

Abstract
Background
Exercise programmes are often recommended for managing ankylosing spondylitis (AS), to reduce pain and improve or maintain functional capacity.
Objectives
To assess the benefits and harms of exercise programmes for people with AS.
Search methods
We searched CENTRAL, the Cochrane Library, MEDLINE Ovid, EMBASE Ovid, CINAHL EBSCO, PEDro, Scopus, and two trials registers to December 2018. We searched reference lists of identified systematic reviews and included studies, handsearched recent relevant conference proceedings, and contacted experts in the field.
Selection criteria
We included reports of randomised controlled trials (RCT) of adults with AS that compared exercise therapy programmes with an inactive control (no intervention, waiting list) or usual care.
Data collection and analysis
We used standard Cochrane methodology.
Main results
We included 14 RCTs with 1579 participants with AS. Most participants were male (70%), the median age was 45 years (range 39 to 47), and the mean symptom duration was nine years. The most frequently used exercises were those designed to help improve strength, flexibility, stretching, and breathing. Most exercise programmes were delivered along with drug therapy or a biological agent. We judged most of the studies at unclear or high risk of bias for several domains. All 14 studies provided data obtained immediately upon completion of the exercise programme. The median exercise programme duration was 12 weeks (interquartile range (IQR) 8 to 16). Three studies (146 participants) provided data for medium‐term follow‐up (< 24 weeks after completion of the exercise programmes), and one (63 participants) for long‐term follow‐up (> 24 weeks after completion of the exercise programmes). Nine studies compared exercise programmes to no intervention; five studies compared them to usual care (including physiotherapy, medication, or self‐management).
Exercise programmes versus no intervention
All data were obtained immediately upon completion of the exercise programme.
For physical function, measured by a self‐reporting questionnaire (the Bath Ankylosing Spondylitis Functional Index (BASFI) scale, 0 to 10; lower is better), moderate‐quality evidence showed a no important clinically meaningful improvement with exercise programmes (mean difference (MD) ‐1.3, 95% confidence interval (CI) ‐1.7 to ‐0.9; 7 studies, 312 participants; absolute reduction 13%, 95% CI 17% to 9%).
For pain, measured on a visual analogue scale (VAS, 0 to 10, lower is better), low‐quality evidence showed an important clinically meaningful reduction of pain with exercise (MD ‐2.1, 95% CI ‐3.6 to ‐0.6; 6 studies, 288 participants; absolute reduction 21%, 95% CI 36% to 6%).
For patient global assessment of disease activity, measured by a self‐reporting questionnaire (the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scale, 0 to 10, lower is better), moderate‐quality evidence showed no important clinically meaningful reduction with exercise (MD ‐0.9, 95% CI ‐1.3 to ‐0.5; 6 studies, 262 participants; absolute reduction 9%, 95% CI 13% to 5%).
For spinal mobility, measured by a self‐reporting questionnaire (the Bath Ankylosing Spondylitis Metrology Index (BASMI) scale, 0 to 10, lower is better), very low‐quality evidence showed an improvement with exercise (MD ‐0.7 95%, ‐1.3 to ‐0.1; 5 studies, 232 participants) with no important clinical meaningful benefit (absolute reduction 7%, 95% CI 13% to 1%).
For fatigue, measured on a VAS (0 to 10, lower is better), very low‐quality evidence showed a no important clinically meaningful reduction with exercise (MD ‐1.4, 95% CI ‐2.7 to ‐0.1; 2 studies, 72 participants; absolute reduction 14%, 95% CI 27% to 1%).
Exercise programmes versus usual care
All data were obtained immediately upon completion of the exercise programme.
For physical function, measured by the BASFI scale, moderate‐quality evidence showed an improvement with exercise (MD ‐0.4, 95% CI ‐0.6 to ‐0.2; 5 studies, 1068 participants). There was no important clinical meaningful benefit (absolute reduction 4%, 95% CI 6% to 2%).
For pain, measured on a VAS (0 to 10, lower is better), moderate‐quality evidence showed a reduction of pain with exercise (MD ‐0.5, 95% CI ‐0.9 to ‐0.1; 2 studies, 911 participants; absolute reduction 5%, 95% CI 9% to 1%). No important clinical meaningful benefit was found.
For patient global assessment of disease activity, measured by the BASDAI scale, low‐quality evidence showed a reduction with exercise (MD ‐0.7, 95% CI ‐1.3 to ‐0.1; 5 studies, 1068 participants), but it was not clinically important (absolute reduction 7%, 95% CI 13% to 1%) with important clinical meaningful benefit
For spinal mobility, measured by the BASMI scale, very low‐quality evidence found a no important clinically meaningful improvement with exercise (MD ‐1.2, 95% CI ‐2.8 to 0.5; 2 studies, 85 participants; absolute reduction 12%, 95% CI 5% less to 28% more). There was no important clinical meaningful benefit.
None of the studies measured fatigue.
Adverse effects
We found very low‐quality evidence of the effect of exercise versus either no intervention, or usual care. We are uncertain of the potential for harm of exercises, due to low event rates, and a limited number of studies reporting events.
Authors' conclusions
We found moderate‐ to low‐quality evidence that exercise programmes probably slightly improve function, may reduce pain, and probably slightly reduce global patient assessment of disease activity, when compared with no intervention, and measured upon completion of the programme. We found moderate‐ to low‐quality evidence that exercise programmes probably have little or no effect on improving function or reducing pain, when compared with usual care, and may have little or no effect on reducing patient assessment of disease activity, when measured upon completion of the programmes. We are uncertain whether exercise programmes improve spinal mobility, reduce fatigue, or induce adverse effects.
Plain language summary
Benefits and harms of exercise programmes for people with ankylosing spondylitis
Review question
We reviewed the evidence for the benefits and harms of exercise programmes for people with ankylosing spondylitis (AS).
Background
Exercise programmes are often recommended for people with AS, to reduce pain, and improve joint mobility or function.
Study characteristics
We searched for randomised controlled trials (RCT) to December 2018. We found 14 reports (1579 participants). Studies were performed in nine different countries. Most participants were men, aged 39 to 47 years old, who had symptom from 9 to 18 years. Mostly, the programmes included exercises developed to improve strength, flexibility, stretching, and breathing, and were added to drug therapy or a biological agent.
Key results
All data were obtained immediately upon completion of the exercise programme.
Exercise programmes versus no intervention
Exercise probably slightly improves function (moderate‐quality evidence), slightly reduces patient‐reported disease activity (moderate‐quality evidence), and may reduce pain (low‐quality evidence). We are uncertain of the effect on spinal mobility and fatigue (very low‐quality evidence).
Physical function was measured on a self‐reporting questionnaire, the Bath Ankylosing Spondylitis Functional Index (BASFI) scale (0 to 10; lower means better function). People who did not exercise rated their function at 4.1 points; those who exercised rated it 1.3 points lower (13% absolute improvement).
Pain was measured on a visual analogue scale (VAS, 0 to 10; lower means less pain). People who did not exercise rated their pain at 6.2 points; those who exercised rated it 2.1 points lower (21% absolute improvement).
Patient global assessment of disease activity was measured on a self‐reporting questionnaire, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI, 0 to 10, lower means less disease activity). People who did not exercise rated their disease activity at 3.7 points; those who exercised rated it 0.9 points lower (9% absolute improvement).
Spinal mobility was measured on a self‐reporting questionnaire, the Bath Ankylosing Spondylitis Metrology Index (BASMI, 0 to 10, lower means better mobility). People who did not exercise rated their spinal mobility at 3.8 points; those who exercised rated it 0.7 points lower (7% absolute improvement).
Fatigue was measured on a VAS (0 to 10, lower means less fatigue). People who did not exercise rated their fatigue at 3 points; those who exercised rated it 1.4 points lower (14% absolute improvement).
Exercise programmes versus usual care
Exercise probably results in little or no improved function or reduced pain (moderate‐quality evidence), and may have little or no effect in reducing patient‐reported disease activity (low‐quality evidence). We are uncertain of the effect on spinal mobility (very low‐quality evidence).
Physical function. People who received usual care rated their function at 3.7 points on the BASFI; those who exercised rated it 0.4 points lower (4% absolute improvement).
Pain. People who received usual care rated their pain at 3.7 points on a 10‐point VAS; those who exercised rated it 0.5 points lower (5% absolute improvement).
Patient global assessment of disease activity. People who received usual care rated their disease activity at 3.7 points on the BASDAI; those who exercised rated it 0.7 points lower (7% absolute improvement).
Spinal mobility. People who received usual care rated their spinal mobility at 8.9 points on the BASMI; those who exercised rated it 1.2 points lower (12% absolute improvement).
None of the studies measured fatigue.
Adverse effects (AE)
One of 67 participants in the exercise groups, and none of 43 participants in the control groups, experienced an AE.
Quality of the evidence
We downgraded the evidence due to issues with study design, variability between interventions, and not enough data, resulting in a rating of moderate to very low‐quality evidence across outcomes.
Summary of findings
Summary of findings for the main comparison. Exercise programmes compared to no intervention for ankylosing spondylitis.
| Exercise programmes compared to no intervention | ||||||
| Patient or population: adults with ankylosing spondylitis Setting: international hospitals, outpatient clinics, or home Intervention: exercise programmes Comparison: no intervention | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with no intervention | Risk with exercise programmes | |||||
|
Physical function
assessed with self‐report questionnaire BASFI scale (0 (easy) to 10 (impossible)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean physical function in the control groups was 4.1a | The mean physical function in the exercise groups was 1.3 lower (1.7 lower to 0.9 lower) | ‐ | 312 (7 RCTs) | ⊕⊕⊕⊝ MODERATEb | 13% absolute reduction (95% CI 17% to 9%) 32% relative change (95% CI 23% to 42%) NNTB 3 (2 to 4) |
|
Pain
assessed with VAS scale (0 (no pain) to 10 (impossible)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean pain in the control groups was 6.2a | The mean pain in the exercise groups was 2.1 lower (3.6 lower to 0.6 lower)c | ‐ | 288 (6 RCTs) | ⊕⊕⊝⊝ LOWb,d | MD ‐2.1 (95% CI ‐3.6 to ‐0.6) 21% absolute reduction (95% CI 36% to 6%) 34% relative change (95% CI 10% to 59%) NNTB = 3 (2 to 8) |
|
Patient global assessment of disease activity assessed with self‐report questionnaire BASDAI scale (0 (absent) to 10 (extreme)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean patient global assessment of disease activity in the control groups was 3.7e | The mean patient global assessment of disease activity in the exercise groups was 0.9 lower (1.3 lower to 0.5 lower) | ‐ | 262 (6 RCTs) | ⊕⊕⊕⊝ MODERATEb | 9% absolute reduction (95% CI 13% to 5%) 27% relative change (95% CI 15% to 39%) NNTB 4 (3 to 8) |
|
Spinal mobility
assessed with self‐report questionnaire BASMI scale (0 (better) to 10 (very severe limitation)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean spinal mobility in the control groups was 3.8e | The mean spinal mobility in the exercise groups was 0.7 lower (1.3 lower to 0.1 lower) | ‐ | 232 (5 RCTs) | ⊕⊝⊝⊝ VERY LOW b, d, f | 7% absolute reduction (95% CI 13% to 1%) 18% relative reduction (95% CI 34% to 3%) NNTB 5 (3 to 14) |
|
Fatigue
assessed with VAS scale (0 (absent) to 10 (extreme)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean fatigue in the control groups was 3e | The mean fatigue in the exercise groups was 1.4 lower (2.7 lower to 0.1 lower) | ‐ | 72 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW b,f,g | 14% absolute reduction (95% CI 27% to1%) 48% relative change (95% CI 5% to 91%) NNTB 3 (1 to 9) |
|
Adverse effects associated with exercises Exercise programme duration: range 3 to 24 weeks |
No adverse effects were reported in 43 control group participants | 1 adverse effect was reported in 67 exercise group participants | Peto OR 6.25 (0.10 to 320.40) | 110 (2 RCTs)j | ⊕⊝⊝⊝ VERY LOW g,h | 2% absolute increase (95% CI 5% less to 8% more) 152% relative change (95% CI 90% less to 5818% more) it was not possible to calculate NNTB as too few events were reported |
|
Withdrawals because of adverse events Exercise programme duration: range 3 to 24 weeks |
90 per 1000 | 96 per 1000 (68 to 134) | Peto OR 1.08 (0.74 to 1.57) | 1343 (8 RCTs) j | ⊕⊕⊝⊝ LOW b, i | 1% absolute increase (95% CI 2% less to 4% more) 7% relative change (95% CI 23% less to 48% more) NNTB was not applicable as results were not statistically significant |
| *The risk in the intervention groups (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; NNTB: number needed to treat (benefit); MD: mean difference; SMD: standardized mean difference; SD: standard deviation; BASFI: Bath Ankylosing Spondylitis Functional Index; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aSouza 2017 is the source document for the control group baseline data
b Downgraded one level due to risk of detection bias for subjective outcomes (lack of blinding of participants)
c We calculated a pooled SMD and re‐expressed it in MD, as the SMD multiplied by the control group baseline SD (SF‐36 pain = 2.5 from Souza 2017)
d Downgraded one level for inconsistency; important heterogeneity
eMasiero 2011 is the source document for the control group baseline data
f Downgraded one level for imprecision; total number of participants less than 400 and large confidence intervals
g Downgraded one level for imprecision; low rate of events
h Downgraded two levels for risk of bias; no blinding, incomplete outcome reporting
i Downgraded one level for indirectness. Since only two studies explicitly monitored adverse events, we used dropouts or withdrawals for any reason as a major outcome measure to estimate adverse events
i Studies were included regardless of the comparator intervention
Summary of findings 2. Exercise programmes compared to usual care for ankylosing spondylitis.
| Exercise programmes compared to usual care | ||||||
| Patient or population: adults with ankylosing spondylitis Setting: international hospitals, outpatient clinics, or home Intervention: exercise programmes Comparison: usual care (current practices included medication, self management, physiotherapy) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with usual care | Risk with exercise programmes | |||||
|
Physical function assessed with self‐report questionnaire BASFI scale (0 (easy) to 10 (impossible)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean physical function in the control groups was 3.7a | The mean physical function in the exercise groups was 0.4 lower (0.6 lower to 0.2 lower) | ‐ | 1068 (5 RCTs) | ⊕⊕⊕⊝ MODERATE b | 4% absolute reduction (95% CI 6% to 2%) 11% relative change (95% CI 5% to 16%) NNTB 10 (6 to 21) |
|
Pain assessed with VAS scale (0 (no pain) to 10 (impossible)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean pain in the control groups was 3.7a | The mean pain in the exercise groups was 0.5 lower (0.9 lower to 0.1 lower) c | ‐ | 911 (2 RCTs) | ⊕⊕⊕⊝ MODERATE b | MD ‐0.5 (95% CI ‐0.9 to ‐0.1) 5% absolute reduction (95% CI 9% to 1%) 15% relative change (95% CI 2% to 22%) NNTB = 10 (7 to 68) |
|
Patient global assessment of disease activity assessed with self‐report questionnaire BASDAI scale (0 (absent) to 10 (extreme)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean patient global assessment of disease activity in the control groups was 3.7a | The mean patient global assessment of disease activity in the exercise groups was 0.7 lower (1.3 lower to 0.1 lower) | ‐ | 1068 (5 RCTs) | ⊕⊕⊝⊝ LOW a,d | 7% absolute reduction (95% CI 13% to 1%) 19% relative change (95% CI 3% to 35%) NNTB 6 (3 to 52) |
|
Spinal mobility assessed with self‐report questionnaire BASMI scale (0 (better) to 10 (very severe limitation)), at the end of intervention Exercise programme duration: range 3 to 24 weeks |
The mean spinal mobility in the control groups was 8.9e | The mean spinal mobility in the exercise groups was 1.2 lower (2.8 lower to 0.5 higher) | ‐ | 85 (2 RCTs) | ⊕⊝⊝⊝
VERY LOW a,d, f |
12% absolute change (95% CI 5% less to 28% more) 13% relative change (95% CI 6% less to 32% more) NNTB = NA |
| Fatigue | see comment | ‐ | (0 RCTs) | ‐ | No included studies measured this outcome | |
|
Adverse effects associated with exercises Exercise programme duration: range 3 to 24 weeks |
No adverse effects were reported in 43 control group participants | 1 adverse effect was reported in 67 exercise group participants | Peto OR 6.25 (0.10 to 320.40) | 110 (2 RCTs) i | ⊕⊝⊝⊝ VERY LOWg, h | 2% absolute increase (95% CI 5% less to 8% more) 152% relative change (95% CI 90% less to 5818% more) it was not possible to calculate NNTB as too few events were reported |
|
Adverse events Exercise programme duration: range 3 to 24 weeks |
see comment | cannot be estimate | ⊕⊝⊝⊝ VERY LOWg,h | Adverse events could not be calculate as events were not monitored or reported | ||
| *The risk in the intervention groups (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; NNTB: number needed to treat (benefit); MD: mean difference; SMD: standardized mean difference; SD: standard deviation; BASFI: Bath Ankylosing Spondylitis Functionnal Index; VAS: visual analogic scale. | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aRodriguez‐Lozano 2013 is the source document for the control group baseline data.
b Downgraded one level due to risk of detection bias for subjective outcomes (lack of blinding of participants)
c We calculated a pooled SMD and re‐expressed it as a MD; we multiplied the SMD by the control group baseline SD (VAS pain = 3.0 from Rodriguez‐Lozano 2013)
d Downgraded one level for inconsistency; important heterogeneity
eAltan 2012 is the source document for the control group baseline data
f Downgraded one level for imprecision; total number of participants less than 400, and large confidence intervals
g Downgraded one level for imprecision; low rate of events
h Downgraded two levels for risk of bias; no blinding, incomplete outcome reporting
i Studies were included regardless of the comparator intervention
Background
Description of the condition
Ankylosing spondylitis (AS) is a chronic, inflammatory rheumatic disease that mainly affects the axial skeleton and sacroiliac joints, causing characteristic inflammatory back pain (Braun 2003; Braun 2010; van der Heijde 2008). The inflammatory back pain is due to sacroiliitis and spondylitis, and to the formation of syndesmophytes, leading to ankylosis of the spine (Baraliakos 2005). AS can start early, and often affects young adults. Men are more affected than women, with a ratio of 2:1 (Braun 2007). The disease affects about 0.1% to 1.4% of the population, depending on the geographical region (Boonen 2006), and is closely associated with positivity for human leukocyte antigen 27 (Dougados 2011). In a recent systematic review, the estimated AS prevalence was reported to be 18.6/10,000 in Europe, 18.0/10,000 in Asia, 12.2/10,000 in Latin America, 39.9/10,000 in North America, and 7.4/10,000 in Africa (Dean 2014). The number of AS cases is estimated to range from 1.30 million to 1.56 million in Europe and 4.63 million to 4.98 million in Asia. The incidence ranges from 0.5 to 14 per 100,000 people per year, depending on the country (Braun 2007).
The main clinical features of AS are back pain and reduced mobility, caused by inflammation in the axial skeleton spinal region. Approximately one‐third of individuals report peripheral joint involvement, most often of the hip, shoulder, and knee joints. AS may also be associated with extra‐articular manifestations, including enthesitis, anterior uveitis, inflammatory bowel disease, and inflammatory skin conditions (Braun 2007). Enthesitis (inflammation of the entheses, the sites at which tendons or ligaments insert into the bone) is typical of, and a key problem in, AS, and occurs at peripheral joints, generally the hip, shoulder, knee, or heel. AS may result in varying degrees of structural and functional impairments and reduced general health (Dagfinrud 2005). The severity of symptoms and radiographic progression of the disease vary considerably: longer disease duration, increasing age, and smoking are associated with decreased functioning (Boonen 2006). A cohort study found individuals with a high C‐reactive protein (CRP) level and syndesmophytes to be at risk for radiographic progression of the spine (Poddubnyy 2012), an indicator of disease severity (Pradeep 2008). However, the major sequela of AS is decreased quality of life. Like many chronic diseases, AS is associated with high medical and socioeconomic costs: in a systematic review, Palla 2012 estimated that AS represents a total cost of USD 31.766 per year for individuals with increased functional disability and severe disease. About 20% of individuals with AS experience disability at work (Reveille 2012). Boonen 2006 found that AS had considerable impact on healthcare costs and workforce participation.
In AS, treatments are expected to reduce the pain and stiffness of the back and sacroiliac joints, and improve spine and peripheral joint mobility (Boonen 2004). Current recommendations for the global management of AS combine appropriate medication and exercises as the two cornerstones of treatment (Braun 2010). Pharmacological therapies have greatly improved disease management (Vliet 2009). Biologic therapies have been efficacious and have changed the management landscape of AS and axial spondyloarthritis (SpA (Baraliakos 2012)), particularly with the introduction of anti‐tumour necrosis factor (TNF) agents (Vliet 2009). However, some individuals with AS (20% to 40%) do not respond well to pharmacological treatments (Dougados 2011). Whether these treatments can prevent structural change is unclear. Non‐steroidal anti‐inflammatory drugs (NSAIDs) seem to affect new bone formation, and some data suggest that they can positively affect the radiographic progression of axial SpA (Poddubnyy 2012). The benefits of biologic treatment on the structural progression of the disease are still debated (van der Heijde 2008). Recent data indicate that biologic therapy can slow the structural progression of AS (Haroon 2013).
Description of the intervention
Exercise programmes have been used to treat AS and remain a part of its management (Braun 2010). Up to 10% to 20% of individuals with AS receive physical therapy in the United States (Reveille 2012). According to the typical clinical features of AS, exercise programmes have focused on improving or maintaining spinal and thoracic mobility. Recently, studies have been designed to target other aspects of physical fitness, and to develop muscular strength and aerobic capacity (Giannotti 2014). A growing body of evidence suggests a dose–response relationship between exercise and health effects, as for drugs, so the effect of exercise depends on the individual's adherence to the prescribed programme (Arem 2015; Vidoni 2015).
