

Abstract
Non-medical use of prescription opioids (NMUPO) and related overdoses are disproportionately elevated among young adults. Efforts to understand the underlying reasons for NMUPO are critical for developing more effective prevention and intervention strategies for this group. Given the robust literature on the association between educational status and substance abuse risk, we examined the reasons for NMUPO through the lens of educational attainment among young adults. Data from the 2016 National Survey on Drug Use and Health came from an unweighted sample of 941 young adults aged 18-25 years who reported past-year NMUPO. Self-reported reasons for most recent NMUPO were compared by educational status. The most commonly-endorsed reasons for past-year NMUPO was physical pain relief (47.6%), followed by feel good/get high (19.8%), relax/relieve tension (13.2%) and experiment/see what it feels like (6.8%). Reasons for NMUPO did not differ as a function educational status (p = 0.17). These findings suggest that efforts to prevent and address opioid misuse among young adults should focus on understanding and improving pain management in this vulnerable population.
Keywords: young adult, opioid analgesics, education, pain
1. INTRODUCTION
Non-medical use of prescription opioids (NMUPO) is second only to marijuana as the most prevalent form of drug use in the United States (SAMHSA, 2015), with 11.5 million (4.7%) Americans reporting NMUPO during the past year (Han et al., 2017). NMUPO is associated with nearly 15,000 overdose deaths and a total economic burden of $78 billion annually (Florence et al., 2016; Meyer et al., 2014). Young adults (individuals aged 18-25 years) are at particularly elevated risk for NMUPO and its serious consequences, with NMUPO more prevalent among young adults (7.6%) compared to individuals aged 12-17 (4.8%) and 26-34 (6.0%) (Hu et al., 2017). Efforts to identify the groups at highest risk for NMUPO, as well as the reasons underlying their use, are critical for developing more effective prevention and intervention strategies.
One of the most robust and consistent markers associated with prevalence of licit and illicit drug use and associated problems is years of educational attainment. Indeed, one of the most consistent findings in the scientific literature is that educational attainment is inversely related with the prevalence of substance use and a wide range of other serious acute and chronic health problems (Cutler and Lleras-Muney, 2008; Grant et al., 2012; Higgins et al., 2009). With specific regard to prescription opioids, past-year NMUPO is greater among those with less than high school degree (5%) relative to those with at least some college education (3.6%)(Saha et al., 2016). Further, among young people, NMUPO is more prevalent among young adults not attending college compared to their college-enrolled peers (Martins et al., 2015; McCabe et al., 2018). However, virtually nothing is known about reasons for NMUPO among young people, particularly among those not enrolled in college (Drazdowski et al., 2016). Efforts to understand the reasons why young adults misuse prescription opioids (e.g., pain relief versus recreational use to get high) are important for guiding the development of more effective prevention and intervention strategies for this group. Given the robust literature on the association between educational status and substance abuse risk, we examined the reasons for NMUPO through the lens of educational attainment using a large nationally-representative dataset of young adults who reported past-year NMUPO.
2. METHODS
We analyzed data from the 2016 National Survey on Drug Use and Health (NSDUH), which used an independent, multistage probability sample of noninstitutionalized US civilians aged ≥ 12 years (n = 56,897; SAMHSA, 2017). The present sample included 941 unweighted young adults aged 18-25 years who reported past-year NMUPO (weighted: 12.8%). Participants who reported past-year NMUPO were also asked to report the main reason for their most recent NMUPO. Respondents were categorized as: in high school (n = 48), in college (n = 270), college graduate (n = 97), or not in college (n = 526). The nine possible reasons for NMUPO, as assessed by the NSDUH survey, included: (1) relieve physical pain, (2) relax or relieve tension, (3) experiment/see what like, (4) feel good/get high, (5) help with sleep, (6) help with feelings or emotions, (7) increase/decrease effects of other drugs, (8) hooked or have to have drug, (9) some other reason. Weighted cross-tabulations with design-adjusted chi-square tests were conducted to examine reasons for most recent NMUPO by educational status. Associations for sociodemographic characteristics (i.e., sex, race/ethnicity, age) previously shown to influence outcomes were then examined in a multinomial logistic regression analysis with the four main reasons for NMUPO as the outcome and education as the exposure (not in college versus other). Taylor series linearization variance estimation was employed to provide 95% confidence intervals (CI). Analyses were conducted using Stata 14.0 and employed survey analysis weights, which accounted for the complex multi-stage sampling plan.
