 recaptures between captures 1 and 2, 103 recaptures between captures 2 and 3, and 155 recaptures between captures 1 and 3. There were 57 MSM captured in all 3 captures. We sampled 962, 965, and 1417 FSW in captures 1, 2, and 3, respectively. There were 316 recaptures between captures 1 and 2, 214 recaptures between captures 2 and 3, and 235 recaptures between captures 1 and 3. There were 109 FSW captured in all 3 rounds. The estimated number of PWID was 3892 (3090-5126), the estimated number of MSM was 14,019 (95% credible interval (CI) 4995-40,949), and the estimated number of FSW was 8848 (95% CI 6337-17,470).
Conclusions
Our population size estimates for PWID, MSM, and FSW in Kampala provide critical population denominator data to inform HIV prevention and treatment programs. The 3-source capture-recapture is a feasible method to advance key population size estimation.
Keywords: sex workers, men who have sex with men, substance-related disorders, HIV, population size
Introduction
Key populations, including people who inject drugs (PWID), men who have sex with men (MSM), and female sex workers (FSW), are disproportionately affected by the HIV epidemic. Compared with the general population, higher prevalences of HIV infection have been documented in these key populations because of high-risk sexual behaviors and injecting drugs [1-3].
Understanding the magnitude of the HIV epidemic among these populations requires accurate population estimates. These estimates inform the scale of prevention and treatment programs and are needed for resource allocation, monitoring, and evaluation of the programs [4,5]. Traditional methods of estimating the size of these populations, such as a census, are challenging because of the marginalized nature of these populations. Criminalization of sexual behaviors and drug use, in addition to human rights abuses, and severe stigma keep these populations socially hidden [6].
Even in Uganda’s generalized epidemic, the high HIV prevalence observed in several studies of key populations suggests that they may account for a substantial number of HIV infections [7-9]. In Kampala, HIV prevalence among MSM was estimated at 13.7% and 31.3% among FSW in 2012 [8]. Studies among PWID have estimated the prevalence between 11% and 34% (report by Uganda Harm Reduction Network, 2017). Size estimates for PWID, FSW, and MSM in Uganda and Kampala, in particular, are scarce. Existing estimates for FSW and MSM (13,200 [95% confidence interval 10,200-16,200] and 7900 [95% credible interval (CI) 4400-11,300], respectively) in Kampala are outdated (2012) (report by The Crane Survey, 2012). Hospital data on people in drug abuse treatment suggest that there are 10 PWID per 100,000 people (or 70 to 80 people) in Kampala [10]. As a result, HIV services and policies to address population specific needs are likely underestimated and inadequate.
There are many methods to estimate population sizes, each with various strengths and limitations [4]. Capture-recapture (CRC) is one method that has been used in epidemiology [11-13] to estimate the size of key populations [14-17]. This method begins with an initial capture, as individual members of the target population are sampled, tagged, or offered a unique object, and released back into the population. A short period later (days or weeks), a second, independent capture is sampled; during this encounter, individuals will be assessed or asked whether they have been previously tagged, that is, received an object. Additional captures increase the number of data points from which estimates are generated, generally resulting in more stable and robust key population size estimates [5,11].
We used CRC to estimate the sizes of key populations in Kampala, Uganda, in June and October 2017.
Methods
Capture-Recapture
The CRC methodology is described in detail elsewhere [11,13,18-20]. Briefly, 4 main assumptions must hold for CRC to produce accurate population estimates: the population is closed; individual captures are independent; the capture history of each target population member is accurate; and the probability of being captured is homogenous [21]. The degree to which these assumptions are violated determine the accuracy of CRC-based population size estimates.
We defined MSM as men, aged 18 years or above, who self-identified as MSM. We defined FSW as women, aged 15 years or above, who reported currently selling sex for money. We defined PWID as people, aged 15 years or above, who reported currently injecting nonprescription or illegal drugs.
Local community-based organizations were consulted to discuss the selected objects (tags) and recommend peer distributors for each target population. Selected objects had no monetary value, were unique (ie, unavailable in Uganda), and differed according to each population. Different objects were used for each capture. Objects were procured in different colors with each color assigned for distribution in a different Division for quality assurance and to get a crude sense of mobility of objects across Kampala. Objects included keychains with bottle openers and lights, bracelets, and compact mirrors with unique phrases or artwork.