How the intervention might work
Exercise programmes are associated with different hypothesised mechanisms of effect (Kujala 2009; Hagen 2012), and may benefit people with AS (Altan 2012). They may help avoid stiffness, and improve or maintain functional capacity by moving joints, especially during back stretching, posture control, muscle strengthening, pulmonary function, and cardiovascular fitness (Fernández‐de‐Las‐Peñas 2005; Niedermann 2013). Other benefits include improving quality of life and reducing pain (Singh 2013). Different exercise programmes are available (Van den Berg 2012). Some clinical trials have reported that the use of tai chi, global posture re‐education, exercises combined with spa treatments, or multimodal exercise programmes may be effective but the effect of different types of exercise programmes remains unclear (Wang 2009). The exercises are extremely heterogeneous: they can vary in dosage, type of exercise, components, modes, and settings (Slade 2016). The optimal mode of delivery, optimal frequency and duration of treatment, and in particular whether particular components of exercise modalities can improve the clinical outcome need to be explored. A Cochrane Review of 11 RCTs of individuals with AS concluded that exercises have a small but significant positive effect on pain, spinal mobility, physical function, and patient global assessment (Dagfinrud 2008).
Why it is important to do this review
Given the publication of new RCTs on exercise programmes in AS, a comprehensive systematic review is important to examine the evidence for exercise for people with AS.
Objectives
To assess the benefits and harms of exercise programmes on physical function, pain, fatigue, and global assessment of disease activity in people with ankylosing spondylitis.
Methods
Criteria for considering studies for this review
Types of studies
We included RCTs.
Types of participants
We included studies involving adults (18 years or older, with no upper age limit) with a diagnosis of ankylosing spondylitis (AS) according to the modified New York criteria (Van der Linden 1984), with critical features of visible structural damage on the sacroiliac joint on X‐rays.
We excluded individuals with non‐radiographic axial spondyloarthritis (SpA (Slobodin 2015)), as defined by the European Spondyloarthropathy Study Group and the Amor criteria, or the Assessment of Spondyloarthritis International Society (ASAS) criteria for axial SpA (Rudwaleit 2009; Van den Berg 2013).
We included studies with other populations only if we were able to extract data for the AS group separately.
Types of interventions
We defined exercise as 'a form of physical activity that is planned, structured and repeated over a period of time' (Bouchard 2012), with the intention of 'reducing pain and disability and improving overall health' (Abenhaim 2000; Hayden 2012).
We included interventions that delivered any type of exercise. The exercises could aim to improve any combination of stretching, flexibility, mobilising, balance, aerobic, strengthening, or functional training. We considered multimodal physical therapy interventions if one group of participants received exercise as part of a multimodal intervention and the comparison group received a non‐exercise intervention (attentional, control intervention), or no intervention.
We considered trials that included co‐interventions. We included trials that compared an exercise programme plus a co‐intervention versus the co‐intervention alone (e.g. exercise training plus a non‐steroidal anti‐inflammatory drug (NSAID) versus the NSAID alone). The only difference between groups was the exercise intervention.
We included exercise programmes carried out in any setting or location (home, inpatient clinic, hospital, or elsewhere), with any type of delivery (individual, group, or mixed); they could be land‐based or water‐based.
We included specific programmes, such as tai chi or yoga.
We considered any trial comparing exercise programmes with:
No exercise (attention, no treatment, waiting list control). Participants were asked not to practice exercises during the study period.
Usual care (participants could practice exercises as usual).
We excluded trials with general activities (e.g. swimming or walking) that required only movements, and did not meet our definition of exercise.
Types of outcome measures
We assessed a core set of outcome measures recommended by the ASAS (www.asas‐group.org; Sieper 2009; Van der Heijde 1997), and the 1999 conference on Outcome Measures for Rheumatoid Arthritis Clinical Trials (Van der Heijde 1999). We extracted all outcomes for analysis according to the following preferred hierarchy:
Major outcomes
Physical function
If data on more than one physical function scale were provided for a trial, we extracted data on the physical function scale that was highest on the following list:
Physical function (Bath Ankylosing Spondylitis Functional Index (BASFI))
Dougados Functional Index (DFI)
Health Assessment Questionnaire for AS (HAQ‐AS)
Pain
If data on more than one type of pain scale were provided for a trial, we extracted data on the type of pain scale that was highest on the following list, according to a previously described hierarchy of pain‐related outcomes (Sieper 2009).
In a visual analogue scale (VAS) or numerical rating scale (NRS):
Total back or spine pain (Bath Ankylosing Spondylitis Disease Activity Index (BASDAI))
Overall pain
Back or spine pain at night
Overall pain at night
Patient global assessment of disease activity
If data on more than one patient global assessment of disease activity scale were provided for a trial, we extracted data on the patient global assessment of disease activity scale that was highest on the following list:
BASDAI
Patient global VAS or NRS (global disease activity in the previous week)
Stiffness VAS or NRS (duration of morning stiffness, spine, last week
Spinal mobility
If data on more than one spinal mobility scale were provided for a trial, we extracted data on the spinal scale that was highest on the following list:
Schober test score
Lateral spinal flexion
Cervical rotation
Occiput to wall movement
Chest expansion
Bath Ankylosing Spondylitis Metrology Index (BASMI)
We considered including BASMI and other spinal scales as separate outcomes.
Fatigue
BASDAI fatigue question.
Safety
Withdrawals due to adverse events (AEs).
Severe AE outcomes: inpatient hospitalisation, life‐threatening events, or death
Adverse effects associated with the exercise intervention: we extracted the proportion of participants who experienced adverse effects related to exercise programmes (including joint or muscle contractures, fatigue, pain, falls, functional limitations)
Minor outcomes
Quality of life
Medical Outcomes Survey Short Form‐36 (SF‐36)
Ankylosing Spondylitis Quality of Life Instrument (ASQoL)
EuroQol (EQ‐5D)
Acute‐phase reactant
C‐reactive protein (CRP) level (mg/L) or erythrocyte sedimentation rate (ESR)
Physician global assessment
Peripheral joints, entheses (pain, swelling, and tenderness)
Number of swollen joints (44‐joint count (Braun 2007))
Validated enthesitis score, such as the Maastricht Ankylosing Spondylitis Enthesis Score (MASES), the University of California, San Francisco Index, and the Berlin Index
Timing of outcome assessment
We extracted outcome measures at the following three times points:
end of intervention – measured immediately after completion of the exercise programme
medium‐term follow‐up – < 24 weeks after completion of the exercise programme
long‐term follow‐up – ≥ 24 weeks after completion of exercise
Search methods for identification of studies
Electronic searches
We searched the following electronic databases for primary studies, from database inception up to the search date. The last search was in 14 December 2018:
the Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 12) in the Cochrane Library (searched 14 December 2018);
MEDLINE Ovid (1946 to 14 December 2018);
Embase Ovid (1974 to 14 December 2018);
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature; 1982 to 14 December 2018);
PEDro (www.pedro.org.au/; searched 14 December 2018);
Scopus (searched 14 December 2018).
We searched the Cochrane Database of Systematic Reviews (14 December 2018) and the Database of Abstracts of Reviews of Effect (up to 14 December 2018) to identify relevant systematic reviews.
The queries combined free text words and controlled vocabulary. The search strategy was based on synonyms of (“exercise”) AND “spondyloarthritis”. The Cochrane Musculoskeletal Review Group's Information Specialist helped to develop each search strategy.
The electronic search strategy for MEDLINE is outlined in Appendix 1. We adapted this search strategy for use with other databases. We used the 'optimal sensitive search strategies' designed to identify clinical trials, described by Lefebvre 2011.
We did not restrict the search by language of publication or publication status.
Searching other resources
We hand‐searched the reference lists of selected trials and systematic reviews identified from electronic searches, and also searched in Google and Google Scholar.
We searched the proceedings of the conferences of the American College of Rheumatology (on July 2013, November 2014) , European League Against Rheumatism (EULAR) (October 2013; November 2014), and Osteoarthritis Research Society International (on April 2013, April 2014) available online, and contacted authors and field experts for any additional published or unpublished data.
We searched the US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched December 2018) and the World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch/; searched December 2018) to identify any studies in progress.
We present a flow diagram of search results and selection of studies in Figure 1.
1.

Study flow diagram. Search results from original June 2015 literature search, and May 2016 and January 2017 updates
Data collection and analysis
Selection of studies
We removed duplicate records from the references identified. Two review authors (JPR, TD) independently reviewed the titles and abstracts of citations identified from the search strategy to select potentially relevant studies. Then, we obtained the full text of all potentially eligible studies and screened them for inclusion, according to the eligibility criteria. We resolved disagreements by reaching a consensus, or by consulting a third review author (MMLC) if necessary. We linked multiple reports relating to the same trial, or to trials with potentially overlapping populations. If the possibility of overlapping populations could not be excluded, we selected the most recent trial.
Data extraction and management
Two review authors (TD, JPR, or MMLC) independently extracted the results of individual trials by using a standardised, piloted extraction form, accompanied by a codebook. Disagreements were resolved by reaching consensus, or by consulting a third review author if necessary. The extraction form, based on other forms used by the Cochrane Musculoskeletal Review Group, was pilot tested with five reports of RCTs.
We extracted the following information:
Trial characteristics (funding, settings and number of centres, country, study design);
Participant characteristics (age, sex, measure of functional status, level of pain, description of radiographic damage, biologic medications, NSAIDs, corticosteroids or other drugs, coexisting diseases, other);
-
Intervention characteristics:
number of intervention groups;
content and type of each intervention (details);
qualitative data: a detailed description of the interventions, including the different components of the programme received by each group, mode of delivery (individual, group, over internet), with or without supervision (face‐to‐face or at home), clinical expertise and background of the healthcare professionals who provided the exercise programmes (physiotherapist, fitness instructor, registered nurse, other), and adherence. We followed the reporting of Saunders 2016 to evaluate adherence by including: (1) attendance at the exercise programme sessions, and (2) compliance with the protocol or exercise instructions during the training sessions.
quantitative data: the number of sessions, timing and duration of each session, duration of each component, and overall duration intensity. We collected these data as more frequent interventions, conducted over a long time, may influence outcomes.
Outcomes reported, including individual effect measures used (continuous or dichotomous data) and timing of outcome measurement.
AEs: we reported any AEs and/ or adverse effects related to the interventions in each group.
Economic data: we summarised economic evaluations in additional tables when available.
When necessary, we used PlotDigitizer to approximate data from graphs (arohatgi.info/WebPlotDigitizer/index.html). We entered the data into Review Manager 5 (RevMan 2014), and checked for accuracy.
Assessment of risk of bias in included studies
We evaluated the risk of bias in each included study according to Cochrane's 'Risk of bias' tool (Higgins 2011a). Two review authors (TD, JPR, or MMLC) independently examined seven specific domains: sequence generation, allocation concealment, blinding of participants, blinding of personnel who delivered exercise programmes, blinding of outcome assessors, incomplete outcome data, and selective outcome, plus other potential sources of bias (i.e. imbalanced baseline characteristics, small study participants, lack of power calculation, no assessments of attendance).
We separately assessed the blinding of self‐reported subjective outcomes (e.g. pain, function, health‐related quality of life) and the blinding of independent outcome assessors to objective outcomes (such as AEs).
Studies were classified at low risk of bias if all domains were assessed at low risk for potential bias; high risk of bias if one or more categories was assessed at high risk of bias; and unclear risk of bias if one or more key domains was assessed at unclear risk of bias. We resolved disagreements by discussion, or by consulting a third review author if necessary.
Measures of treatment effect
We calculated point estimates and 95% confidence intervals (CIs) for outcomes of individual RCTs whenever possible.
We summarised the intervention effect estimates in a meta‐analysis only when estimates displayed sufficient clinical and statistical homogeneity. The estimate of the common treatment effect was the weighted average of the individual estimates for each study.
If the meta‐analysis resulted in statistically significant overall estimates, we transformed these treatment effect measures (pooled estimate of the relative risk or SMD) into measures that are clinically useful in daily practice, such as number needed to treat for an additional beneficial outcome (NNTB), or number needed to treat for an additional harmful outcome (NNTH), and the absolute or relative improvement in the original units. We calculated the absolute risk difference and relative percentage change by using the recommendations provided by the Musculoskeletal Review Group (musculoskeletal.cochrane.org).
We assumed a minimal clinically important difference (MCID) of 1.5 on a 10‐cm scale for pain, patient global assessment of disease activity, physical function, or physician global assessment. We defined an important clinical benefit as an outcome improvement that was more than 15% for an absolute change, and more than 20% for a relative change (Tubach 2012). We did not consider outcome changes that were below these values to be clinically important.
For dichotomous data
We analysed AEs by using Peto odds ratios (Peto ORs).
For dichotomous outcomes, we calculated the NNTB or NNTH from the control group event rate (unless the population event rate was known) and the relative risk, by using the Visual Rx NNT calculator (Cates 2008). We used the baseline values observed in the comparator group in the trials.
For continuous data
We summarised results, such as mean differences (MD), if the same tool was used to measure the same outcome across studies. We calculated the standardised MD (SMD) when the same outcome was measured with different units and methods of assessment across studies (e.g. pain scales). SMDs are calculated by dividing the MD by the standard deviation (SD); we calculated 95% CIs.
To enhance interpretability of continuous outcomes, we back‐transformed pooled SMDs for overall pain and disability to an original 0 to 10 VAS for pain. When the direction of a scale (i.e. SF‐36, 100 representing more favourable state of health) differed from the VAS for pain (10 defining high pain), we subtracted the mean from the maximum possible value for the scale, following the procedure recommended by Cochrane, and described in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011).
For continuous outcomes, we calculated the absolute risk difference as the mean difference between intervention and control groups in the original measurement units (divided by the scale), expressed as a percentage; the relative difference was calculated as the absolute change (or MD) divided by the baseline mean of the control group obtained from a representative trial, or the pooled baseline mean calculated in RevMan 5 by using the generic inverse variance method (Buchbinder 2015). We re‐expressed outcomes pooled using SMDs as changes by multiplying by a representative control group baseline SD. We calculated the NNTB by using the Wells calculator software available at the Cochrane Musculoskeletal Review Group editorial office.
If we could not summarise results as described above, we reported them as 'other data' in narrative form, but did not include them in the meta‐analysis (Deeks 2011).
Unit of analysis issues
For studies containing more than two intervention groups, we combined groups to create a single pair‐wise comparison following the procedure recommended by Cochrane (Higgins 2011b).
Dealing with missing data
We contacted the original investigators to request any missing outcome data. If we did not receive a response, we sent two e‐mail reminders, with two‐week intervals.
For continuous outcomes with no SD reported, we calculated SDs from standard errors (SEs), 95% CIs, or P values (Higgins 2011c).
Assessment of heterogeneity
As recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2019, ch10.10), we assessed the presence of heterogeneity. We used the I² statistic: the percentage of the variability in effect estimates that is due to heterogeneity rather than sampling error (Higgins 2011a). We interpreted the value of the I² statistic according to the following thresholds:
0% to 40%: might not be important
30% to 60%: may represent moderate heterogeneity
50% to 90%: substantial heterogeneity
75% to 100%: considerable heterogeneity (Deeks 2011).
We also computed the 95% CI for the I² statistic (Ioannidis 2007a), and the between‐study variance Tau², estimated from the random‐effects model (Rucker 2008). .
When we found substantial to considerable heterogeneity (severe heterogeneity), we checked the extracted data and insured that the numbers were correctly entered in the analysis software. When the number of trials was sufficient, we discussed the potential sources of heterogeneity by identifying a study that could be responsible of the presence of heterogeneity. As it is recommended, we did not exclude any study from the meta‐analyses unless it can be considered as an outlier for an obvious reason (ie conflicting data). We also used the random‐effects model with the DerSimonian and Laird approach to take into account the clinical differences between the studies included (Deeks 2011, Deeks 2019).
Assessment of reporting biases
To assess the presence of small study effects, we had planned to visually inspected funnel plots for each meta‐analysis when the required statistical conditions were met (≥ 10 studies, no significant heterogeneity, and a ratio of the maximal to minimal variance across studies > 4).
Data synthesis
We performed a meta‐analysis if the data from the studies were sufficiently clinically and statistically homogeneous. Because of large clinical heterogeneity between exercise programmes, participants, and characteristics, we used the random‐model effects for all meta‐analyses . We analysed and presented data separately by common control group intervention: exercise programmes versus no intervention, and exercise programmes versus usual care.
We analysed data at study completion, medium‐term follow‐up (< 24 weeks after study completion), and long‐term follow‐up (> 24 weeks after study completion).
In this review, we included studies with different characteristics, used different types of interventions, and reported effects on different outcomes measures. For a better description and standardisation, we presented a synthesis of these different characteristics in additional tables. We systematically described the key exercise programme components, according to the items recently proposed by Slade 2016 in the 'Characteristics of included studies' tables.
Subgroup analysis and investigation of heterogeneity
We planned to separate the data analysis on the basis of the control group intervention. We did not perform the other planned subgroup analyses (see the "Differences between protocol and review" section) because of the small number of studies in each group.
Sensitivity analysis
We did not perform any sensitivity analyses (see the "Differences between protocol and review" section).
'Summary of findings' tables
We included 'Summary of findings' tables to provide key information concerning the quality of evidence, the magnitude of effect of the interventions examined, and the sum of available data on the main outcomes, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2011a). We assessed the overall quality of the evidence for each main outcome by using the GRADE approach (Schünemann 2011b).
We developed 'Summary of findings' tables using GRADEpro GDT (GRADEpro GDT).
For the 'Summary of findings' tables, we included the following outcomes for each main comparison:
Physical function
Pain
Patient global assessment of disease activity
Spinal mobility
Fatigue
Adverse effects associated with exercise
Adverse events
Results
Description of studies
Results of the search
January 2015: we identified 806 citations after removing duplicates, and excluded 745 studies after screening titles and abstracts. In total, we selected 64 full‐text reports for evaluation. After assessing all records, we included 11 unique studies. Among the 64 full‐text reports, we contacted 18 authors (see Table 3): nine responded, and we obtained data for one study (Dönmez 2014). We identified two congress reports, but had insufficient information to include or extract the data, so we listed one study in the Characteristics of studies awaiting classification section. In addition, we identified four ongoing trials (Gallinaro 2016; Souza 2017; ChiCTR‐TRC‐14004650; NCT02098694). See Characteristics of ongoing studies.
1. Authors contacted for missing or additional data.
| Authors | First contact | Second contact | Response |
| Altan 2012 | 25/05/2015 | ‐ | 28/05/2015 |
| Colina 2009 | 04/05/2015 | 13/05/2015 | no e‐mail response |
| Durmus 2009 | 15/04/2015 | 04/05/2015 | no e‐mail response |
| Dönmez 2014 | 15/04/2015 | ‐ | 18/04/2015 |
| Gunay 2012 | 15/04/2015 | 04/05/2015 | no e‐mail response |
| Ince 2006 | 02/06/2015 | ‐ | 05/06/2015 |
| Kjeken 2013 | 02/06/2015 | ‐ | 03/06/2015 |
| Kraag 1990 | 02/06/2015 | ‐ | 03/06/2015 |
| Lim 2005 | no available contact | ‐ | no e‐mail response |
| Masiero 2011 | 20/04/2015 | 04/05/2015 | 04/05/2015 |
| Masiero 2015 | 16/06/2016 | ‐ | 20/06/2016 |
| Mesquita 2014 | 15/04/2015 | 04/05/2015 | no e‐mail response |
| Rodriguez‐Lozano 2013 | 02/06/2015 | ‐ | 03/06/2015 |
| Sveaas 2014 | 02/06/2015 | ‐ | 04/06/2015 |
| Sveeas 2018 | 24/01/2018 | no e‐mail response | |
| Sweeney 2002 | 19/05/2015 | 02/06/2015 | no e‐mail response |
| Widberg 2009 | 02/06/2015 | ‐ | 06/06/2015 |
Updated search in May 2016: we searched the listed electronic databases for reports of randomised controlled trials (RCT) published from January 2015 to May 2016. The search resulted in 75 records to screen. We assessed two full‐text records to determine their eligibility. We included one new study (Garcia 2015).
Updated search in January 2017: we searched the listed electronic databases for RCT reports published from May 2016 to 31 January 2017. The search identified 51 records. We included two new studies identified in a previous search as ongoing trials (Gallinaro 2016; Souza 2017). Souza 2017 had published their data in a scientific journal, and Gallinaro 2016 had limited data published on ClinicalTrials.gov, and additional data on a thesis online website (www.teses.usp.br/teses/disponiveis/5/5169/tde‐04112016‐150051/fr.php).
A flow chart shows the overall search process in Figure 1.
We performed a further search in December 2018. We added those results to Characteristics of studies awaiting classification, and will incorporate them into the review at the next update.
Included studies
We provided a full description of each included study in the 'Characteristics of included studies' table. We also provided a descriptive summary of the information on trials, participants, and exercise programmes in additional tables (Table 4; Table 5; Table 6).