3. RESULTS
The overall prevalence of past year NMUPO among 18-25 year olds was 7.2% (95% CI: 6.6%, 7.8%). Prevalence of past year NMUPO for those not in college was 8.4% (95% CI: 7.5%, 9.4%), which was significantly higher than other 18-25 year olds (5.8%, 95% CI: 5.1%, 6.6%; p = 0.001). More specifically, prevalence of past-year NMUPO was 5.7% (95% CI: 3.9%, 8.3%), 5.9% (95% CI: 5.0%, 6.9%), 5.6% (95% CI: 4.3%, 7.1%), and 8.4% (95% CI: 7.5%, 9.4%) for young adults in high school, in college, with a college degree, and not currently enrolled in college, respectively.
Of those young adult respondents who reported past-year NMUPO, 55.2% were male, 61.7% non-Hispanic White, 18.9% Hispanic and 13.2% non-Hispanic Black (Table 1). Of the nine possible reasons for most recent NMUPO, the most commonly-endorsed reason was to relieve physical pain (47.6%), followed by to feel good or get high (19.8%), relax or relieve tension (13.2%) and experiment/see what it feels like (6.8%). Reasons for NMUPO did not significantly differ as a function of educational status (p = 0.17; Figure 1, Table 2), with pain relief as the most frequently-cited reason for NMUPO regardless of education status. Among college graduates, the second most common reason was relaxation or relief of tension, while feeling good or getting high ranked second among all other YAs. In examining whether age, sex, or race was associated with the relationship between reasons for NMUPO and educational status among young adults, there was only one significant association found for sex in adjusted analyses (see Supplemental Table). Males’ main reason for NMUPO was more likely to ‘feel good/get high’ versus to ‘relieve physical pain’ than females (p = 0.003). For age, 18-21 year olds were more likely to have NMUPO to ‘experiment/see what like’ or ‘feel good/get high’ versus to ‘relieve physical pain’ than 22-25 year olds. There were no differences by race (p’s > 05).
Table 1.
Sociodemographic characteristics for 18-25 year olds with non-medical prescription pain reliever use in the past year (n = 941), 2016 National Survey on Drug Use and Healtha
| Weighted %, 95% Confidence Interval | |
|---|---|
| Male | 55.2 (50.8, 59.6) |
| Age, years | |
| 18-21 | 46.4 (42.5, 50.3) |
| 22-25 | 53.6 (49.7, 57.5) |
| Race/ethnicity | |
| White, non-Hispanic | 61.7 (57.6, 65.7) |
| Black, non-Hispanic | 13.2 (11.1, 15.6) |
| Other, non-Hispanic | 6.2 (4.4, 8.8) |
| Hispanic | 18.9 (15.6, 22.6) |
| Family income | |
| Less than $20,000 | 28.7 (25.6, 33.2) |
| $20,000-$49,999 | 32.8 (28.9, 37.0) |
| $50,000-$74,999 | 13.5 (11.0, 16.4) |
| $75,000+ | 25.0 (21.9, 28.5) |
Numbers may not sum to 100% due to rounding.
Figure 1.
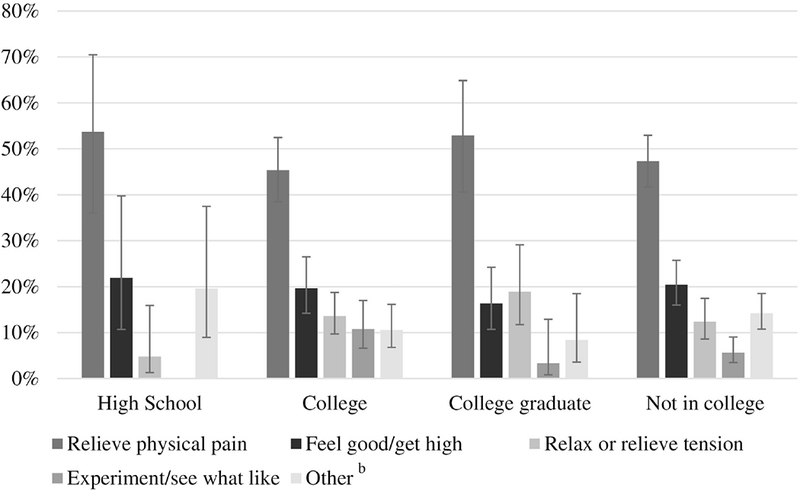
Main reason for most recent non-medical use of prescription opioids as a function of educational status, National Survey of Drug Use and Health (NSDUH) 2016a
a Bars represent weighted percentages with 95% confidence intervals; b Other reasons included help with sleep, help with feelings or emotions, to increase/decrease the effects of other drugs, because hooked or have to have drug, or some other reason.