Data from mapping exercises and previous FSW and MSM size estimation conducted in 2011 and 2012 in Kampala were used to generate a range of the number of objects to be distributed in each of the 5 administrative Divisions of Kampala. As the PWID population had no prior population estimates, we utilized data from a nongovernmental organization, Community Health Alliance Uganda, that provided an estimated number of PWID hotspots per Division.
Data Collection
Peer staff were assigned to a particular Division in Kampala and within that Division, to a set of parishes (there were a total of 99 parishes in Kampala). Each parish had only 1 distributor per capture. A total of 2 peer FSW and MSM distributors were assigned to each of the 5 Divisions, whereas 1 PWID distributor was assigned to each Division. To facilitate independence between captures, new MSM and FSW distributors were selected for each capture stage. For PWID, the distributors remained the same, but were rotated and assigned to a new Division. Peer distributors were asked to visit their assigned parishes and to distribute unique objects in areas where the population members work (FSW) or congregate (MSM and PWID). This included public spaces such as streets, bars, clubs, restaurants, and brothels.
Data collection for PWID and MSM CRC was conducted during June 2017 and during October 2017 for FSW. Each capture was set one week apart to minimize the effect of migration in and out of Kampala. All data were collected using ODK Collect on Android smartphones [22]. When a distributor encountered a likely member of the target population, they verified that the individual (1) was a member of the target population and (2) had not been previously approached by another distributor (in a different Division or parish that same week). Target population members were instructed to keep the unique objects with them for the next 2 weeks and not to give it away. Distributors recorded whether the target population member accepted or rejected an object, estimated the age group (15 to 17 years, 18 to 24 years, or >25 years), and documented the global positioning system (GPS) point of the encounter. MSM who appeared to be under the age of 18 years were not approached. No personal identifiers were collected and no compensation was provided. All questions in the ODK Collect program were contingent on the previous question being recorded to limit missing information. Per the protocol, women in the target population who were estimated to be under 18 years of age were referred for specialized support services.
During captures 2 and 3, members of the target population were asked to produce all of the objects they had received. If the approached population member claimed to have received one, but did not have the object with them, they were asked to identify the correct object from a piece of paper with pictures of 10 to 15 different objects (some similar to the real objects, some very different). Distributors recorded the picture the individual identified, but did not reveal whether they were correct or not. Target population members could have received no object, the capture 1 object, the capture 2 object, or both capture 1 and 2 objects. We defined a recapture as an individual who presented the object or was able to identify the correct object from a set of pictures.
Statistical Analysis
We calculated 3-source CRC (3SCRC) size estimates for all populations and when unable to calculate a 3SCRC, a 2-source CRC (2SCRC) size estimate was calculated in its place. We summarized 2-source capture histories into a 2×2 contingency table where the rows and columns represent the 2 capture occasions. Population size (N) for this group was calculated using the Lincoln-Petersen estimator assuming independence as follows [23]:
 = M1*M2/R
= M1*M2/R
where
=
estimated population size
M1=number of individuals recorded in first capture
M2=number of individuals recorded in second capture
R=number of individuals recorded in both captures
As the population size distribution was skewed and violated the normality assumption, we calculated a bootstrap 95% confidence interval for by resampling capture 2 data, 10,000 times (with replacement).
Furthermore, 3SCRC data were aggregated by captures into 2k-1 observed frequencies, where k represents the number of captures (k=3). Each capture is listed as either 1 or 0 representing whether individuals are captured or not captured, respectively. Population sizes and 95% credible intervals (CI) were estimated using a Bayesian approach.
Latent-Class Bayesian Nonparametric Model
Consider the Kampala FSW and MSM populations to each be a closed finite population of N individuals. We conducted 3 capture stages for each population. Let xi=(x1i, xi2, xi3), with xik=1 if the ith individual was captured in the kth FSW capture stage and 0 otherwise. Thus, xi,i=1,…,N, represents the complete capture history of each individual in the FSW population (similarly for the MSM population). However, of the N individuals in the population, we are only able to capture n<N, where any individual with a capture history equal to (0,0,0) is unobserved. The total number of unobserved individuals is n0=N – n, the number to be estimated. Hence, 3SCRC estimation of the size of a closed population is essentially a missing data problem.
