

Abstract
Aberrant positioning of the ulnar nerve volar to the carpal tunnel is a rare anatomic variation. We present the case of a 55-yearold female with unique ulnar nerve anatomy that was discovered intraoperatively during carpal tunnel release. The ulnar nerve was running directly adjacent to the median nerve in the distal forearm and as the median nerve traversed dorsal to the transverse carpal ligament (flexor retinaculum) to enter the carpal tunnel the ulnar nerve continued directly volar to this structure before angling towards Guyon’s Canal. The unique ulnar nerve anatomy was successfully identified, carefully dissected and managed with a successful patient outcome. Variations of the anatomy at the level of the carpal tunnel are rare but do exist. Awareness of these anatomic variations and adequate visualization of the ulnar nerve along with the surrounding structures is crucial to avoid iatrogenic injuries during carpal tunnel release.
Key words: carpal tunnel release, ulnar nerve positioning, aberrant positioning
Introduction
In the United States, carpal tunnel syndrome (CTS) affects 1-3/1,000 patients per year with approximately 600,000 carpal tunnel releases performed annually.1 CTS is caused by median nerve compression at the wrist that causes numbness, tingling, and pain in the hand. Complication rates following transverse carpal ligament release (carpal tunnel release) have been reported to be 0.19-35% and primarily include lacerations of nerves, vessel and tendons.2 Additional complications can include infection, scar tenderness, pillar pain, sympathetic dystrophy, and persistent median nerve symptoms.
On rare occasions, aberrant position of the ulnar nerve has been reported in patients undergoing carpal tunnel release and occurs less than 0.1% of the time.3-6 We present a case of a 55-year old female who had an aberrant ulnar nerve that was discovered intraoperatively during carpal tunnel release. We discuss her clinical and operative course that led to a successful postoperative outcome.
Case Report
A 55-year-old right hand dominant female was followed for pain and numbness in her hands present for several years and consistent with carpal tunnel syndrome. On physical exam there was no thenar atrophy nor sensory irregularities, but provocative testing was positive and an electromyogram/ nerve conduction study was consistent with moderately severe bilateral carpal tunnel syndrome. After failing to improve with night splints, the patient elected to proceed with staged bilateral carpal tunnel releases under local anesthesia beginning with the right side. The right carpal tunnel release proceeded without complication and the patient noted resolution of her symptoms. The patient elected to return to the operating room one month later for her left carpal tunnel release again under local anesthesia. A standard mini-open approach was used. As the transverse carpal ligament was sharply incised from proximal to distal the patient complained of a sudden sharp pain. Closer inspection revealed a large nerve angling from radial to ulnar at the distal edge of the released transverse carpal ligament. This headed into Guyon’s Canal and appeared to be the ulnar nerve proper. Under loupe magnification, the epineurium to this nerve was noted to have been lacerated and three discrete nerve fascicles had been transected. At this point the distal antebrachial fascia was released with tenotomy scissors, which allowed better visualization of the median and ulnar nerves in this region. It appeared that the ulnar nerve was running directly adjacent to the median nerve in the distal forearm and as the median nerve traversed dorsal to the transverse carpal ligament (flexor retinaculum) to enter the carpal tunnel the ulnar nerve continued directly volar to this structure before angling towards Guyon’s Canal (Figure 1).
At this point, the rent in the epineurium was repaired with 10-0 nylon sutures and there appeared to be good reapproximation of the three injured fascicles. The tourniquet was subsequently deflated, the wound was closed and sterile dressings were applied.
Immediately postoperatively, the patient had 5/5 abduction strength of her digits and a negative Froment’s sign. Two weeks postoperatively at her first follow-up visit, she had intact sensation to light touch in all her fingers and 5/5 abduction strength of all digits. She indicated that she was pleased with the surgery as her nocturnal symptoms of pain and numbness had resolved. Given the known nerve injury she was seen back again for follow-up at four months, but had no complaints and no motor or sensory deficits on exam. The patient is aware of and has consented to the presentation of her surgery as a case report.
Discussion
Aberrant ulnar nerve position at the level of the transverse carpal ligament is a rare variation that has been documented infrequently.3-6 This case highlights the importance of careful dissection and awareness of possible anatomical variations found within the carpal tunnel. Much of the literature regarding anatomical variations within the carpal tunnel focuses on the variations of the median nerve itself as first discussed by Lanz in 1977.7 These include high bifurcation of the median nerve, aberrant origin of the motor branch, transligamentous palmar cutaneous branch of the median nerve, and ulnar to median nerve connections (Marinaccci communications). However, abnormalities within the tunnel are not limited to the median nerve.
