

Abstract
Aim:
Problem gambling in adolescents constitutes a major health problem. Very few studies have investigated the relationship of adolescent gambling with emotional/behavioral problems. The aim of this study was to examine the association between adolescent problem gambling and emotional/behavioral problems using data from a school survey in the greater Athens area.
Material and Methods:
The total sample consisted of 2159 high school students (45.4% males and 54.6% females) from a random and representative sample of public and private schools in the greater Athens area. Data were collected in the form of self-reported questionnaires during one school hour. To access problem gambling the Diagnostic and Statistical Manual of Mental Disorders-IV Multiple Response Adapted for Juveniles questionnaire was administered to the study population. The presence of emotional/behavioral problems was assessed via the Strengths and Difficulties Questionnaire. Full data from 2141 participants were analyzed. Eighteen questionnaire with incomplete data were excluded.
Results:
Problem gambling in adolescence is in line with the presence of emotional/behavioral problems. All Strengths and Difficulties Questionnaire subscales were significantly associated with problem gambling. Specifically, emotional symptoms, conduct problems, attention/hyperactivity, and social dysfunction were all significantly and independently associated with adolescent pathologic gambling. The prosocial scale had lower scores in problem gamblers.
Conclusion:
This article aims to highlight and discuss the coexistence of adolescent problem gambling with other symptoms. The significant association of emotional/behavioral problems among adolescents with problem gambling indicates a need to screen for these symptoms and for their subsequent treatment among adolescents with problem gambling.
Keywords: Adolescents, emotional behavioral problems, gambling
Abstract
Amaç:
Ergenlerde patolojik kumar oynama önemli bir sağlık sorununu oluşturmaktadır. Çok az sayıda çalışma ergenlikte kumar oynama ile duygusal/davranışsal sorunlar arasındaki ilişkiyi araştırmıştır. Bu çalışmanın amacı, büyük Atina bölgesinde yapılan bir okul araştırmasının verilerini kullanarak ergenlikte patolojik kumar oynama ile duygusal/davranışsal sorunlar arasındaki ilişkiyi incelemekti.
Gereç ve Yöntemler:
Toplam örneklem, büyük Atina bölgesinde bulunan ve rastgele seçilen temsili bir grup özel ve devlet okuluna devam eden 2 159 lise öğrencisinden (%45,4 erkek ve %54,6 kız) oluşmaktaydı. Veriler, bir okul saati içinde doldurulan öz bildirim anketleri kullanılarak toplanmıştır. Patolojik kumar oynama verilerine erişim için çalışma grubuna Ruhsal Bozuklukların Tanısal ve İstatistiksel El Kitabı-IV Gençler için Adapte Edilmiş Çoklu Yanıt anketi uygulandı. Duygusal/davranışsal sorunların varlığı Güçler ve Güçlükler anketi ile değerlendirildi. İki bin yüz kırk bir katılımcının bütün verileri incelendi. Tamamlanmamış veriler bulunan on sekiz anket çalışma dışında bırakıldı.
Bulgular:
Ergenlikte patolojik kumar oynayanlarda duygusal/davranışsal sorunlar saptandı. Bütün Güçler ve Güçlükler anketi alt ölçekleri patolojik kumar oynama ile anlamlı derecede ilişkili bulundu. Özellikle, duygusal belirtiler, davranış bozuklukları, dikkat/hiperaktivite ve sosyal işlev bozukluğu, ergenlikte patolojik kumar oynama ile anlamlı derecede ve bağımsız olarak ilişkili bulundu. Patolojik kumar oynayanlarda prososyal ölçek puanları daha düşük bulundu.
Çıkarımlar:
Bu makale ergenlikte patolojik kumar oynama ile diğer belirtilerin birlikteliğini aydınlatmayı ve tartışmayı hedeflemiştir. Patolojik kumar oynama bozukluğu olan ergenlerde duygusal/davranışsal sorunların anlamlı şekilde eş zamanlı olarak bulunması, bu ergenlerde bu belirtilerin taranması ve daha sonra bunların tedavi edilmesi gereksinimini göstermektedir.
Introduction
Problem gambling (PG) is a term used to describe “a syndrome of gambling-related behaviours that often leads to significant harm to individuals, to others close to the gambler and to the community” (1). Problem gambling is one of the most common forms of addiction in the adolescent population (2, 3). In the United States of America, 20–40% of adolescents gamble on a weekly basis, 10–20% are in danger of developing this disorder, and 2–9% are already addicted (4).
