

Abstract
Background
Although extensive use of tyrosine kinase inhibitors has resulted in high and durable response rate and prolonged survival time in patients with BCR-ABL1 positive chronic myeloid leukemia (CML) and acute leukemia, relapse and drug resistance still remain big challenges for clinicians. Monitoring the expression of BCR-ABL1 fusion gene and identifying ABL kinase mutations are effective means to predict disease relapse and resistance. However, the prognostic impact of BCR-ABL1 signal patterns detected by fluorescence in situ hybridization (FISH) remains largely unaddressed.
Methods
BCR-ABL1 signal patterns were analyzed using FISH in 243 CML-chronic phase (CML-CP), 17 CML-blast phase (CML-BP) and 52 BCR-ABL1 positive acute lymphoblastic leukemia (ALL) patients.
Results
The patterns of BCR-ABL1 signals presented complexity and diversity. A total of 12 BCR-ABL1 signals were observed in this cohort, including 1R1G2F, 1R1G1F, 2R1G1F, 1R2G1F, 2R2G1F, 1R2G2F, 1R1G3F, 1G3F, 2G3F, 1G4F, 1R1G4F and 1R4F. Complex BCR-ABL1 signal patterns (≥ two types of signal patterns) were observed in 52.9% (n = 9) of the CML-BP patients, followed by 30.8% (n = 16) of the ALL patients and only 2.1% (n = 5) of the CML-CP patients. More importantly, five clonal evolution patterns related to disease progression and relapse were observed, and patients with complex BCR-ABL1 signal patterns had a poorer overall survival (OS) time compared with those with single patterns (5.0 vs.15.0 months, p = 0.006).
Conclusions
Our data showed that complex BCR-ABL1 signal patterns were associated with leukemic clonal evolution and poorer prognosis in BCR-ABL1 positive leukemia. Monitoring BCR-ABL1 signal patterns might be an effective means to provide prognostic guidance and treatment choices for these patients.
Keywords: BCR-ABL1, Fluorescence in situ hybridization, Clonal evolution, Prognosis
Background
BCR-ABL1 fusion gene, produced by the specific t (9;22) (q34;q11) chromosomal translocation, occurs in approximately 90% of the chronic myeloid leukemia (CML), 25% of the acute lymphoblastic leukemia (ALL) and less than 5% of the acute myeloid leukemia (AML) cases [1–3], and it constitutively encodes tyrosine kinase BCR-ABL1 oncoprotein, which is responsible for proliferative signals and leukemogenesis by activating Raf/MEK/ERK, PI3K/AKT, and JAK/STAT pathways [4, 5]. Although extensive use of tyrosine kinase inhibitors (TKIs) has resulted in high and durable response rate as well as prolonged survival time in BCR-ABL1 positive CML or ALL patients, relapse and drug resistance still remain big challenges for clinicians. Some studies have suggested that mutations in the BCR-ABL1 tyrosine kinase domain induce disease relapse or resistance to TKIs [6–8]. Moreover, the presence of +der(22) (9;22), deletions of the derivative chromosome 9 and other complex chromosome karyotypes are usually not sensitive to TKIs, suggesting worse clinical outcomes in these patients [9].
Conventional cytogenetic analysis (karyotyping) is the most commonly used method to confirm the presence of the t(9;22) and other chromosomal abnormalities [10, 11]. However, such analysis can not detect subtle changes, such as microdeletion. Meanwhile, monitoring the expression of BCR-ABL1 fusion gene by quantitative PCR (q-PCR) and identifying ABL kinase mutations by sequencing are also effective means to predict disease relapse and resistance. Fluorescence in situ hybridization (FISH) with locus-specific dual-color, dual-fusion probe (DCDF-FISH) not only confirms the presence of the t(9;22), but also shows typical or atypical signal patterns [12–14]. The atypical patterns usually represent deletions on the derivative chromosome 9 (−der 9 t(9;22)), three- or more-way variant t(9;22), gain of an additional Philadelphia chromosome (+der 22 t(9;22)) or other abnormalities [13]. However, the prognostic impact of BCR-ABL1 signal patterns identified by DCDF-FISH in BCR-ABL1 positive leukemia patients remains largely unaddressed.
