

Abstract
Background:
Ministry of Health and Family Welfare has developed National Quality Framework to assess the quality of services for improvement and helps in certification of facilities, while Kayakalp was launched to promote cleanliness and hygiene in public health facilities.
Objective:
The objective of the study is to assess if Kayakalp implementation within the public health facilities supports quality certification of health facilities.
Methods:
A retrospective study was designed to gather data for 32 quality-certified district hospitals under National Quality Assurance Standards (NQAS) between May 2015 and April 2018 by reviewing records. Certification criteria and their external assessment checklist under NQAS and Kayakalp program for district hospitals were extracted from their respective states. External assessment score of all district hospitals under study was entered and analyzed using Statistical Package for the Social Sciences version 22 for Pearson's correlation analysis and MS Excel 2016 for statistical analysis.
Results:
Pearson's correlation coefficient was 0.217, which means that Kayakalp implementation has less significance on the quality certification of public health facilities to NQAS. A scatter chart was plotted which depicts nonlinear relationship between dependent and independent variable.
Conclusion:
Overall impact of implementation of Kayakalp initiative on quality certification of public health facilities to NQAS was significantly low; however, this could be due to less weightage given to the checkpoints in NQAS as compared to in NQAS.
Keywords: District hospitals, Kayakalp, National Quality Assurance Standards, quality
INTRODUCTION
Quality defines as a measure of scale, range of elements of care, includes targets (individual and population) for quality assurance as output, with desire for increase health outcomes, aiming for the outcome by converting process of health care into health outcome. It assesses the individual patient's need and involves them in decision-making and policy-making and undermines the barriers on performance of health-care provider using their technical, medical, and scientific knowledge.
It is well known that poor quality of services leads to additional burden on health system by diminishing effectiveness of its interventions and increasing the cost of care. To reduce the cost of poor quality, Juran,[1] an evangelist of quality management, gave the famous trilogy of quality planning, quality control, and quality improvement.
Quantifying quality in public health facility has never been an easy task in India, though quality framework and quality standards are available globally. In this regard, “Indian Public Health Standard” was launched for public health facilities’ infrastructure planning and upgradation; however, sooner, it was realized that in this process, component was still missing. Further, in this direction, several approaches for certification/accreditation were being adopted by different states, including NABH, ISO 9001:2008, Family Friendly Hospital Initiative, and other initiatives in 2008–2012.
Later, in 2013, the Ministry of Health and Family Welfare (MoHFW) has developed “National Quality Framework” which defines their approach to quality of care and its organizational arrangement and mandate in public healthcare institutions, and it is named as “operational guidelines for quality assurance for public health-care facilities” and subsequently for community health centre (CHCs), primary health centre (PHCs) in 2014, and for urban primary health centre (UPHCs) in 2016.[2,3,4] In 2015, Swatch Bharat Mission was launched by Honorable Prime Minister, and to complement it, “Kayakalp” was launched by the MoHFW. It focuses on promoting cleanliness and hygiene in public health facilities and also felicitates exemplary efforts of such facilities.[5,6]
The emphasis is now on the evaluation of public health systems for delivery of quality-assured services. National Quality Assurance Program (NQAP) and Kayakalp are a dynamic mechanism of objectively assessing and facilitating the conversion of inputs/processes into the expected outputs and outcomes with quality ultimately borne out by the client satisfaction. This study aims for how implementation of Kayakalp initiative in the public health facilities has impacted on certification of facilities to National Quality Assurance Standards (NQAS) and comparative analysis between the two offshoot programs of Government of India (GoI) for health-care facilities.