2. Summary of characteristics of included studies (N = 14).
| Characteristics | N (%) or median (IQR) |
|
Location Brazil Canada Italy Korea Norway Spain Sweden Turkey UK |
2 (14%) 1 (7%) 1 (7%) 1 (7%) 2 (14%) 2 (14%) 1 (7%) 3 (21%) 1 (7%) |
|
Study design RCT |
14 (100%) |
|
Number of study arms 2 3 |
11 (79%) 3 (21%) |
|
Type of comparator Usual care No treatment |
5 (36%) 9 (64%) |
| Total number participants per study | 55 (35 to 73) |
|
Trial size > 100 subjects/arm ≤ 100 subjects/arm |
3 (21) 11 (79) |
| Number subjects per arm | 26 (15 to 29) |
| Study duration (weeks) | 14 (range 12 to 24) |
N (%) is the number of studies that reported the characteristic of interest
3. Summary of characteristics of participants in included studies (N = 14).
| Characteristics | N (%) or median (IQR) |
| Age (years) | 45 (39 to 47) |
|
Gender Male Female |
70 (56 to 77) 33 (25 to 45) |
|
Diagnostic criteria* Modified New York The Ankylosing Spondylitis Disease Activity Score European spondyloarthropathy not reported |
10 (71%) 2 (14%) 1 (7%) 2 (14%) |
|
Severity disease* Bath Ankylosing Spondylitis Disease Activity Index ≥ 3.5 Bath Ankylosing Spondylitis Disease Activity Index < 3.5 Ankylosing Spondylitis stage1 or 2 no information |
5 (36%) 2 (14%) 4 (29%) 3 (21%) |
| Disease duration (years) | 9 (9 to 18) |
|
coexisting medical treatments Analgesics (in 2 studies) Anti‐Tumour Necrosis Factor (in 7 studies) Disease Modifying Anti‐Rheumatic Drug (in 5 studies) Nonsteroidal anti‐inflammatory drugs (in 9 studies) Sulfasalazine (in 4 studies) No treatment (in 2 studies) No information reported (in 4 studies) |
21% (16% to 26%) 29% (14% to 38%) 17% (11% to 19%) 75% (32% to 76%) 22% (11% to 49%) 17% (10% to 15%) NA |
* N (%) is the number of studies that reported the characteristic of interest
4. Summary of exercise programme characteristics in the included studies (N = 14).
| Characteristics | N (%) or median (IQR) |
|
Modalities Monomodal Multidisciplinary |
9 (64%) 5 (36%) |
|
Exercise components Pain relief Breathing Cardio fitness Flexibility, stretching Endurance Motion (active or passive) Proprioception, posture Relaxation Strength no information |
1 (7%) 7 (50%) 2 (14%) 8 (57%) 1 (7%) 5 (36%) 4 (29%) 2 (14%) 9 (64%) 1 (7%) |
|
Provider Physiotherapist Other trainer Self delivery Unclear |
7 (50%) 3 (21%) 2 (14%) 2 (14%) |
|
Supervision With supervision No supervision Unclear |
8 (50%) 3 (21%) 3 (21%) |
|
Dose Session duration (minutes) Frequency (session/week) programme duration (weeks) |
60 (50 to 60) 3 (2 to 3) 12 (8 to 16) |
N (%) is the number of studies that reported the characteristics of interest
We included a total of 14 reports of RCTs. Reports were published between 1990 and 2017. Three trials were conducted in Turkey (Altan 2012; Dönmez 2014; Ince 2006), two in Spain (Garcia 2015; Rodriguez‐Lozano 2013), two in Norway (Kjeken 2013; Sveaas 2014), two in Brazil (Gallinaro 2016; Souza 2017), and one in Canada (Kraag 1990), South Korea (Lim 2005), Italy (Masiero 2011), United Kingdom (Sweeney 2002), and Sweden (Widberg 2009).
Design
All included studies were RCTs, with a parallel‐group design. There were no cross‐over trials. Eleven studies included two groups, and three included three groups (Dönmez 2014; Gallinaro 2016; Masiero 2011). Most studies (N = 11, 79%) included fewer than 100 participants per group. The median number of participants per group was 26 (interquartile range (IQR): 15 to 29). All studies reported final values or pre–post differences for the exercise and control groups. We calculated individual study effects from means and standard deviations (SD). In one study, Masiero 2011 reported medians and IQRs. We used the formulas described by Hozo 2005 to estimate the mean and SD.
Participants
Participiants were recruited from hospital departments (Gallinaro 2016; Ince 2006; Kjeken 2013; Lim 2005; Masiero 2011; Rodriguez‐Lozano 2013; Souza 2017; Sveaas 2014; Sweeney 2002; Widberg 2009), clinics (Altan 2012), and arthritis patient associations (Garcia 2015; Kraag 1990; Sweeney 2002); the source was unclear in Dönmez 2014.
The 14 studies included a total of 1579 participants. The median sample size was 55 (range 35 to 73). The median age was 45 years (range 39 years to 47 years). Most participants were male (median 70% men). The modified New York criteria for ankylosing spondylitis (AS) diagnosis were most frequently used (71%). The median disease duration was nine years from diagnosis (range 9 years to 18 years). Many participants received non‐steroidal anti‐inflammatory drugs (NSAID (75%)); others received tumour necrosis factor (TNF) blockers (29%), or sulphasalazine (22%).
Interventions and comparators
Descriptions are provided in Table 6 and the 'Characteristics of included studies' tables.
The median exercise programme duration was 12 weeks (IQR 8 weeks to 16 weeks), with a median of three sessions (range two to seven) per week, and a median duration of 60 minutes per session (IQR 50minutes to 60 minutes). The description of dose components of exercise programmes was limited in three studies, in which exercise programmes were practiced at home (Kraag 1990; Lim 2005; Sweeney 2002). Intensity was variable and incompletely reported across studies.
Exercise programmes
For the 14 included studies, nine (64%) investigated exercise programmes alone in the experimental group (monomodal), and five (36%) combined exercise programmes with other interventions (education, self‐management). The exercise programmes included a variety of components. The most commonly used components were strengthening exercises (64%), flexibility or stretching exercises (57%), and breathing exercises (50%). Most of the studies were land‐based (11 studies). Two studies included an aquatic component in their exercise programmes (Garcia 2015; Kjeken 2013). One study was conducted only in water (Garcia 2015).
Exercise programmes were performed under the supervision of a therapist in nine studies (Altan 2012; Dönmez 2014; Gallinaro 2016; Garcia 2015; Ince 2006; Kraag 1990; Souza 2017; Sveaas 2014; Widberg 2009). Two studies instructed participants to undertake unsupervised exercise at home (Lim 2005; Sweeney 2002); three did not clearly report exercise supervision (Kjeken 2013; Masiero 2011; Rodriguez‐Lozano 2013).
Nine studies reported the setting of the intervention. Six studies delivered exercise programmes in facilities (Garcia 2015; Ince 2006; Sveaas 2014; Widberg 2009), or combined them with home delivery (Masiero 2011; Rodriguez‐Lozano 2013). Three studies were performed at participants' homes (Kraag 1990; Lim 2005; Sweeney 2002); five did not clearly mention where the exercise programmes were performed (Altan 2012; Dönmez 2014; Gallinaro 2016; Kjeken 2013; Souza 2017).
Control group interventions
Five included studies (36%) compared an exercise programme to usual care (Altan 2012; Kjeken 2013; Rodriguez‐Lozano 2013; Sweeney 2002; Widberg 2009). Nine studies (64%) compared an exercise programme to no intervention (Dönmez 2014; Gallinaro 2016; Garcia 2015; Ince 2006; Kraag 1990; Lim 2005; Masiero 2011; Souza 2017; Sveaas 2014). For two of the nine studies, the description of the control intervention was unclear, and we had to contact the trial authors for additional information (Dönmez 2014; Ince 2006; Table 3). Based on the response from the two trial authors, we classified the control intervention as 'no intervention'.
Adherence to exercise programmes
We were unable to analyse the attendance, since attendance or compliance was not clearly reported in most of the included studies.
Compliance: only four studies reported information, and reported that compliance was high. No data were provided (Altan 2012; Masiero 2011; Rodriguez‐Lozano 2013; Widberg 2009).
Two studies reported on attendance. Participants participated in at least 80% of the sessions in Sveaas 2014, and less than 50% of the exercise programmes in Gallinaro 2016.
Outcomes
The outcomes measured in each trial are summarised in Table 7, Table 8 and Table 9. For all 14 studies, the end of the intervention was considered the final data collection point (range 3 to 24 weeks).
5. Major outcomes reported in the 14 included studies (part 1).
| Study | Physical function (BASFI) | Patient global assessment (BASDAI) | Mobility (BASMI) | Mobility (chest expansion) | Mobility (occiput to wall distance) | Mobility ( Schober test) | Mobility (Fingertip to floor) | Mobility (Cervical Rotation) |
| Altan 2012 | Yes | Yes | Yes | Yes | ‐ | ‐ | ‐ | ‐ |
| Dönmez 2014 | Yes | Yes | Yes | ‐ | ‐ | ‐ | ‐ | ‐ |
| Garcia 2015 | Yes† | Yes† | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Gallinaro 2016 | Yes †† | Yes †† | Yes †† | Yes †† | Yes †† | Yes †† | Yes | |
| Ince 2006 | ‐ | ‐ | ‐ | Yes | Yes | Yes (modified) | Yes | ‐ |
| Kjeken 2013 | Yes | Yes | Yes* | ‐ | ‐ | ‐ | ‐ | |
| Kraag 1990 | ‐ | ‐ | ‐ | ‐ | Yes | Yes | Yes | ‐ |
| Lim 2005 | Yes | ‐ | ‐ | ‐ | ‐ | ‐ | Yes | ‐ |
| Masiero 2011 | Yes | Yes | Yes | Yes | ‐ | ‐ | ‐ | Yes |
| Rodriguez‐Lozano 2013 | Yes | Yes | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Souza 2017 | Yes | Yes | Yes | Yes | ‐ | ‐ | ‐ | ‐ |
| Sveaas 2014 | Yes | Yes | Yes | ‐ | ‐ | ‐ | ‐ | ‐ |
| Sweeney 2002 | Yes | Yes | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Widberg 2009 | Yes | Yes | Yes | Yes | ‐ | ‐ | ‐ | ‐ |
* Data are missing. cannot be included in the analysis
† median and 25th to 75th percentile reported
†† multiple exercise groups combined
BASFI: Bath Ankylosing Spondylitis Functionnal Index
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index
BASMI: Bath Ankylosing Spondylitis Metrology Index
6. Major outcomes reported in the 14 included studies (part 2).
| Study | Pain (VAS) | Pain(SF‐36) | Pain (BASDAI) |
Pain (Nocturnal pain) |
Pain (Self efficacy scale Pain) |
Fatigue (Basdai) |
Adverse Effects associated with exercise |
| Altan 2012 | ‐ | ‐ | ‐ | ‐ | ‐ | Yes | |
| Dönmez 2014 | Yes† | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Garcia 2015 | ‐ | ‐ | Yes | ‐ | ‐ | Yes | ‐ |
| Gallinaro 2016 | Yes †† | ‐ | ‐ | ‐ | ‐ | ‐ | Yes †† |
| Ince 2006 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Kjeken 2013 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Kraag 1990 | Yes | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Lim 2005 | Yes | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Masiero 2011 | Yes** | ‐ | ‐ | ‐ | ‐ | Yes | ‐ |
| Rodriguez‐Lozano 2013 | Yes | ‐ | ‐ | Yes | ‐ | ‐ | ‐ |
| Souza 2017 | ‐ | Yes | ‐ | ‐ | ‐ | ‐ | ‐ |
| Sveaas 2014 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Sweeney 2002 | ‐ | ‐ | ‐ | ‐ | Yes | ‐ | ‐ |
| Widberg 2009 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
** mean score calculated from lumbar and cervical pain
† median and 25th to 75th percentile reported
†† multiple exercise groups combined
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index
VAS: visual analogue scale
SF‐36: 36‐Item Short‐Form Health Survey
7. Minor outcomes reported in the 14 included studies.
| Study | Quality of life (ASQoL) | Quality of life (SF‐36) |
Quality of life (SF‐12) physical component |
CRP level (mg/dL) |
ESR (mm/h) |
MASES |
| Altan 2012 | Yes | ‐ | ‐ | ‐ | ‐ | ‐ |
| Dönmez 2014 | ‐ | Yes* | ‐ | ‐ | ‐ | ‐ |
| Garcia 2015 | ‐ | ‐ | Yes† | ‐ | ‐ | ‐ |
| Gallinaro 2016 | ‐ | ‐ | Yes †† | ‐ | ‐ | Yes †† |
| Ince 2006 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Kjeken 2013 | ‐ | Yes* | ‐ | ‐ | ‐ | ‐ |
| Kraag 1990 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Lim 2005 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Masiero 2011 | ‐ | ‐ | ‐ | not reported | not reported | ‐ |
| Rodriguez‐Lozano 2013 | Yes | ‐ | ‐ | ‐ | ‐ | ‐ |
| Souza 2017 | ‐ | Yes* | ‐ | Yes | Yes | ‐ |
| Sveaas 2014 | ‐ | ‐ | ‐ | Yes | Yes | ‐ |
| Sweeney 2002 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Widberg 2009 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
* global score was not reported; could not be included in the analysis
† median and 25th to 75th percentile reported
†† multiple exercise groups combined
ASQoL: the Ankylosing Spondylitis Quality of Life
SF‐36: 36‐Item Short‐Form Health Survey
SF‐12: 12‐Item Short Form Health Survey
CRP: C‐reactive protein
ESR: erythrocyte sedimentation rate
MASES: Maastricht Ankylosing SpondylitisEnthesitis Score
Major Outcomes
Among the main outcomes (Table 7, Table 8), most trials included a measure of physical function (Bath Ankylosing Spondylitis Functional Index (BASFI), N = 12), and global patient assessment of disease activity (Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), N = 11); fewer included measures of overall pain (N = 9), fatigue (N = 2), or adverse effects (N = 2). For spinal mobility, the Bath Ankylosing Spondylitis Metrology Index (BASMI) was the most commonly reported (N = 8), but other descriptors were also reported (chest expansion N = 6; distance occiput to wall distance N = 2; distance finger to floor N = 4; or the Schober test N = 3). No study explicitly reported adverse events. Only two studies monitored and reported adverse effects associated with the exercise intervention.
Minor outcomes
Quality of life was reported for five studies (Table 9): two studies used the Ankylosing Spondylitis Quality of Life (ASQoL) scale (Altan 2012; Rodriguez‐Lozano 2013), three used the SF‐36 (Dönmez 2014; Kjeken 2013; Souza 2017), and one used the SF‐12 (Garcia 2015). Only Sveaas 2014 and Souza 2017 reported C‐reactive protein (CRP) levels and erythrocyte sedimentation rates (ESR). No study reported peripheral joint modification scales.
Follow‐up
Three studies reported data at medium‐term follow‐up, from 12 to 24 weeks (Altan 2012; Dönmez 2014; Masiero 2011). The mean duration follow‐up period was 18 weeks. One study reported a 48‐week long‐term follow‐up (Kjeken 2013). We contacted 10 trial authors requesting missing data for unreported or partially reported outcomes (Table 3).
Excluded studies
We excluded 54 studies at full‐paper review, as described in (Figure 1). We excluded eight studies (Characteristics of excluded studies: ; Ciprian 2013; Colina 2009; Durmus 2009; Gunay 2012; Karahan 2016; Kraag 1990, Lee 2008; Masiero 2015); five were controlled but not randomised trials (Colina 2009; Durmus 2009; Gunay 2012, Lee 2008; Masiero 2015), one study was a duplicate of an included study (Kraag 1990); The intervention was irrelevant in two studies (Ciprian 2013; Karahan 2016).
Ongoing studies
See Characteristics of ongoing studies.
We identified two ongoing studies registered in the WHO ICTRP as potentially eligible, but results were not available. The two studies compared exercise programmes in Norway (NCT02098694), and China (ChiCTR‐TRC‐14004650).
Awaiting Studies
See Characteristics of studies awaiting classification.
We identified one study as potentially eligible after we read the abstract, but we could not access the full‐text article (Mesquita 2014). We tried to contact the trial authors for additional information, but received no response (Table 3).
We added one study report from our updated January 2018 search (Sveeas 2018), as we were unable to determine if the results of this study were new, or if it was a secondary analysis from the previous study (Sveaas 2014). We attempted to contact the authors, but received no response.
Risk of bias in included studies
The overall risk of bias assessment of the included studies is presented in Figure 2.
2.
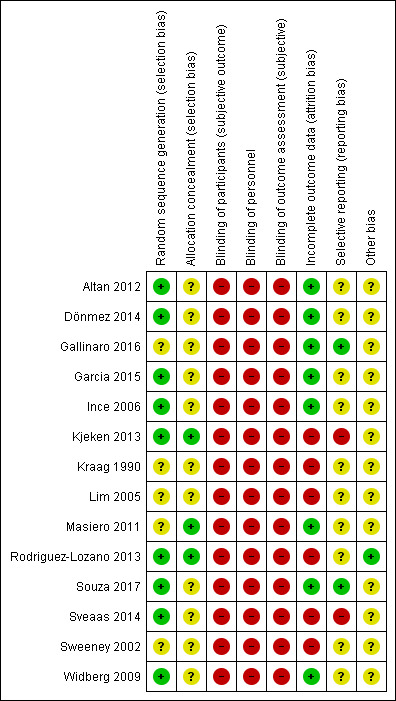
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study
Allocation
Random sequence
We judged nine studies (64%) at low risk of bias, because they used and reported an appropriate method of randomisation (Altan 2012; Dönmez 2014; Garcia 2015; Ince 2006; Kjeken 2013; Rodriguez‐Lozano 2013; Souza 2017; Sveaas 2014; Widberg 2009).
We assessed five trials (36%) at unclear risk of bias because the methods used to generate allocation sequence were not described, or were unclear (Gallinaro 2016; Kraag 1990; Lim 2005; Masiero 2011; Sweeney 2002).
Allocation concealment
We judged three studies (21%) at low risk of bias, since they provided adequate information on the method of allocation concealment (Kjeken 2013; Masiero 2011; Rodriguez‐Lozano 2013).
For 11 studies (79%), the method used to conceal allocation sequence was unclear, or not described (Altan 2012; Dönmez 2014; Gallinaro 2016; Garcia 2015; Ince 2006; Kraag 1990; Lim 2005; Souza 2017; Sveaas 2014; Sweeney 2002; Widberg 2009).
Blinding
Participant and care provider blinding
We judged all studies at high risk of bias.
Blinding participants and care providers is difficult because of the nature of the intervention. Most of the included studies did not report information on blinding, or a masking procedure for treatment allocation or delivery. No studies reported using a blinding procedure (sham or attentional comparator, or blinding of study hypothesis (Boutron 2007)).
Outcome assessor
We judged all studies at high risk of bias. Most included studies used subjective outcomes (self‐reporting, self‐performance). Because participants were not blinded to treatment allocation, we considered the outcome assessors to be unblinded.
For studies that reported spinal mobility outcome, we considered them to be at unclear risk of bias, because it was impossible to evaluate whether assessors were blinded to treatment allocation (Gallinaro 2016; Ince 2006; Kraag 1990).
Incomplete outcome data
Eight studies (57%) reported no withdrawals, and drop‐out rates were less than 20% at study completion (Altan 2012; Dönmez 2014; Gallinaro 2016; Garcia 2015; Ince 2006; Masiero 2011; Souza 2017; Widberg 2009). We judged these studies at low risk of bias.
Five studies (36%) reported higher rates (Kjeken 2013; Lim 2005; Rodriguez‐Lozano 2013; Sveaas 2014; Sweeney 2002), and one trial reported an unbalanced rate between groups (Kraag 1990). Consequently, we judged these studies at high risk of bias. Only one study used an intention‐to‐treat approach for analysis (Souza 2017).
Selective reporting
Three studies (21%) had a registered protocol (Gallinaro 2016; Souza 2017; Sveaas 2014). We assessed two of them (14%) at low risk of reporting bias, because all outcomes reported were pre‐specified in the protocol (Gallinaro 2016; Souza 2017).
We judged two studies (14%) at high risk of bias, because we found outcomes listed and not reported in the results section of the published report (Kjeken 2013, Sveaas 2014).
We judged the 10 remaining studies (71%) at unclear risk of reporting bias, because we could not compare the pre‐specified outcomes with the reported ones.
Other potential sources of bias
We judged one study at low risk of bias because we identified no other potential source of bias (Rodriguez‐Lozano 2013). Three studies (21%) reported a power sample calculation (Rodriguez‐Lozano 2013; Souza 2017; Sveaas 2014).
Effects of interventions
Exercise programmes versus no intervention
Major outcomes
Data were obtained at the end of the intervention; see Table 1.
Physical function (BASFI, 0 to 10 scale; lower score indicates higher function)
Seven studies (312 participants) found a reduction in physical function score with exercise versus no intervention at the end of the intervention (mean difference (MD) ‐1.3, 95% confidence interval (CI) ‐1.7 to ‐0.9); absolute risk difference 13% (95% CI 9% to 17%); relative change 32% (95% CI 23% to 42%); Analysis 1.1). The statistical heterogeneity was not important (I²= 23%) . There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one point for high risk of bias; we rated the quality of the evidence as moderate (Dönmez 2014; Gallinaro 2016; Garcia 2015; Lim 2005; Masiero 2011; Souza 2017; Sveaas 2014).
1.1. Analysis.
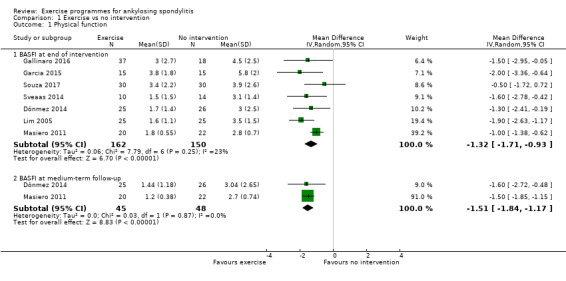
Comparison 1 Exercise vs no intervention, Outcome 1 Physical function.
Two studies (93 participants) found a reduction in physical function score with exercise at medium‐term follow‐up (overall 14 weeks (MD ‐1.5, 95% CI ‐1.8 to ‐1.2; Analysis 1.1)), which was clinically important (absolute risk difference 15% (95% CI 12% to 18%); relative change 57% (95% CI 44% to 67%)) (Dönmez 2014; Masiero 2011). The statistical heterogeneity was not important (I² = 0%).