In the present study, we reported the characteristics and evolution of BCR-ABL1signal patterns using FISH in 243 CML-chronic phase (CML-CP), 17 CML-blast phase (CML-BP) and 52 ALL patients. Our data indicated that monitoring BCR-ABL1 signal patterns might be an effective way to provide prognostic guidance and treatment choices for patients with BCR-ABL1 positive leukemia.
Methods
Patients
This study was performed in accordance with the guidelines of the Helsinki Declaration (1996) and approved by the Ethics Committee of the Institute of Hematology, the First Affiliated Hospital of Nanchang University. A total of 243 newly diagnosed CML-CP, 17 CML-BP and 52 newly diagnosed BCR-ABL1 positive ALL patients were enrolled in this study from March 2011 to June 2016. Written informed consents were obtained from all participants. All of the patients received TKI monotherapy (CML-CP patients) or TKI in combination with chemotherapy (CML-BP and ALL patients). Blood count, serum chemistry and BCR-ABL1 FISH were performed in all of the patients at the time of diagnosis. Subsequently, FISH for BCR-ABL1 was performed monthly in CML-BP and ALL patients, while not routinely checked later in CML-CP patients. Therefore, the clinical significance of BCR-ABL1 signal patterns was only evaluated in CML-BP and ALL patients. Table 1 lists the clinical parameters of CML-BP and ALL patients.
Table 1.
FISH signal details in BCR-ABL1 positive leukemia patients
| CML-CP (n = 243) | CML-BP (n = 17) | BCR-ABL1+ ALL (n = 52) | |
|---|---|---|---|
| FISH signals | 1R1G1F;1R2G1F;2R1G1F; 2R2G1F;1R1G2F;1R1G3F | 1R1G1F;1R1G2F;1R1G3F;1G4F; 1R2G1F;1R2G2F;1R2G3F;2R2G1F; 2R1G2F; 2R2G2F | 1R1G1F;1R1G2F;1R1G3F; 1G4F;1R2G1F;1R2G2F;2R1G1F; 2R2G1F;1G3F;2G3F; 1R4F;1R1G4F |
| Complex signal patterns | 1R1G2F/2R1G1F(n = 1) | 1R1G1F/1R2G1F(n = 1) | 1R1G2F/1R1G4F/1R1G3F (n = 1) |
| 1R1G2F/2R2G1F(n = 2) | 1R2G1F/1R1G2F(n = 1) | 1R1G2F/1R1G3F/1R2G2F (n = 1) | |
| 1R1G2F/1R1G1F(n = 1) | 1G4F/1R1G2F (n = 1) | 1R1G2F/1R1G3F/1G3F/2R4F | |
| 1R1G1F/2R1G1F(n = 1) | 1R1G2F/1R2G2F/1R2G3F (n = 1) | (n = 1) | |
| 2R1G2F/2R2G2F (n = 1) | 1R1G3F/1R1G2F (n = 6) | ||
| 1R1G1F/1R2G2F (n = 1) | 1R1G3F/1R1G2F/1G3F n = 1) | ||
| 1R1G2F/1R1G3F (n = 3) | 1R2G2F/1RnG2F (n = 1) | ||
| 1R1G2F/1R1G4F (n = 1) | |||
|
2G3F/3F (n = 1) 1R1G2F/1G4F/2G8F (n = 1) | |||
| 1R1G2F/2R2G1F (n = 1) | |||
| 1R1G2F/1R2G1F (n = 1) | |||
| Typical single patterns | 1R1G2F (n = 179) | 1R1G2F (n = 5) | 1R1G2F (n = 28) |
| Atypical single patterns | 2R1G1F (n = 16) | 1R1G1F (n = 1) | 2R2G1F (n = 1) |
| 1R2G1F (n = 8) | 1R1G3F(n = 2) | 1R1G1F (n = 3) | |
| 1R1G1F (n = 20) | 1G3F (n = 1) | ||
| 2R2G1F (n = 14) | 1R1G3F (n = 2) | ||
| 1R1G3F (n = 1) | 2R1G1F (n = 1) |
Some BCR-ABL1 signal patterns and their interpretations (R = red signal; G = green signal; F = fusion signal) [21]
1R1G2F: t(9;22)
1R2G1F: t(9;22) with deletion of the derivative chromosome 9 involving only the sequences 5′ of the ABL1 breakpoint