Following Little and Rubin [24], we can use a Bayesian approach to model the mechanism that leads to missing data and then to estimate the number of missing individuals. When there is heterogeneity of capture probabilities among individuals, this modeling is complicated as the heterogeneity induces dependency among capture stages. A mixture model approach is one technique used in CRC to account for individual heterogeneity [25]. Our choice of mixture model is the latent-class Bayesian nonparametric model of Dunson and Xing [26]. This choice of model avoids the model selection problem of choosing an appropriate number of latent classes, K, in advance [26].
The latent-class Bayesian nonparametric model accommodates various forms of capture probabilities and implements an automatic model selection procedure [27]. Uninformative priors, that is, those that have minimal influence on the inference and dominated by the likelihood function, were specified for the Dirichlet process parameter (α~Gamma (0.25, 0.25)) as suggested in the literature [28]. We used K=10 latent classes; 150,000 samples from the posterior distribution were drawn with a burn-in of 10,000 iterations and a thinning interval of 100 iterations to specify the MCMC sampling.
We performed a sensitivity analysis to investigate the robustness of the posterior distribution of N to a range of priors for α. Smaller values favor sparse mixtures, whereas large values favor a more complex joint distribution. Convergence of the Markov Chain Monte Carlo sampling was assessed using trace plots and by setting various burn-in periods. Statistical analysis was performed in R (version 3.4.2) [29] and the Bayesian nonparametric latent-class capture-recapture package (LCMCR; sample R code for LCMCR analysis is available in Multimedia Appendix 1) [30].
The study protocol was approved by the human subjects protection board at Makerere University School of Public Health and the Centers for Disease Control and Prevention (CDC).
Results
Sampling
People Who Inject Drugs
Individuals accepted 467 bracelets and refused 5 during capture 1. Individuals accepted 450 bracelets and refused 18 during capture 2. In total, 54 PWID were captured in both capture 1 and 2 (Figure 1). During capture 3, distributors approached and asked 475 PWID to present/identify the object(s); however, recording errors prevented the use of capture 3 data (Figure 1).
Figure 1.
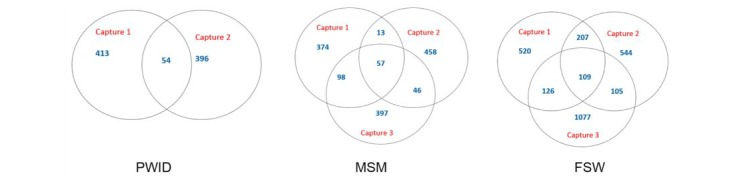
Capture history diagrams for people who inject drugs (PWID), men who have sex with men (MSM), and female sex workers (FSW), Kampala, Uganda, 2017.
Men Who Have Sex With Men
Individuals accepted 542 keychains and refused 52 during capture 1. Individuals accepted 574 keychains and refused 26 during capture 2. During capture 3, distributors approached and asked 598 MSM to present/identify the object(s). There were 70 captured in captures 1 and 2, 103 captured in captures 2 and 3, and 155 captured in captures 1 and 3. There were 57 MSM captured in all 3 captures.
Female Sex Workers
Individuals accepted 962 mirrors and refused 77 during capture 1. Individuals accepted 965 mirrors and refused 41 during capture 2. During capture 3, distributors approached and asked 1417 FSW to present/identify the object(s). There were 316 captured in captures 1 and 2, 214 captured in captures 2 and 3, and 235 captured in captures 1 and 3. There were 109 FSW captured in all 3 captures.
We estimated the number of PWID to be 3892 (95% confidence interval: 3090-5126) using 2SCRC (Table 1). We estimated the population of MSM in Kampala to be 14,019 (95% CI 4995-40,949) and the number of FSW to be 8848 (95% CI 6337-17,470) using the Bayesian approach to 3SCRC. Sensitivity analyses results for the MSM and FSW estimates showed no substantial difference between the estimates as can be seen from the overlapping 95% CI (Figure 2).
Table 1.