Pain (VAS, 0 to 10; lower score indicates less pain)
The pooled analysis of six studies (288 participants) showed a decrease in pain with exercise at the end of the intervention (standardised mean difference (SMD) ‐0.82, 95% CI ‐1.4 to ‐0.25; Analysis 1.2; need to report the back‐translated mean difference too here, as per methods (MD ‐2.1, 95% CI ‐3.6 to ‐0.6; 6 studies; absolute reduction 21%, 95% CI 36% to 6%) absolute reduction 21% (95% CI 6% to 3 6% better); relative reduction 34% (95% CI 10% to 59% better); (Dönmez 2014; Gallinaro 2016; Garcia 2015; Lim 2005; Masiero 2011; Souza 2017)). There was an important clinical meaningful benefit. The statistical heterogeneity was considerable (I² = 81%). No rationale could be found to explain the observed severe heterogeneity. Because of study limitations, we downgraded the evidence by one level each for high risk of bias and imprecision; we rated the quality of the evidence as low. One study of 52 participants reported conflicting data (Kraag 1990) in their report. As the reported size effect (MD 0.4, 95% CI ‐0.2 to 0.9) was discordant and inconsistent with the findings of the other six studies, we decided not to include this study in the pooled analysis.
1.2. Analysis.
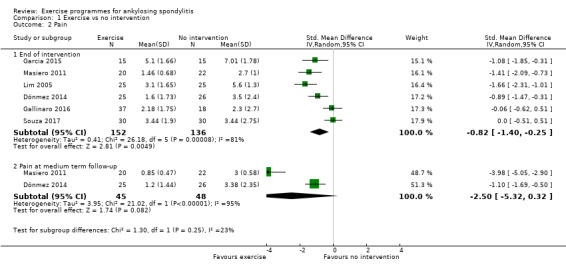
Comparison 1 Exercise vs no intervention, Outcome 2 Pain.
At medium‐term follow‐up (12 to 16 weeks), two studies (93 participants) assessed pain (Dönmez 2014; Masiero 2011) ; We found a statistically significant reduction of pain (SMD ‐2.46, 95% CI ‐5.19 to 0.28). The statistical heterogeneity was considerable (I² = 95%). No rationale could be found to explain the observed severe heterogeneity.
Patient global assessment of disease activity (BASDAI, 0 to 10 scale; lower score indicates lower disease activity)
Six studies (262 participants) found participants who exercised reported statistically significantly lower activity disease at the end of the intervention (MD ‐0.9, 95% CI ‐1.3 to ‐0.5; Analysis 1.3; absolute risk difference 9% (95% CI 5% to 13%); relative change 27% (95% CI 15% to 39%; Dönmez 2014; Gallinaro 2016; Garcia 2015; Masiero 2011; Souza 2017; Sveaas 2014)). The statistical heterogeneity was not important (I² = 18%). There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level for high risk of bias; we rated the quality of the evidence as moderate.
1.3. Analysis.
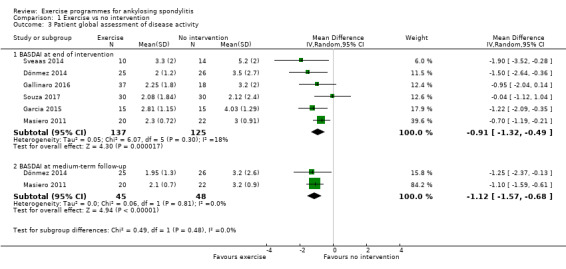
Comparison 1 Exercise vs no intervention, Outcome 3 Patient global assessment of disease activity.
Two studies (93 participants) found a statistically significant reduction in patient global assessment of disease activity with exercise at medium‐term follow‐up (MD ‐1.1, 95% CI ‐1.6 to ‐0.7; Analysis 1.3; Dönmez 2014; Masiero 2011). The statistical heterogeneity was not important (I² = 0%).
Spinal mobility
Schober test (tape distance in cm; longer distance indicates greater spinal mobility)
Three studies used the Schober test to assess spinal mobility. One study (51 participants) reported change from baseline, and found no evidence of difference between groups in spinal mobility (Kraag 1990). Two studies (85 participants) reported final values from a Schober test (Gallinaro 2016), and a modified Schober test (Ince 2006). Pooled results found no evidence of difference between groups (SMD 0.4, 95% CI ‐1.0 to 0.25) at the end of the intervention. The statistical heterogeneity was moderate (I² = 45%). There was no important clinical benefit. Because of study limitations, we downgraded the evidence by one level for high risk of bias, and by two levels for imprecision; we rated the quality of the evidence as very low.
BASMI (0 to 10 scale; lower score indicates greater spinal mobility)
Five studies (232 participants) found more spinal mobility with exercise at the end of the intervention (MD ‐0.7, 95% CI ‐1.3 to ‐0.1; Analysis 1.4; absolute risk difference 7% (95% CI 1% to 13%); relative change 18% (95% CI3% to 34%) (Dönmez 2014; Gallinaro 2016; Masiero 2011; Souza 2017; Sveaas 2014). The statistical heterogeneity was substantial (I² = 51%).There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level each for high risk of bias, inconsistency, and imprecision; we rated the quality of the evidence as very low.
1.4. Analysis.
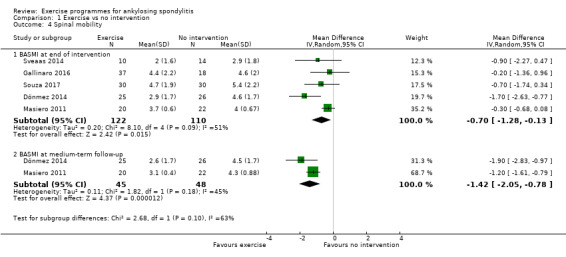
Comparison 1 Exercise vs no intervention, Outcome 4 Spinal mobility.
Two studies (93 participants) found more spinal mobility at medium‐term follow‐up (overall 14 weeks) with exercise (MD ‐1.4, 95% CI ‐2.0 to ‐0.8; Analysis 1.4; (Dönmez 2014; Masiero 2011)). The statistical heterogeneity was moderate (I² = 45%).
Fatigue (VAS, 0 to 10; lower score indicates less fatigue)
Two studies (72 participants) found a statistically significant reduction in fatigue with exercise versus no intervention at the end of the intervention (MD ‐1.4, 95 CI% ‐2.7 to ‐0.1; Analysis 1.5; absolute risk difference 14%, 95% CI 1% to 27%; relative change 48% (95% CI 5% to 91%; Garcia 2015; Masiero 2011). The statistical heterogeneity was substantial (I² = 70%). There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level each for high risk of bias, imprecision, and inconsistency; we rated the quality of the evidence as very low.
1.5. Analysis.

Comparison 1 Exercise vs no intervention, Outcome 5 Fatigue.
At medium‐term follow‐up (24 weeks), one study (42 participants) found a reduction of fatigue with exercise (Masiero 2011). The mean fatigue with exercise was 2.1 on a 10‐point VAS scale, with no exercise it was 3.7 (MD 1.6, 95% CI ‐2 to ‐1.2 ).
Minor outcomes
Quality of life (lower number is better)
We meta‐analysed two of the five studies that assessed quality of life as an outcome.Two studies (85 participants) found inconclusive effects of exercise (MD 1.74, 95% CI ‐0.44 to 3.91; Analysis 1.6; Gallinaro 2016; Garcia 2015). The statistical Heterogeneity was not important (I² = 0%). For three studies, data were either not available (Dönmez 2014), or could not be extracted (Kjeken 2013; Souza 2017).
1.6. Analysis.
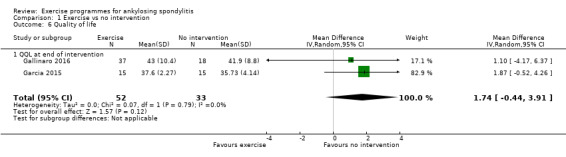
Comparison 1 Exercise vs no intervention, Outcome 6 Quality of life.
C‐Reactive Protein (CRP) and Erythrocyte Sedimentation Rate (ESR)
Two studies (84 participants) reported data for CRP and ECR (Souza 2017; Sveaas 2014). For CRP, we found inconclusive results (MD 1.38, 95% CI ‐4.34 to 7.10 Analysis 1.7) at the end of the intervention . The statistical heterogeneity was substantial (I2 = 71 %). No rationale could be found to explain the observed severe heterogeneity. For ESR, exercise reduced the level of ESR (MD ‐5.36, 95% CI ‐10.31 to ‐0.41 Analysis 1.8). The statistical heterogeneity was not important (I2 = 0%).
1.7. Analysis.
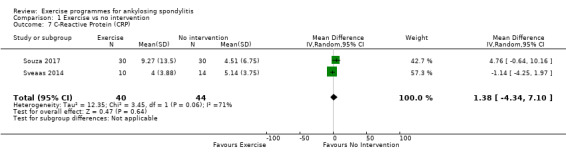
Comparison 1 Exercise vs no intervention, Outcome 7 C‐Reactive Protein (CRP).
1.8. Analysis.
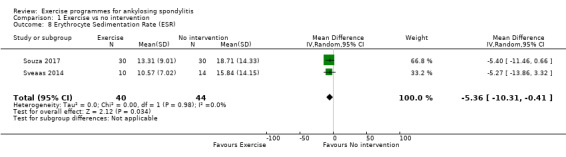
Comparison 1 Exercise vs no intervention, Outcome 8 Erythrocyte Sedimentation Rate (ESR).
Maastricht ankylosing spondylitis enthesitis score (MASES; 0 to 13 scale, lower is better)
One study (55 participants) reported final values at 16 weeks for the exercise and control groups on the 13‐point MASES. No statistical difference was reported between groups (Gallinaro 2016).
Exercise programmes versus usual care
Major outcomes
Data were obtained at the end of the intervention; See Table 2.
Physical function (BASFI, 0 to 10 scale, lower score indicates higher function)
Five studies (1068 participants) found a reduction in physical function score (improvement; indicates higher function) with exercise (MD ‐0.4, 95% CI ‐0.6 to ‐0.2; absolute risk difference 4%; 95% CI 2% to 6%; relative change 11%, 95% CI 5% to 16%; Analysis 2.1; Altan 2012; Kjeken 2013; Rodriguez‐Lozano 2013; Sweeney 2002; Widberg 2009). The statistical heterogeneity was not important (I² = 0%). There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level for high risk of bias; we rated the quality as moderate.
2.1. Analysis.
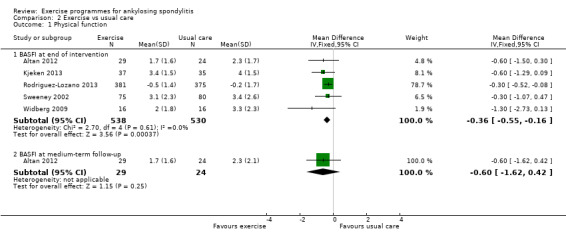
Comparison 2 Exercise vs usual care, Outcome 1 Physical function.
One study (53 participants) reported data at medium‐term follow‐up (Altan 2012). The results were inconclusive (MD ‐0.60, 95% CI ‐1.6 to 0.4; Analysis 2.1). One study (63 participants) reported data at long‐term follow‐up (48 weeks). The results were inconclusive (MD ‐0.10, 95% CI ‐0.84 to 0.64; Kjeken 2013).
Pain (VAS, 0 to 10; lower score indicates less pain)
Two studies (911 participants) reported pain, but used different scales (Rodriguez‐Lozano 2013; Sweeney 2002). Rodriguez‐Lozano 2013 used a VAS to measure pain; Sweeney 2002 used the Standford Self efficacy pain Scale (SES). Pooled analysis found a reduction in pain with exercise (SMD ‐0.2, 95% CI ‐0.3 to ‐0.03; Analysis 2.2; absolute reduction 6%, 95% CI 1% to 8% better; relative reduction 15%, 95% CI 2% to 22% better. The statistical heterogeneity was not important (I² = 0%). There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level for high risk of bias; we rated the quality as moderate.
2.2. Analysis.
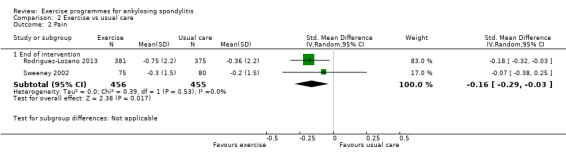
Comparison 2 Exercise vs usual care, Outcome 2 Pain.
Patient global assessment of disease activity (BASDAI, 0 to 10 scale; lower score indicates lower disease activity)
Five studies (1068 participants) found a statistically significant reduction in patient global assessment of disease activity with exercise (MD ‐0.7, 95% CI ‐1.3 to ‐0.1; Analysis 2.3; absolute risk difference 7%, 95% CI 1% to 13%; relative change 19%, 95% CI 3% to 35%; Altan 2012; Kjeken 2013; Rodriguez‐Lozano 2013; Sweeney 2002; Widberg 2009). The statistical heterogeneity was substantial (I² = 70%). No rationale could be found to explain the observed severe heterogeneity. There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level each for high risk of bias and inconsistency; we rated the quality as low.
2.3. Analysis.
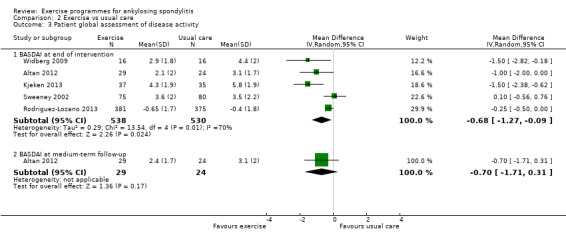
Comparison 2 Exercise vs usual care, Outcome 3 Patient global assessment of disease activity.
One study (93 participants) reported data at medium‐term follow‐up (24 weeks). A statistically significant improvement was found in patient global assessment of disease activity with exercise (MD ‐0.70, 95% CI ‐1.7 to 0.3; Altan 2012).
One study (63 participants) reported data at long‐term follow‐up (48 weeks); the results were inconclusive (MD ‐0.5, 95% CI ‐1.4 to 0.4; Kjeken 2013).
Spinal mobility
Schober test (tape distance in cm; longer distance indicates greater spinal mobility)
No study used the Schober test.
BASMI (0 to 10 scale; lower score indicates greater spinal mobility)
We meta analysed two of the three studies that used the BASMI (Altan 2012; Kjeken 2013; Widberg 2009). Kjeken 2013 did not report data. Two studies (85 participants) found inconclusive results for spinal mobility (MD ‐1.2, 95% CI ‐2.8 to 0.5; Analysis 2.4; absolute risk difference 12%. 95% CI 5% to 28%; relative change 163%, 95% CI 6% to 32%). The statistical heterogeneity was considerable (I² = 82%). No rationale could be found to explain the observed severe heterogeneity. There was no important clinical meaningful benefit. Because of study limitations, we downgraded the evidence by one level each for high risk of bias, inconsistency, and imprecision; we rated the quality as very low.
2.4. Analysis.
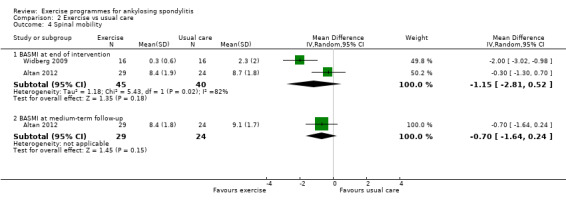
Comparison 2 Exercise vs usual care, Outcome 4 Spinal mobility.
One study reported (53 participants) data at medium‐term follow‐up (24 weeks); the results were inconclusive for spinal mobility (MD ‐0.7 (95% CI ‐1.6 to 0.2; Analysis 2.4; Altan 2012).
One study (63 participants) reported data at long‐term follow‐up (48 weeks); the results were inconclusive (MD ‐0.00, 95% CI ‐0.6 to 0.6; Kjeken 2013).
Fatigue (VAS, 0 to 10; lower score indicates less fatigue)
We found no study measuring fatigue.
Minor outcomes
Quality of life (18‐point ASQol scale; lower number is better)
Data from two studies (809 participants) found inconclusive evidence for quality of life (MD ‐0.36, 95% CI ‐1.68 to 0.95; Analysis 2.5; Altan 2012; Rodriguez‐Lozano 2013). The statistical heterogeneity was moderate (I² = 46%)
2.5. Analysis.
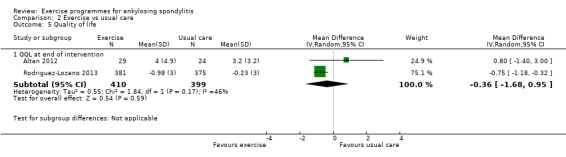
Comparison 2 Exercise vs usual care, Outcome 5 Quality of life.
C‐Reactive Protein (CRP) and Erythrocyte Sedimentation Rate (ESR)
No study measured CRP or ESR.
MASES (0 to 13 scale, lower is better)
No study measured the enthesitis index.
Safety
Adverse effects (AE) associated with exercises
Two studies (110 participants) reported adverse effects related to exercises programmes (Altan 2012; Gallinaro 2016). Because of very low‐quality evidence, we are uncertain of the effect of exercise programmes on AEs (Peto odds ratio (OR) 6.25, 95% CI 0.1 to 320; absolute risk difference 2%, 95% CI 5% fewer to 8% more; relative change 152%, 90% decrease to 5818% increase). The absolute numbers were very low: 1/67 in the exercise group versus 0/43 in the control group. Altan 2012 reported that one participant had an increase of back pain related to exercise. He did not mention whether this resulted in hospitalisation or not (Analysis 3.1). No adverse effects were considered serious. Because of study limitations, we downgraded the evidence by one point for high risk of bias and by two points for imprecision (large CI, small number of studies).
3.1. Analysis.
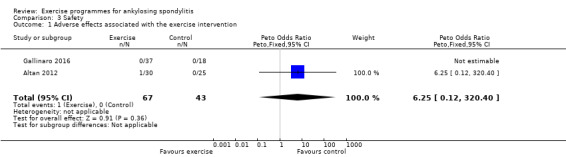
Comparison 3 Safety, Outcome 1 Adverse effects associated with the exercise intervention.
Adverse events
We found no study reporting adverse events.
Subgroup and sensitivity analyses
Given the small number of studies, we did not conduct subgroup analysis to explore the possible effect of type of delivery (supervision versus non‐supervised, mono versus multimodal intervention) on estimated effect size. Neither did we conduct a sensitivity analysis, because we judged all studies at unclear or high risk of bias for most items.
Assessment of publication bias
We had planned to assess publication bias by visual inspection of funnel plots, but we did not generate funnel plots because of the limited number of studies (< 10), and the risk of an underpowered test. We were unable to determine the existence of publication bias.
Discussion
Summary of main results
The main purpose of this review was to evaluate the benefit and harmful effects of exercise programmes for participants in trials of ankylosing spondylitis (AS). Overall, 14 randomised controlled trials (RCT; total of 1579 participants) met the inclusion criteria. Exercise programmes were examined alone in nine trials, and were combined with other interventions (education or self‐management) in five trials. Exercise programmes were compared to usual care in five trials, and to no intervention (waiting list, advice, no exercise) in nine trials. Exercise programmes included different components, and were delivered in a variety of ways.
We found moderate‐ to low‐quality evidence suggesting that exercise programmes, compared to no intervention, probably slightly improve function, may reduce pain (with an important clinical benefit), and probably slightly reduce patient assessment of disease activity at the end of the intervention. Whether there was an effect on spinal mobility and fatigue is unclear.
There is moderate‐ to low‐quality evidence that compared with usual care (including physiotherapy, medication, or self‐management), exercise programmes probably have little or no difference in improving function or reducing pain, and may have little or no difference in patient assessment of disease activity. We are uncertain whether exercise programmes improve spinal mobility.
All studies reported effects at the completion of the intervention. Only two studies assessed the medium‐term follow‐up effect of exercise programmes on physical function, patient global assessment of disease activity, and spinal mobility. One study reported long‐term follow‐up effects.
We have no clear evidence that exercise programmes can induce more adverse effects. Two studies reported adverse effects as an outcome. Only a small number of events were observed (one versus none in comparator groups). We were unable to draw any conclusions.
Overall completeness and applicability of evidence
The evidence provided by this review is limited to the 14 included RCTs that assessed the effects of exercise programmes versus no intervention, or usual care. We did not include three RCTs that were potentially eligible for this review, because their results have not yet been reported in full. Two were ongoing trials (ChiCTR‐TRC‐14004650; NCT02098694). According to the abstract of one trial, home exercises may improve function and spinal mobility, and ameliorate patient‐assessment of disease activity after 10 weeks. However, the control intervention is unknown.
Whether the trial participants reflect individuals with AS undergoing treatment is difficult to determine. Most of the studies in this review included more than 70% men. Since AS seems to affect men and women differently, our results may have limited applicability to women (Dagfinrud 2005; Ramiro 2014). The median age of participants across the included studies was 45 years (interquartile range (IQR) 39 to 47), which is representative of the overall population of patients with AS (Ramiro 2014; Webers 2016). The mean duration of disease of the participants was nine years in the included studies.The effects of exercise programmes of this review should be extrapolated with cautious to people with a shorter disease duration. None of the studies investigated the impact of exercise programmes in people with early or newly diagnosed AS. Only one study included participants with a short disease duration (median 2.5 to 3.5 years), and showed beneficial effects of exercise on mobility (Widberg 2009). In the last decade, improved imaging techniques and criteria for early diagnosis of AS have facilitated earlier and more effective medical treatment (Liang 2015; Lubrano 2015). However, we lack studies of the efficacy of physical exercises on individuals with early forms of AS. Five studies included participants with a BASDAI score ≥ 3.5, corresponding to patients with a low patient‐assessed disease activity (i.e. because the BASDAI scores were < 4/10 units). However, a cutoff of 3.9 to 4 is frequently used to define active disease, discriminating between people with well or poorly controlled disease, but this cutoff does not have a firm justification (Cohen 2006).