2R1G1F: t(9;22) with deletion of the derivative chromosome 9 involving only the chromosome 22 sequences 3′ of the BCR breakpoint
1R1G1F: t(9;22) with deletion of the derivative chromosome 9 involving sequences 5′ of the ABL1 breakpoint as well the chromosome 22 sequences 3′ of the BCR breakpoint
1R1G3F: t(9;22) with additonal Philadelphia chromosome
2R2G1F: Variant (three-or four-way) t(9;22)
1RnG2F: nG represents many added green signals that we are different to count
Treatment response
Due to the small sample size of CML-BP patients, the treatment response was only evaluated in 52 newly diagnosed BCR-ABL1 positive ALL patients. Among these patients, only 3 patients received dasatinib in combination with chemotherapy, other 49 patients received imatinib based chemotherapies. Only two patients subsequently received allogeneic hematopoietic stem cell transplantation (allo-HSC). Complete remission (CR) and partial remission (PR) were determined based on morphological assessment of their bone marrow (BM) after a course of TKI in combination with chemotherapy. CR was defined by the presence of < 5% blasts in the BM, with > 1 × 109/L neutrophils and > 100 × 109/L platelets in the peripheral blood with no detectable extramedullary disease (EMD). PR was defined by the presence of 5–19% blasts in the BM. Relapse was defined by ≥5% blasts in the BM, circulating leukemic blasts, or the development of EMD.
BCR-ABL1 fusion gene detected by DCDF-FISH
DCDF-FISH for BCR-ABL1 (Vysis Inc., Downers Grove, IL, USA) was performed on BM cells prepared according to the routine FISH methods. At least 200 cells with well-delineated signals were evaluated. The cut-off level was set as 0.98% according to mean ± standard deviation in twenty normal controls.
Statistical analysis
Statistical analysis was conducted using SPSS software (version 22.0). Categorical variables were compared using nonparametric tests. Overall survival (OS) was calculated from date of initial diagnosis until death. Survival curves were plotted by the Kaplan–Meier method, and statistical differences between the curves were analyzed using the log-rank test. Multivariate analysis of variables associated with survival was conducted by Cox Proportional-Hazard model for OS. P ≤ 0.05 was considered as statistically significant.
Results
The patterns of BCR-ABL1 signal present complexity and diversity
To explore the characteristics of BCR-ABL1 signals among CML-CP, CML-BP and ALL patients, we assessed and analyzed BCR-ABL1 signals in 243 CML-CP, 17 CML-BP and 52 BCR-ABL1 positive ALL patients using DCDF-FISH. The classic BCR-ABL1 FISH pattern has two fusions, each fusion includes one ABL signal and one BCR signal. However, we found that the BCR-ABL1 signal patterns presented complexity and diversity in this cohort (Table 1). We observed a total of 12 types of BCR-ABL1 signals, including 1R1G2F, 1R1G1F, 2R1G1F, 1R2G1F, 2R2G1F, 1R2G2F, 1R1G3F, 1G3F, 2G3F, 1G4F, 1R1G4F and 1R4F (Fig. 1a and Table 1). Interestingly, some patients presented two or more BCR-ABL1 signals simultaneously (Fig. 1b).
Fig. 1.