Research in context
In India, around 5.2 million injuries occur due to medical negligence, resulting in around 3 million preventable deaths every year; of these, the major factors are medications and hospital-acquired infections.[7] This makes medical errors one of the major causes of death. More than 43 million people suffered across the world each year due to medical mishaps. These errors account for nearly 23 million years of disability-adjusted life years. For every 100 hospitalization, an average of 12.7 adverse events occur. This provides evidence that adverse events due to medical negligence represent a major cause of morbidity and mortality. Moreover, how it is important to critically evaluate the quality and safety of the care provided to the person when he/she accesses health services. A study in Uganda 1994 said that implementation of NQAP in Uganda was done to strengthen primary health-care services. Within 18 months, significant objective and subjective improvement in the quality of services was observed.[8]
Another such program was adopted by Delhi Hospitals and dispensaries to overcome shortage of essential medicines by developing list of essential drugs, setting a centralized pooled procurement system, and promoting activities which support rational use of drugs. This resulted in supply of good-quality drugs with saving of nearly 30% on the annual drug bill for the Government of Delhi, which in turn improved approximately up to 80% availability of drugs.[9]
Considering the above facts, figures, and the current situation of the country, the “National Health Mission (NHM)” was launched with the goal “to enhance the availability of and access to good quality health care for people, especially for vulnerable population.[10] In this process, different program was launched by the NHM, namely, NQAP, Kayakalp, Swachh Swasth Sarvatra, and recently LaQshya to provide a mix of evidence-based clinical practice and quality of care.
Both programs have certain standards on basis of which assessment of health facilities has been done followed by incentivization of facilities for their exemplary efforts. On review of those guidelines, it was observed that Kayakalp standards are directly or indirectly embedded in the NQAS. Hence, it could be said that there can be some correlation in both programs. Till date, as of now, no such studies have been done.
METHODS
Participants and procedures
Data were collected from secondary-level health facilities, i.e., district hospitals, who were certified against NQAS along with their external assessment score for Kayakalp in the current year. We included data from May 2014 to April 2018. The retrospective study involving quantitative method was designed to do assess the impact of implementation of “Kayakalp” initiative on quality certification of public health facilities to NQAS. Initially, all the primary- and secondary-level public health facilities certified under NQAS were planned to be included in the study. After considering paucity of time and scope of the study, only district hospitals were considered for the study.
Eligibility criteria included
District hospitals either quality certified or quality certified with conditionality against NQAS under NQAP were included in the study.
Measures
Record review of the external assessment checklist was used in the study. Data were extracted from central as well as state level. Variable for the study was the external assessment score [Table 1] of the certified district hospital under NQAP and Kayakalp score for the current year. Award of quality certification was based on the criteria as approved by the Central Quality Supervisory Committee, which accounts for either full certification of the facility or certification with conditionality. The certification criteria are published in the report and are accessible online.