Anomalies of the tendons though rare have been described,8 and women more commonly have elongated bellies of the flexor digitorum and profundus muscles extending into the carpal tunnel.9 In patients with carpal tunnel syndrome, it is also more common to find hypoplastic variants of the hook of the hamate compared to those without carpal tunnel syndrome.10 There are few case reports in the literature of an anomalous course of the ulnar nerve within the carpal tunnel, but it appears that this anomaly remains exceedingly rare.3,4,11
Figure 1.
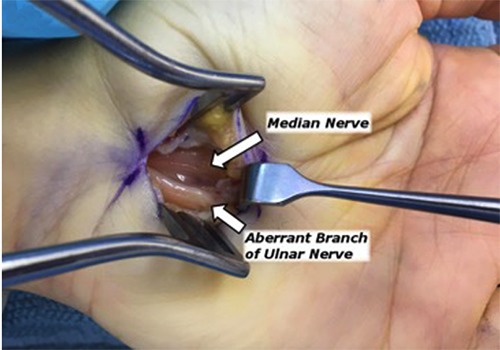
Intraoperative photograph of aberrant branch of ulnar nerve traversing over the now split transverse carpal ligament towards Guyon’s canal.
Good visualization of the carpal canal and surrounding structures as well as the awareness of anatomical variations are imperative in avoiding iatrogenic injuries during a carpal tunnel release. In this case, the three nerve fascicles that were injured did not result in any obvious sensory or motor deficits to the ulnar nerve postoperatively. Recognition of the aberrant anatomy and careful dissection spared the patient from further injury. While the senior author’s preferred technique of carpal tunnel release involves a mini-open incision, other methods are also acceptable. In this particular instance, however, we speculate that the use of an endoscopic technique may have resulted in complete transection of the ulnar nerve since it lay directly on the transverse carpal ligament and could not have been visualized from within the carpal tunnel.
Conclusions
We present an aberrant positioning of the ulnar nerve during carpal tunnel release. This case highlights the importance of careful dissection and awareness of anatomical variants that may exist during a straightforward carpal tunnel release. Proper identification and management is necessary prior to carpel tunnel release to avoid intraoperative iatrogenic injury.
Funding Statement
Funding: none.
References
- 1.Fajardo M, Kim SH, Szabo RM. Incidence of carpal tunnel release: trends and implications within the United States ambulatory care setting. J Hand Surg Am 2012;37:1599-605. [DOI] [PubMed] [Google Scholar]
- 2.Benson LS, Bare AA, Nagle DJ, et al. Complications of endoscopic and open carpal tunnel release. Arthroscopy 2006;22:919-24. [DOI] [PubMed] [Google Scholar]
- 3.Papanastasiou S, Sood M. Aberrant position of the ulnar nerve within the carpal canal. Microsurgery 2004;24:24-5. [DOI] [PubMed] [Google Scholar]
- 4.Galzio RJ, Magliani V, Lucantoni D, D’Arrigo C. Bilateral anomalous course of the ulnar nerve at the wrist causing ulnar and median nerve compression syndrome. Case report. J Neurosurg 1987;67: 754-6. [DOI] [PubMed] [Google Scholar]
- 5.Lindley SG, Kleinert JM. Prevalence of anatomic variations encountered in elective carpal tunnel release. J Hand Surg Am 2003;28:849-55. [DOI] [PubMed] [Google Scholar]
- 6.Bas H, Kleinert JM. Anatomic variations in sensory innervation of the hand and digits. J Hand Surg Am 1999;24: 1171-84. [DOI] [PubMed] [Google Scholar]
- 7.Lanz U. Anatomical variations of the median nerve in the carpal tunnel. J Hand Surg Am 1977;2:44-53. [DOI] [PubMed] [Google Scholar]
- 8.Smith RJ. Anomalous muscle belly of the flexor digitorum superficialis causing carpal-tunnel syndrome. Report of a case. J Bone Joint Surg Am 1971;53: 1215-6. [PubMed] [Google Scholar]
- 9.Holtzhausen LM, Constant D, de Jager W. The prevalence of flexor digitorum superficialis and profundus muscle bellies beyond the proximal limit of the carpal tunnel: a cadaveric study. J Hand Surg Am 1998;23:32-7. [DOI] [PubMed] [Google Scholar]
- 10.Chow JC, Weiss MA, Gu Y. Anatomic variations of the hook of hamate and the relationship to carpal tunnel syndrome. J Hand Surg Am 2005;30:1242-7. [DOI] [PubMed] [Google Scholar]
- 11.Eskesen V, Rosenorn J, Osgaard O. Atypical carpal tunnel syndrome with compression of the ulnar and median nerves. Case report. J Neurosurg 1981;54:668-9. [DOI] [PubMed] [Google Scholar]