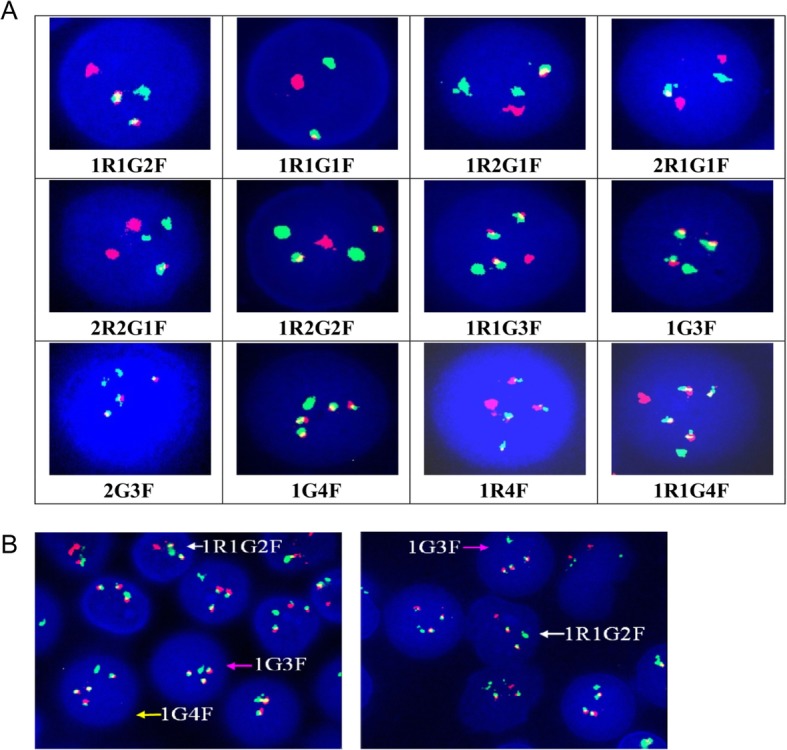
The patterns of BCR-ABL1 signals presented as complexity and diversity detected by specific dual-color, dual-fusion FISH probe (DCDF-FISH). (a) Twelve types of BCR-ABL1 signals were observed in CML-CP, CML-BP and ALL patients. (b) Complex BCR-ABL1 signal patterns (two or three BCR-ABL1 signals) could be observed in the same patient
Complex BCR-ABL1 signal patterns are more frequently detected in CML-BP and ALL patients
We further found that only six types of signals were observed in CML-CP patients, while 12 and 10 types of signals were detected in ALL and CML-BP patients, respectively (Table 1). Next, we indentified two or more BCR-ABL1 signal patterns as complex BCR-ABL1 signal patterns. Typical single BCR-ABL1 signal pattern means single 1R1G2F fusion signal. Atypical single BCR-ABL1 signal pattern indicates single BCR-ABL1 fusion signals other than 1R1G2F (such as 1R1G1F or 1R1G3F). Our results showed that complex BCR-ABL1 signal patterns were observed in 52.9% (n = 9) of the CML-BP patients, followed by 30.8% (n = 16) of the BCR-ABL1 positive ALL patients and only 2.1% (n = 5) of the CML-CP patients (p < 0.001) (Fig. 2a). Conversely, typical single BCR-ABL1 signal pattern was observed in 29.4% (n = 5) of the CML-BP patients, 53.8% (n = 28) of the BCR-ABL1 positive ALL patients and 73.7% (n = 179) of the CML-CP patients (p < 0.001) (Fig. 2b). The proportions of patients with atypical BCR-ABL1 signal patterns were similar, accounting for 17.6% (n = 3), 15.4% (n = 8) and 24.3% (n = 59) in the CML-BP, ALL and CML-CP patients, respectively (p = 0.369) (Fig. 2c). The expressed patterns of BCR-ABL1 signal were significantly different among the three groups (p < 0.001). These data suggested that ALL and CML-BP patients possessed more heterogeneous BCR-ABL1 cloned cells, indicating greater chromosomal abnormality and genomic instability. Due to the limited space of article, we listed the FISH signal details in BCR-ABL1 positive ALL patients in the Additional file 1: Table S1.
Fig. 2.

Complex BCR-ABL1 signal patterns were more frequently detected in CML-BP and ALL patients. (a) Complex BCR-ABL1 signal patterns were observed in 52.9% of the CML-BP patients, followed by 30.8% of the ALL patients and only 2.1% of the CML-CP patients (p < 0.001). (b) Typical single BCR-ABL1 signal pattern was observed in 29.4% of the CML-BP, 53.8% of the ALL patients and 73.7% of the CML-CP patients (p < 0.001). (C) The proportions of patients with atypical single BCR-ABL1 signal patterns were similar among three groups (17.6, 15.4 and 24.3%) (p = 0.369)
The comparison of clinical features between BCR-ABL1 positive CML-BP and ALL patients
We compared whether there was any difference in clinical features between BCR-ABL1 positive ALL and CML-BP patients. We analyzed the clinical data including age, sex, leukocyte count, hemoglobin count, thrombocyte count, cytogenetic abnormality, BCR-ABL1 FISH signal pattern and splenomegaly, in 17 CML-BP patients and 52 ALL patients. Except that moderate-severe splenomegaly was more often found in the CML-BP patients (p < 0.001) and lower thrombocyte count was more often detected in the BCR-ABL1 positive ALL patients (p < 0.001), there was no difference between the two groups (Table 2). We further compared the clinical features in BCR-ABL1 positive ALL patients with complex and single signal patterns, but the difference was not statistically significant (Table 3).
