

Abstract
Objectives:
To determine the prevalence of sarcopenia and related factors in individuals aged ≥65 years living in the Bornova district of Izmir, Turkey. Sarcopenia is one of the most serious health problems among elderly individuals.
Methods:
This cross-sectional study was conducted in the Bornova district of Izmir, Turkey, between February-July 2015. This study participants were comprised of 909 individuals aged ≥65 years. The dependent variable was the presence of sarcopenia and the European Working Group on Sarcopenia in Older People (EWGSOP) approach was used for determining sarcopenia. The independent variables were socio-demographic and economic characteristics, healthy life behaviors and health status/condition. Data were collected at home through face-to-face interviews and measurements, analysed using chi-square test, t-test and logistic regression analysis.
Results:
The participants’ mean age was 72.8±6.2 (range: 65-100) years, and 60.2% were female (n=582). The prevalence of sarcopenia was 5.2% and that of low gait speed was 41.0%, low grip strength was 57.0%, low calf circumference was 6.1% and the combination of low gait speed and low grip strength was 14.3%. Risk factors of sarcopenia included increasing age, physical inactivity, low body mass index and the presence or risk of malnutrition.
Conclusion:
The prevalence of sarcopenia was 5.2% in this population and increased with age, physical inactivity, low body mass index and the presence or risk of malnutrition.
The European Working Group on Sarcopenia in Older People (EWGSOP) proposed the definition of sarcopenia to be a syndrome characterized by progressive and generalized loss of skeletal muscle mass.1 Compared to other age groups, the incidence is higher in elderly individuals; thus, it can be described as a geriatric syndrome.1 Studies have reported that sarcopenia is not only associated with several diseases, but also decreases the quality of life and increases dependence, mortality and hospitalisations.1,2 Prevalence depends on the location of the study, the indices used or measures, and the age group. For example, the prevalence is higher in elderly individuals who are hospitalised or are living in nursing homes than in those living in communities. In community-based studies, the prevalence of sarcopenia varies between 1-29%, with an incidence range of 5-13% at 60-70 years and 11-50% at >80 years.1,3 Other risk factors include female gender, low birth weight, genetic predisposition, malnutrition, inadequate protein intake, alcohol and cigarette consumption, physical inactivity, immobilisation and chronic diseases.1 Studies conducted in Turkey were mainly on the elderly residing in nursing homes or hospitals. There was only one published community-based study in Turkey whose objective was to determine the prevalence of muscle function-dependent sarcopenia; among the 89,303 elderly invited to participate, only 879 showed up at the Family Health Center.4
The aim of our study was to determine the prevalence of sarcopenia and related factors in community-dwelling individuals of 65 and above, residing in the Bornova district of Izmir, Turkey.
Methods
This study was part of a larger project aimed to determine the prevalence of sarcopenia among community-dwelling elderly, the affecting factors and the consequences of sarcopenia, such as depressive symptoms and functional status. The latter was explained elsewhere and details of methods are also available.5
This was a cross-sectional, community-based study conducted in the Bornova district of Izmir, Turkey, between February-July of 2015. According to the Address-Based Population Registration System 2014 published by the Turkish Statistical Institute, the study population comprised 28,323 community-dwelling individuals aged ≥65 years living in the Bornova district of Izmir, Turkey. The minimum sample size was calculated to be 839 elderly individuals, assuming a prevalence of sarcopenia of 10%, at a 2% error rate and 95% confidence interval. After considering the design effect as 1.2, the aim was to access a minimum sample size of 1007 individuals. A multi-stage sample selection was conducted. According to municipality registrations, the neighbourhoods in the district were stratified as low, middle and high socioeconomic status. Using a random numbers table, a neighbourhood was selected from each socioeconomic strata. All the existing streets were listed in those neighbourhoods and then streets were randomly selected to reach enough participants. All the elderly residing on those streets were included in the study. As a result, the final sample included 909 elderly participants (namely, a 90.3% response rate).
Variables
In this study, sarcopenia was the dependent variable, whereas age, gender, educational status, marital status, food insecurity, house ownership, cohabitants, access to social support, physical activity, body mass index (BMI), presence of malnutrition, co-morbidities (diabetes mellitus, hypertension, cancer, heart disease and chronic obstructive pulmonary disease) and the number of routinely used medications (regardless of whether they were prescribed or not), were the independent variables.