Psychodynamic, neurobiological, and sociologic theories mainly describe those with PG as a homogeneous population group. However, data regarding the heterogeneity of the population with PG and its relationship with emotional/behavioral problems are scarce (5). Nevertheless, for patients with PG and concurrent emotional/behavioral problems, both the diagnostic approach and the treatment process may become complicated. It may also be difficult to recognize the heterogeneity of the population with PG and the possible dangers. Within this framework, the presence of associated mental health problems in patients with PG is related to heavier symptoms and less compliance to treatment (6, 7).
Pathologic gamblers may use gambling as a means to relieve themselves from undesirable psychological conditions that they are experiencing. For these patients, gambling is an escape and a way to avoid anxiety or feelings of depression (8, 9). Adolescents also often gamble to escape reality and to relieve themselves from depressive symptoms (9, 10).
Meta-analysis research on PG in adult population has shown that problematic or pathologic gamblers are more prone to also display emotional/behavioral problems. The most frequent comorbid disorders were found to be nicotine addiction, use of substances, emotional disorders, and anxiety disorders (11). Furthermore, alcohol addiction and other impulse control disorders are also observed (12).
As far as the adolescent population is concerned, there is little research on the presence of emotional/behavioral problems symptoms in those who are pathologic gamblers. According to the available data, adolescents with PG rank higher in terms of impulsivity, depression, anxiety, and delay discounting compared with the adolescents who do not gamble at all, or those who do gamble, but in a non-pathologic way (9, 10).
In a study on PG’s comorbidity in adolescence, the authors investigated the different subtypes of adolescent problem gamblers (13). The categories that they proposed, which are also applicable for the adult population were behaviorally conditioned, emotionally vulnerable, and antisocial impulsive problem gamblers. Additionally, two new categories have been created only for adolescents; one that features depressive symptoms and a second that features both internalized and externalized symptoms.
In another study, two different groups of adolescent problem gamblers were created on the basis of the severity of their gambling symptoms. Members of the group that was heavily affected also used substances, had infringing conduct and violent behavior, similar to the third category of the above-mentioned pathway model for adolescents (14).
Another common comorbidity is the coexistence of attention-deficit/hyperactivity disorder (ADHD) and PG, with ADHD being reported as a risk factor for the development of gambling addiction in adolescence. Neurobiological studies that support the relation between these two disorders mostly focus on one of the basic symptoms of ADHD, the impulsive behavior, which also constitutes a defining factor of PG (15).
Overall, there is limited research on concurrent emotional/behavioral problems in adolescents with PG and further investigation is needed within this research field in order to be able to reach safer conclusions. Our objective was to contribute to this purpose. The aim of this study was to investigate the coexistence of pathologic gambling with other psychiatric symptoms in adolescent students in the greater Athens area.
More specifically, we set out the following research objectives:
To investigate the relation of PG with emotional symptoms;
To investigate the relation of PG with conduct symptoms;
To investigate the relation of PG with hyperactivity/inattention symptoms;
To investigate the relation of PG with peer relationship problems;
To investigate the relation of PG with prosocial behavior.
Material and Methods
1. Sample
A total of 2141 students were recruited from a representative sample of 51 schools (44 public schools and seven private schools) in the greater Athens area. For the selection of schools, a complex sampling procedure was implemented, consisting of two stages: (1) stratification in terms of geographic region, and (2) selection of a random sample of schools within each stratum. Consistent with this, the first stage of the sampling procedure produced the following five strata: central Athens, northeastern suburbs, western suburbs, eastern suburbs, and Piraeus. In the second stage of sampling, within each stratum, a random sample of private and public schools was selected from the pertinent list of the Ministry of Education. In each school unit, a random sample of classrooms was chosen.
2. Assessment
The research instrument consisted of the following sub-sections:
The questionnaire had an introductory part in which the following personal and family data were recorded: sex, age, nationality, living arrangements (both parents, one parent, neither parent), parental involvement with gambling activities, type of school (public, private).