Table 1.
External assessment score of certified district hospitals (n=32)
| Facility name | NQAS Score (%) | Kayakalp Score (%) |
|---|---|---|
| Civil Hospital-Panchkula | 86 | 98 |
| Civil Hospital-Gurugram | 83 | 85 |
| Civil Hospital-Rohtak | 96 | 94.80 |
| B.K. Hospital Faridabad | 85 | 76.83 |
| General Hospital-Vyara (Tapi) | 81 | 86.20 |
| General Hospital-Mehsana | 91 | 64.80 |
| PKG Rajkot | 82 | 78 |
| General Hospital-Nadiad (Kheda) | 82 | 90.20 |
| Jallian Wallan Bagh Martyrs Memorial CH Amritsar (JBBM) | 86.20 | 74.40 |
| Civil Hospital- Pathankot | 86 | 99.80 |
| CH Nawanshahar | 83 | 97.80 |
| DH Faridkot | 84 | 99.60 |
| A.P. Jain Civil Hospital Rajpura, Patiala | 74 | 89.80 |
| DH-Vizianagram | 82 | 99.40 |
| DH-Rajamahendravaram | 88 | 78.30 |
| DH-Anakapalli | 87 | 91.10 |
| DH Eluru, West Godavari District | 90 | 93.60 |
| DH Machilipatnm, Krishna Distt | 85 | 81 |
| MJN Hospital, Cooch Behar | 92 | 66.80 |
| Siliguri DH | 86 | 99.80 |
| Pt. Madan Mohan Malivaya Hospital | 93 | 96.80 |
| District Hospital-Koppal | 83 | 67.60 |
| District Hospital-Tumakuru | 94 | 99.8 |
| District Hospital-Vijayapura | 89 | 99.80 |
| District Hospital-Aizwal (West) | 96 | 89.30 |
| Sardar Vallabh Bhai Patel Jila Hospital-Satna | 92 | 98.60 |
| DH Rajsamand | 90 | 92.20 |
| District Headquarters Hospital-Koraput | 86 | 81.20 |
| Veerangana Avantibai Mahila Hospital-Lucknow | 76 | 82 |
| Dr. Bhim Rao Ambedkar District Male Hospital-Etawah | 91 | 83.40 |
| District Women Hospital-Ghaziabad | 73 | 68.90 |
| Shri. Vinoba Bhave Civil Hospital-Silvassa | 88 | 92.40 |
NQAS: National Quality Assurance Standards
Statistical analysis
We compared the external assessment score of district hospital for NQAS and Kayakalp on a bivariate Pearson's correlation coefficient (r). All the external assessment scores were checked, coded, and entered in Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corporation, Java). Under this, district hospital's Kayakalp score is independent variable while their NQAS score is dependent variable. Hence, here, it was assumed that there is correlation between these two programs, i.e., facilities certified under NQAS might be having good Kayakalp score or Kayakalp implementation to support NQAP. To check this, null hypothesis was formulated which says there is no correlation between these two programs.
RESULTS
A total number of district hospitals (n) included was 32. The following analyses are restricted to these 32 district hospitals. The Pearson's correlation coefficient was 0.217 [Table 2]. Most hospitals were from Andhra Pradesh, Gujarat, Haryana, and Punjab. Small proportion were reported from Odisha, Mizoram, Madhya Pradesh, and Uttar Pradesh. Most of the hospitals were full certified against NQAS; few were quality certified with conditionality. Nearly two-third hospitals had scored >90% in their Kayakalp external assessment, while very few scored <70% [Table 1].
Table 2.
Correlation analysis
| Correlations | ||
|---|---|---|
| NQAS Score | Kayakalp Score | |
| NQAS score | ||
| Pearson’s correlation | 1 | 0.217 |
| Significant (two-tailed) | 0.234 | |
| n | 32 | 32 |
| Kayakalp score | ||
| Pearson’s correlation | 0.217 | 1 |
| Significant (two-tailed) | 0.234 | |
| n | 32 | 32 |
NQAS: National Quality Assurance Standards
As seen in Table 2, Pearson's correlation coefficient is 0.217, which shows that correlation sign is positive, signifying that there is some correlation between these two quality-of-care programs but of weak strength. However, Figure 1 shows scatter-plot chart representing vague distribution of dots along the X-axis and Y-axis which says nonlinear relationship between independent and dependent variables meaning that no correlation. Henceforth, it proves that our null hypothesis is correct and there is no correlation between NQAP and Kayakalp program.
Figure 1.