Sarcopenia was defined according to the EWGSOP approach, which recommends 3 primary outcome variables, namely, low muscle mass, low muscle strength and low physical performance.1 Muscle mass was measured via the calf circumference (CC), where a CC of <31 cm corresponded to low muscle mass.6 Muscle strength was measured using the Takei T.K.K. Grip D digital hand grip dynamometer (Takei Scientific Instruments Co. Ltd, Tokyo, Japan). Three measurements were taken, and the highest measurement corresponded to the final strength of the dominant hand. A muscle strength of <30 kg for men and <20 kg for women was classified as low.7 Physical performance was assessed using the usual gait speed (over a 6-m course); unlike EWGSOP criteria, a gait speed of <1 m/s is considered slow.8 Educational status was determined as the highest-grade level from which a participant graduated. Social support was established using the question ‘Is there anybody that you could call and get support from if you needed it?’ For chronic diseases, a physician’s diagnosis was requested, and the participants’ own statements were evaluated. Malnutrition was ascertained via the Mini Nutritional Assessment-short form (MNA-SF) tool, where a score of 12-14 indicates well-nourished, 8-11 indicates a risk of malnutrition and <8 indicates malnutrition.9 Body mass index was obtained by dividing the body weight (kg) by the square of height (m2).10 Weight and height measurements were taken by interviewers at home when the participants were wearing light clothes and no shoes. For weight measurement, a digital scale was used, whereas height measurements were conducted with a portable stadiometer on a Frankfurt plane. To determine food insecurity, the following 3 questions were asked based on the protocol described in the Nutrition Survey of the Elderly in New York State (NSENY): ‘Do you have enough money to buy the food you need most of the time?’; ‘In the past 6 months, have you skipped one or more meals because you had no food in the house or because you thought that soon you might not have enough food?’; and the final question was ‘In the past 6 months, have you had to choose between buying food and paying bills or buying something else you needed?’. An affirmative response to at least one of these questions was evaluated as ‘food insecurity’.11 The Physical Activity Scale for Elderly (PASE) was used to identify the physical activity status. The Turkish version of the PASE has previously been shown as a valid and reliable tool by Ayvat et al.12
Data collection
Data was collected through face-to-face interviews conducted in the participants’ homes by trained interviewers comprised of nutrition and dietetic students. Prior to the study, there were 3 training sessions for the interviewers administered by the 3 academician authors of this study: a geriatrist, a physician with a public health PhD and a dietician with a public health PhD. In the first session, the questionnaire was presented; in the second, all the anthropometric measurements, gait speed and hand grip measurements were explained in detail and then practiced; in the third and final session, interpersonal relationships and communication skills were enriched. As a pilot study, the questionnaire was administered to individuals 65 years or older from outside the study universe. Researchers checked the data collection process weekly. The homes of each participant were visited on 3 occasions, once during the day, once in the late afternoon-evening and once on the weekend. The participants who did not complete the interviews in 3 visits were excluded from the study.
Ethical approval
This study was approved by the Ethics Committee of Izmir Bozyaka Education and Research Hospital in Izmir, Trurkey (4/2014). This study was carried out in accordance with the principles of Helsinki Declaration and written-informed consents were obtained from the participants.
Statistical analysis
Data was analysed using Statistical Package for the Social Sciences (SPSS) version 15.0 (SPSS Inc., Chicago, IL, USA). Continuous data are presented as mean±standard deviation, and categorical variables are presented as percentages. The Chi-square test was used to determine the relationship between variables and t-tests were conducted to compare means. and a univariate analysis and multivariate logistic regression (LR) model were used to identify factors associated with sarcopenia. The multivariate LR model was conducted using variables that were found to be significant in the univariate analyses. In order to abstain from collinearity, for the variables which were found to be highly correlated, only one of them was included in the model (namely, the number of chronic diseases was highly correlated with the number of routinely used drugs; thus, only the number of chronic diseases was included in the model). The significance level was set at p<0.05. Multivariate LR results were evaluated with OR (95% confidence intervals [CI]) and p-values.