For the assessment of gambling involvement in the adolescents, the Diagnostic and Statistical Manual of Mental Disorders-IV Multiple Response Adapted for Juveniles questionnaire (DSM-IV-MR-J) was employed (16). This is a self-report questionnaire consisting of 12 items (nine categories), which tap the pertinent Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) criteria for PG in adolescents. The majority of the items are rated on a four-point scale: (a) never, (b) once or twice, (c) sometimes, and (d) often. However, answers are transformed into binary responses (presence-absence of the criterion). A positive answer to more than four categories corresponds to the presence of PG in the adolescent.
The questionnaire was translated and back translated in Greek by bilingual mental health professionals. A group of experts comprising psychiatrists, epidemiologists, child psychiatrists, and psychologists read through the questionnaire and revised its content in accordance to the Greek culture. Finally, a group of 20 adolescents commented on the comprehensibility and clarity of the items.
For the assessment of associated psychopathology, the Strengths and Difficulties Questionnaire (SDQ) was used. The SDQ is a behavioral screening questionnaire for children and adolescents aged 4–16 years (17). The SDQ contains 25 items, some positive and other negative, divided in five scales: emotional symptoms (five items), conduct problems (five items), hyperactivity/inattention (five items), peer relationship problems (five items), and prosocial behavior (five items). The official Greek adaptation of the SDQ was employed in this study (18, 19).
3. Procedure
Data were collected in the form of a self-report questionnaire during one school hour. The study was approved by the Ministry of Education, and we also obtained approval from the Ethics Committee of our hospital, as is required for any research initiative (Ethics Committee approval number: 51538/Γ2). In addition, the study was designed in accordance with the Declaration of Helsinki. Informed consent was obtained from the parents prior to participation in the study. Members of the research team visited each school in order to inform the School Principal, the staff and the Parents’ Association about the project. In agreement with the School Principal, they entered the classrooms and introduced themselves and the study to the students, while distributing the informed consent forms. One week after the first visit, members of the research team visited the classrooms for a second time to administer the questionnaires to the students who had previously provided signed informed consent for participation from their parents.
Statistical Analysis
Quantitative variables are expressed as mean values (±SD). Qualitative variables are expressed as absolute and relative frequencies. The Mann-Whitney test was used for the comparison of SDQ subscales between two groups. Logistic regression analysis allows one to say that the presence of a risk factor increases the odds of a given outcome by a specific factor. Each SDQ subscale was examined separately in the multiple logistic regression model because they were highly correlated and model diagnostics indicated that the regression estimates were highly collinear. Model diagnostics were evaluated using the Hosmer and Lemeshow statistic. The independent variable that entered in the model along with each SDQ subscale were age, nationality, sex, living with both parents, parents gamblers, last year’s grade, weekly pocket money, type of school (public, private), weekly hours in extracurricular activities, weekly hours in school activities, availability of food during the last month in the family. Each of the logistic models had all the aforementioned independent variables and one of the SDQ subscales. Adjusted odds ratios (OR) with 95% confidence intervals were computed from the results of the logistic regression analyses. All p values reported are two-tailed. Statistical significance was set at 0.05 and analyses were conducted using the SPSS statistical software (version 19.0).
Results
The sample consisted of 2141 adolescents (45.4% males and 54.6% females). Problem gambling according to DSM was identified in 5.6% of the sample (Figure 1).
Figure 1.
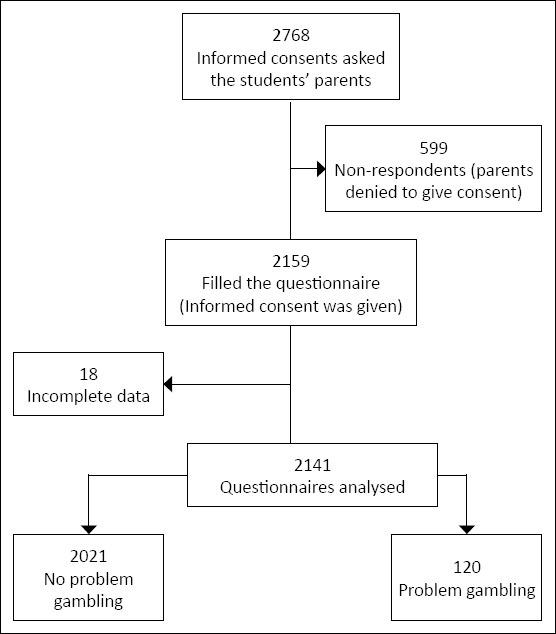
Study flow diagram
Around one-fifth (20%) of the total sample was aged up to 13 years, and 68% were aged 16 years or older (Figure 2). Most (90.3%) of the participants attended a public school, and 9.7% attended a private school. The majority (87.0%) of the participants were Greek and most of the adolescents (80.5%) lived with both parents. Parental gambling was reported in 24.4% of the sample and 78.5% of the adolescents had pocket money from their parents.