Table 2.
Primary reason for past year non-medical prescription pain reliever use by education status among 18-25 year olds (weighted %, 95% Confidence Interval), 2016 National Survey on Drug Use and Healtha
| In high school | In college | College graduate | Not in college | |
|---|---|---|---|---|
| Relieve physical pain | 53.4 (36.0, 70.5) | 45.4 (38.4, 52.4) | 52.9 (40.6, 64.9) | 47.3 (41.7, 53.0) |
| Relax or relieve tension | 4.8 (1.3, 15.9) | 13.6 (9.7, 18.7) | 18.9 (11.7, 29.1) | 12.4 (8.6, 17.4) |
| Experiment/see what feels like | 0 | 10.8 (6.6, 17.0) | 3.3 (0.8, 12.9) | 5.7 (3.5, 9.1) |
| Feel good/get high | 21.9 (10.7, 39.8) | 19.7 (14.2, 26.5) | 16.4 (10.7, 24.2) | 20.4 (16.0, 25.7) |
| Other | 19.6 (9.0, 37.5) | 10.6 (6.8, 16.2) | 8.4 (3.6, 18.5) | 14.2 (10.8, 18.5) |
Education status groups are mutually exclusive.
4. DISCUSSION
In the present study, we examined whether reasons for NMUPO among young adults differed as a function of educational status. Previous research has indicated that reasons for opioid use are important predictors of use patterns and problems in young adults (McCabe et al., 2009). Given that young adults who are not enrolled in college are more likely to engage in NMUPO compared to their college-enrolled peers, a better understanding of why these individuals misuse their prescriptions may allow for the identification of young adults at the greatest risk for continued drug use and drug-related problems and inform intervention efforts.
In this nationally representative sample of young adults reporting past-year NMUPO, pain relief was the most commonly cited reason for their drug use. These data underscore the significance of untreated pain among young adults. These findings are also consistent with prior reports among older adults (Barth et al., 2013) and college-enrolled young adults (McCabe et al., 2007) identifying pain relief as a primary reason for NMUPO.
In the present study, participants’ primary reasons for NMUPO did not vary as a function of educational attainment. Thus, efforts to address opioid misuse among young adults, regardless of their educational status, should emphasize strategies for improving pain evaluation and management. Prior studies have reported that 67% of young adults report pain within the previous six months, with 14% reporting chronic pain (Mallen et al., 2005). Young adults with a recent history of NMUPO are less likely to receive adequate pain treatment and subsequently are more likely to report continued self-medication with prescription opioids and initiation of intravenous drug use (Fibbi et al., 2016). In addition to efforts to improve pain management, the development and dissemination of educational interventions may reduce the risk for NMUPO among young adults. This may include tailored information that could be provided to young adults detailing the potential risks of prescription opioid misuse, as well as additional training regarding safe opioid prescribing practices among physicians who often treat young adults (e.g., dentists, primary care providers, orthopedic specialists).
Although pain relief was the most commonly-cited reason for NMUPO, a subset of young adults reported misusing prescription opioids for other reasons (e.g., to feel good, get high, relax, relieve tension). Furthermore, some young adults may misdiagnose or rationalize their symptoms and use opioids in response to withdrawal or somatic symptoms of anxiety and depression. It is imperative that physicians and other healthcare providers assess young adults’ reasons for opioid use and distinguish between unmanaged pain, psychiatric symptoms, aberrant opioid use behaviors, and opioid withdrawal symptoms so that appropriate recommendations and referrals may be offered. For example, young adults who use prescription opioids to get high or to relieve symptoms of opioid withdrawal may be more likely to benefit from early referral to drug treatment services (e.g., buprenorphine maintenance) than they would from referral to pain management services.