Results
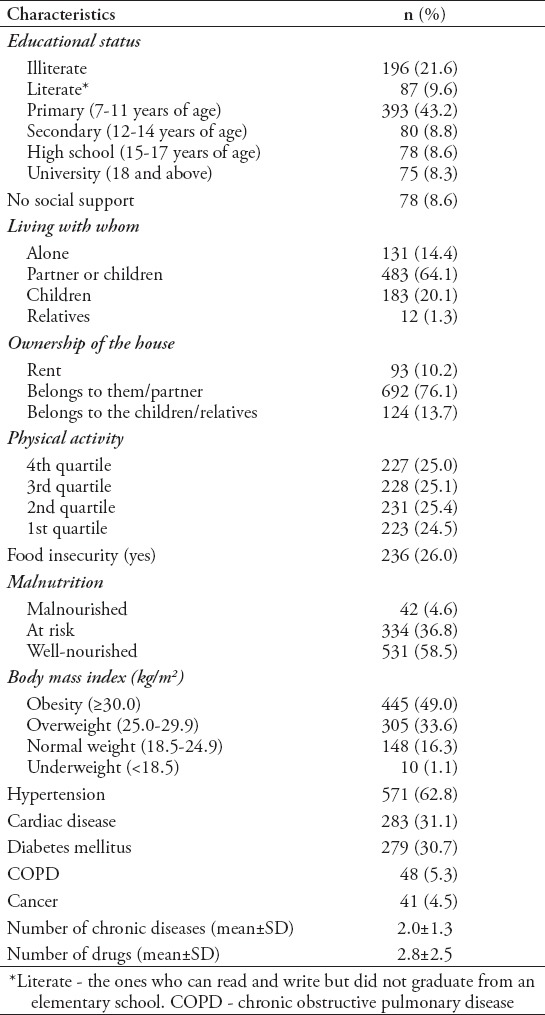
A total of 909 elderly participants were included, of whom 59.2% were female and 65.7% were married. The mean age of participants was 72.4±5.9 (range: 65-98) years. Other demographic characteristics of participants are presented in Table 1.
Table 1.
Descriptive characteristics of the study participants.
The participants had a mean gait speed of 1.4±0.9 m/s, mean grip strength of 23.8±10.3 and a mean CC of 37.4±4.5 cm. Frequencies of the diagnostic algorithm according to the EWGSOP are presented in Figure 1. The prevalence of sarcopenia was 5.2% (female: 4.1%, male: 6.7%).
Figure 1.
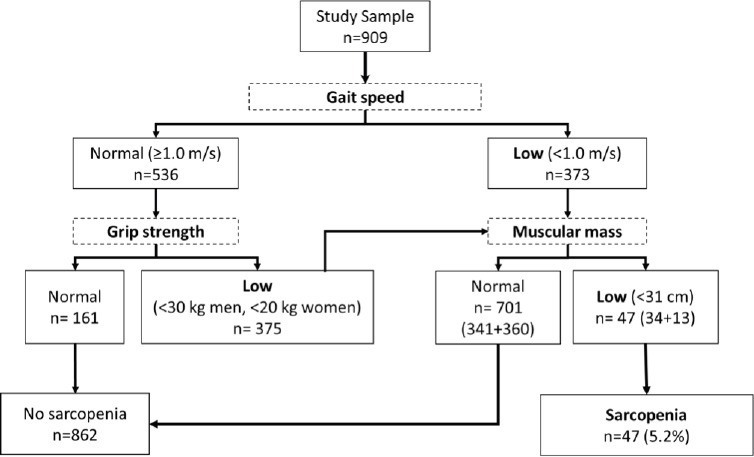
Frequencies of the diagnostic algorithm.