Figure 2.
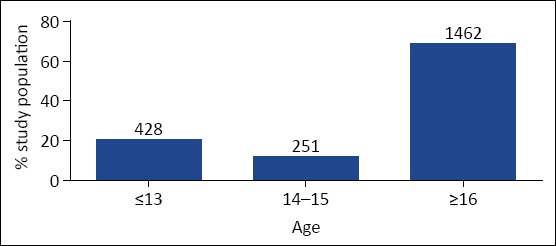
Age distribution of the study population (absolute numbers are indicated above each column)
Table 1 shows SDQ subscales according to the presence of problem gambling. All SDQ subscales were significantly associated with problem gambling. Specifically, emotional symptoms, conduct problems, hyperactivity, peer problems, and total scores were greater in adolescents who were identified as problem gamblers. The prosocial scale, as expected, had lower scores in problem gamblers.
Table 1.
Strengths and difficulties questionnaire subscales according to the presence of problem gambling
| Problem gambling | No (n=2021, 94.4%) Mean (SD) | Yes (n=120, 5.6%) Mean (SD) | pa |
|---|---|---|---|
| Conduct problems | 2.5 (1.5) | 4.8 (2.3) | <0.001 |
| Emotional/ behavioral | |||
| problems | 2.9 (2.5) | 4.0 (2.7) | <0.001 |
| Hyperactivity | 3.4 (2.2) | 5.1 (2.2) | <0.001 |
| Peer problems | 1.8 (1.7) | 3.3 (2.5) | <0.001 |
| Prosocial | 7.8 (1.9) | 6.0 (2.8) | <0.001 |
| Total difficulties score | 10.5 (5.3) | 17.1 (6.9) | <0.001 |
Mann-Whitney test; SD: Standard deviation
When multiple logistic regression analysis was conducted with dependent variables for the presence of PG (Table 2), and after adjusting for demographic factors, it was found that the odds for PG was increased as the total SDQ score and the SDQ subscales increases.
Table 2.
Results from multiple logistic regression analysis for strengths and difficulties questionnaire dimensions with dependent variable the presence of problem gambling
| OR (95% CI)+ | p | |
|---|---|---|
| Conduct problems scale | 1.69 (1.46–1.96) | <0.001 |
| Emotional/behavioral problems scale | 1.29 (1.16–1.43) | <0.001 |
| Hyperactivity scale | 1.39 (1.24–1.56) | <0.001 |
| Peer Problems scale | 1.26 (1.10–1.44) | 0.001 |
| Prosocial scale | 0.80 (0.72–0.89) | 0.001 |
| Total difficulties score | 1.19 (1.14–1.25) | <0.001 |
Odds Ratio (95% Confidence Interval) adjusted for demographic factors (age, nationality, sex, living with both parents, parents gamblers, last year’s grade, weekly pocket money, type of school (public, private), weekly hours in extracurricular activities, weekly hours in school activities, availability of food during the last month in the family.) *Indicates reference category; OR: Odds ratio
Discussion
We investigated the relationship between adolescent problem gambling and adolescents’ emotional/behavioral problems. Problem gambling was associated with higher levels of emotional/behavioral problems and the association was not moderated after controlling for the effects of other variables.
Hyperactivity/inattention problems in our sample were associated with problem gambling (OR 1.39). It seems that adolescent gamblers try to reduce the intensity of the symptoms of ADHD through their preoccupation with games of chance.
Neurobiological studies support our findings showing that patients with ADHD and patients with PG share analogous deficits in the regulation of behavior (20, 21). There is evidence that impulsivity and poor behavioral control, which are core characteristics of ADHD, are considered to be the breeding ground for the development of addictive behavior (22). Indications exist that impulsive behavior is present in addicted patients long before the onset of their addictive disorder (23). In our study conduct problems (OR 1.69), problems with peers (OR1.26), and prosocial problems (OR 0.80) were also associated with PG.
Gambling in adolescence constitutes a delinquent behavior because it requires contravention of rules and law. It is to be noted that many of the related leisure activities also constitute delinquent behaviors such as drinking alcohol (24).