Several strengths warrant mention. The present study represents the first effort to our knowledge to examine reasons for young adult NMUPO through the lens of educational attainment, a widely-used and consistent predictor of illicit drug use and drug-related adverse consequences in the broader population. Although, previous studies have examined NMUPO in young adults, prior research has been limited by a predominance of college-enrolled young adult samples (McCabe et al., 2007; McCabe et al., 2018); thus, a notable strength of this study is the use of a nationally-representative dataset that included young adults who were not enrolled in college. Second, to our knowledge, this study represents the first to examine whether education status is associated with differences in reasons for NMUPO. Finally, the finding that pain relief functioned as a primary reason for NMUPO among young adults highlights the need for improved pain management education and support for young people and should inform efforts to develop more effective prevention and management strategies in this at-risk population.
Several limitations are also worth noting. First, because of the cross-sectional nature of the data, we are unable to comment on the temporal relations between reasons for NMUPO and educational status. Second, although prior studies have established the reliability and validity of key NSDUH measures (SAMHSA, 2010; Harrison et al., 2007), all measures were based on self-reports and young adults may have been reluctant to disclose information related to NMUPO. Finally, the present study was constrained by NSDUH measures such that only the main reason for most recent NMUPO was assessed. Young adults may engage in NMUPO for myriad reasons and previous research indicates that young adults may report different reasons for lifetime or past-year NMUPO (McCabe et al., 2009). It also remains unclear whether young adult participants’ reports of pain relief may have related to pain from an acute injury, a chronic problem or even opioid-related withdrawal discomfort.
5. CONCLUSIONS
Among young adults reporting past-year NMUPO, pain relief was the most frequently-cited reason for NMUPO independent of education status. These data highlight the need for improved education and support around pain management with young people independent of their educational status and should inform efforts to develop more effective prevention and management strategies in this vulnerable group.
Supplementary Material
HIGHLIGHTS.
Young adults (YAs) are at risk for non-medical use of prescription opioids (NMUPO).
Reasons for NMUPO were examined using a nationally-representative dataset of YAs
Reasons for NMUPO did not differ by educational status.
Pain relief was the most commonly-endorsed reason for NMUPO among YAs.
Efforts to reduce NMUPO in young people should focus on addressing pain management.
Acknowledgments:
All authors have made significant contributions to the manuscript and have reviewed and approved the revised manuscript.
Funding sources: This work was supported in part by the National Institute on Drug Abuse (R01DA042790), the Laura and John Arnold Foundation, and the National Institute of General Medical Sciences (P20GM103644). The funding agencies had no role in study design, in the collection, analysis and interpretation of data, in the preparation of the manuscript, or in the decision to submit the paper for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of interest: None
Human participation protection: The data collection protocol of the National Survey on Drug Use and Health was approved by the Institutional Review Board at the RTI International.