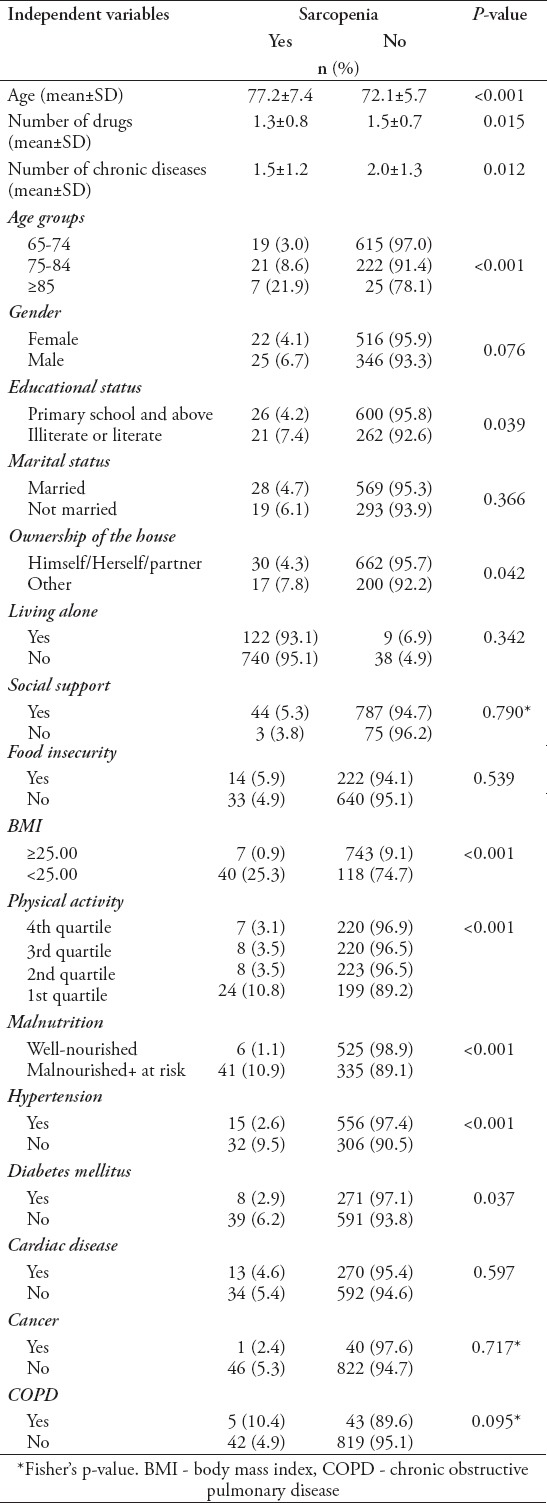
Univariate analysis revealed that all independent variables, along with aging, such as gender, marital status, presence of social support, food insecurity and the presence of cardiac disease, cancer and chronic obstructive pulmonary disease, were factors associated with sarcopenia (Table 2).
Table 2.
Association between independent variables and sarcopenia (univariate analysis).
According to the LR analysis, increasing age (OR=1.086, 95% CI: [1.024-1.152], p=0.006), low physical activity (OR=3.262, 95% CI: [1.055-10.080], p=0.040), low BMI (OR=24.853, 95% CI: [10.147-60.869], p<0.001) and the presence or risk of malnutrition (OR=8.006, 95% CI: [3.069-20.885], p<0.001) significantly increases the risk of sarcopenia (Table 3).
Table 3.
Association between independent variables and sarcopenia (logistic regression analysis).

Discussion
The present study evaluated sarcopenia and related factors in community-dwelling elderly individuals living in the Bornova district of Izmir, Turkey. In this study, the prevalence of sarcopenia was 5.2% and was determined using 3 instruments; handgrip strength was measured using a handgrip dynamometer, physical performance was measured via the usual gait speed and muscle mass was determined through the calf circumference. Each of these methods is an important tool for screening because they are easily applicable, non-invasive, simple and low-cost. In addition, the World Health Organization (WHO) has accepted calf circumference measures as the most sensitive anthropometric criterion for the measurement of muscle mass in elderly individuals.13 The EWGSOP was revised in 2019.14 Thus, according to EWGSOP criteria, calf circumference measures may be used as a diagnostic proxy for older adults in settings where no other muscle mass diagnostic methods are available.14
The prevalence of sarcopenia varies according to study location (country/community/institution/hospital), age group, gender distribution and diagnostic schemes and tools. A previous cross-sectional study reported that the prevalence of sarcopenia varied between 0-45.2% according to different criteria and age groups.15 A systematic review of individuals aged ≥50 years reported that differences in age and living areas could affect the prevalence of sarcopenia; reported to be 1-29% in community-based studies, 14-33% in long-term care patients and 10% in an acute hospital care group.3
Other previous studies have reported that the prevalence of sarcopenia is 12.5% among the elderly aged ≥80 years in Belgium, 7.5% among those aged ≥65 years in Japan, 4.8% among the individuals aged ≥65 years in Brazil, 4.5% among those aged ≥70 years in Germany and 7.1% among those aged ≥65 years in Taiwan.16-21 Our results are similar to these findings.