Research on adult populations emphasizes that some antisocial characteristics and the antisocial personality disorder constitute a risk factor for the development of PG (25). Gene association studies primarily report the involvement of the dopaminergic and serotonergic systems in problem and pathologic gambling (26). The tendency to anti-social behavior has also been shown in some other studies conducted on adolescent populations, revealing the difficulty of addicted adolescents to comply with social norms. These studies report comorbidity with conduct disorder and participation in dangerous actions, frequent fights, and acts of violence (27).
Peer relationships during adolescence have a strong impact on the behavior of young people. Adolescents who develop pathologic gambling start to socialize with peers who also gamble and move away from friends who do not gamble. Having friends who gamble makes gambling less likely to be perceived as a high-risk activity (28, 29).
According to our results, emotional symptoms were also associated with PG (OR 1.29). It is possible that emotional/behavioral problems foster gambling. According to the Jacob’s theory of addictions (30), depression would likely precede the addiction because gambling is perceived as a solution to unpleasant states of existence. Gambling activities may help adolescents cope with their already existing emotional symptoms thus it is important not only to identify the factors that correlate with PG in adolescence and but also to study the etiopathology of each correlation. We believe that a crucial step for the early identification, prevention, and treatment of adolescents’ PG is the investigation of adolescents’ emotional/behavioral problems.
The clinical awareness of the frequent co-existence of emotional/behavioral problems with PG could be very useful for early therapeutic intervention. Adolescents who experience multiple problems should be distinguished from teenagers displaying only gambling-related problems because they may differ in etiopathology, prognosis, and therapeutic planning.
Adolescents with PG and other mental health problems constitute a population with multiple needs. Therefore, developing effective therapeutic models and interventions is crucial.
Certain limitations should be considered in understanding the results of this study. The cross-sectional design of the study could not demonstrate causal directions between PG and emotional/behavioral problems. The refusal rate was 22%. Additionally, the findings of the study are limited to the greater Athens area and therefore results cannot be extrapolated to the rest of the country. Furthermore, sampling bias might have occurred in the study design because only students whose parents consented to taking part in the survey were administered the questionnaire.
It is also possible, that factors other than the variables included in the study are related to the association between PG and emotional/behavioral problems. For example, genetic factors and personality variables could moderate this relationship.
Conclusion
This article aims to highlight and discuss the coexistence of adolescent PG with emotional/behavioral problems.
In summary, we set out to investigate whether there would be an association of specific psychopathologic symptoms (evaluated by SDQ questionnaire) and PG in a representative sample of adolescents in the greater Athens area of Greece.
The results clearly show that gambling problems in adolescence are strongly related with emotional/behavioral problems. According to our results, emotional symptoms, conduct problems, hyperactivity/inattention, peer problems, and social problems were all significantly and independently associated with adolescent PG.
Taking this into account may offer us useful clinical information for patients in complicated conditions, such as problem gamblers, allowing for a more effectively targeted treatment.
Footnotes
Ethics Committee Approval: The study was approved by the Ministry of Education, and we also obtained approval from the Ethics Committee of our hospital, as is required for any research initiative (Ethics Committee approval number: 51538/Γ2).
Informed Consent: Informed consent was obtained from the parents prior to participation in the study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.E., M.M., C.P., G.P.; Design - D.A., H.E., M.E.; Supervision - D.A., C.P.; Data Collection and/or Processing - M.P., D.A.; Analysis and/or Interpretation - M.A., DA.; Literature Review - M.P.; Writing - M.P., D.A.; Critical Review - D.A., H.E.
Conflict of Interest: Research Funding Support: Greek Organization of Football Prognostics SA (OPAP SA).
Financial Disclosure: Research Funding Support: OPAP S.A.
Etik Kurul Onayı: Çalışma Milli Eğitim Bakanlığı tarafından onaylandı ve aynı zamanda herhangi bir araştırma girişimi için gerekli olduğu gibi hastanemiz Etik Kurulu’ndan da onay aldık (Etik Kurulu onay numarası: 51538/Γ2).
Hasta Onamı: Çalışmaya katılmadan önce ebeveynlerden bilgilendirilmiş onam alındı.
Hakem Değerlendirmesi: Dış bağımsız.