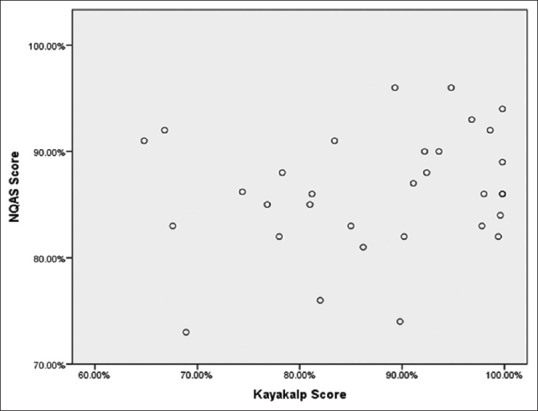
Scatter-plot diagram showing correlation between Kayakalp and NQAS)
DISCUSSION
Quality framework incorporated within NQAS and Kayakalp is based upon well-accepted “Donabedian model,”[7] which classifies quality of care into three components – structure, process, and outcome. NQAS program consists of eight major areas of concern, 74 standards, and approximately 808 checkpoints. On the other hand, Kayakalp consists of six thematic areas, 50 standards, and 500 checkpoints. On evaluation of checklist for both programs, it was found out that all standard used in Kayakalp checklist was taken out of NQAS checklist only. When we did a comparative analysis of standards common to both the programs, following result came out of the analysis: As depicted from Figure 2, in NQAS area named “infection control” covers only 14.6% of total scorecard, while in Kayakalp, this segment comprises 20% of total pie chart. On further digging deep into this, following observation are seen. As apparent from Table 3, standard A5 is only 8.87% of area of concern “Service Provision” which comprises of only 4.49% of total score under NQAS. This area of concern is comparable to hospital support services thematic area of Kayakalp. Similarly, others like Standard D4 comprises of 19.9% of are of concern “Support Services” which in turn holds only 15.95% under NQAS, is comparable to hospital upkeep thematic area of Kayakalp. Standard F6 is 24.15% of “Infection Control” area of concern which in turn comprises of 14.6% under NQAS. This area is comparable to waste management of Kayakalp. Standard B1 is 29.16% of area of concern patient rights, later accounts for 8.1% under NQAS. Standard D8, and D11 are 9.51% of support services which accounts for 15.95% under NQAS. All three (B1, D8 & D11) are comparable to hygiene promotion thematic area of Kayakalp. All earlier mentioned standards comprise little arc under the NQAS pie chart as compared to similar standards under Kayakalp, so this could also be an important reason for weak correlation of two programs.
Figure 2.
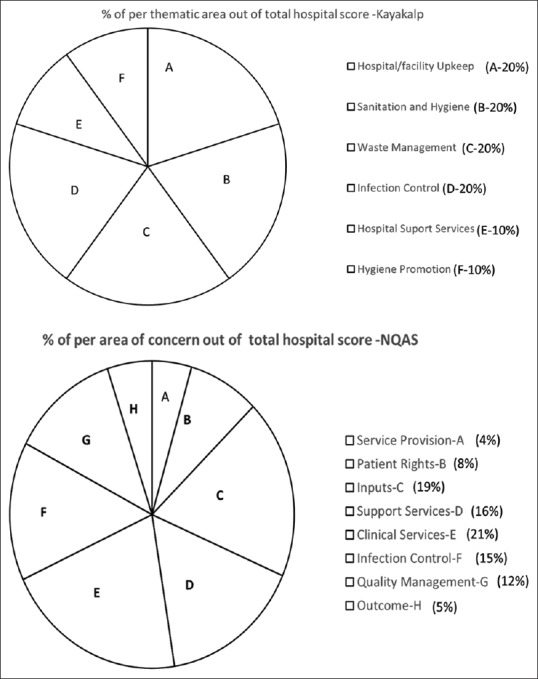
Graphical presentation for percentage of share by individual area of concern under NQAS and Kayakalp
Table 3.
Percentage of standard in their respective area of concern under National Quality Assurance Standards checklist
| Kayakalp thematic area | NQAS scorecard | |||
|---|---|---|---|---|
| Standard Name | Standard Score | Percentage of total of respective area of concern | Percentage of standard in their respective area of concern | |
| Hospital support services | Standard A5 | 52 | 8.87 | |
| Hospital upkeep | Standard D4 | 414 | 19.90 | |
| Waste management | Standard F6 | 460 | 24.15 | |
| Hygiene promotion | Standard B1 | 308 | 29.16 | |
| Standard D8 | 20 | 0.96 | 5.24 | |
| Standard D11 | 178 | 8.55 | ||
NQAS: National Quality Assurance Standards
Other possible reason could be with the sustainability of process variables under NQAS for long term as district hospital's Kayakalp score has been recorded for the current year (2017–2018) while there NQAS score could be from last 3 years. Hence, to achieve sustainable outcomes, continuous monitoring and evaluation of the already planned interventions under the program must be done along with the generation of evidence-based intervention outcomes.