In Turkey, studies focusing on sarcopenia were mostly conducted on the elderly residing in nursing homes or individuals who were hospitalized. Moreover, different methods were used to define sarcopenia and this resulted in a varying range of sarcopenia prevalence. Among the elderly residing in nursing home, the prevalence was observed to be 29.0-85.4% and among the elderly who were admitted to hospital, it was 10.5-49.0%.22-26 The only study published on community-dwelling elderly found muscle function sarcopenia (via gait speed and hand grip) prevalence as 63.4%; whereas, according to muscle mass via calf circumference, it was determined to be 6.7%.4 The main issue with this study was the concerns about sample selection because the study was conducted only on volunteers who agreed to come to family health centres to participate in the study (among the 89,303 elderly, only 879 participated).
Our present study determined that increasing age, physical inactivity, low BMI or the presence or risk of malnutrition are risk factors for sarcopenia. Consistent with these results, several studies have reported that increasing age, low BMI and physical inactivity are associated with sarcopenia.4,16-18,21-29 Although only a limited number of community-based studies have investigated malnutrition as a factor, all these studies have reported a relationship between malnutrition and sarcopenia.18,21 Some studies have indicated a higher prevalence of sarcopenia in females, whereas others have found a higher prevalence among males.4,21,30 Socio-economic factors have been studied less frequently and have generally not been found to be related with sarcopenia.16 This could be due to a lack of significant differences in the socio-economic aspects of the study groups. In general, the socio-economic gap between the elderly may diminish because of factors such as retirement or unemployment. Furthermore, no significant differences are observed in the level of education among the elderly. Some studies have reported that the number/presence of chronic diseases increases the prevalence of sarcopenia, whereas others have found no such relationship.16,21,27,29 In the present study, univariate analysis revealed that the lack of a chronic disease, such as hypertension or diabetes, is a risk factor for sarcopenia. However, this factor did not persist in the multivariate analysis, the results of which can be explained by the presence of chronic disease in majority of individuals constituting the study group.
Limitations
The main limitation of the present study was that compared with other causality studies, the value of causal evidence are limited by the cross-sectional nature of this study. Moreover, because the study was conducted in Izmir, Turkey alone, its results cannot be generalised to elderly individuals worldwide. Our study aimed to determine sarcopenia prevalence among a community-dwelling elderly population, within their home circumstances. Thus, we were not able to use gold standard methods, such as Dual-energy X-ray absorptiometry, Computed tomography or Magnetic resonance imaging in determining muscle mass. Instead, we chose to use calf circumference measurements, the best option available for a home setting, as a surrogate for muscle mass. Not using gold standard methods for muscle mass may be considered a limitation; however, optimizing our measurements in accordance to our aim can also be evaluated to be a strength.
The main strengths of the study were its community-based nature, the method used to calculate sample size and the high rate of access to the target population, all of which prevented selection bias. The use of the EWGSOP approach, which has been recently more frequently used as a diagnostic tool, qualifies as another strength of this study. Data standardization was ensured both by the training provided to interviewers and weekly data controls. The study results can serve as a guide to determine factors associated with sarcopenia in the elderly population.
In conclusion, sarcopenia has a considerable prevalence in society, and its risk increases with age, physical inactivity, low BMI or the presence or risk of malnutrition. It is important to correctly diagnose sarcopenia, which is common in elderly individuals and associated with their mortality and morbidity. A program should be developed whereby the elderly can be monitored by primary care institutions within the home setting, and healthcare workers can be trained to raise their awareness regarding sarcopenia to reach and diagnose the elderly who are homebound and unable to receive health services. By taking into account the factors associated with sarcopenia and its association with malnutrition and low BMI, physicians may be guided in the diagnosis of sarcopenia. Age is not a preventable factor, but active ageing, (namely, ensuring that the elderly are physically active) should be targeted. Although health workers have an important role in motivating the elderly, the public districts should provide an environment whereby individuals can both engage in and maintain an active lifestyle.
Acknowledgment
The authors gratefully acknowledge JoAnne Aliye Noonan Kutup for English language editing.
