

Abstract
Objectives:
To assess the capacity and readiness of primary healthcare centers (PHC) for the implementation of basic strategies for the prevention and control of non-communicable diseases (NCDs) at the Ministry of National Guard-Health Affairs (MNG-HA) in Saudi Arabia.
Methods:
Facility-based face-to-face interviews were conducted in 41 PHCs included in this survey, using the World Health Organization (WHO) questionnaire. Main area survived were: availability of human resources, medical equipment, infrastructure, medicines, service utilization, referral systems, and community outreach.
Results:
Approximately 90% of the PHC centers were located in urban areas of the country. The level of staff training on NCD prevention and control strategies was reported to be inadequate, particularly for nurses and other healthcare providers. As for diagnostic equipment, diagnostic tests, essential medication, access to referral facilities and medical records most of them were available in all the PHCs among the different categories.
Conclusions:
The MNG-HA PHCs appear to have the capacity to integrate strategies for the prevention and control of NCDs as part of their daily functions. However, improvements are required in some areas to facilitate the integration process and training the health care workers (HCWs) on prevention and control of NCDs as part of their daily practice.
The prevalence and impact of non-communicable diseases (NCDs) is growing at a remarkable rate.1 Currently, NCDs, such as cardiovascular diseases, diabetes, cancer, chronic lung diseases account for approximately 60% of all deaths worldwide, with 80% of these deaths occurring in developing countries.2 In Saudi Arabia, epidemiological data indicate an alarming increase in the incidence and prevalence of NCDs, which are responsible for 70% of all deaths in this country.3 The World Health Organization (WHO) develop a strategy to assess some specific areas in the primary health care (PHC) centers regarding the prevention and control of NCD. Among the key objectives of the WHO Global NCD Action Plan 2013–2020, is strengthening and reorienting health systems towards the health promotion, prevention and control of NCDs and the underlying social determinants through people-centered PHC and universal health coverage.4
The Kingdom of Saudi Arabia (KSA) have developed and implemented sound and sustainable National Disease Control Programs (NDCPs), which are essential to strengthen public health approaches to prevention and control activities, with a special focus on PHC settings. Moreover, the NDCPs fit into the broader of the WHO framework as part of the implementation of the Action Plan for the Global Strategy for the Prevention and Control of NCDs, which was endorsed by the World Health Assembly in May 2008 and reemphasized in 2011.1 Strategy for prevention and control of NCD in KSA are clearly stated in the policies and strategies of Ministry of Health, and have been reemphasized recently through the Saudi Arabia Ministry of Health Initiatives,5 and Saudi Vision 2030,6 which addressing the elements of the WHO Global Action Plan (2018).7 Assessment of primary healthcare services at PHC centers is a vital step in improving their roles in health promotion, disease prevention, early detection, and integrated care. This information is required to highlight the main barriers to the implementation of processes for NCD prevention in addition to early detection and control strategies in PHC facilities in the KSA. Information obtained from this study will provide the evidence-base to devise policies and strategies for integrating the NCD interventions within the existing PHC services. This study was conducted with the aim to assess the capacity and readiness of primary healthcare centers (PHC) for the implementation of basic strategies for the prevention and control of NCDs at the Ministry of National Guard-Health Affairs (MNG-HA) in KSA.
Methods
A cross-sectional design was used to survey 41 out of 75 PHC facilities affiliated to the MNG-HA in 3 main regions of KSA; Central, Western and Eastern regions between January 2014 and January 2015. These centers were classified as A, B, C, and D based on their capacity, human resources, size of catchment area, and type of services provided. Class A centers have family medicine physicians, general practicioners (GPs), and other specialty professionals. Class B centers have only family medicine physicians and GPs. Class C centers have either family medicine physicians or GPs to serve small catchment areas and/or military employees. Class D centers belong to the remote military posts. Each PHC center covers a specific catchment area plus other patients referred from other regions in KSA.8 A total of 41 PHC centers included in this study were provide a wide spectrum of healthcare services, including curative, preventive, and rehabilitation services across the 3 regions in the kingdom and they meet the inclusion criteria (providing curative and preventive healthcare services).
Ethical approval was obtained from the Ethics Committee of the King Abdullah International Medical Research Center (RC12/084/R), Jeddah, KSA. In addition, verbal informed consent was provided by all the respondents before the start of each interview.