Our result suggests that Kayakalp program is a subcomponent of NQAS program. If facility prepares themselves for certification against NQAS, they achieved their result through Kayakalp external assessment score initially, followed by quality certification against NQAS. For the continued achievement of desirable outcomes, sustainability of the continued use of program activities and components are required. There is symbiotic relationship between sustainability, outcome, and process. If one component is missing from this trilogy, it could have disbalance the desired results of the program.
We acknowledge the limitations of our analysis: (1) Sample size taken was small due to time constraint, and hence, it might have resulted in lower value of Pearson's correlation coefficient. (2) Less weightage given to standards of the Kayakalp checklist might lead to underestimated weightage analysis result.
CONCLUSION
Both the programs were launched by NHM to provide quality services to the community. Significant findings have come out of this study, one of which states no correlation between aforesaid program despite the presence of some similar standards for assessment. Another interesting finding comes to notice that facility's national assessment is a long process, and so, it needs several arrangements to be made such as training of the external assessors for assessment of facilities, sensitization of state nodal officers, facility doctors, and staff for this program, awareness of the program protocols and framework to the facilities, and long-term impact of programs. All of these processes need time for completion. As once the facility prepares itself for NQAS certification, in-directly, it prepares itself for Kayakalp external assessment as well.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We thank the quality improvement team of National Health Systems Resource Centre, New Delhi, who participated and helped in the completion of this study.
REFERENCES
- 1.Juran J. Total Quality Management. 2009. Jun 07, [Last accessed on 2018 Apr 27]. Available from: https://totalqualitymanagement.wordpress.com/2009/06/07/dr-joseph-juran/
- 2.Department of Health and Family Welfare. Operational Guidelines for Quality Assurances in Public Health Facilities 2013. India: Ministry of Health and Family Welfare; 2018. [Google Scholar]
- 3.Department of Health and Family Welfare. National Quality Assurance Standards for Public Health Facilities 2016. India: Ministry of Health and Family Welfare; 2018. [Google Scholar]
- 4.Department of Health and Family Welfare. Assessor's Guidebook for Quality Assurance in District Hospitals 2013. India: Ministry of Health and Family Welfare; 2018. [Google Scholar]
- 5.Department of Health and Family Welfare. Award to Public Health Facilities KAYAKALP 2015. India: Ministry of Health and Family Welfare; 2018. [Google Scholar]
- 6.Quality Improvement Division, National Health System Resource Centre. New Delhi: [Last accessed on 2018 Apr 27]. Available from: http://qi.nhsrcindia.org/nationalquality-assurance-standards . [Google Scholar]
- 7.India Records 5.2 Million Medical Injuries a Year. The Times of India. 2013. Sep 21, [Last accessed on 2018 Apr 27]. Available from: https://timesofindia.indiatimes.com/india/India-records-5-2-million-medical-injuries-a-year/articleshow/22832260.cms .
- 8.Omaswa F, Burnham G, Baingana G, Mwebesa H, Morrow R. Introducing quality management into primary health care services in Uganda. Bull World Health Organ. 1997;75:155–61. [PMC free article] [PubMed] [Google Scholar]
- 9.Chaudhury RR, Parameswar R, Gupta U, Sharma S, Tekur U, Bapna JS, et al. Quality medicines for the poor: Experience of the Delhi programme on rational use of drugs. Health Policy Plan. 2005;20:124–36. doi: 10.1093/heapol/czi015. [DOI] [PubMed] [Google Scholar]
- 10.Department of Health and Family Welfare. National Health Policy 2017. India: Ministry of Health and Family Welfare; 2018. [Google Scholar]