Population size estimates for people who inject drugs, men who have sex with men, and female sex workers, Kampala, Uganda, 2017.
| Populationa | Estimates (95% confidence interval)b |
| People who inject drugs | 3892 (3090-5126) |
| Men who have sex with men | 14,019 (4995-40,949) |
| Female sex workers | 8848 (6337-17,470) |
aPopulation of people who inject drugs was estimated using 2-source capture-recapture; populations of men who have sex with men and female sex workers were estimated using 3-source capture-recapture with the Bayesian nonparametric latent-class capture-recapture (LCMCR) package.
b95% confidence interval for people who inject drugs and 95% credible interval for men who have sex with men and female sex workers.
Figure 2.
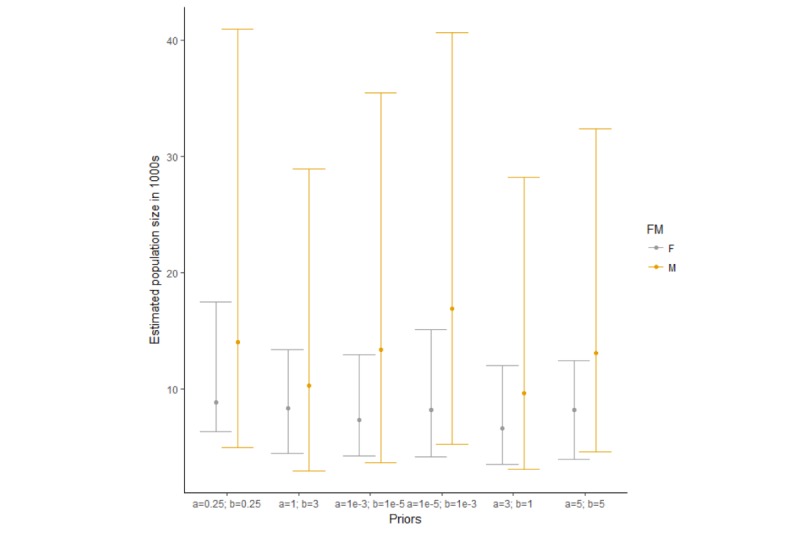
Three-source capture-recapture sensitivity analysis comparing the median and 95% credible intervals of the population size for men who have sex with men and female sex workers, Kampala, Uganda, 2017. Error bars denote the lower and upper bounds of the 95% credible intervals, whereas the filled circles indicate the median. F: female; M: male.
Discussion
These population size estimates represent the first use of 3SCRC for FSW and MSM and the first use of 2SCRC for PWID in Kampala, Uganda.
Our 2SCRC PWID estimate of 3892 (95% confidence interval: 3090-5126) is substantially higher than previous estimates (10 PWID per 100,000 people or 70 to 80 PWID total) which were based on clinic data and counts at hotspots [10]. Although we were unable to use data from a third capture of PWID because of data collection errors, our 2-source estimate suggests that injection drug use may be more prevalent than originally expected [10].
We compared our MSM and FSW results with the population size estimates from 2012. Our MSM estimate (14,019) is higher than the 2012 estimate of 7900 (report by The Crane Survey, 2012). Our crude Kampala MSM estimate represents approximately 4% of the adult male population (aged 18 years or above) in Kampala [31]. Factors influencing our MSM population size estimate might reflect long-term migration patterns among MSM, both rural to urban, as well as migration from smaller to larger urban settings [32,33]. To some extent, MSM size estimates are also determined by the proportion of gay men who may or may not practice their same sex sexuality, a potentially large factor given the highly stigmatized climate in Uganda and its accompanying social norms (marriage and having children). Global estimates suggest that MSM represent 3% to 5% of the general population (ie, before taking migration patterns into account) and can be higher depending on the region [34]. To the extent that rural gay men may be more likely to migrate to urban settings compared with rural heterosexual men, we can expect correspondingly larger proportions of adult urban MSM. Furthermore, Kampala and other urban settings are rapidly growing in total general population size; hence, we can expect the use of equal proportional estimates in 2012 and 2017 to lead to higher absolute estimates in 2017.