Most exercise programmes were delivered in conjunction with drug therapy (standard NSAIDs, disease‐modifying anti‐rheumatic drugs (DMARDs), or biological agents). The benefits of exercise programmes, depending on the type of drug therapy received, cannot be determined. Participants received different types of drug therapy. Nine of the included studies reported that 75% of the participants were taking NSAIDs. For seven studies, 29% of participants received anti‐TNF agents. Four studies did not report or provide any information. No study specifically evaluated the efficacy of physical exercises with biologic versus standard NSAID or DMARD therapy. Since the introduction of TNF blockers, the role of physical exercise in individuals receiving TNF blockers has rarely been studied. We found only one RCT of participants receiving TNF blockers (Masiero 2011). In this study, for participants with clinically stabilised AS who had started TNF blocker therapy at least nine months previously, an educational‐behavioural intervention and exercise training further improved spinal mobility, and reduced pain, stiffness, and disability. One hypothesis is that TNF blockers that reduce inflammation, pain, and fatigue may improve the efficacy of, and compliance with, regular physical exercises and activities, thereby resulting in better function and less disability (Maxwell 2015). Moreover, more motivated individuals are likely to spend longer periods of time on exercise, because they will have greater perceived benefits of exercise regimes (Dubey 2008). Further research should aim to determine the efficacy of exercise interventions in patients with AS receiving TNF blockers.
The included studies investigated a number of different types and combinations of exercise components. Breathing, strengthening, and stretching exercises were the most frequent exercise components. However, the components were incompletely described in most trials. For example the material used, who provided the intervention, how it was supervised, and where the exercise was delivered were often missing. However, the duration (mean 60 minutes) and frequency (three sessions/week) was similar among studies. The minimal effective dose and optimal level was unclear. The exercise dosage could not be explored with indirect statistical techniques, such as meta‐regression. Thus, we did not investigate heterogeneity by the type of exercise, because we were unable to isolate individual types of exercise from the programme reported by the authors.
Information was also lacking on adherence to exercise, which is important to assess with regular exercise and long disease duration. The optimal exercise programme for individuals with AS, and its efficacy, are still unknown. The poor reporting of non‐pharmacological interventions is well known, despite the existence of reported guidelines (TIDieR), thereby limiting the implementation of research results in clinical practice (Hoffmann 2014). Slade 2016 recently developed a specific template, Consensus on Exercise Reporting Template (CERT), for reporting exercise programmes in clinical trials. We hope that this template will help authors improve the reporting of exercise in clinical trials.
Another issue relates to outcomes. We assessed important outcomes for participants based on the ASAS/EULAR recommendations, to show a short‐term clinical benefit of exercise programmes versus no intervention (Sieper 2009; Van der Heijde 1997; www.asas‐group.org). The most common outcomes measured in the included studies were physical function (N = 12, 86%), patient global assessment of disease activity (N = 11, 79%), spinal mobility and pain (N = 7, 50%). Quality of life and fatigue were not frequently reported. The RCTs ranged from 8 to 12 weeks’ duration, so all data for benefit are based on only short‐term studies. Follow‐up effects were measured in only 14% of studies (N = 2). Whether the effects persist after the completion of exercise programmes is unknown.
Lastly, we were unable to assess the safety of exercise programmes, because adverse effects were not systematically monitored and reported in publications. Severe adverse events are rare with exercises but it can happen (for example fall). Exercise programmes are generally associated with minor adverse effects (muscle or joint pain, soreness) related to interventions (Kunutsor 2018). In our review, adverse effects were reported in one study, and only one event was associated with exercise programmes. Direct evidence for safety was not found, particularly for populations at risk, such as older people, or those with more severe AS. Data provided by Jacques 2014 suggested that mechanical strain can trigger inflammation, and cause bone degradation in mice. This result supports the need to systematically monitor adverse effects of exercise programmes, to determine if exercises are safe or if some adverse effects might be expected for example with a modification of exercise dosing / intensity (McGonagle 2014).
Quality of the evidence
We had concerns about risk of bias for all studies included: 79% (N = 11) had unclear allocation concealment; all failed to blind participants, staff, or outcome assessors; 43% had incomplete outcome data (N = 6), and 86% had unclear selective reporting, or a high risk of other bias (N = 12). Given the number of studies included in the review, we cannot rule out the existence of a small‐study effect, explaining the magnitude of the positive results we found.
We considered statistically significant group differences between exercise programmes versus no intervention or usual care. Larger effects were found when exercise was compared to no intervention. For each comparison, the number of studies (< 10), and small samples (many studies were small, with < 100 participants) might have contributed to a low‐power analysis. Low power is associated with bias (Button 2013). Most studies we included were assessed at high or unclear risk of bias, which suggests that the estimated effects might be over‐estimated, and reduces the likelihood that they reflect a true effect. We cannot provide conclusions with a high level of confidence. The magnitude of the estimated effects may change with larger studies.
We only presented the findings of trials that reported the major outcomes of interest in Table 1 and Table 2; and used the GRADE approach to assess the quality of the evidence examined for each outcome (Schünemann 2011b). Most of the evidence was downgraded to low or very low quality, based on three factors: risk of bias, inconsistency generated by heterogeneity, and imprecision with small trials and large confidence intervals.
Potential biases in the review process
We made all attempts to reduce the bias involved in the review process by including the best available evidence. All studies included were randomised trials. We conducted an extensive search of the literature in all relevant databases, but because two studies have not yet been incorporated, this may be a source of potential bias. Two review authors independently selected studies, extracted data, and assessed the risk of bias. For missing data, we attempted to extract data that were graphically displayed by using software tools (arohatgi.info/WebPlotDigitizer/index.html), or to systematically seek information from authors of the included studies.
The review itself has some limitations. We could not determine whether participants who received usual care also had exercises, because the included studies poorly described the content of usual care interventions. Participants in the usual care group could have practiced exercises, which could explain why a smaller effect size was always found when comparing exercise programmes to usual care. A possible explanation could also be the result of performance bias, due to lack of blinding.
We found wide variations among the trials, likely related to different exercise components. . Despite the pre‐specification stated in the protocol, we could not perform subgroup analyses to explore heterogeneity for factors, such as supervision, modalities of exercises, or participant characteristics. Lastly, the number of included studies was too small.
Agreements and disagreements with other studies or reviews
Different systematic reviews have examined the effects of exercise programmes in people with AS. None included all of the RCTs we identified, all of which compared the effects of exercise programmes to no intervention or usual care.
Dagfinrud 2008 included 11 RCTs and quasi‐randomised trials (763 participants). Only four studies compared exercise programmes with no intervention (Ince 2006; Kraag 1990; Lim 2005; Sweeney 2002). The other included studies compared different modalities of exercise programmes. The systematic review did not meta‐analyse the results of the comparator groups. Only the effects of individual studies were reported. The authors reported low‐quality evidence for effects on spinal mobility and physical function. An update was performed by Dagfinrud 2011, which included one additional study. The authors included the same four previously included studies that compared different types of exercise programmes to no intervention. They did not meta‐analyse the results.
Van den Berg 2012 performed a systematic review that included randomised and uncontrolled trials (cohort studies, case–control studies, and cross‐sectional studies), which evaluated any type of non‐pharmacological intervention. They concluded that exercise programmes were better than no intervention. This review included only one of the 14 trials included in our review (Widberg 2009).
O'Dwyer 2014 included randomised and quasi‐randomised trials. This systematic review included only five of the 14 RCTs included in our review, and concluded that therapeutic exercise improved physical function, joint mobility, and cardiorespiratory function, and ameliorated patient‐assessed disease activity, pain, and stiffness compared with controls. They assessed the evidence to be of moderate quality.
A recent systematic review compared specific pulmonary exercise programmes to conventional exercise or no intervention (Saracoglu 2017). The authors included eight RCTs or controlled trials. Two of the trials were included in our review, but the other six were excluded, because they did not meet our inclusion criteria (Altan 2012; Ince 2006). Evidence showed that exercise improved functional capacities and pulmonary functions, but the authors did not provide a critical appraisal of available studies. They did not conduct a meta‐analysis.
Three systematic reviews examined the effect of exercises combined with stabilised TNF blocker therapy versus patients with AS stabilised by TNF blocker therapy (Giannotti 2014; Liang 2015; Lubrano 2015). These systematic reviews included non‐randomised controlled trials, observational studies, and abstracts, which evaluated spa exercise therapy combined with stabilised TNF blocker therapy. The authors concluded that exercises combined with stabilised TNF blocker therapy might reduce patient‐assessed disease activity, improve function and quality of life compared with biologic therapy alone. Our findings are consistent with previous reviews and guidelines that found short‐term effects of exercise programmes (Regel 2017; Ward 2016).
Authors' conclusions
Implications for practice.
We found moderate‐ to low‐quality evidence indicating that exercise programmes compared to no intervention probably slightly improve function, may reduce pain (important clinical benefit), and probably slightly reduce patient‐assessed disease activity, measured after the completion of the exercise programmes. Whether there was an effect on spinal mobility and fatigue is uncertain. We found moderate‐ to low‐quality evidence that compared with usual care (including physiotherapy, medication, or self‐management), exercise programmes probably have little or no effect on improving function and reducing pain, and may have little or no difference on patient‐assessed disease activity. We are uncertain whether exercise programmes improve spinal mobility.
Readers should understand that we are uncertain of the potential for harm from exercise programmes, because of the limited number of studies reporting AEs, and the low rate of events.
We are unable to distinguish the best type of exercise, its components, or its mode of delivery.
Implications for research.
The evidence for some of the major outcomes was low or very low quality, so new studies could change the estimate effects.
This review has raised new questions to answer:
The long‐term effects of exercise programmes for people with AS, and whether they are clinically relevant are unclear.
New trials should provide an accurate description of the content, dose, application, and adherence to the exercise interventions. The most effective components (e.g. supervised or home delivery) are unknown, as is the most effective dose, including frequency, intensity, and duration.
AEs were rarely measured and reported in RCT reports. Whether exercise programmes produce harmful effects is difficult to determine. AEs may be worthwhile to investigate in people with more advanced or severe stages of the disease. Studies should systematically investigate and report AEs.
Further studies should investigate the effect of exercise therapy in the early stages of the disease (even in the pre‐radiographic stages). Exercise programmes should be evaluated at different stages of the disease. This evaluation would be useful to ascertain whether the use of biologic agents and rehabilitation programmes in people with newly‐diagnosed, or early AS, are effective to prevent deformity and disability.
Studies of the effects of TNF blockers combined with exercise programmes, with cost‐effectiveness, are needed.
Cost‐effectiveness of interventions should be evaluated.
Future studies should use the Consensus on Exercise Reporting Template, or the CONSORT Template for Intervention Description and Replication, to improve the description of exercise programmes and facilitate their application in clinical practice.
What's new
| Date | Event | Description |
|---|---|---|
| 28 January 2020 | Amended | Corrected SoF table 1 |
Acknowledgements
The authors thank L Trinquart for statistical expertise, the Cochrane Musculoskeletal Review Group editorial team for helpful support, and T Rader, D Wendling, and the reviewers for editorial comments. We also thank Laura Smales for her suggestions for translation and formatting.
Appendices
Appendix 1. MEDLINE Ovid search strategy
1 Spondylitis, Ankylosing/
2 Spondylarthritis/ )
3 (axial adj2 spondylarthritis).tw.
4 (axial adj2 spa).tw.
5 (ankylos$ or spondyl$).tw.
6 (bekhterev$ or bechterew$).tw.
7 (Marie adj struempell$).tw.
8 (AS or axSPA).tw.
9 Sacroiliitis/
10 ((axial or spin$ or peripheral or vertebral or enthesitis) adj3 (joint$ or spondyloarthritis or arthritis or ankylosing)).tw.
11 or/1‐10
12 exp Exercise/
13 Physical Exertion/
14 Physical Fitness/
15 exp Physical Endurance/
16 exp Sports/
17 Pliability/
18 exertion$.tw.
19 exercis$.tw.
20 sport$.tw.
21 ((physical or motion) adj5 (fitness or therapy or therapies)).tw.
22 (physical$ adj2 endur$).tw.
23 manipulat$.tw.
24 (skate$ or skating).tw.
25 jog$.tw.
26 swim$.tw.
27 bicycl$.tw.
28 (cycle$ or cycling).tw.
29 walk$.tw.
30 (row or rows or rowing).tw.
31 weight train$.tw.
32 muscle strength$.tw.
33 exp Yoga/
34 yoga.tw.
35 exp Tai Ji/
36 tai chi.tw.
37 Ai Chi.tw.
38 exp Vibration/
39 vibration.tw.
40 pilates.tw.
41 Motor Activity/
42 exp Exercise Therapy/
43 exp Proprioception/
44 exp Physical Therapy Modalities/
45 exp Rehabilitation/
46 or/12‐45
47 11 and 46
48 randomized controlled trial.pt.
49 controlled clinical trial.pt.
50 randomized.ab.
51 placebo.ab.
52 clinical trials as topic.sh.
53 randomly.ab.
54 trial.ti.
55 or/48‐54
56 exp animals/ not humans.sh.
57 55 not 56
58 47 and 57
Appendix 2. CENTRAL search strategy
1. MeSH descriptor: [Exercise] explode all trees
2. Exert:ti,ab
3. MeSH descriptor: [Physical Fitness] explode all trees
4. MeSH descriptor: [Exercise Test] explode all trees
5. MeSH descriptor: [Exercise Tolerance] explode all trees
6. MeSH descriptor: [Sports] explode all trees
7. MeSH descriptor: [Pliability] explode all trees
8. MeSH descriptor: [Physical Endurance] explode all trees
9. exertion*:ti,ab
10. exercis*:ti,ab
11. sport*:ti,ab
12. ((physical or motion) near/5 (fitness or therap*)):ti,ab
13. (physical* near/2 endur*):ti,ab
14. ((strength* or isometric* or isotonic* or isokinetic* or aerobic* or endurance or weight*) near/5 (exercis* or train*)):ti,ab
15. MeSH descriptor: [Physical Therapy Modalities] explode all trees
16. (physical next therap*):ti,ab
17. physiotherap*:ti,ab
18. manipulat*:ti,ab
19. kinesiotherap*:ti,ab
20. MeSH descriptor: [Rehabilitation] explode all trees
21. rehab*:ti,ab
22. (skate* or skating):ti,ab
23. run*:ti,ab
24. jog*:ti,ab
25. treadmill*:ti,ab
26. swim*:ti,ab
27. bicycl*:ti,ab
28. (cycle* or cycling):ti,ab
29. walk*:ti,ab
30. (row or rows or rowing):ti,ab
31. muscle next strength:ti,ab
32. (#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31)
33. MeSH descriptor: [Spondylitis, Ankylosing] explode all trees
34. MeSH descriptor: [Spondylarthropathies] explode all trees
35. ankylosing or spondyl:ti,ab
36. bekhterev or bechterew:ti,ab
37. ((axial or spin* or peripheral or vertebral or enthesitis) near/3 (joint* or spondyloarthritis or arthritis or ankylosing)) .tw.
38. #33 or #34 or #35 or #36 or #37
39. #32 and #38
Appendix 3. Embase search strategy
1 ankylosing spondylitis/
2 (ankylos$ or spondyl$).tw.
3 (bekhterev$ or bechterew$).tw.
4 (Marie adj struempell$).tw.
5 sacroiliitis/
6 ((axial or spin$ or peripheral or vertebral or enthesitis) adj3 (joint$ or spondyloarthritis or arthritis or ankylosing)).tw.
7 (AS or axSPA).tw.
8 or/1‐7
9 exp EXERCISE/
10 fitness/
11 exercise test/
12 exercise tolerance/
13 exp Sport/
14 pliability/
15 exp "physical activity, capacity and performance"/
16 exertion$.tw.
17 exercis$.tw.
18 sport$.tw.
19 ((physical or motion) adj5 (fitness or therap$)).tw.
20 (physical$ adj2 endur$).tw.
21 ((strength$ or isometric$ or isotonic$ or isokinetic$ or aerobic$ or endurance or weight$) adj5 (exercis$ or train$)).tw.
22 exp physiotherapy/
23 physiotherap$.tw.
24 manipulat$.tw.
25 kinesiotherap$.tw.
26 exp REHABILITATION/
27 rehab$.tw.
28 (skate$ or skating).tw.
29 run$.tw.
30 jog$.tw.
31 treadmill$.tw.
32 swim$.tw.
33 bicycl$.tw.
34 (cycle$ or cycling).tw.
35 walk$.tw.
36 (row or rows or rowing).tw.
37 muscle strength$.tw.
38 or/9‐37
39 random$.ti,ab.
40 factorial$.ti,ab.
41 (crossover$ or cross over$ or cross‐over$).ti,ab.
42 placebo$.ti,ab.
43 (doub$ adj blind$).ti,ab.
44 (singl$ adj blind$).ti,ab.
45 assign$.ti,ab.
46 allocat$.ti,ab.
47 volunteer$.ti,ab.
48 crossover procedure.sh.
49 double blind procedure.sh.
50 randomized controlled trial.sh.
51 single blind procedure.sh.
52 or/39‐51
53 exp animal/ or nonhuman/ or exp animal experiment/
54 exp human/
55 53 and 54
56 53 not 55
57 8 and 38 and 56
Appendix 4. CINAHL search strategy
| S40 | S7 AND S39 |
| S39 | S38 or S37 or S36 or S35 or S34 or S33 or S32 or S31 or S30 or S29 or S28 or S27 or S26 or S25 or S24 or S23 or S22 or S21 or S20 or S19 or S18 or S17 or S16 or S15 or S14 or S13 or S12 or S11 or S10 or S10 or S9 or S8 |
| S38 | (ti "muscle strength*") or (ab "muscle strength*") |
| S37 | (ti row or rows or rowing) or (ab row or rows or rowing) |
| S36 | (ti walk*) or (ab walk*) |
| S35 | (ti cycle* or cycling) or (ab cycle* or cycling) |
| S34 | (ti bicycl*) or (ab bicycl*) |
| S33 | (ti swim*) or (ab swim*) |
| S32 | (ti swim*) or (ab swim*) |
| S31 | (ti treadmill*) or (ab treadmill*) |
| S30 | (ti jog*) or (ab jog*) |
| S29 | (ti run*) or (ab run*) |
| S28 | (ti skate* or skating) or (ab skate* or skating) |
| S27 | (ti rehab*) or (ab rehab*) |
| S26 | (MH "Rehabilitation+") |
| S25 | (ti kinesiotherap*) or (ab kinesiotherap*) |
| S24 | (ti manipulat*) or (ab manipulat*) |
| S23 | (ti physiotherap*) or (ab physiotherap*) |
| S22 | (MH "Physical Therapy+") |
| S21 | TI ( strength* or isometric* or isotonic* or isokinetic*or aerobic* or endurance or weight* ) or AB ( strength* or isometric* or isotonic* or isokinetic*or aerobic* or endurance or weight* ) |
| S20 | TI physical* n2 endur* or AB physical* n2 endur* |
| S19 | TI physical N5 fitness or TI physical N5 therap* or AB physical N5 fitness or AB physical N5 therap* or TI motion n5 therap* or AB motion n5 therap* |
| S18 | (ti sport*) or (ab sport*) |
| S17 | (ti exercis*) or (ab exercis*) |
| S16 | (ti exertion*) or (ab exertion*) |
| S15 | (MH "Physical Endurance+") |
| S14 | (MH "Pliability") |
| S13 | (MH "Sports+") |
| S12 | (MH "Exercise Tolerance+") |
| S11 | (MH "Exercise Test+") |
| S10 | (MH "Physical Fitness") |
| S9 | (MH "Exertion+") |
| S8 | (MH "Exercise+") |
| S7 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 |
| S6 | (MH "Spondylarthritis") |
| S5 | "Sacroiliitis" |
| S4 | "Axial Spondyloarthritis" |
| S3 | "AS or axSPA" |
| S2 | "(bekhterev or bechterew)" |
| S1 | (MH "Spondylitis, Ankylosing") |
Appendix 5. PEDro search strategy
Topic: spondylitis or spondyloarthritis
Intervention: Fitness training, Strength training, Stretching, mobilisation, manipulation, massage
Appendix 6. Clinicaltrials.gov search strategy
all years
Ankylosing spondylitis in Condition
Exercise in Intervention
Appendix 7. WHO ICTRP search strategy
Ankylosing spondylitis in Condition Exercise in Intervention
Data and analyses
Comparison 1. Exercise vs no intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Physical function | 7 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 BASFI at end of intervention | 7 | 312 | Mean Difference (IV, Random, 95% CI) | ‐1.32 [‐1.71, ‐0.93] |
| 1.2 BASFI at medium‐term follow‐up | 2 | 93 | Mean Difference (IV, Random, 95% CI) | ‐1.51 [‐1.84, ‐1.17] |
| 2 Pain | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 End of intervention | 6 | 288 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.82 [‐1.40, ‐0.25] |
| 2.2 Pain at medium term follow‐up | 2 | 93 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.50 [‐5.32, 0.32] |
| 3 Patient global assessment of disease activity | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 BASDAI at end of intervention | 6 | 262 | Mean Difference (IV, Random, 95% CI) | ‐0.91 [‐1.32, ‐0.49] |
| 3.2 BASDAI at medium‐term follow‐up | 2 | 93 | Mean Difference (IV, Random, 95% CI) | ‐1.12 [‐1.57, ‐0.68] |
| 4 Spinal mobility | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 BASMI at end of intervention | 5 | 232 | Mean Difference (IV, Random, 95% CI) | ‐0.70 [‐1.28, ‐0.13] |
| 4.2 BASMI at medium‐term follow‐up | 2 | 93 | Mean Difference (IV, Random, 95% CI) | ‐1.42 [‐2.05, ‐0.78] |
| 5 Fatigue | 2 | 72 | Mean Difference (IV, Random, 95% CI) | ‐1.43 [‐2.73, ‐0.14] |
| 5.1 BASDAI at end of intervention | 2 | 72 | Mean Difference (IV, Random, 95% CI) | ‐1.43 [‐2.73, ‐0.14] |
| 6 Quality of life | 2 | 85 | Mean Difference (IV, Random, 95% CI) | 1.74 [‐0.44, 3.91] |
| 6.1 QQL at end of intervention | 2 | 85 | Mean Difference (IV, Random, 95% CI) | 1.74 [‐0.44, 3.91] |
| 7 C‐Reactive Protein (CRP) | 2 | 84 | Mean Difference (IV, Random, 95% CI) | 1.38 [‐4.34, 7.10] |
| 8 Erythrocyte Sedimentation Rate (ESR) | 2 | 84 | Mean Difference (IV, Random, 95% CI) | ‐5.36 [‐10.31, ‐0.41] |
Comparison 2. Exercise vs usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Physical function | 5 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 BASFI at end of intervention | 5 | 1068 | Mean Difference (IV, Fixed, 95% CI) | ‐0.36 [‐0.55, ‐0.16] |
| 1.2 BASFI at medium‐term follow‐up | 1 | 53 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.62, 0.42] |
| 2 Pain | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 End of intervention | 2 | 911 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.29, ‐0.03] |
| 3 Patient global assessment of disease activity | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 BASDAI at end of intervention | 5 | 1068 | Mean Difference (IV, Random, 95% CI) | ‐0.68 [‐1.27, ‐0.09] |
| 3.2 BASDAI at medium‐term follow‐up | 1 | 53 | Mean Difference (IV, Random, 95% CI) | ‐0.70 [‐1.71, 0.31] |
| 4 Spinal mobility | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 BASMI at end of intervention | 2 | 85 | Mean Difference (IV, Random, 95% CI) | ‐1.15 [‐2.81, 0.52] |
| 4.2 BASMI at medium‐term follow‐up | 1 | 53 | Mean Difference (IV, Random, 95% CI) | ‐0.70 [‐1.64, 0.24] |
| 5 Quality of life | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 QQL at end of intervention | 2 | 809 | Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐1.68, 0.95] |
Comparison 3. Safety.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Adverse effects associated with the exercise intervention | 2 | 110 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 6.25 [0.12, 320.40] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Altan 2012.