A rapid standardized WHO assessment package tool (WHO-PEN) was used to assess the capacity of the PHC services in preventing and control of NCDs.9 It consist of 33 questions designed to gather data on the following areas: service utilization, facility classification, served population, infrastructure, human resources, equipment, and diagnostic tests, available medications, funding and administration, medical information system, and referral services. The assessment focused on the availability of biochemical tests (n=7), basic instruments (n=17), technical procedures (n=18), medicines and medical information systems (n=27), and basic NCD interventions (n=14). Face to face interview with the key informants (director) in each PHC center was conducted.
Measuring scores
In this study, the readiness score of the primary health care centers was calculated through the use of 5 domains: basic equipment, essential services, diagnostic investigation capacity, counseling services, and availability of essential medicines. For each domain, we calculated an index as the mean score of items expressed as percentage in each domain. A code score of “1” as “available/present”, and the score of “0” for “no”. Accordingly, the PHC category readiness index was then calculated as the average of domain indices. To facilitate comparison and display a level of readiness, a cut-off point of 70% was constructed, as it was used in many previous studies elsewhere.10 Therefore, those PHC categories above the 70% reflects the readiness of the underlining specific domain to manage the NCDs. In the other side, those PHC categories under the line indices was considered as ‘not ready’ to manage NCDs at that level.
Statistical analysis
Descriptive statistics was used to present the data as number and percentage (%) values (categorical variables) or mean±SD (continuous variables). Moreover, we used Fisher’s exact test to assess differences in essential medicine availability in different PHC center variables, and the one-way analysis of variance (ANOVA) was applied to present association between type of PHC center’s category and the different domain index of the readiness. All statistical analyses were carried out using the Statistical Package of Social Science (SPSS) version 20 (SPSS Inc., Armonk, NY, USA), and the threshold for statistical significance was set at p<0.05.
Results
Characteristics of the surveyed PHC centers
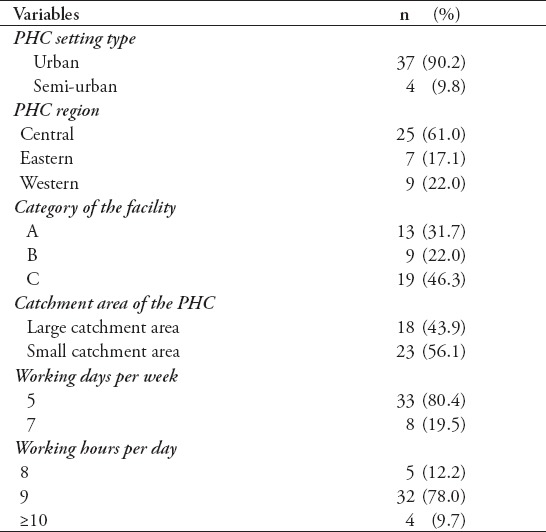
The majority of existing PHC centers are located in urban areas (37/41, 90.2%), and approximately half classed as type C (46.3%). Twenty-three (56.1%) of the PHC centers covered small catchment areas compared to 18 (43.9%) covering large catchment areas. Concerning the working hours, more than 80% of these centers worked 5 days a week, and only 8 (19.5%) provided their services 7 days a week. The majority of the PHC centers (90%) worked 8-9 hours per day (Table 1).
Table 1.
Characteristics of surveyed primary healthcare (PHC) facilities, National Guard-Health Affairs, Saudi Arabia (N=41).
Human resources capacity. An overall low level of training offered to the health care providers including doctors, nurses or other health care staff working in all the PHC setting. In particular, the PHC centers type C have received very low or none training to improve their performance.
Availability of basic diagnostic equipment and diagnostic tests
Among the 16 items of diagnostic equipment surveyed, 10 were available and functioning in almost all the PHC facilities. In contrast, some equipment, such as the vaginal speculum and pap smear kits, were not available in most of the category C facilities due to the limited functions of these centers in terms of obstetrics and gynecology services. All basic diagnostic tests were available in every PHC such as urine albumin/protein, urine glucose/sugar, urine ketone bodies, blood sugar, troponin, blood cholesterol, and serum creatinine were all available in all the centers with 100%. Variation was reported between centers in the implementation of the NCD interventions techniques such as ECG ( 61%), peak flow test (78%), and digital rectal examination (75.6%).
Access to essential medicines for NCDs in PHC facilities and referral facilities
With no charge and regular supply of 36 types of medications related to anti-diabetic, anti-hypertension drugs, analgesics, basic antibiotics, and those related to heart diseases were available in all 41 PHC facilities. Referral services such as referral to another facility, referral for a second opinion regarding NCDs, referral for NCD screening, as well as the ability of file retrieval and consultation on each visit to the facility were available and applicable in all the 41 PHC centers (100%).