The FSW result (8848) is lower than the 2012 estimate of 13,200 (report by The Crane Survey, 2012). Our FSW estimate represents approximately 2% of the Kampala adult female population (aged 15 years and above) [31]. Global FSW population size estimates differ depending upon the sampling method and location. In sub-Saharan African FSW estimates generally fall within 0.7% to 4.3% of the adult female population [35].
Both the MSM and FSW 2012 estimates fall within our 95% CI; however, the CRC methods reported here differ from the previous round of population size estimation for MSM and FSW. Although both employed CRC methodology, the previous estimates used respondent-driven sampling (RDS) surveys as capture 2. There was a difference of 9 to 12 months between captures, compared with only a week for our study. A longer period between captures allows for more in- and out-migration (to and from Kampala), violating one of the four assumptions. As a result, fewer recaptures can be expected, resulting in an inflated size estimate.
There were a number of limitations to the design of the estimation activity. Possible violations of the underlying CRC assumptions could influence the validity of our outcomes and may have resulted in inaccurate population sizes and wider confidence intervals. First, we used unique objects as a tagging mechanism to maintain the anonymity of sampled populations. However, not all individuals were carrying the unique object during subsequent captures, complicating the identification of recaptures. In addition, we must assume that the person presenting the object is the person who received the object (an inherent limitation present in anonymous sampling-based CRC). We tried to mitigate the bias involved in tagging individuals with objects by offering individuals the opportunity to identify the objects from a set of pictures, in addition to reducing the time between captures to 1 week. The short time between each capture also gave us more confidence in the assumption of a closed population. Although we recognize that these populations are mobile, there was likely little change over a 1-week period.
To minimize dependencies between captures, we used different distributors for each capture. Nevertheless, the capture probabilities were likely heterogeneous and target population members tagged in capture 1 may have been more likely to be tagged in captures 2 and 3. This is especially true for MSM and PWID, where we collected captures at known MSM- or PWID-friendly venues. Individuals with higher social visibility are more likely captured at these known sites. Individuals with higher social visibility are more likely to be captured, thus our results are likely to be underestimates for all populations. One way to capture individuals with lower social visibility would be to use an RDS survey as the third capture; however, the target sample size would need to be achieved quickly to mitigate in- and out-migration. In addition, one might expand captures to various other data sources (not just object distribution) to include service lists, social media or other Web-based sites to reach those who might not attend venues.
Our final estimates were based on a Bayesian approach to accommodate the complex patterns of heterogeneity between captures and aggregation of homogenous strata into latent classes, whereas other statistical approaches make reasonably strong assumptions about the structure of the joint distribution of capture patterns [27]. In contrast, the latent-class Bayesian approach is a model-averaging technique and attempts to estimate the joint distribution directly from the data as much as possible [27]. Our use of the LCMCR method to estimate the size of hard-to-reach human population is innovative as the approach is not originally developed for analyzing epidemiological data such as those obtained from in-person listing of key populations. The unique individual characteristic of these populations contributes to most of the dependence between capture histories; therefore, the nonparametric latent-class model implemented in LCMCR is reasonable to use.
Working with each of the key populations brought on unique challenges and could have resulted in biased population size estimates. Our definition of each key population was sensitive and it is possible that nontarget population members were counted in each capture. We had substantial challenges finding and training MSM for this activity. In addition, the refusal rate for the unique object among MSM was higher than among the other 2 populations who rarely refused the object (8.8% of MSM compared with 1.2% for FSW and 1.0% for PWID). Furthermore, we found at least one problematic distributor in each target population, which may have biased our results. For example, in capture 3, one particular PWID distributor sampled 54 PWID (all found in the same Division) who had received both objects distributed in capture 1 and 2. Allegedly, all 54 PWID had the exact same color objects. As investigators knew which color had been distributed in each Division (a quality assurance mechanism), and the recorded color of the object had been distributed in another Division, it became clear that the data had very likely been fabricated; hence, we decided to exclude capture 3. There were also anecdotal observations of target population members approaching the distributor hoping to get an object, especially among the FSW population. This suggested that the objects may not always have been given out at random and the members of the target populations did not necessarily have an equal chance of being tagged. Increased monitoring and supervisor would likely help mitigate some of these challenges. One of the benefits of using 3SCRC is the ability to partially account for such dependencies by allowing sources to be examined pairwise (interactions) [13].