Footnotes
References
- 1.Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia:European consensus on definition and diagnosis:Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–423. doi: 10.1093/ageing/afq034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cruz-Jentoft AJ, Landi F, Topinková E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Curr Opin Clin Nutr Metab Care. 2010;13:1–7. doi: 10.1097/MCO.0b013e328333c1c1. [DOI] [PubMed] [Google Scholar]
- 3.Cruz-Jentoft AJ, Landi F, Schneider SM, Zúñiga C, Arai H, Boirie Y, et al. Prevalence of and interventions for sarcopenia in ageing adults:a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS) Age Ageing. 2014;43:748–759. doi: 10.1093/ageing/afu115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Akın S, Mucuk S, Öztürk A, Mazıcıoğlu M, Göçer Ş, Arguvanlı S, et al. Muscle function-dependent sarcopenia and cut-off values of possible predictors in community-dwelling Turkish elderly:calf circumference, midarm muscle circumference and walking speed. Eur J Clin Nutr. 2015;69:1087–1090. doi: 10.1038/ejcn.2015.42. [DOI] [PubMed] [Google Scholar]
- 5.Kilavuz A, Meseri R, Savas S, Simsek H, Sahin S, Bicakli DH, et al. Association of sarcopenia with depressive symptoms and functional status among ambulatory community-dwelling elderly. Arch Gerontol Geriatr. 2018;76:196–201. doi: 10.1016/j.archger.2018.03.003. [DOI] [PubMed] [Google Scholar]
- 6.Rolland Y, Lauwers-Cances V, Cournot M, Nourhashémi F, Reynish W, Rivière D, et al. Sarcopenia, calf circumference, and physical function of elderly women:a cross-sectional study. J Am Geriatr Soc. 2003;51:1120–1124. doi: 10.1046/j.1532-5415.2003.51362.x. [DOI] [PubMed] [Google Scholar]
- 7.Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, et al. Age-associated changes in skeletal muscles and their effect on mobility:an operational diagnosis of sarcopenia. J Appl Physiol. 2003;95:1851–1860. doi: 10.1152/japplphysiol.00246.2003. [DOI] [PubMed] [Google Scholar]
- 8.Cesari M, Kritchevsky SB, Newman AB, Simonsick EM, Harris TB, Penninx BW, et al. Added value of physical performance measures in predicting adverse health-related events:results from the Health, Aging And Body Composition Study. J Am Geriatr Soc. 2009;57:251–259. doi: 10.1111/j.1532-5415.2008.02126.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice:developing the short-form mini-nutritional assessment (MNA-SF) J Gerontol A Biol Sci Med Sci. 2001;56:M366–M372. doi: 10.1093/gerona/56.6.m366. [DOI] [PubMed] [Google Scholar]
- 10.WHO. Global Database on Body Mass Index [Internet] [Accessed 10 October 2014];World Health Organization. 2014 Available from:http://www.who.int/bmi/index.jsp?introPage=intro_3.html . [Google Scholar]
- 11.Lee JS, Frongillo EA. Factors associated with food insecurity among US elderly persons:importance of functional impairments. J Gerontol Soc Sci. 2001;56:94–99. doi: 10.1093/geronb/56.2.s94. [DOI] [PubMed] [Google Scholar]
- 12.Ayvat E, Kilinç M, Kirdi N. The Turkish version of the Physical Activity Scale for the Elderly (PASE):its cultural adaptation, validation, and reliability. Turk J Med Sci. 2017;47:908–915. doi: 10.3906/sag-1605-7. [DOI] [PubMed] [Google Scholar]
- 13.Physical status:the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452. [PubMed] [Google Scholar]
- 14.Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia:revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16–31. doi: 10.1093/ageing/afy169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bijlsma AY, Meskers CG, Ling CH, Narici M, Kurrle SE, Cameron ID, et al. Defining sarcopenia:the impact of different diagnostic criteria on the prevalence of sarcopenia in a large middle aged cohort. Age (Dordr) 2013;35:871–881. doi: 10.1007/s11357-012-9384-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Legrand D, Vaes B, Matheï C, Swine C, Degryse JM. The prevalence of sarcopenia in very old individuals according to the European consensus definition:insights from the BELFRAIL study. Age Ageing. 2013;42:727–734. doi: 10.1093/ageing/aft128. [DOI] [PubMed] [Google Scholar]