Table 2.
The clinical features of CML-BP and BCR-ABL1 positive ALL patients
| Characteristics | CML-BP | BCR-ABL1+ ALL | P value |
|---|---|---|---|
| Number of patients | 17 | 52 | |
| Median Age, y (Range) | 42.9 (15–70) | 39.0 (13–76) | 0.306 |
| Male/Female, % | 52.9/47.1 | 57.7/42.3 | 0.631 |
| Leukocyte count, 109/L (range) | 97.2 (1.0–303) | 57.4 (1.1–308) | 0.131 |
| Hemoglobin, g/L (range) | 82.5 (48–132) | 87.3 (38–149) | 0.630 |
| Thrombocyte count, 109/L (range) | 268.5 (13–2488) | 43.0 (3–230) | 0.000 |
| LDH, U/L (range) | 1059 (98–5490) | 836 (156–5353) | 0.526 |
| Cytogenetic abnormalities, % | 0.684 | ||
| t (9;22) | 4/17 (23.5%) | 11/52 (21.2%) | |
| ACAs | 5/17 (29.4%) | 11/52 (21.2%) | |
| No split phase | 8/17 (47.1%) | 30/52 (57.7%) | |
| BCR-ABL1 FISH | 0.068 | ||
| Complex signal pattern | 9/17 (52.9%) | 16/52 (30.8%) | |
| Typical single pattern | 5/17 (29.4%) | 28/52 (53.8%) | |
| Atypical single pattern | 3/17 (17.6%) | 8/52 (15.4%) | |
| Splenomegaly | 0.000 | ||
| Normal-mild | 8/17 (47.1%) | 51/52 (98.0%) | |
| Moderate- severe | 9/17 (52.9%) | 1/52 (2.0%) |
Abbreviations: CML-BP = chronic myeloid leukemia-blast phase, ALL = acute lymphoblastic leukemia, LDH = Lactate dehydrogenase, ACAs = additional cytogenetic abnormalities, Complex signal pattern = two or more types of BCR-ABL signal patterns, Single pattern = single 1R1G2F fusion signal or other single BCR-ABL fusion signals other than 1R1G2F. Mild splenomegaly: <3 cm under the ribs; Moderate splenomegaly: 3 ~ 6 cm under the ribs; Severe splenomegaly: >6 cm under the ribs
Table 3.
Comparison of patients’characteristics at diagnosis in BCR-ABL1 positive ALL with complex and single patterns
| Characteristics | Complex patterns | Single pattern | P value |
|---|---|---|---|
| Number of patients | 16 | 36 | |
| Median Age, y (Range) | 38.3 (16–61) | 39.0 (13–76) | 0.945 |
| Male/Female, % | 43.8/56.3 | 57.7/42.3 | 0.124 |
| Leukocyte count, 109/L (range) | 41.4 (1.2–106) | 57.4 (1.1–308) | 0.753 |
| Hemoglobin, g/L (range) | 84.9 (38–127) | 87.3 (38–149) | 0.784 |
| Thrombocyte count, 109/L (range) | 47.8 (7–230) | 43.0 (3–230) | 0.753 |
| LDH, U/L (range) | 978 (250–5353) | 766 (156–3723) | 0.364 |
| Cytogenetic abnormalities, % | 0.379 | ||
| t (9;22) | 2/16 (12.5%) | 9/36 (25.0%) | |
| ACAs | 5/16 (31.3%) | 6/36 (16.7%) | |
| No split phase | 9/16 (56.3%) | 21/36 (58.3%) |
BCR-ABL1 clonal evolution in ALL patients predicts disease progression and relapse
More importantly, we further found that the development of BCR-ABL1 signal patterns could indicate leukemic clonal evolution. Disease progression and relapse can be predicted by sequentially monitoring the BCR-ABL1 modes at different time points using FISH. In the present study, we observed that five clonal evolution modes were related to disease progression in BCR-ABL1 positive ALL patients. For example, clonal evolution modes in five patients were respectively listed below (Fig. 3). Patient one presented sensitive single clone (1R1G2F) at disease onset, which disappeared after treatment, and it was still observed as the primary clone (1R1G2F) during relapse (Fig. 3a). Patient two presented sensitive single clone (1R1G2F) at disease onset, which disappeared after treatment, whereas new single clone (1R1G4F) was observed during relapse (Fig. 3b). Patient three presented sensitive single clone (1R1G2F) at disease onset, whereas new and primary clones (1R1G2F and 1R1G3F) simultaneously occurred during relapse (Fig. 3c). The fourth patient presented many different subclones (1R1G2F, 1R1G3F and 1R1G4F) during disease onset, some sensitive subclones (1R1G4F and 1R1G3F) disappeared after treatment, whereas minor resistant subclones (1R1G2F) gradually progressed to preponderant subclones until relapse (Fig. 3d). The fifth patient simultaneously presented two different subclones (1R1G2F and 1R1G3F) at disease onset. Minor subclones (1R1G2F) were sensitive and decreased after treatment, whereas the preponderant subclones (1R1G3F) were resistant to TKIs or chemotherapy drugs (Fig. 3e). Regrettably, due to the retrospective analysis and the incomplete data, we did not provide the accurate incidence of different modes in all ALL patients.