| Methods | RCT with two groups No intention‐to‐treat analysis |
|
| Participants | Location: Turkey Randomised: 55 Analysed: 53 Age: 45 years Gender: 55% men Recruited: from a rheumatology clinic, mono‐centre Inclusion criteria: AS according to the modified New York criteria, regular follow‐up protocol in the clinic Exclusion criteria: systemic problem contraindicating exercising, peripheral arthritis, total spinal ankylosis, ESR over 50 mm/h, CRP more than 10 times the normal value, changed treatment regimens during the 2 months prior to the study Severity and duration of the disease: the duration of disease was 2 to 22 years (mean: 9) Coexisting medication treatment: 31% received NSAID, 32% sulphasalazine, and 21% biological agent treatment regularly, while 17% did not use regular medication. No change of medication during the study. |
|
| Interventions | Exercise group (N = 29)
Control group (N = 24)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 12, follow‐up = 24 Major outcomes
Minor outcomes
|
|
| Notes | Number of missing participants: 2 (4%) Dropouts or withdrawals: n = 2; 1 in the exercise group and 1 in the control group Adverse effects: n = 1 (2%) in exercise group complained of increased back pain Sample size calculation: not reported Funding source: not available Declaration of interest: authors declared no conflict of interest Protocol registration number not found Additional information provided after e‐mail contact |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: adequate method of random sequence generation Quote: "The participants were assigned randomly into two groups using random number table by the researcher other than the one who performed the evaluation throughout the study." |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the intervention allocated Quote: "The participants were fully informed about the nature and purpose of the study." |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded Quote: "the same researcher who was totally unaware of the groups the participants belonged to, and all participants were requested not to give information to the examiner about their treatment protocol." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: as treated analysis was carried out. Few balanced dropouts (1 in each group). May have a minor influence on the estimate of effect size. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported. Outcomes listed in the method section were all reported in the results section. Safety was not reported as an outcome. Major and minor outcomes were specified. |
| Other bias | Unclear risk | Comment: attendance and compliance were not reported. Small sample size. Baseline performances were similar on major outcomes. Rates of medications did not differ between the two groups. No power sample calculation. Funding and conflict of interest were not declared. |
Dönmez 2014.
| Methods | RCT with three groups intention‐to‐treat analysis performed |
|
| Participants | Location: Turkey Randomised: 77 Analysed: 77 Age: 42 years Gender: 53% men Recruited: unclear Inclusion criteria: having a diagnosis of AS (meeting the Modified New York, ASAS criteria, or both, for axial SpA). Not doing any regular physical exercise in the last 6 months Exclusion criteria: severe cardiac, neurologic, or cognitive dysfunction, history of surgical intervention for spinal cord, pregnancy, severe psychiatric disorder, fractures due to secondary osteoporosis, being wheelchair‐bound Severity and duration of the disease: not reported Coexisting medication treatment: no interruption or change of medication during the study |
|
| Interventions | Exercise group (N = 25)
Control group (N = 26)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 3, follow‐up = 12 Major outcomes
Minor outcomes
|
|
| Notes | Unclear if participants in the control group could practice community‐based exercises Number of missing participant: n = 0; unclear reporting Dropouts or withdrawals: n = 0; unclear reporting Adverse events: not reported Adverse effects: not reported Sample size calculation: not reported Funding source: not available Declaration of interest: authors declared no conflict of interest Protocol registration number not found Additional information provided after e‐mail contact |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "patients [.] were allocated to three groups using a random numbers table" |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the intervention allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: the study did not provide information about missing data. After e‐mail contact, the authors stated that no data were missing |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported; no information provided in the publication. After e‐mail contact, the authors stated that all the outcomes were reported. |
| Other bias | Unclear risk | Comment: attendance and compliance were not reported. Inbalance at baseline was reported. No sample size calculation. Limited information in the published abstract. Funding and conflict of interest were not stated. |
Gallinaro 2016.
| Methods | RCT with three groups Intention‐to‐treat: unclear |
|
| Participants | Location: Brazil Randomised: 55 Analysed: 55 Age: 48.7 years Gender: 87% men Recruited: from outpatient centre of São Paulo University, clinics of São Paulo. Inclusion criteria: having a diagnosis of AS (meeting the Modified New York); BASDAI < 4; stable medication for 6 months, not doing any regular physical exercise in the last 6 months. Functional class I to III. Exclusion criteria: change of medication during the study, doing exercise during the study period, important functional or walking limitation, cardiac problem contraindicating exercising, fibromyalgia, pain VAS over 8 Severity and duration of the disease: the mean BASDAI was 2.2; disease duration was 18.2 years Coexisting medication treatment: NSAIDs, biological treatment, DMARDs |
|
| Interventions | Exercise group (N = 37)
Control group (N = 18)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0 , final point = 16 Major outcomes
Safety: reported as an outcome Minor outcomes
|
|
| Notes | Number of missing participant: n = 0 Dropouts or withdrawals: n = 0 Adverse events: reported Averse effects: reported Sample size calculation: not reported Funding source: not available Declaration of interest: not available Protocol registration number: NCT01690273 We did not contact the author; additional information was found in a thesis manuscript (www.teses.usp.br/teses/disponiveis/5/5169/tde‐04112016‐150051/fr.php) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: not sufficient information provided Quote: "The AS patients were randomly assigned into three groups". |
| Allocation concealment (selection bias) | Unclear risk | Comment: incomplete description found about allocation concealment Quote "em 3 grupos de pesquisa atraves de envelope pardo lacrado". |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the intervention allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all patients were included for analysis; Tables 2 & 3 |
| Selective reporting (reporting bias) | Low risk | Comment: The study protocol and the results were posted on ClinicalTrials.gov |
| Other bias | Unclear risk | Comment: small number of subjects; no power sample size calculation; conflicts of interest were not declared |
Garcia 2015.
| Methods | RCT with two groups intention‐to‐treat analysis performed |
|
| Participants | Location: Spain Randomised: 30 Analysed: 30 Age: 47 years Gender: 53% men Recruited: from association of arthritis and spondylitis Inclusion criteria: having a diagnosis of AS by a rheumatologist (meeting the modified New York, ASAS criteria, or both, for axial SpA), take only NSAIDS a month before, and during the study period Exclusion criteria: cardiovascular disease Severity and duration of the disease: mean time since diagnosis = 7 years Coexisting medication treatment: NSAIDS (100%) |
|
| Interventions | Exercise group (N = 15)
Control group (N = 15)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0 , final point = 8 Major outcomes
Minor outcomes
|
|
| Notes | Number of missing participant: n = 0 Dropouts or withdrawals: n = 0 Adverse events: not reported Averse effects: not reported Sample size calculation: not reported Funding source: not available Protocol registration number not found Declaration of interest: authors declared no conflict of interest |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "individuals were randomised using random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the intervention allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all patients were included in the analysis |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported. Outcomes listed in the methods section were all reported in the results section. Safety was not reported as an outcome. |
| Other bias | Unclear risk | Comment: attendance and compliance were not reported; imbalance at baseline was reported; no sample size calculation |
Ince 2006.
| Methods | RCT with two groups intention‐to‐treat analysis unclear |
|
| Participants | Location: Turkey Randomised: 30 Analysed: unclear Age: 35 years Gender: 60% men Setting: referred by their physician to the university department hospital, monocentre Inclusion criteria: AS according to the modified New York criteria Exclusion criteria: not reported Severity and duration of the disease: 4 participants with a stage II, 26 with a stage I (according to the modified New York criteria), mean disease duration = 9 years Coexisting medication treatment: NSAIDS + Sulfasalazine (100%) |
|
| Interventions | Exercise group (N = 15)
Control group (N = 15)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 12 Major outcomes
Minor outcomes |
|
| Notes | Number of missing participant: not reported Dropouts or withdrawals: not reported Adverse events: not reported Adverse effects: not reported sample size calculation: not provided Funding source: this study was supported by the Research Project Unit of Cukurova University, Adana, Turkey (Project No: SBE2002D12) Protocol registration number not found Declaration of interest: not reported Additional informations provided after e‐mail contact |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: more information provided after e‐mail contact: "randomisation with coin tossing" Quote: "the 30 subjects with AS were randomly divided into two groups" |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: inadequate blinding; personnel unblinded Quote: "The exercise instructor was blinded to physiologic measures." |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: the study did not provide information about missing data; additional information provided after e‐mail contact. The authors stated that all the patients completed the study and were analysed. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported. Outcomes listed in the methods section were all reported in the results section; no major and minor outcomes designation |
| Other bias | Unclear risk | Comment: small number of subjects; main and recommended outcomes not used (no BASDAI, BASMI, or BASDAI), no power sample size calculation. Conflicts of interest were not declared. |
Kjeken 2013.
| Methods | RCT with two groups No Intention‐to‐treat analysis. |
|
| Participants | Location: Norway Randomised: 100 Analysed: 95 Age: 49 years Gender: 67% men Recruited: from the hospital outpatient clinic and rheumatology department, multicentre (two different hospitals) Inclusion criteria: age between 18 and 65 years, AS according to the modified New York criteria, regular follow‐up protocol in the clinic, BASDAI ≥ 40 mm Exclusion: coronary heart disease; pregnancy; impaired function due to other significant medical problems; surgery or rehabilitation within the last 6 months; or cognitive or mental impairment. "In addition, participants in the control group were excluded at the 4‐month control if they reported participation in multidisciplinary rehabilitation after baseline assessment. Also, participants in both groups were excluded at the 12‐month control if they had started biological therapy during the trial period, or reported multidisciplinary rehabilitation after the 4‐month assessment." Severity and duration of the disease: disease duration = 15.5 yrs Coexisting medication treatment: analgesics (30.5%), NSAIDs (75.8%), biological therapy (7.4%), DMARDS (4.2%) |
|
| Interventions | Exercise group (N = 46)
Control group (N = 49)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0 , final point = 16 , follow‐up = 48 Major outcomes
Minor outcomes
|
|
| Notes | Unclear if participants in the control group could practice community‐based exercises Number of missing participants: 10 participants were excluded prior to follow‐up assessments, most frequently due to participation in rehabilitation programmes at other centres in the trial period (n = 6 in the control group, and 4 in the exercise group). A total of 80% and 63% completed 4‐ and 12‐month assessments in the rehabilitation group, vs 71% and 61% in the control group Dropouts or withdrawals: n = 25 (n = 12 in the exercise group; n = 13 in the control group) Adverse events: n =3 (3%) Averse effects: not reported Sample size calculation: reported; needed 50 patients in each group Funding source: this work was supported by Health South‐East, Norway, grant number 2006077 Protocol registration number: ISRCTN75685576 Declaration of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: a computer‐based sequence generation was used Quote: "Patients were randomly assigned to the intervention or control group. A statistician not involved in the study made a computer‐generated randomisation list." |
| Allocation concealment (selection bias) | Low risk | Comment: additional information after e‐mail contact. The authors reported that envelopes were numbered Quote: "Concealed, opaque envelopes, prepared by a secretary, were used to allocate the patients [...] open after baseline assessments". |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded Quote: "In this trial, the patients and therapists delivering the intervention were aware of the treatment assigned." |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: high rate of drop‐out (28%); no intention‐to‐treat analysis; no imputation techniques used |
| Selective reporting (reporting bias) | High risk | Comment: differences found between outcomes stated in the protocol and outcomes reported in the publication Quote: "Biological signs of inflammation: erythrocyte sedimentation rate and C‐reactive protein" were not reported. We could not incorporate data from the SF‐36 scale in the meta‐analysis |
| Other bias | Unclear risk | Comment: attendance and compliance not reported. No systematic reporting of adverse events. Outcomes reported a medium‐ and long‐term follow‐up. Power sample size calculation. Data adjusted for baseline values. Conflicts of interest were not declared |
Kraag 1990.
| Methods | RCT with two groups modified intention‐to‐treat analysis |
|
| Participants | Location: Canada Randomised: 53 Analysed: 52 Age: 38 years (range: 19 to 73) Gender: 79% men Recruited: from the Arthritis Society home physiotherapy service Inclusion criteria: AS according to the New York criteria, English comprehension, absence of corticotherapy for at least 3 months, absence of immunotherapy for at least 6 months pre study, stable clinical status and drug therapy, ARA functional class 1, 2, or 3, no surgery anticipated in the next 4 months, if female, practising reliable contraception and not pregnant Exclusion criteria: more than 10% loss of flexion in either hip joint Severity and duration of the disease: no information mean pain at baseline (in mm): 35 morning stiffness: 75% Coexisting medication treatment: no change of medication treatment during the study |
|
| Interventions | Exercise group (N = 25)
Control group (N = 27)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0 , final point = 16 Major outcomes
Minor outcomes |
|
| Notes | Number of missing participant: 5 (9%) dropouts or withdrawals: n = 5 (exercise group = 4, control group = 1) adverse events:
adverse effect: not reported sample size calculation: not reported Funding source: supported by Nathonal Health Research and development programme, Health and Welfare Canada FGrant number 6606‐2385‐43 Protocol registration number not found Declaration of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: sufficient information not provided Quote: "fifty‐three patients with ankylosing spondylitis (AS) were randomly allocated". |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: modified intention‐to‐treat analysis. Unbalanced rate of dropouts (exercise group 15%; control group 4%) as 1 subject was missing for the final analysis. Reasons for dropouts were unclear. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported. Major and minor outcomes were specified. Outcomes listed in the method section were all reported in the results section. |
| Other bias | Unclear risk | Comment: small number of participants, no information on baseline disease severity between the 2 groups, adherence and compliance to treatments was not monitored. No power sample size calculation. Conflicts of interest were not declared |
Lim 2005.
| Methods | RCT with two groups No intention‐to‐treat analysis |
|
| Participants | Location: Korea Randomised: 58 Analysed: 50 Age: 28 years Gender: 78% men Recruited: from Rheumatism Center at the University Medical Center and home, monocentre Inclusion criteria: patients with AS (a) an outpatient without complications, (b) sedentary, as defined by a lack of regular exercise during the previous 6 months, (c) able to understand the content of questionnaires and experimental schedules, (d) had no changes in their current prescription medication, and (e) were classified in the functional class II for AS Exclusion criteria: not reported Severity of the disease: classified as functional class II Disease duration: 9 years Coexisting medication treatment: no change of medication during the study |
|
| Interventions | Exercise group (N = 25)
Control group (N = 25)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 8 Major outcomes
Minor outcomes
|
|
| Notes | Unclear if participants in the control group could practice community‐based exercises Number of missing participants: 8 (14%) Dropouts or withdrawals: n = 0 Adverse events: n = 0 (0%) Averse effects: not reported Funding source: not reported Protocol number registration not found Declaration of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: no clear information provided in the report Quote: "Subjects were randomly assigned to either an exercise group or a wait‐list control group." |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: participants were not blinded Quote: "The subjects were informed about the exercise therapy when we explained the nature of AS and procedures for the study." |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: no intention‐to‐treat analysis; 8 dropouts; no imputation technique was used |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol reported; outcomes listed in the method section were all reported in the results section; no major outcomes specified |
| Other bias | Unclear risk | Comment: small number of subjects; unclear description of the intervention; no power sample calculation; multiple outcomes from comparisons with no inflation risk alpha correction; funding and conflict of interest were not declared; attendance and compliance were not reported |
Masiero 2011.
| Methods | RCT with three groups No intention‐to‐treat analysis |
|
| Participants | Location: Italy Randomised: 45 Analysed: 42 Age: 47 years Gender: 79% men Recuited: from outpatient of a rheumatology hospital department Inclusion criteria: treated by anti‐TNF medication (infliximad, etanercept, or adalimumad) for a least 9 months, no major change of the clinical status in the last 3 months, aged between 18 and 65 years, diagnosis of AS on the modified New York criteria, no severe disease associated Exclusion criteria: suffering from complete spine ankylosing, being involved in other rehabilitation treatments, failure to take part in the study, variations in standard biological therapy regimens during the study Severity and duration of the disease: the mean disease duration was 9 years Coexisting medication treatment: NSAIDS (0%) |
|
| Interventions | Exercise group
Control group
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 8, follow‐up = 16 Major outcomes
Minor outcomes |
|
| Notes | Unclear if participants in the control group could practice community‐based exercises Number of missing participants: 3 (7%) Dropouts or withdrawals: n = 3 (7%) two withdraws and one dropout Adverse events: not reported Averse effects: not reported Funding source: not reported Registration number: protocol not found Declaration of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: no clear information provided in the report Quote: "Subjects were randomly allocated to attend either rehabilitation therapy." |
| Allocation concealment (selection bias) | Low risk | Quote: "Casual randomisation using a statistical programme was carried out by a rheumatologist not involved in the study evaluation or rehabilitation intervention" |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: not described, but it's unlikely that personnel were blinded to the treatment allocated |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: few balanced dropouts (2 and 1 in the groups). May have a minor influence on the estimates effect size |
| Selective reporting (reporting bias) | Unclear risk | Comment: outcomes listed in the method section were all reported in the results section. No protocol registration was found. No major outcomes specified |
| Other bias | Unclear risk | Comment: attendance and compliance were not reported; small sample size; baseline performances were similar for major outcomes; no power sample calculation; funding and conflict of interest were not stated |
Rodriguez‐Lozano 2013.
| Methods | RCT with two groups No intention‐to‐treat analysis |
|
| Participants | Location: Spain Randomised: 802 Analysed: 756 Age: 45 years Gender: 72% men Recuited: from outpatient of rheumatology services, multicentre (24 hospitals) Inclusion criteria: aged 18 to 70 years, diagnosis of AS on the modified New York criteria Exclusion criteria: suffered from severe form of AS with loss of motion, form of AS or coexistent disease with a contraindication for exercises Severity and duration of the disease: the mean duration of disease was 17 years, low to moderate disease activity Coexisting medication treatment: NSAIDS (75%), corticosteroids (4%), biologic agents (39%), analgesics (11.5%), Sulfasalazine (9%) |
|
| Interventions | Exercise group (N = 381)
Control group (N = 375)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 24 Major outcomes
Minor outcomes:
|
|
| Notes | Number of missing participants: 57 (7%) Dropouts or withdrawals: n = 46 (6%) "failed to attend the final visit" Adverse events: not reported Averse effects: not reported Funding source: from the Spanish Society of Rheumatology Registration number: protocol not found Declaration of interest: authors declared no conflict of interest |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The central agency was located in Madrid. A random sequence for the allocation was generated. It was sent to every hospital in an opaque envelope". |
| Allocation concealment (selection bias) | Low risk | Comment: sealed envelopes with assignment code were used Quote: "concealment of allocation was assured by opening an opaque envelope which contained the assignation number"... "contained a consecutive number". |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: no intention‐to‐treat analysis; missing data; no imputation technique was used; possible influence on treatment effect |
| Selective reporting (reporting bias) | Unclear risk | Comment: outcomes listed in the method section were all reported in the results section; no protocol registration was found; no major outcomes specified |
| Other bias | Low risk | Comment: convenient number of subjects included in the study; adherence to treatments was monitored; power sample size calculation was reported; size effect calculation adjusted on baseline variables |
Souza 2017.