Yazar Katkıları: Fikir - M.E., M.M., C.P., G.P.; Tasarım - D.A., H.E., M.E.; Denetleme - D.A., C.P.; Veri Toplanması ve/veya İşlemesi - M.P., D.A.; Analiz ya/ya da Yorum - M.A., DA.; Dizin Taraması - M.P.; Yazıyı Yazan - M.P., D.A.; Eleştirel İnceleme - D.A., H.E.
Çıkar Çatışması: Research Funding Support: Greek Organization of Football Prognostics SA (OPAP SA).
Mali Destek: Research Funding Support: OPAP S.A.
References
- 1.Neal P, Delfabbro P.H, O'Neil M. Problem gambling and harm: Towards a national definition. Melbourne: Gambling Research Australia; 2005. [Google Scholar]
- 2.Calado F, Griffiths D. Problem gambling worldwide:an update and systematic review of empirical research. J Behav Addict. 2016;5:592–613. doi: 10.1556/2006.5.2016.073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hurt H, Giannetta JM, Brodsky NL, Shera D, Romer D. Gambling initiation in preadolescents. J Adolesc Health. 2008;43:91–3. doi: 10.1016/j.jadohealth.2007.12.018. [DOI] [PubMed] [Google Scholar]
- 4.Welte JW, Barnes GM, Tidwell MC, Hoffman JH. The prevalence of problem gambling among U.S. adolescents and young adults:results from a national survey. J Gambl Stud. 2008;24:119–33. doi: 10.1007/s10899-007-9086-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Anagnostopoulos DC, Lazaratou H, Paleologou MP, et al. Adolescent gambling in greater Athens area:a cross-sectional study. Soc Psychiatry Psychiatr Epidemiol. 2017;52:1345–51. doi: 10.1007/s00127-017-1431-8. [DOI] [PubMed] [Google Scholar]
- 6.Holdsworth L, Haw J, Hing N. The temporal sequencing of problem gambling and comorbid disorders. Int J Ment Health Addiction. 2012;10:197–209. [Google Scholar]
- 7.Dowling NA, Cowlishaw S, Jackson AC, Merkouris SS, Francis KL, Christensen DR. Prevalence of psychiatric co-morbidity in treatment-seeking problem gamblers: A systematic review and meta-analysis. J Psychiatry. 2015;49:519–39. doi: 10.1177/0004867415575774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Keough MT, Penniston TL, Vihena-Churchill N, Michael Bagby Quilty LC. Depression symptoms and reasons for gambling sequentially mediate the associations between insecure attachment styles and problem gambling. Addict Behav. 2017;78:166–72. doi: 10.1016/j.addbeh.2017.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Nigro G, Cosenza M, Ciccarelli M. The blurred future of adolescent gamblers: impulsivity, time horizon, and emotional distress. Front Psychol. 2017;8:486. doi: 10.3389/fpsyg.2017.00486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cosenza M, Nigro G. Wagering the future:Cognitive distortions, impulsivity, delay discounting, and time perspective in adolescent gambling. J Adolesc. 2015;45:56–66. doi: 10.1016/j.adolescence.2015.08.015. [DOI] [PubMed] [Google Scholar]
- 11.Lorains FK, Cowlishaw S, Thomas SA. Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction. 2011;106:490–8. doi: 10.1111/j.1360-0443.2010.03300.x. [DOI] [PubMed] [Google Scholar]
- 12.Hodkins DC, Stea JN, Grant JE. Gambling disorders. Lancet. 2011;378:1874–84. doi: 10.1016/S0140-6736(10)62185-X. [DOI] [PubMed] [Google Scholar]
- 13.Gupta R, Nower L, Derevensky JL, Blaszczynski A, Faregh N, Temcheff C. Problem gambling in adolescents: an examination of the pathways model. J Gambl Stud. 2012;29:575–88. doi: 10.1007/s10899-012-9322-0. [DOI] [PubMed] [Google Scholar]
- 14.Goldstein AL, Faulkner B, Cunningham RM, Zimmerman MA, Chermack S, Walton MA. A latent class analysis of adolescent gambling: application of resilience theory. Int J Ment Health Addiction. 2013;11:13–30. [Google Scholar]
- 15.Grant JE, Chamberlain SR. Impulsive action and impulsive choice across substance and behavioral addictions: cause or consequence? Addict Behav. 2014;39:1632–9. doi: 10.1016/j.addbeh.2014.04.022. [DOI] [PubMed] [Google Scholar]