In conclusion, we generated new size estimates for key populations in Kampala and demonstrated that 3SCRC is a feasible size estimation method. These estimates will provide critical denominators that may serve as a basis for HIV prevention and treatment program planning by HIV coordinating bodies in Uganda. As we move closer to HIV epidemic control, estimating the size of these key populations will be important to examine and document progress.
Acknowledgments
The authors would like to thank the Crane Survey staff for their dedication. In addition, the authors would like to thank the community based organizations who dedicated their time to this activity: Uganda Harm Reduction Network, Women’s Organization Network for Human Rights Advocacy, Lady Mermaid's Bureau, Alliance of Women, Advocating for Change, Women Arise for Change, Organization for Gender Empowerment and Rights Advocacy (Ogera Uganda), Empower at Dusk, Women’s Association, Serving Lives Under Marginalization, Women’s Positive Empowerment Initiative, Ice Breakers, Youth on the Rock Foundation, Spectrum Uganda, Come out Post Test Club, Kuchu Shiners Uganda, Frank and Candy Uganda, and Rainbow Mirrors Uganda.
This project work has been supported by the President’s Emergency Plan for AIDS Relief through the CDC under the terms of project number U2GGH000466.
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the funding agencies.
Abbreviations
- 2SCRC
2-source capture-recapture
- 3SCRC
3-source capture-recapture
- CDC
Centers for Disease Control and Prevention
- CI
credible interval
- CRC
capture-recapture
- FSW
female sex workers
- LCMCR
Bayesian nonparametric latent-class capture-recapture package
- MSM
men who have sex with men
- PWID
people who inject drugs
- RDS
respondent-driven sampling
Sample R code for LCMCR analysis.
Footnotes
Authors' Contributions: All authors substantially contributed to the study’s design, conduct, or to data analysis and interpretation and wrote or edited parts of the paper and approved the final version for publication.
Conflicts of Interest: None declared.
References
- 1.Baral S, Beyrer C, Muessig K, Poteat T, Wirtz AL, Decker MR, Sherman SG, Kerrigan D. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012 Jul;12(7):538–49. doi: 10.1016/S1473-3099(12)70066-X.S1473-3099(12)70066-X [DOI] [PubMed] [Google Scholar]
- 2.Aceijas C, Stimson GV, Hickman M, Rhodes T, United Nations Reference Group on HIV/AIDS Prevention and Care among IDU in Developing and Transitional Countries Global overview of injecting drug use and HIV infection among injecting drug users. AIDS. 2004 Nov 19;18(17):2295–303. doi: 10.1097/00002030-200411190-00010.00002030-200411190-00010 [DOI] [PubMed] [Google Scholar]
- 3.Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz AL, Brookmeyer R. Global epidemiology of HIV infection in men who have sex with men. Lancet. 2012 Jul 28;380(9839):367–77. doi: 10.1016/S0140-6736(12)60821-6. http://europepmc.org/abstract/MED/22819660 .S0140-6736(12)60821-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.UNAIDS. 2011. Dec 31, [2019-06-03]. Guidelines on Estimating the Size of Populations Most at Risk to HIV https:/www.unaids.org/en/resources/documents/2011/2011_Estimating_Populations .
- 5.Abdul-Quader AS, Baughman AL, Hladik W. Estimating the size of key populations: current status and future possibilities. Curr Opin HIV AIDS. 2014 Mar;9(2):107–14. doi: 10.1097/COH.0000000000000041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization. 2016. [2019-06-03]. Estimating Sizes of Key Populations: Guide for HIV Programming in Countries of the Middle East and North Africa http://applications.emro.who.int/dsaf/EMROPub_2016_EN_19361.pdf .