| Methods | RCT with two groups intention‐to‐treat analysis |
|
| Participants | Location: Brazil Randomised: 60 Analysed: 60 Age: 44 years Gender: 73% men Recruited: outpatient clinic of a university hospital Inclusion criteria: diagnosis of AS on the modified New York criteria, a Steinbrocker functional class of I to II, on stable medication, disease‐modifying anti‐rheumatic drug (DMARDS) for at least 3 months, and NSAIDs or corticoids (or both) for at least 4 weeks. If not using medication for AS, should be medication‐free for at least 3 months Exclusion criteria: uncontrolled hypertension, history of coronary artery disease, history of syncope or arrhythmias induced by exercise, decompensated diabetes mellitus, severe psychiatric disorders, fibromyalgia, a more disabling condition than AS, a history of regular exercise of at least 30 min, two times a week, in the last 3 months, any condition that could prevent the patient from performing exercises in the last three months Severity and duration of the disease: a Steinbrocker functional class of I to II; mean time since diagnosis of 9.2 years Coexisting medication treatment: NSAIDS (27%), biologic agents (38%), DMARDS (17%), Sulfasalazine (12%), no medication (8%) |
|
| Interventions | Exercise group (N = 27)
Control group (N = 28)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 16 Major outcomes
Minor outcomes
|
|
| Notes | Number of missing participants: none Dropouts or withdrawals: 5 participants dropped out Adverse events: not explicitly reported Averse effects: not explicitly reported Sample size calculation: 27 subjects per arm Funding source: granted by a research foundation (# 2011/03459‐9) Declaration of interest: authors declared no conflict Protocol registration number: NCT0351311 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computer‐generated randomisation list was utilised to randomly allocate patients into intervention (IG) or control (CG) groups". |
| Allocation concealment (selection bias) | Unclear risk | incomplete information provided Quote: "a concealed randomization with an opaque, sealed envelope" |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded Quote: "The evaluations were performed by a blinded evaluator " |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: intention‐to‐treat analysis; technique of imputation – the last evaluation carried forward; reasons for dropouts were not clearly reported |
| Selective reporting (reporting bias) | Low risk | Comment: protocol number registration was provided; no difference was found between the protocol and the published report; all the outcomes pre‐specified were reported |
| Other bias | Unclear risk | Comment: attendance and compliance not reported; no systematic reporting of adverse events; no outcomes reported at medium‐ and long‐term follow‐up; power sample size calculation; no baseline adjustment of data |
Sveaas 2014.
| Methods | RCT with two groups No intention‐to‐treat |
|
| Participants | Location: Norway Randomised: 28 Analysed: 24 Age: 48 years Gender: 50% men Recruited: from Diakonhjemmet Hospital, monocentre Inclusion criteria: axSpA according to the Assessment of SpA International Society (ASAS) classification criteria; age 18 to 70 years; no change in TNF inhibitor use during the last 3 months, moderate to high disease activity (Bath AS Disease Activity Index (BASDAI)), did not perform regular endurance or strength exercise during the last year (1 hour per week) Exclusion criteria: established CVD, other comorbidity involving reduced exercise capacity, inability to participate in weekly exercise sessions in Oslo, pregnancy Severity and duration of the disease: mean ASDAS = 2.6, mean duration = 25 years Coexisting medication treatment: NSAIDS (75%), TNF inhibitor (29%) |
|
| Interventions | Exercise group (N =13)
Control group (N = 15)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 12 Major outcomes
Minor outcomes
|
|
| Notes | Number of missing participant: 4 (14%) Dropouts or withdrawals: n = 4 (14%) Adverse events: n = 3 (10%) in the exercise group Averse effects: n = 1 (4%) in the exercise group, because intervention was physically challenging and time consuming Funding source: by the Norwegian Foundation for Postgraduate Physiotherapists Protocol registration number: NCT01436942 Declaration of interest: authors declared they had no competing interests |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Allocation to EG or CG followed a computer‐generated randomisation list" |
| Allocation concealment (selection bias) | Unclear risk | Comment: incomplete description of the allocation procedure Quote: the group assignment was concealed in numbered envelopes, and revealed consecutively after baseline testing |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded Quote: "The assessors were blinded for group assignment". |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: per‐protocol analysis; no imputation technique was used; possible influence on treatment effect |
| Selective reporting (reporting bias) | High risk | Comment: a protocol registration number was provided. Different outcomes were mentioned in the protocol (generic General Health Questionnaire (GHQ‐12); international Physical Activity Questionnaire short version (IPAQ‐s), which were not reported in the published article. There is a possible risk of bias. |
| Other bias | Unclear risk | Comment: limited number of subjects per group; size effect estimates adjusted for baseline performance (covariance analysis); no power sample calculation; multiple outcomes for comparisons with no inflation risk alpha correction |
Sweeney 2002.
| Methods | RCT with two groups No intention‐to‐treat analysis |
|
| Participants | Location: United Kingdom Randomised: 200 Analysed: 155 Age: 47 years Gender: 69% men Recruited: from members of outpatient service or National Ankylosing Spondylitis Society (NASS) Inclusion criteria: 16 to 65 years, outpatients of the RNHRD or members of the National Ankylosing Spondylitis Society (NASS) Exclusion criteria: not reported Severity and duration of the disease: the duration of disease was 21 years Coexisting medication treatment: non reported |
|
| Interventions | Exercise group (N = 75)
Control group (N = 80)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 24 Major outcomes
Minor outcomes
|
|
| Notes | Number of missing participant: 45 (22%) Dropouts or withdrawals: n = 45 Adverse events: not reported Averse effects: not reported Funding source: supported by grants from BUPA, National Ankylosing Spondylitis Society, John Coates Charitable Trust, and Col. W.W. Pilkington Trust Protocol registration number not found Declaration of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: incomplete description Quote: "The selected patients were then randomly assigned to 2 groups". |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: unsupervised home delivery; personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: data were missing; no ITT analysis; can have a possible influence on the estimates of effect size |
| Selective reporting (reporting bias) | Unclear risk | Comment: no registration protocol number reported; major and minor outcomes were not specified; outcomes listed in the methods section were all reported in the results section; reasons for dropouts were not reported |
| Other bias | Unclear risk | Comment: no sample size calculation; sample size > 30; multiple statistical comparisons without corrections; unclear if it could have an influence on the estimates of effect size; adverse effects were not monitored or reported; funding and conflict of interest were not stated |
Widberg 2009.
| Methods | RCT with 2 groups intention‐to‐treat analysis |
|
| Participants | Location: Sweden Randomised: 32 Analysed: 32 Age: 36 years Gender: 100% men Recruited: at Karolinska University Hospital, monocentre Inclusion criteria: diagnosis of ankylosing spondylitis according to the modified New York criteria, 20 to 60 years old, and had stable pharmacological treatment with non‐steroidal anti‐inflammatory drugs and disease‐modifying anti‐rheumatic drugs Exclusion criteria: inflammatory disease activity, which could be subject to pharmacological changes, radiological ossification between the thoracic vertebrae, concomitant effects of other severe illnesses Severity and duration of the disease: duration of disease (median) = 2.5 to 3.5 years Coexisting medication treatment: NSAIDS (75%), and DMARDS (44%) |
|
| Interventions | Exercise group (N = 16)
Control group (N = 16)
Adherence
|
|
| Outcomes | Time points (weeks): baseline = 0, final point = 8 Major outcomes
Minor outcomes |
|
| Notes | Number of missing participants: 0 (0%) Dropouts or withdrawals: n = 0 Adverse events: not reported Averse effects: not reported Funding source: Swedish Rheumatism Association and Nacka Rehab centre Protocol registration number not found Declaration of interest: authors declared no conflict of interest |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: adequate method of random sequence generation Quote: "The participants were assigned randomly into two groups using random number table by the researcher other than the one who performed the evaluation throughout the study." |
| Allocation concealment (selection bias) | Unclear risk | Comment: the study did not provide information about allocation concealment |
| Blinding of participants (subjective outcome) | High risk | Comment: not described, but it's unlikely that participants were blinded to the treatment allocated |
| Blinding of personnel | High risk | Comment: personnel unblinded |
| Blinding of outcome assessment (subjective) | High risk | Comment: participants were the assessors; they were unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all the patients randomised were analysed |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol registration number reported; outcomes listed in the methods section were all reported in the results section; safety was not reported as an outcome; major outcomes were specified |
| Other bias | Unclear risk | Comment: small sample size; baseline performances were similar for major outcomes; rates of medications did not differ between the two groups; no power sample calculation |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ciprian 2013 | Does not meet the intervention inclusion criteria. The exercise programme was combined with different cointerventions: thermal water and mud pack |
| Colina 2009 | Controlled study with no randomisation |
| Durmus 2009 | Controlled study with no randomisation |
| Gunay 2012 | A quasi‐randomised study: all patients were randomised with their outpatient clinic registration numbers |
| Karahan 2016 | Does not meet the intervention inclusion criteria. The experimental intervention included recreational physical activities |
| Lee 2008 | Controlled study with no randomisation |
| Masiero 2015 | Controlled study with no randomisation |
Characteristics of studies awaiting assessment [ordered by study ID]
Mesquita 2014.
| Methods | RCT |
| Participants | Patients with ankylosing spondylitis |
| Interventions | Home‐based exercise programme; no information on control intervention |
| Outcomes | BASDAI, BASFI, BASMI, WHOQOL‐bref; measurements at baseline and 10 weeks after |
| Notes | Abstract of congress; incomplete data; we contacted the authors but they did not respond |
Sveeas 2018.
| Methods | RCT |
| Participants | Patients with axial spondyloarthritis |
| Interventions | Exercise group (EG), which performed cardiorespiratory and strength exercises, or a control group (CG), which received treatment as usual |
| Outcomes | Emotional distress, fatigue, and ability to do a full day's activities, measurements at baseline and 12 weeks after |
| Notes | Same authors as Sveaas 2014; it might be the same study with different outcomes; awaiting confirmation from authors |
Characteristics of ongoing studies [ordered by study ID]
ChiCTR‐TRC‐14004650.
| Trial name or title | The effect of traditional exercise 'Baduanjin' for physical functioning of ankylosing spondylitis: a randomised, controlled, prospective study |
| Methods | Randomised parallel control |
| Participants | experimental group: 30; control group: 30 |
| Interventions | experimental group: Baduanjin exercise; control group: maintain present treatment and lifestyle |
| Outcomes | BASDAI index; BASMI index; BASFI index; HAQ‐9; patients global |
| Starting date | 16 May 2014 |
| Contact information | 77612802@qq.com |
| Notes | Study recruiting; apps.who.int/trialsearch/Trial2.aspx?TrialID=ChiCTR‐TRC‐14004650 |
NCT02098694.
| Trial name or title | Physiotherapy‐led outpatient clinic for patients with spondyloarthritis |
| Methods | RCT |
| Participants | outpatient with spondyloarthritis |
| Interventions | home‐exercises (experimental) versus usual care (control) |
| Outcomes | BASMI, BASFI, ASDAS. measurements at baseline and at 8 months |
| Starting date | June 2014 |
| Contact information | Ann‐Katrin Stensdotter, Norwegian University of Science and Technology |
| Notes | Study completed. NCT02098694 |
Differences between protocol and review
We did not perform contour‐enhanced funnel plots to assess the presence of small‐study effects because the required statistical conditions were not met.
We did not perform subgroup analysis to explore a relationship between the modalities of exercises, participant characteristics, or pharmacological treatments because of insufficient data. Meta‐regression (i.e. dose–effect relationship) was also not possible because of the small number of included studies for each reported outcome.
The protocol stated that we would attempt to perform a sensitivity analysis to explore how the results of meta‐analysis might be affected by including only studies at low risk of bias. However, because all the identified studies were at high risk of bias, we did not perform the analysis.
We used Peto odds ratios (Peto ORs) for calculating AEs because too few events were reported in each group (Higgins 2011b).
We planned in the protocol to report outcome assessments from the included studies in three time frames: at completion (end of intervention), medium‐term follow‐up (6 to 12 months), and long‐term follow‐up (> 12 months). We revised the time frames in the review to: at completion (end of intervention), medium‐term (less than six months after completion of exercise), and long‐term (6 months and more after completion of exercise) follow‐up.
In the protocol, we named the outcome to measure the patient‐assessment of disease activity, 'Patient global assessment of health status'. We changed the name to 'Patient global assessment of disease activity' in the review
François Rannou and Alexandra Roren were added as authors.
Contributions of authors
JPR, MMLC, CP, SP, TD, and IB contributed to the development of the protocol. All authors were involved in the conception and interpretation of the review.
Sources of support
Internal sources
-
French School of Public Health (EHESP) Paris Sorbonne Cité, France.
in‐kind support
-
Centre de Recherche Inserm Epidémiologie et Statistique Paris Sorbonne Cité (CRESS), France.
in‐kind support
-
Hôpital Hôtel‐Dieu, APHP, France.
in‐kind support
External sources
No sources of support supplied
Declarations of interest
JPR: none known
MMLC: none known
CP: received consultancy remuneration from Merz, Novartis, Ipsen, and support for travel from Merz; received remuneration from BMS for participating in Delphi study to develop a questionnaire on fear, beliefs, and expectations regarding pain induced by physiotherapy, and from Pfizer for the analysis of a national survey in 2010‐2011. Pfizer, BMS, Roche contributed to expenses to conferences (EULAR 2011 and 2012, SFR 2012).
AR: none known
FR: declares competing interest outside the submitted work: board membership of Pfizer, Sanofi Aventis, Pierre Fabre, Expansciences and Thuasne. Consultancy for Genevrier and Bayer. Payment for lectures from Thuasne, Grünenthal and IPSEN.
TD: association Robert Debré provided a grant for master studies; he works as a physiotherapist.
IB: is a co‐convener of the Bias Methods Group (BMG) of the Cochrane Collaboration and the French satellite co‐ordinator of the Cochrane Musculoskeletal Review Group (CMSG)
Edited (no change to conclusions)
References
References to studies included in this review
Altan 2012 {published data only}
- Altan L, Korkmaz N, Dizdar M, Yurtkuran M. Effect of Pilates training on people with ankylosing spondylitis. Rheumatology International 2012 Jul;32(7):2093‐9. [PUBMED: PMID: 21499876] [DOI] [PubMed] [Google Scholar]
Dönmez 2014 {published data only}
- Dönmez U, Ozturk C, Kocanaogullari H, Gucenmez S, Hepguler S. Do physical therapy modalities have additional benefit over exercise therapy in the management of ankylosing spondylitis? A randomized controlled trial. Annals of the Rheumatic Diseases 2014;73(Suppl2):727. [SAT0369] [Google Scholar]
Gallinaro 2016 {published data only}
- Gallinaro AL. Effects of Two Exercise Therapy Programs with and without Elastic Resistance in Ankylosing Spondylitis Patients [Doctoral Thesis]. São Paulo (Brazil): Faculdade de Medicina, Universidade de São Paulo, 2016. [USP/FM/DBD‐199/16; www.teses.usp.br/teses/disponiveis/5/5169/tde‐04112016‐150051/fr.php] [Google Scholar]
- NCT01690273. Exercise therapy program in ankylosing spondylitis patients. clinicaltrials.gov/ct2/show/NCT01690273 (first received 21 September 2012).
Garcia 2015 {published data only}
- Fernández García R, Sánchez Sánchez L de C, López Rodríguez M del M, Sánchez Granados G. Effects of an exercise and relaxation aquatic program in patients with spondyloarthritis: a randomized trial. Medicina Clínica (Barc) 2015 Nov 6;145(9):380‐4. [PUBMED: PMID: 25639496] [DOI] [PubMed] [Google Scholar]
Ince 2006 {published data only}
- Ince G, Sarpel T, Durgun B, Erdogan S. Effects of a multimodal exercise program for people with ankylosing spondylitis. Physical Therapy 2006;Jul; 86(7):924‐35. Erratum in: Physical Therapy. 2006 Oct;86(10):1452. [PUBMED: PMID: 16813473] [PubMed] [Google Scholar]
Kjeken 2013 {published data only}
- Kjeken I, Bø I, Rønningen A, Spada C, Mowinckel P, Hagen KB, et al. A three‐week multidisciplinary in‐patient rehabilitation programme had positive long‐term effects in patients with ankylosing spondylitis: randomized controlled trial. Journal of Rehabilitation Medicine 2013;Mar; 45(3):260‐7. [PUBMED: PMID: 23138412] [DOI] [PubMed] [Google Scholar]
Kraag 1990 {published data only}
- Kraag G, Stokes B, Groh J, Helewa A, Goldsmith C. The effects of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis‐a randomized controlled trial. The Journal of Rheumatology 1990;Feb; 17(2):228‐33. [PUBMED: PMID:2181127] [PubMed] [Google Scholar]
- Kraag G, Stokes B, Groh J, Helewa A, Goldsmith CH. The effects of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis – an 8‐month follow‐up. The Journal of Rheumatology 1994 Feb;21(2):261‐3. [PUBMED: PMID:8182634] [PubMed] [Google Scholar]
Lim 2005 {published data only}
- Lim HJ, Moon YI, Lee MS. Effects of home‐based daily exercise therapy on joint mobility, daily activity, pain, and depression in patients with ankylosing spondylitis. Rheumatology International 2005;Apr; 25(3):225‐9. [PUBMED: PMID: 15650833] [DOI] [PubMed] [Google Scholar]
Masiero 2011 {published data only}
- Masiero S, Bonaldo L, Pigatto M, Lo Nigro A, Ramonda R, Punzi L. Rehabilitation treatment in patients with ankylosing spondylitis stabilized with tumor necrosis factor inhibitor therapy: a randomized controlled trial. The Journal of Rheumatology 2011 Jul;38(7):1335‐42. [PUBMED: PMID: 21459942] [DOI] [PubMed] [Google Scholar]
Rodriguez‐Lozano 2013 {published data only}
- Rodríguez‐Lozano C, Juanola X, Cruz‐Martínez J, Peña‐Arrébola A, Mulero J, Gratacós J, Collantes E, Spondyloarthropathies Study Group of the Spanish Society of Rheumatology. Outcome of an education and home‐based exercise programme for patients with ankylosing spondylitis: a nationwide randomized study. Clinical and Experimental Rheumatology 2013 Sep‐Oct;31(5):739‐48. [PUBMED: PIMD: 23899791] [PubMed] [Google Scholar]
Souza 2017 {published data only}
- Souza MC, Jennings F, Morimoto H, Natour J. Swiss ball exercises improve muscle strength and walking performance in ankylosing spondylitis: a randomized controlled trial. Revista Brasileira de Reumatologia [English edition] 2017 Jan ‐ Feb;57(1):45‐55. [PUBMED: PMID: 28137402] [DOI] [PubMed] [Google Scholar]
Sveaas 2014 {published data only}
- Sveaas SH, Berg IJ, Provan SA, Semb AG, Hagen KB, Vøllestad N, et al. Efficacy of high intensity exercise on disease activity and cardiovascular risk in active axial spondyloarthritis: a randomized controlled pilot study. PLoS One 2014;Sep 30; 9(9):e108688. [PUBMED: PMID: 25268365] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sweeney 2002 {published data only}
- Sweeney S, Taylor G, Calin A. The effect of a home based exercise intervention package on outcome in ankylosing spondylitis: a randomized controlled trial. The Journal of Rheumatology 2002;Apr; 29(4):763‐6. [PUBMED: PMID: 11950019] [PubMed] [Google Scholar]
Widberg 2009 {published data only}
- Widberg K, Karimi H, Hafström I. Self‐ and manual mobilization improves spine mobility in men with ankylosing spondylitis – a randomized study. Clinical Rehabilitation 2009;Jul; 23(7):599‐608. [PUBMED: PMID: 19403551] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Ciprian 2013 {published data only}
- Ciprian L, Lo Nigro A, Rizzo M, Gava A, Ramonda R, Punzi L, et al. The effects of combined spa therapy and rehabilitation on patients with ankylosing spondylitis being treated with TNF inhibitors. Rheumatology International 2013, Jan;33(1):241‐5. [PUBMED: PMID: 21947374] [DOI] [PubMed] [Google Scholar]
Colina 2009 {published data only}
- Colina M, Ciancio G, Garavini R, Conti M, Trotta F, Govoni M. Combination treatment with etanercept and an intensive spa rehabilitation program in active ankylosing spondylitis. International Journal of Immunopathology and Pharmacology 2009 Oct‐Dec;22(4):1125‐9. [PUBMED: PMID: 20074478] [DOI] [PubMed] [Google Scholar]
Durmus 2009 {published data only}
- Durmus D, Alayli G, Cil E, Canturk F. Effects of a home‐based exercise program on quality of life, fatigue, and depression in patients with ankylosing spondylitis. Rheumatology International 2009 Apr;29(6):673‐7. [PUBMED: PMID: 18985351] [DOI] [PubMed] [Google Scholar]
Gunay 2012 {published data only}
- Gunay MO, Bal S, Bayram KB, Harman E, Dalgic EE, Kocyitit H, et al. The effect of breathing and posture exercise on the clinical, functional status and disease related quality of life in patients with ankylosing spondylitis. Medicine Science 2012;1(2):103‐17. [10.5455/medscience.2012.01.103‐117] [Google Scholar]
Karahan 2016 {published data only}
- Karahan AY, Tok F, Yildirim P, Ordahan B, Turkoglu G, Sahin N. The effectiveness of exergames in patients with ankylosing spondylitis: a randomized controlled trial. Advances in Clinical and Experimental Medicine 2016;25(5):931‐6. [DOI: 10.17219/acem/32590] [DOI] [PubMed] [Google Scholar]
Lee 2008 {published data only}
- Lee EN, Kim YH, Chung WT, Lee MS. Tai chi for disease activity and flexibility in patients with ankylosing spondylitis – a controlled clinical trial. Evidence‐based Complementary and Alternative Medicine: ECAM 2008 Dec;5(4):457‐62. [PUBMED: PMID: 18955296] [DOI] [PMC free article] [PubMed] [Google Scholar]
Masiero 2015 {published data only}
- Masiero S. A controlled clinical trial on balance parameters improvement after physical rehabilitation in ankylosing spondylitis. Archives of Physical Medicine and Rehabilitation 2015;10:e91. [CN‐01126811] [Google Scholar]
References to studies awaiting assessment
Mesquita 2014 {published data only}
- Mesquita C, Lopes S, Moreira EM, Lopes P, Cameiro A, Silva D, et al. Effect of home exercise program in quality of life in patients with ankylosing spondylitis. Annals of the Rheumatic Diseases 2014;73(suppl 1):A41. [DOI: 10.1136/annrheumdis-2013-205124.93] [DOI] [Google Scholar]
Sveeas 2018 {published data only}
- Sveaas SH, Berg IJ, Fongen C, Provan SA, Dagfinrud H. High‐intensity cardiorespiratory and strength exercises reduced emotional distress and fatigue in patients with axial spondyloarthritis: a randomized controlled pilot study.. Scandinavian Journal of Rheumatology 2018 Mar;47(2):117‐21. [DOI: 10.1080/03009742.2017.1347276; PUBMED: PMID: 28891743] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
ChiCTR‐TRC‐14004650 {published data only}
- ChiCTR‐TRC‐14004650. The effect of traditional exercise "Baduanjin" for physical functioning of ankylosing spondylitis: a randomized, controlled, prospective study. www.chictr.org.cn/hvshowproject.aspx?id=10477 (last refreshed 02 May 2015).