Index of readiness to integrate and manage NCDs in PHC centers
The Post Hoc (Tukey HSD) analysis was performed to assess differences in domains subscales across PHC categories (A, B, and C). There is a remarkable difference of equipment availability score found in category C (diff. 10.6, p=0.003) compare to category A and B (diff. 11.6, p=0.005) (Figure 1A). Similarly, category C was significantly different from category A (diff. 26.2, p=0.001) and category B (diff. 20.6, p=0.018) in the essential services. There is no difference in score belongs to the other 3 domains (availability of diagnostic test, counselling, and medication) between PHC categories (p>0.05) (Figures 1C-1E).
Figure 1.
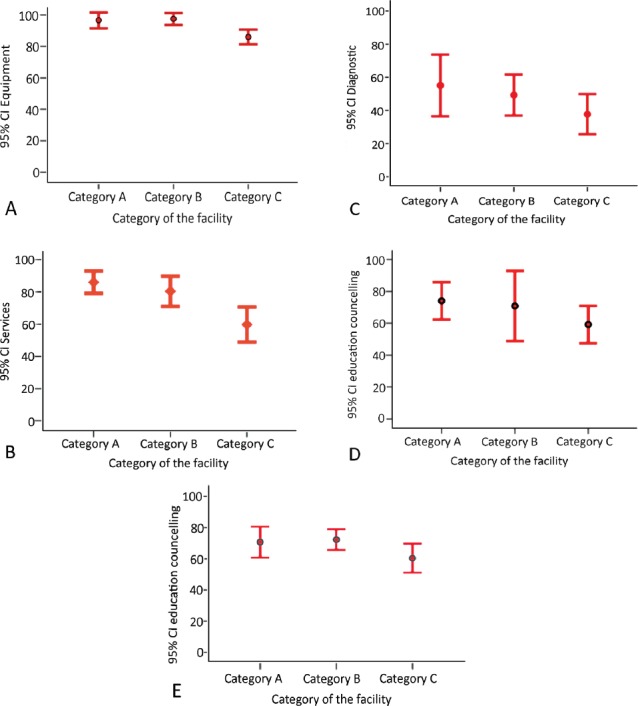
Post hoc test for readiness in A) basic equipment, B) essential services, C) investigation, D & E) counselling, and available medication between the PHC categories.
Despite a clear variation in the subscales of each domain in the study, the most 2 domains (equipment availability, and essential services) displayed the highest percentage over 70% cut-off point, when measuring the readiness index for managing NCDs in PHC centers with an overall score of 92% and 73%, respectively (Figure 2). The overall score of the other 2 domains (counselling sessions, and availability of medicines, 66% for each) were found near the border line but below 70%, while the least overall score below the 70% cut-off belongs to the availability of diagnostic investigations (46%).
Figure 2.
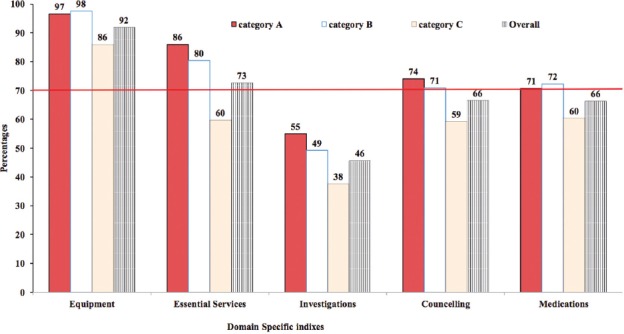
Indexis of readiness to manage non-communicable diseases (NCDs) in primary healthcare centers (PHC) centers. The red horizontal line indicates the 70% cut-off for the domain specific index by PHC category.
Discussion
The aim of this study was to assess the capacity of the PHC centers at the MNG-HA to cope with the prevention, early detection and control of NCDs. Some moderate-to-major deficiencies related to the training in the prevention, early detection and management of NCDs were identified.
It is the first time in Saudi Arabia to use the WHO PEN tool to assess the readiness of the PHC centers in the country to manage NCDs. Our findings are not unique to Saudi Arabia, similar studies were conducted in other countries where marked deficiencies were found in health system infrastructure, workforce capacity, surveillance, planning, policy, and program management.10-13 Our study has revealed that nearly all PHC facilities of category (A and B) could meet the minimum threshold to manage NCDs in line with WHO recommendations. It brings to focus the need to empower category (C) PHC centers to deliver NCD interventions consistent with their level of care as has been carried out elsewhere with satisfactory results. Some of the findings from our study such as inadequate level of training, insufficient skills in using some intervention technologies for diagnosis and early detection, and an absence of clear guidance and policy for the inclusion of promotion and prevention initiatives such as tobacco secession, dietary health education, strengthening physical activity programs and infrastructure could have a great influence in the implementation of a comprehensive approach based on promotion, prevention, early detection and control of the NCDs in the PHC facilities surveyed.