- 7.Hladik W, Baughman AL, Serwadda D, Tappero JW, Kwezi R, Nakato ND, Barker J. Burden and characteristics of HIV infection among female sex workers in Kampala, Uganda - a respondent-driven sampling survey. BMC Public Health. 2017 Jun 10;17(1):565. doi: 10.1186/s12889-017-4428-z. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-017-4428-z .10.1186/s12889-017-4428-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hladik W, Sande E, Berry M, Ganafa S, Kiyingi H, Kusiima J, Hakim A. Men who have sex with men in Kampala, Uganda: results from a bio-behavioral respondent driven sampling survey. AIDS Behav. 2017 May;21(5):1478–90. doi: 10.1007/s10461-016-1535-2.10.1007/s10461-016-1535-2 [DOI] [PubMed] [Google Scholar]
- 9.Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA, Wodak A, Panda S, Tyndall M, Toufik A, Mattick RP, 2007 Reference Group to the UN on HIV and Injecting Drug Use Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet. 2008 Nov 15;372(9651):1733–45. doi: 10.1016/S0140-6736(08)61311-2.S0140-6736(08)61311-2 [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization. 2010. [2019-06-04]. Atlas of Substance Use: Resources for the Prevention and Treatment of Substance Use Disorders https://www.who.int/substance_abuse/activities/msbatlasfrontncont.pdf?ua=1 .
- 11.Hook EB, Regal RR. Capture-recapture methods in epidemiology: methods and limitations. Epidemiol Rev. 1995;17(2):243–64. doi: 10.1093/oxfordjournals.epirev.a036192. [DOI] [PubMed] [Google Scholar]
- 12.Hook EB, Regal RR. Recommendations for presentation and evaluation of capture-recapture estimates in epidemiology. J Clin Epidemiol. 1999 Oct;52(10):917–26; discussion 929-33. doi: 10.1016/s0895-4356(99)00060-8.S0895435699000608 [DOI] [PubMed] [Google Scholar]
- 13.van Hest R. Capture-Recapture Methods in Surveillance of Tuberculosis and Other Infectious Diseases. Rotterdam, the Netherlands: University Medical Center; 2007. [Google Scholar]
- 14.Des Jarlais D, Khue PM, Feelemyer J, Arasteh K, Thi Huong D, Thi Hai Oanh K, Thi Giang H, Thi Tuyet Thanh N, Vinh VH, Heckathorn DD, Moles JP, Vallo R, Quillet C, Rapoud D, Michel L, Laureillard D, Hammett T, Nagot N. Using dual capture/recapture studies to estimate the population size of persons who inject drugs (PWID) in the city of Hai Phong, Vietnam. Drug Alcohol Depend. 2018 Apr 01;185:106–11. doi: 10.1016/j.drugalcdep.2017.11.033. http://europepmc.org/abstract/MED/29432973 .S0376-8716(18)30030-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Karami M, Khazaei S, Poorolajal J, Soltanian A, Sajadipoor M. Estimating the population size of female sex worker population in Tehran, Iran: application of direct capture-recapture method. AIDS Behav. 2017 Aug;21(8):2394–400. doi: 10.1007/s10461-017-1803-9.10.1007/s10461-017-1803-9 [DOI] [PubMed] [Google Scholar]
- 16.Ruiz MS, O'Rourke A, Allen ST. Using capture-recapture methods to estimate the population of people who inject drugs in Washington, DC. AIDS Behav. 2016 Feb;20(2):363–8. doi: 10.1007/s10461-015-1085-z. http://europepmc.org/abstract/MED/25963771 .10.1007/s10461-015-1085-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Vuylsteke B, Sika L, Semdé G, Anoma C, Kacou E, Laga M. Estimating the number of female sex workers in Côte d'Ivoire: results and lessons learned. Trop Med Int Health. 2017;22(9):1112–8. doi: 10.1111/tmi.12911. doi: 10.1111/tmi.12911. [DOI] [PubMed] [Google Scholar]
- 18.Nanan DJ, White F. Capture-recapture: reconnaissance of a demographic technique in epidemiology. Chronic Dis Can. 1997;18(4):144–8. [PubMed] [Google Scholar]
- 19.Neugebauer R. Application of a capture-recapture method (the Bernoulli census) to historical epidemiology. Am J Epidemiol. 1984 Oct;120(4):626–34. doi: 10.1093/oxfordjournals.aje.a113924. [DOI] [PubMed] [Google Scholar]
- 20.Qiu C, Shi L. [Capture-recapture methods and its uses in epidemiology] Zhonghua Yu Fang Yi Xue Za Zhi. 1998 Jan;32(1):54–5. [PubMed] [Google Scholar]
- 21.Neugebauer R, Wittes J. Voluntary and involuntary capture-recapture samples--problems in the estimation of hidden and elusive populations. Am J Public Health. 1994 Jul;84(7):1068–9. doi: 10.2105/ajph.84.7.1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hartung C, Lerer A, Anokwa Y, Tseng C, Brunette W, Borriello G. ICTD. 2010. [2019-06-04]. Open Data Kit: Tools to Build Information Services for Developing Regions http://www.nixdell.com/classes/Tech-for-the-underserved/Hartung.pdf .