REFERENCES
- 1.Barth KS, Maria MM-S, Lawson K, et al. , 2013. Pain and motives for use among non-treatment seeking individuals with prescription opioid dependence. Am. J. Addict. 22, 486–491. DOI: 10.1111/j.1521-0391.2013.12038.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cutler D, Lleras-Muney A, 2008. Education and health: evaluating theories and evidence In: House J, Schoeni R, Kaplan G, Pollack H, (Eds.) Making Americans Healthier: Social and Economic Policy as Health Policy. Russel Sage Foundation, New York, pp. 29–60. [Google Scholar]
- 3.Drazdowski TK, 2016. A systematic review of the motivations for the non-medical use of prescription drugs in young adults. Drug Alcohol Depend. 162, 3–25. DOI: doi: 10.1016/j.drugalcdep.2016.01.011. [DOI] [PubMed] [Google Scholar]
- 4.Fibbi M, Silva K, Johnson K, Langer D, Lankenau SE, 2012. Denial of prescription opioids among young adults with histories of opioid misuse. Pain Med. 13, 1040–1048. DOI: 10.1111/j.1526-4637.2012.01439.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Florence CS, Zhou C, Luo F, Xu L, 2016. Economic burden of prescription opioid overdose, abuse, and dependence in the United States, 2013. Med. Care. 54, 901–906. DOI: 10.1097/MLR.0000000000000625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Grant JD, Scherrer JF, Lynskey MT, et al. , 2012. Associations of alcohol, nicotine, cannabis, and drug use dependence with educational attainment: evidence from cotwin-control analyses. Alcohol Clin. Exp. Res. 36, 1412–1420. DOI: 10.1111/j.1530-0277.2012.01752.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Han B, Compton WM, Blanco C, et al. , 2017. Prescription opioid use, misuse, and use disorders in U.S. Adults: 2015 National Survey on Drug Use and Health. Ann. Intern. Med. 167, 293–301. DOI: 10.7326/M17-0865. [DOI] [PubMed] [Google Scholar]
- 8.Harrison LD, Martin SS, Enev T, Harrington D, 2007. Comparing Drug Testing and Self-Report of Drug Use among Youths and Young Adults in the General Population Substance Abuse and Mental Health Services Administration, Rockville, MD. [Google Scholar]
- 9.Higgins ST, Heil SH, Badger GJ, et al. , 2009. Education disadvantage and cigarette smoking during pregnancy. Drug Alcohol Depend. 104, S100–105. DOI: 10.1016/j.drugalcdep.2009.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hu MC, Griesler P, Wall M, Kandel DB, 2017. Age-related patterns in non-medical prescription opioid use and disorder in the US population at ages 13-34 from 2002 to 2014. Drug Alcohol Depend. 177, 237–243. DOI: 10.1016/j.drugalcdep.2017.03.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mallen C, Peat G, Thomas E, Croft P, 2005. Severely disabling chronic pain in young adults: Prevalence from a population-based postal survey in North Staffordshire. BMC Musculoskelet. Disord. 6, 42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Martins SS, Kim JH, Chen LY, et al. , 2015. Nonmedical prescription drug use among U.S. young adults by educational attainment. Soc. Psychiatry Psychiatr. Epidemiol. 50, 713–724. DOI: 10.1007/s00127-014-0980-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McCabe SE, Cranford JA, Boyd CJ, Teter CJ, 2007. Motives, diversion and routes of administration associated with nonmedical use of prescription opioids. Addict. Behav. 32, 562–575. DOI: 10.1016/j.addbeh.2006.05.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McCabe SE, Boyd CJ, Cranford JA, Teter CJ, 2009. Motives for nonmedical use of prescription opioids among high school seniors in the United States: Self-treatment and beyond. Arch. Pediatr. Adolesc. Med, 163, 739–744. DOI: 10.1001/archpediatrics.2009.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McCabe SE, Teter CJ, Boyd CJ, Wilens TE, Schepis TS, 2018. Sources of prescription medication misuse among young adults in the United States: the role of educational status. J. Clin. Psychiatry. 79, 17m11958 DOI: 10.4088/JCP.17m11958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Meyer R, Patel AM, Rattana SK, Quock TP, Mody SH, 2014. Prescription opioid abuse: A literature review of the clinical and economic burden in the United States. Popul. Health Manag. 17, 372–387. DOI: 10.1089/pop.2013.0098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Saha TD, Kerridge BT, Goldstein RB et al. , 2016. Nonmedical prescription opioid use and DSM-5 nonmedical prescription opioid use disorder in the United States. J. Clin. Psychiatry. 77, 772–780. DOI: 10.4088/JCP.15m10386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Substance Abuse and Mental Health Services Administration (SAMHSA), 2010. Reliability of key measures in the National Survey on Drug Use and Health Substance Abuse and Mental Health Services Administration, Rockville, MD. [PubMed] [Google Scholar]
- 19.Substance Abuse and Mental Health Services Administration (SAMHSA), 2015. Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health Substance Abuse and Mental Health Services Administration, Rockville, MD. [Google Scholar]
- 20.Substance Abuse and Mental Health Services Administration (SAMHSA), 2017. 2016 National Survey on Drug Use and Health: Methodological Summary and Definitions Substance Abuse and Mental Health Services Administration, Rockville, MD. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.