- 17.Yoshida D, Suzuki T, Shimada H, Park H, Makizako H, Doi T, et al. Using two different algorithms to determine the prevalence of sarcopenia. Geriatr Gerontol Int. 2014;14:46–51. doi: 10.1111/ggi.12210. [DOI] [PubMed] [Google Scholar]
- 18.Alexandre TDS, Duarte YAO, Santos JLF, Lebrão ML. Prevalence and associated factors of sarcopenia, dynapenia, and sarcodynapenia in community-dwelling elderly in São Paulo - SABE Study. Rev Bras Epidemiol. 2019;21:e180009. doi: 10.1590/1980-549720180009.supl.2. [DOI] [PubMed] [Google Scholar]
- 19.Yamada M, Nishiguchi S, Fukutani N, Tanigawa T, Yukutake T, Kayama H, et al. Prevalence of sarcopenia in community-dwelling Japanese older adults. J Am Med Dir Assoc. 2013;14:911–915. doi: 10.1016/j.jamda.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 20.Kemmler W, Teschler M, Goisser S, Bebenek M, von Stengel S, Bollheimer LC, et al. Prevalence of sarcopenia in Germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community:results of the FORMoSA study. Clin Interv Aging. 2015;10:1565–1573. doi: 10.2147/CIA.S89585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wu CH, Chen KT, Hou MT, Chang YF, Chang CS, Liu PY, et al. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community:the Tianliao Old People study 04. Geriatr Gerontol Int. 2014;14:69–75. doi: 10.1111/ggi.12233. [DOI] [PubMed] [Google Scholar]
- 22.Yalcin A, Aras S, Atmis V, Cengiz OK, Varli M, Cinar E, et al. Sarcopenia prevalence and factors associated with sarcopenia in older people living in a nursing home in Ankara Turkey. Geriatr Gerontol Int. 2016;16:903–910. doi: 10.1111/ggi.12570. [DOI] [PubMed] [Google Scholar]
- 23.Halil M, Ulger Z, Varlı M, Döventaş A, Oztürk GB, Kuyumcu ME, et al. Sarcopenia assessment project in the nursing homes in Turkey. Eur J Clin Nutr. 2014;68:690–694. doi: 10.1038/ejcn.2014.15. [DOI] [PubMed] [Google Scholar]
- 24.Bahat G, Saka B, Tufan F, Akin S, Sivrikaya S, Yucel N, et al. Prevalence of sarcopenia and its association with functional and nutritional status among male residents in a nursing home in Turkey. Aging Male. 2010;13:211–214. doi: 10.3109/13685538.2010.489130. [DOI] [PubMed] [Google Scholar]
- 25.Bahat G, Tufan F, Bahat Z, Aydin Y, Tufan A, Akpinar TS, et al. Assessments of functional status, comorbidities, polypharmacy, nutritional status and sarcopenia in Turkish community-dwelling male elderly. Aging Male. 2013;16:67–72. doi: 10.3109/13685538.2013.771329. [DOI] [PubMed] [Google Scholar]
- 26.Yadigar S, Yavuzer H, Yavuzer S, Cengiz M, Yürüyen M, Döventaş A, et al. Primary Sarcopenia in Older People with Normal Nutrition. J Nutr Health Aging. 2016;20:234–238. doi: 10.1007/s12603-015-0562-4. [DOI] [PubMed] [Google Scholar]
- 27.Lee JS, Auyeung TW, Kwok T, Lau EM, Leung PC, Woo J. Associated factors and health impact of sarcopenia in older chinese men and women:a cross-sectional study. Gerontology. 2007;53:404–410. doi: 10.1159/000107355. [DOI] [PubMed] [Google Scholar]
- 28.Kim H, Suzuki T, Kim M, Kojima N, Yoshida Y, Hirano H, et al. Incidence and predictors of sarcopenia onset in community-dwelling elderly Japanese women:4-year follow-up study. J Am Med Dir Assoc. 2015;16:85.e1–e8. doi: 10.1016/j.jamda.2014.10.006. [DOI] [PubMed] [Google Scholar]
- 29.Iannuzzi-Sucich M, Prestwood KM, Kenny AM. Prevalence of sarcopenia and predictors of skeletal muscle mass in healthy, older men and women. J Gerontol A Biol Sci Med Sci. 2002;57:M772–M777. doi: 10.1093/gerona/57.12.m772. [DOI] [PubMed] [Google Scholar]
- 30.Arango-Lopera VE, Arroyo P, Gtierrez-Robledo LM, Perez-Zepeda MU. Prevalence of sarcopenia in Mexico City. Eur Geriatr Med. 2012;3:157–160. [Google Scholar]