- 23.Wittes JT, Colton T, Sidel VW. Capture-recapture methods for assessing the completeness of case ascertainment when using multiple information sources. J Chronic Dis. 1974 Feb;27(1-2):25–36. doi: 10.1016/0021-9681(74)90005-8. doi: 10.1016/0021-9681(74)90005-8. [DOI] [PubMed] [Google Scholar]
- 24.Little RJ, Rubin DB. Statistical Analysis With Missing Data: Second Edition. New York: John Wiley & Sons; 2002. [Google Scholar]
- 25.McCrea RS, Morgan BJ. Analysis Of Capture-Recapture Data. Boca Raton: Chapman And Hall; 2014. [Google Scholar]
- 26.Dunson DB, Xing C. Nonparametric Bayes modeling of multivariate categorical data. J Am Stat Assoc. 2012 Jan 01;104(487):1042–51. doi: 10.1198/jasa.2009.tm08439. http://europepmc.org/abstract/MED/23606777 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Manrique-Vallier D. Bayesian population size estimation using Dirichlet process mixtures. Biometrics. 2016 Dec;72(4):1246–54. doi: 10.1111/biom.12502. [DOI] [PubMed] [Google Scholar]
- 28.Si Y, Reiter JP. Nonparametric Bayesian multiple imputation for incomplete categorical variables in large-scale assessment surveys. J Educ Behav Stat. 2013 Oct;38(5):499–521. doi: 10.3102/1076998613480394. [DOI] [Google Scholar]
- 29.The R Project. [2019-06-05]. The R Project for Statistical Computing https://www.R-project.org/
- 30.Manrique-Vallier D. R Package Documentation. 2019. [2019-06-04]. LCMCR: Bayesian Non-Parametric Latent-Class Capture-Recapture https://rdrr.io/cran/LCMCR/
- 31.United Nations Statistics Division. Kampala, Uganda: Uganda Bureau of Statistics; 2016. [2019-06-04]. The National Population and Housing Census 2014: Main Report https://unstats.un.org/unsd/demographic/sources/census/wphc/Uganda/UGA-2016-05-23.pdf . [Google Scholar]
- 32.Lieb S, Fallon SJ, Friedman SR, Thompson DR, Gates GJ, Liberti TM, Malow RM. Statewide estimation of racial/ethnic populations of men who have sex with men in the U.S. Public Health Rep. 2011;126(1):60–72. doi: 10.1177/003335491112600110. http://europepmc.org/abstract/MED/21351396 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lieb S, Thompson DR, Misra S, Gates GJ, Duffus WA, Fallon SJ, Liberti TM, Foust EM, Malow RM, Southern AIDS Coalition MSM Project Team Estimating populations of men who have sex with men in the southern United States. J Urban Health. 2009 Nov;86(6):887–901. doi: 10.1007/s11524-009-9401-4. http://europepmc.org/abstract/MED/19911282 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cáceres C, Konda K, Pecheny M, Chatterjee A, Lyerla R. Estimating the number of men who have sex with men in low and middle income countries. Sex Transm Infect. 2006 Jun;82(Suppl 3):iii3–9. doi: 10.1136/sti.2005.019489. http://europepmc.org/abstract/MED/16735290 .82/suppl_3/iii3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vandepitte J, Lyerla R, Dallabetta G, Crabbé F, Alary M, Buvé A. Estimates of the number of female sex workers in different regions of the world. Sex Transm Infect. 2006 Jun;82(Suppl 3):iii18–25. doi: 10.1136/sti.2006.020081. http://europepmc.org/abstract/MED/16735288 .82/suppl_3/iii18 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Sample R code for LCMCR analysis.