- 16.Fisher S. Developing the DSM-IV-MR-J criteria to identify adolescent problem gambling in non-clinical populations. J Gambl Stud. 2000;16:253–73. doi: 10.1023/a:1009437115789. [DOI] [PubMed] [Google Scholar]
- 17.Stinchfield R. A critical review of adolescent problem gambling assessment instruments. Int J Adolesc Med Health. 2010;22:77–93. [PubMed] [Google Scholar]
- 18.Goodman A, Goodman R. Strengths and Difficulties questionnaire as a dimentional measure of child and adolescent mental health. J Am Acad Child Psy. 2009;48:400–3. doi: 10.1097/CHI.0b013e3181985068. [DOI] [PubMed] [Google Scholar]
- 19.Giannakopoulos G, Tzavara C, Dimitrakaki C, Kolaitis G, Rotsika V. Tountas. The factor structure of the Strengths and Difficulties Questionnaire (SDQ) in Greek Adolescents. Ann Gen Psychiatry. 2009;8:20. doi: 10.1186/1744-859X-8-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Breyer JL, Botzet AM, Winters KC, Stinchfield RD, August G, Realmuto G. Young adult gambling behaviors and their relationship with the persistence of ADHD. J Gambl Stud. 2009;25:227–38. doi: 10.1007/s10899-009-9126-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Faregh N, Derevensky J. Gambling Behavior Among Adolescents with Attention Deficit/Hyperactivity Disorder. J Gambl Stud. 2011;27:243–56. doi: 10.1007/s10899-010-9211-3. [DOI] [PubMed] [Google Scholar]
- 22.Goudriaan AE, Oosterlaan J, De Beurs E, Van Den Brink W. The role of self-reported impulsivity and reward sensitivity versus neurocognitive measures of disinhibition and decision-making in the prediction of relapse in pathological gamblers. Psychol Med. 2008;38:41–50. doi: 10.1017/S0033291707000694. [DOI] [PubMed] [Google Scholar]
- 23.Lazaratou H, Palaiologou A, Anagnostopoulos D. [Impulsivity as an immediate factor between addictive disorders and Attention Deficit-Hyperactivity Disorder] [Article in Greek, Modern] Psychiatriki. 2017;28:156–64. doi: 10.22365/jpsych.2017.282.156. [DOI] [PubMed] [Google Scholar]
- 24.Holdsworth L, Haw J, Hing N. The temporal sequencing of problem gambling and Comorbid disorders. Int J Ment Health Addiction. 2012;10:197–209. [Google Scholar]
- 25.Johansson Α.Ζ, Jon E, Grant Ζ, Suc Won Kim Ζ, Brian L, Odlaug ΖK. Risk Factors for Problematic Gambling: A Critical Literature Review. J Gambl Stud. 2009;25:67–92. doi: 10.1007/s10899-008-9088-6. [DOI] [PubMed] [Google Scholar]
- 26.Gyollai A, Griffiths MD, Barta C, et al. The genetics of problem and pathological gambling: a systematic review. Curr Pharm Des. 2014;20:3993–9. doi: 10.2174/13816128113199990626. [DOI] [PubMed] [Google Scholar]
- 27.Slavin M, Pilver CE, Hoff RA, et al. Serious Physical Fighting and Gambling-Related Attitudes and Behaviors in Adolescents. J BehavAddict. 2013;2:167–78. doi: 10.1556/JBA.2.2013.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Welte JW, Barnes GM, Tidwell MC, Hoffman JH. Association between problem gambling and conduct disorder in a national survey of adolescents and young adults in the United States. J Adolesc Health. 2009;45:396–401. doi: 10.1016/j.jadohealth.2009.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sarti S, Triventi M. The role of social and cognitive factors in individual gambling: An empirical study on college students. Soc Sci Res. 2017;62:219–37. doi: 10.1016/j.ssresearch.2016.08.009. [DOI] [PubMed] [Google Scholar]
- 30.Sanscartier MD, Edgerton JD, Roberts LW. A Latent class Analysis of Gambling Activity Patterns in a Canadian University sample of emerging adults: socio-demographic, motivational and mental health correlates. J Gambl Stud. 2018;34:863–80. doi: 10.1007/s10899-017-9734-y. [DOI] [PubMed] [Google Scholar]