Although, this study has a limitation to explain causative linkages across the different domains (cross-sectional design), the findings showed the applicability and adequacy of the WHO PEN used tool to capture the different domains of health system and it is ability to distinguish performance across the domains in different PHC centers. Therefore it is useful to be apply across the Saudi Arabia health sectors.
In conclusions, the findings of this study showed no critical gap in the capacity related to the main areas of the essential PHC services to integrate and manage NCDs, such as the availability of basic equipment, basic diagnostic tests, medication, and access to referral facilities and medical records. These findings support the growing consensus that strengthening the primary health care centers, is a prerequisite for scaling up prevention and control of NCDs in the country. Similar study should be conducted at PHC centers of the Ministry of Health and other Health related sector to review their current approach to NCD care at the primary care level.
Acknowledgments
The King Abdullah International Medical Research Center (KAIMRC), Ministry of the National Guard Health Affairs financed the data collection process and associated requirements for this study. We wish to acknowledge helpful role of Dr. Salwa Bahkaly for her support in the collection of the study data.
Footnotes
References
- 1.World Health Organization. [cited 2008];The world health report 2008 - primary health care now more than ever. Available from URL:http://www.who.int/whr/2008/en/
- 2.World Health Organization. [cited 2011];Global Status Report on Noncommunicable Diseases 2010. Available from URL:http://www.who.int/nmh/publications/ncd_report2010/en/ ISBN 978 92 4 156422 9 .
- 3.World Health Organization. [cited 2013];Country cooperation strategy for WHO and Saudi Arabia 2012 - 2016. Available from URL:Mediterranean WROftE:25.www.emro.who.int/about-who/country-cooperation-strategy/
- 4.World Health Organization. [cited 2018];Assessing national capacity for the prevention and control of noncommunicable diseases:report of the 2017 global survey. Available from URL:https://apps.who.int/iris/bitstream/handle/10665/276609/9789241514781-eng.pdf .
- 5.Ministry of Health. [cited 2019];The MOH Initiatives Related to the NTP 2020 and Saudi Vision 2030. Available from URL:https://www.moh.gov.sa/en/Ministry/nehs/Pages/vision2030.aspx .
- 6.Saudi Vision 2030. [cited 2019];National Transformation Program (2030) Available from URL:http://vision2030.gov.sa/en .
- 7.World Health Organization. [cited 2018];Global Action Plan on Physical Activity 2018-2030:More Active People for a Healthier World. Available from URL:https://www.who.int/ncds/prevention/physical-activity/global-action-plan-2018-2030/en/
- 8.Ministry of National Guard Health Affairs. [cited 2009];Health report of the National Guard for Health Affair. Available from:http://ngha.med.sa/english/medicalcities/AlRiyadh/FMPHC/Pages/default.aspx .
- 9.World Health Organization. [cited 2010];Package of essential noncommunicable disease interventions for primary health care in low-resource settings. Available from URL:https://www.who.int/nmh/publications/essential_ncd_interventions_lr_settings.pdf .
- 10.Mutale W, Bosomprah S, Shankalala P, Mweemba O, Chilengi R, Kapambwe S, et al. Assessing capacity and readiness to manage NCDs in primary care setting: Gaps and opportunities based on adapted WHO PEN tool in Zambia. PloS One. 2018;13:e0200994. doi: 10.1371/journal.pone.0200994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nyarko KM, Ameme DK, Ocansey D, Commeh E, Markwei MT, Ohene S-A. Capacity assessment of selected health care facilities for the pilot implementation of package for essential non-communicable diseases (PEN) intervention in Ghana. Pan Afr Med J. 2016;25(Suppl 1):16. doi: 10.11604/pamj.supp.2016.25.1.6252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rogers HE, Akiteng AR, Mutungi G, Ettinger AS, Schwartz JI. Capacity of Ugandan public sector health facilities to prevent and control non-communicable diseases:an assessment based upon WHO-PEN standards. BMC Health Serv Res. 2018;18:606. doi: 10.1186/s12913-018-3426-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Islam MR, Laskar SP, Macer D. A Study on Service Availability and Readiness Assessment of Non-Communicable Diseases Using the WHO Tool for Gazipur District in Bangladesh. Bangladesh Journal of Bioethics. 2016;7:1–13. [Google Scholar]