NCT02098694 {published data only}
- NCT02098694. Physiotherapy‐led outpatient clinic for patients with spondyloarthritis. clinicaltrials.gov/ct2/show/NCT02098694 (first posted 28 March 2014).
Additional references
Abenhaim 2000
- Abenhaim L, Rossignol M, Valat JP, Nordin M, Avouac B, Blotman F, et al. The role of activity in the therapeutic management of back pain. Report of the International Paris Task Force on Back Pain. Spine 2000;25(4 Suppl):1S‐33S. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Arem 2015
- Arem H, Moore SC, Patel A, Hartge P, Berrington de Gonzalez A, Visvanathan K, et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose‐response relationship. JAMA Internal Medicine 2015 Jun;175(6):959‐67. [DOI: 10.1001/jamainternmed.2015.0533; PUBMED: PMID: 25844730] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baraliakos 2005
- Baraliakos X, Landewé R, Hermann KG, Listing J, Golder W, Brandt J, et al. Inflammation in ankylosing spondylitis: a systematic description of the extent and frequency of acute spinal changes using magnetic resonance imaging. Annals of the Rheumatic Diseases 2005;64(5):730‐4. [PUBMED: PMC1755467] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baraliakos 2012
- Baraliakos X, Berg R, Braun J, Heijde D. Update of the literature review on treatment with biologics as a basis for the first update of the ASAS/EULAR management recommendations of ankylosing spondylitis. Rheumatology (Oxford) 2012;51(8):1378‐87. [PUBMED: 22427410] [DOI] [PubMed] [Google Scholar]
Boonen 2004
- Boonen A, Tubergen A, Linden S, Mihai C, Ottawa Methods Group. Spondyloarthropathies. In: Tugwell P, Shea B, Boers M, Brooks P, Simon LS, Strand V, et al. editor(s). Evidence‐Based Rheumatology. London: BMJ Books, 2004:393‐429. [Google Scholar]
Boonen 2006
- Boonen A, Linden SM. The burden of ankylosing spondylitis. The Journal of Rheumatology 2006;78(Suppl):4‐11. [PUBMED: 17042055.] [PubMed] [Google Scholar]
Bouchard 2012
- Bouchard C, Blair S, Haskell W. Physical Activity and Health. Champaign, IL: Human Kinetics, Inc, 2012. [Google Scholar]
Boutron 2007
- Boutron I, Guittet L, Estellat C, Moher D, Hróbjartsson A, Ravaud P. Reporting methods of blinding in randomized trials assessing non pharmacological treatments. PLoS Med 2007 Feb;4(2):e61. [PUBMED: PMID: 17311468] [DOI] [PMC free article] [PubMed] [Google Scholar]
Braun 2003
- Braun J, Pham T, Sieper J, Davis J, Linden S, Dougados M, et al. International ASAS consensus statement for the use of anti‐tumour necrosis factor agents in patients with ankylosing spondylitis. Annals of the Rheumatic Diseases 2003;62(9):817‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Braun 2007
- Braun J, Sieper J. Ankylosing spondylitis. Lancet 2007;369(9570):1379‐90. [DOI] [PubMed] [Google Scholar]
Braun 2010
- Braun J, Berg R, Baraliakos X, Boehm H, Burgos‐Vargas R, Collantes‐Estevez E. 2010 update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis. Annals of the Rheumatic Diseases 2011;70(6):896‐904. [PUBMED: PMC3086052] [DOI] [PMC free article] [PubMed] [Google Scholar]
Buchbinder 2015
- Buchbinder R, Golmohammadi K, Johnston RV, Owen RJ, Homik J, Jones A, et al. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database of Systematic Reviews 2015, Issue 4. [CENTRAL: CD006349; DOI: 10.1002/14651858.CD006349.pub2] [DOI] [PubMed] [Google Scholar]
Button 2013
- Button KS, Ioannidis JP, Mokrysz C, Nosek BA, Flint J, Robinson ES, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nature Reviews. Neuroscience 2013 May;14(5):365‐76. [PUBMED: PMID: 23571845] [DOI] [PubMed] [Google Scholar]
Cates 2008 [Computer program]
- Cates CD. Visual Rx version 3.0. London (UK): Chris Cates, (accessed 16 July 2014).
Cohen 2006
- Cohen JD, Cunin P, Farrenq V, Oniankitan O, Carton L, Chevalier X, et al. Estimation of the Bath Ankylosing Spondylitis Disease ActivityIndex cutoff for perceived symptom relief in patients with spondyloarthropathies. Journal of Rheumatology 2006 Jan;33(1):79‐81. [PubMed] [Google Scholar]
Dagfinrud 2005
- Dagfinrud H, Kjeken I, Mowinckel P, Hagen KB, Kvien TK. Impact of functional impairment in ankylosing spondylitis: impairment, activity limitation, and participation restrictions. Journal of Rheumatology 2005;32(3):516‐23. [PubMed] [Google Scholar]
Dagfinrud 2008
- Dagfinrud H, Kvien TK, Hagen KB. Physiotherapy interventions for ankylosing spondylitis. Cochrane Database of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD002822.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dagfinrud 2011
- Dagfinrud H, Halvorsen S, Vøllestad NK, Niedermann K, Kvien TK, Hagen KB. Exercise programs in trials for patients with ankylosing spondylitis: do they really have the potential for effectiveness?. Arthritis Care & Research 2011 Apr;63(4):597‐603. [PUBMED: PMID: 21452270] [DOI] [PubMed] [Google Scholar]
Dean 2014
- Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford) 2014;53(4):650‐7. [PUBMED: 24324212] [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Deeks 2019
- Deeks JJ, Higgins JPT, Altman DG. Chapter 10: Analysing data and undertaking meta‐analyses. Cochrane Handbook for Systematic Reviews of Interventions. Version 6. Draft version (29 january 2019). Available from handbook.cochrane.org.
Dougados 2011
- Dougados M, Baeten D. Spondyloarthritis. Lancet 2011;377(9783):2127‐37. [DOI] [PubMed] [Google Scholar]
Dubey 2008
- Dubey SG, Leeder J, Gaffney K. Physical therapy in anti‐TNF treated patients with ankylosing spondylitis. Rheumatology (Oxford) 2008 Jul;47(7):1100‐1. [PUBMED: PMID: 18495822] [DOI] [PubMed] [Google Scholar]
Fernández‐de‐Las‐Peñas 2005
- Fernández‐de‐Las‐Peñas C, Alonso‐Blanco C, Morales‐Cabezas M, Miangolarra‐PageJC. Two exercise interventions for the management of patients with ankylosing spondylitis: a randomized controlled trial. American Journal of Physical Medicine & Rehabilitation 2005 Jun;84(6):407‐19. [PUBMED: 15905654] [DOI] [PubMed] [Google Scholar]
Giannotti 2014
- Giannotti E, Trainito S, Arioli G, Rucco V, Masiero S. Effects of physical therapy for the management of patients with ankylosing spondylitis in the biological era. Clinical Rheumatology 2014 Sep;33(9):1217‐30. [PMID: 24797772] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Hagen 2012
- Hagen KB, Dagfinrud H, Moe RH, Østerås N, Kjeken I, Grotle M, et al. Exercise therapy for bone and muscle health: an overview of systematic reviews. BMC Medicine 2012 Dec;19(10):167. [PUBMED: PMC3568719] [DOI] [PMC free article] [PubMed] [Google Scholar]
Haroon 2013
- Haroon N, Inman RD, Learch TJ, Weisman MH, Lee M, Rahbar MH, et al. The impact of tumor necrosis factor α inhibitors on radiographic progression in ankylosing spondylitis. Arthritis and Rheumatism 2013;65(10):2645‐54. [PUBMED: 23818109] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hayden 2012
- Hayden JA, Cartwright J, Tulder MW, Malmivaara A. Exercise therapy for chronic low back pain. Cochrane Database of Systematic Reviews 2012, Issue 4. [DOI: 10.1002/14651858.CD009790] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JPT, Deek JJ, Altman DG. Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011c
- Higgins JPT, Deeks JJ. editor(s). Chapter 7: Selecting studies and collecting data. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org. The Cochrane Collaboration.
Hoffmann 2014
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon‐Woods M, McCulloch P, WyattJC, Chan AW, Michie S. Better reporting of interventions: template forintervention description and replication (TIDieR) checklist and guide. BMJ 2014 Mar 7;348:g1687. [10. 1136/bmj. g1687] [DOI] [PubMed] [Google Scholar]
Hozo 2005
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical Research Methodology 2005 Apr;20(5):13. [PUBMED: PMID: 15840177] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ioannidis 2007a
- Ioannidis JP, Patsopoulos NA, Evangelou E. Uncertainty in heterogeneity estimates in meta‐analyses. BMJ 2007;336(7626):914‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jacques 2014
- Jacques P, Lambrecht S, Verheugen E, Pauwels E, Kollias G, Armaka M, et al. Proof of concept: enthesitis and new bone formation in spondyloarthritis are driven by mechanical strain and stromal cells. Annals of the Rheumatic Diseases 2014 Feb;73(2):437‐45. [PUBMED: PMID: 23921997] [DOI] [PubMed] [Google Scholar]
Kujala 2009
- Kujala UM. Evidence on the effects of exercise therapy in the treatment of chronic disease. British Journal of Sports Medicine 2009 Aug;43(8):550‐5. [PUBMED: 19406731] [DOI] [PubMed] [Google Scholar]
Kunutsor 2018
- Kunutsor S, Leyland S, Skelton D, James L, Cox M, Gibbons N, Whitney J, Clark E. Adverse events and safety issues associated with physical activity and exercise for adults with osteoporosis and osteopenia: A systematic review of observational studies and an updated review of interventional studies. Journal of Fraitly, Sarcopenia & Frails 2018 December;3(4):155‐178. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Liang 2015
- Liang H, Li WR, Zhang H, Tian X, Wei W, Wang CM. Concurrent intervention with exercises and stabilized tumor necrosis factor inhibitor therapy reduced the disease activity in patients with ankylosing spondylitis: a meta‐analysis. Medicine (Baltimore) 2015 Dec;94(50):e2254. [PUBMED: PMC5058915] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lubrano 2015
- Lubrano E, Spadaro A, Amato G, Benucci M, Cavazzana I, Chimenti MS, et al. Tumour necrosis factor alpha inhibitor therapy and rehabilitation for the treatment of ankylosing spondylitis: a systematic review. Seminars in Arthritis and Rheumatism 2015 Apr;44(5):542‐50. [PUBMED: PMID: 25450240] [DOI] [PubMed] [Google Scholar]
Maxwell 2015
- Maxwell LJ, Zochling J, Boonen A, Singh JA, Veras MM, Tanjong Ghogomu E, et al. TNF‐alpha inhibitors for ankylosing spondylitis. Cochrane Database of Systematic Reviews 2015, Issue 4. [DOI: 10.1002/14651858.CD005468.pub2; PUBMED: PMID: 25887212] [DOI] [PMC free article] [PubMed] [Google Scholar]
McGonagle 2014
- McGonagle D, Thomas RC, Schett G. Spondyloarthritis: may the force be with you?. Annals of the Rheumatic Diseases 2014 Feb;73(2):321‐3. [PUBMED: PMID: 24220157] [DOI] [PubMed] [Google Scholar]
Niedermann 2013
- Niedermann K, Sidelnikov E, Muggli C, Dagfinrud H, Hermann M, Tamborrini G, et al. Effect of cardiovascular training on fitness and perceived disease activity in people with ankylosing spondylitis. Arthritis Care & Research 2013 Nov;65(11):1844‐52. [PUBMED: 23836515] [DOI] [PubMed] [Google Scholar]
O'Dwyer 2014
- O'Dwyer T, O'Shea F, Wilson F. Exercise therapy for spondyloarthritis: a systematic review. Rheumatology International 2014 Jul;34(7):887‐902. [PMID: 24549404] [DOI] [PubMed] [Google Scholar]
Palla 2012
- Palla I, Trieste L, Tani C, Talarico R, Cortesi PA, Mosca M, et al. A systematic literature review of the economic impact of ankylosing spondylitis. Clinical and Experimental Rheumatology 2012;30(4 Suppl 73):S136‐41. [PUBMED: 23072824] [PubMed] [Google Scholar]
Poddubnyy 2012
- Poddubnyy D, Rudwaleit M, Haibel H, Listing J, Märker‐Hermann E, Zeidler H, et al. Effect of non‐steroidal anti‐inflammatory drugs on radiographic spinal progression in patients with axial spondyloarthritis: results from the German Spondyloarthritis Inception Cohort. Annals of the Rheumatic Diseases 2012;71(10):1616‐22. [PUBMED: 22459541] [DOI] [PubMed] [Google Scholar]
Pradeep 2008
- Pradeep DJ, Keat A, Gaffney K. Predicting outcome in ankylosing spondylitis. Rheumatology (Oxford) 2008;47(7):942‐5. [PUBMED: 18492709] [DOI] [PubMed] [Google Scholar]
Ramiro 2014
- Ramiro S, Heijde D, Tubergen A, Stolwijk C, Dougados M, denBosch F, et al. Higher disease activity leads to more structural damage in the spine in ankylosing spondylitis: 12‐year longitudinal data from the OASIS cohort. Annals of the Rheumatic Diseases 2014 Aug;73(8):1455‐61. [PUBMED: PMID: 24812292] [DOI] [PubMed] [Google Scholar]
Regel 2017
- Regel A, Sepriano A, Baraliakos X, Heijde D, Braun J, Landewé R, et al. Efficacy and safety of non‐pharmacological and non‐biological pharmacological treatment: a systematic literature review informing the 2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis. Rheumatic and Musculoskeletal Diseases Open 2017;3(1):e000397. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reveille 2012
- Reveille JD, Ximenes A, Ward MM. Economic considerations of the treatment of ankylosing spondylitis. The American Journal of the Medical Sciences 2012;343(5):371‐4. [PUBMED: PMC3613240.] [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rucker 2008
- Rucker G, Schwarzer G, Carpenter JR, Schumacher M. Undue reliance on I² in assessing heterogeneity may mislead. BMC Medical Research Methodology 2008;8:79. [DOI: 10.1186/1471-2288-8-79] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rudwaleit 2009
- Rudwaleit M, Heijde D, Landewé R, Listing J, Akkoc N, Brandt J, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Annals of the Rheumatic Diseases 2009 Jun;68(9):777‐83. [PUBMED: PMID: 19297344] [DOI] [PubMed] [Google Scholar]
Saracoglu 2017
- Saracoglu I, Kurt G, Okur EO, Afsar E, Seyyar GK, Calik BB, et al. The effectiveness of specific exercise types on cardiopulmonary functions in patients with ankylosing spondylitis: a systematic review. Rheumatology International 2017 Mar;37(3):409‐21. [PUBMED: PMID: 27837263] [DOI] [PubMed] [Google Scholar]
Saunders 2016
- Saunders DH, Sanderson M, Hayes S, Kilrane M, Greig CA, Brazzelli M, et al. Physical fitness training for stroke patients. Cochrane Database of Systematic Reviews 2016, Issue 3. [DOI: 10.1002/14651858.CD003316.pub6; PUBMED: 27010219] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schünemann 2011a
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Schünemann 2011b
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Sieper 2009
- Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos‐Vargas R, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Annals of the Rheumatic Diseases 2009;68(Suppl 2):ii1‐44. [DOI] [PubMed] [Google Scholar]
Singh 2013
- Singh B, Upadhyay A, Garg M, Mahajan A. Effects of physical and rehabilitative treatment on quality of life of ankylosing spondylitis patients. The Internet Journal of Orthopedic Surgery 2013;21(2):1‐5. [Google Scholar]
Slade 2016
- Slade SC, Dionne CE, Underwood M, Buchbinder R, Beck B, Bennell K, et al. Consensus on Exercise Reporting Template (CERT): modified Delphi study. Physical Therapy 2016 [Epub 2016 May 5];96(10):1514‐24. [DOI: 10.2522/ptj.20150668; PUBMED: 27149962] [DOI] [PubMed] [Google Scholar]
Slobodin 2015
- Slobodin G, Eshed I. Non‐radiographic axial spondyloarthritis. Israel Medical Association Journal 2015;17(12):770‐6. [PUBMED: PMID: 26897981] [PubMed] [Google Scholar]
Tubach 2012
- Tubach F, Ravaud P, Martin‐Mola E, Awada H, Bellamy N, Bombardier C, et al. Minimum clinically important improvement and patient acceptable symptom state in pain and function in rheumatoid arthritis, ankylosing spondylitis, chronic back pain, hand osteoarthritis, and hip and knee osteoarthritis: results from a prospective multinational study. Arthritis Care & Research 2012 Nov;64(11):1699‐707. [PUBMED: 22674853] [DOI] [PubMed] [Google Scholar]
Van den Berg 2012
- Berg R, Baraliakos X, Braun J, Heijde D. First update of the current evidence for the management of ankylosing spondylitis with non‐pharmacological treatment and non‐biologic drugs: a systematic literature review for the ASAS/EULAR management recommendations in ankylosing spondylitis. Rheumatology (Oxford) 2012;51(8):1388‐96. [DOI] [PubMed] [Google Scholar]
Van den Berg 2013
- Berg R, Hooge M, Rudwaleit M, Sieper J, Gaalen F, Reijnierse M, et al. ASAS modification of the Berlin algorithm for diagnosing axial spondyloarthritis: results from the SPondyloArthritis Caught Early (SPACE)‐cohort and from the Assessment of SpondyloArthritis international Society (ASAS)‐cohort. Annals of the Rheumatic Diseases 2013;72(10):1646‐53. [PUBMED: PMID: 23139266] [DOI] [PubMed] [Google Scholar]
Van der Heijde 1997
- Heijde D, Bellamy N, Calin A, Dougados M, Khan MA, Linden S. Preliminary core sets for endpoints in ankylosing spondylitis. Assessments in Ankylosing Spondylitis Working Group. Journal of Rheumatology 1997;24(11):2225‐9. [PUBMED: 9375888] [PubMed] [Google Scholar]
Van der Heijde 1999
- Heijde D, Linden S, Bellamy N, Calin A, Dougados M, Khan MA. Which domains should be included in a core set for endpoints in ankylosing spondylitis? Introduction to the ankylosing spondylitis module of OMERACT IV. Journal of Rheumatology 1999;26(4):945‐7. [PUBMED: 10229424] [PubMed] [Google Scholar]
van der Heijde 2008
- Heijde D, Landewé R, Baraliakos X, Houben H, Tubergen A, Williamson P, et al. Radiographic findings following two years of infliximab therapy in patients with ankylosing spondylitis. Arthritis and Rheumatism 2008;58(10):3063‐70. [DOI] [PubMed] [Google Scholar]
Van der Linden 1984
- Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis and Rheumatism 1984;27(4):361‐8. [DOI] [PubMed] [Google Scholar]
Vidoni 2015
- Vidoni ED, Johnson DK, Morris JK, Sciver A, Greer CS, Billinger SA, et al. Dose‐response of aerobic exercise on cognition: a community‐based, pilot randomized controlled trial. PLoS One 2015 Jul 9;10(7):e0131647. [DOI: 10.1371/journal.pone.0131647; PUBMED: PMID: 26158265] [DOI] [PMC free article] [PubMed] [Google Scholar]
Vliet 2009
- Vliet Vlieland TP, Li LC. Rehabilitation in rheumatoid arthritis and ankylosing spondylitis: differences and similarities. Clinical and Experimental Rheumatology 2009;27(4 Suppl 55):S171‐8. [PubMed] [Google Scholar]
Wang 2009
- Wang CY, Chiang PY, Lee HS, Wei JC. The effectiveness of exercise therapy for ankylosing spondylitis: a review. International Journal of Rheumatic Diseases 2009;12(3):207‐10. [DOI] [PubMed] [Google Scholar]
Ward 2016
- Ward MM, Deodhar A, Akl EA, Lui A, Ermann J, Gensler LS, et al. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 Recommendations for the treatment of ankylosing spondylitis and non‐radiographic axial spondyloarthritis. Arthritis Care & Research 2016 Feb;68(2):151‐66. [PUBMED: PMID: 26401907] [DOI] [PMC free article] [PubMed] [Google Scholar]
Webers 2016
- Webers C, Essers I, Ramiro S, Stolwijk C, Landewé R, Heijde D, et al. Gender‐attributable differences in outcome of ankylosing spondylitis: long‐term results from the Outcome in Ankylosing Spondylitis International Study. Rheumatology (Oxford) 2016 Mar;55(3):419‐28. [DOI: 10.1093/rheumatology/kev340; PUBMED: PMID: 26385369] [DOI] [PubMed] [Google Scholar]