Fig. 3.

BCR-ABL1 clonal evolution in ALL patients predicted disease progression and relapse. (a) 1R1G2F was sensitive single clone at disease onset, which disappeared after treatment, and it was still the primary clone (1R1G2F) during relapse. (b) 1R1G2F was sensitive single clone at disease onset, which disappeared after treatment, whereas new single clone (1R1G4F) was observed during relapse. (c) 1R1G2F was sensitive single clone at disease onset, whereas new and primary clones (1R1G2F and 1R1G3F) simultaneously occurred during relapse. (d) 1R1G2F, 1R1G3F and 1R1G4F presented different subclones during disease onset, some subclones (1R1G4F and 1R1G3F) were sensitive, whereas minor subclones (1R1G2F) were resistant. (d) 1R1G2F and 1R1G3F presented two different subclones at disease onset. Minor subclones (1R1G2F) were sensitive, whereas the preponderant subclones (1R1G3F) were resistant
Complex BCR-ABL1 signal patterns are associated with a poorer survival compared with single pattern in ALL patients
According to above-mentioned findings, complex BCR-ABL1 signal patterns were more frequently found in ALL and CML-BP patients, which could predict genomic instability. We further analyzed the prognostic factors for OS time in this cohort. The median follow-up time was 13.0 months (range, 1.0–54.0 months). Figure 4a and Table 4 reveal that patients with BCR-ABL1 complex signal patterns (5.0 vs. 15.0 months, p = 0.006), additional cytogenetic abnormalities (ACAs) (6.0 vs. 27.0 months, p = 0.001) or without achieving CR + PR (7.0 vs. 19.0 months, p = 0.019) had a poorer OS time compared with control patients. Meanwhile, in thirty patients with no split phase, patients with complex BCR-ABL1 pattern (n = 9) have poorer OS time than patients with single BCR-ABL1 pattern (n = 9) (9.6 vs 28.3 months, p = 0.026). However, due to the limited number of patients, multivariate analysis showed that only ACA was the independent prognostic factor for OS (HR: 0.16, 95% CI: 0.05–0.55, p = 0.004) (Table 5).
Fig. 4.

The analysis of survival in BCR-ABL1 positive ALL and CML-BP patients. (a) BCR-ABL1 positive ALL patients with complex signal patterns had poor OS time compared with patients with single signal patterns (P = 0.006). (b) BCR-ABL1 positive ALL and CML-BP patients had similar OS time (P = 0.984)
Table 4.
Univariate analysis of risk factors for OS in BCR-ABL1 positive ALL
| Group | Numbers | OS (range, month) | P value |
|---|---|---|---|
| Leukocyte count, 109/L | 0.736 | ||
| ≥ 50 | 21 | 13 (6.5~19.5) | |
| < 50 | 29 | 14 (6.7~21.3) | |
| LDH | 0.775 | ||
| ≥ 250 U/L | 37 | 13.0 (10.7~15.3) | |
| < 250 U/L | 10 | 8.0 (0.0~27.3) | |
| CR + PR | 0.019 | ||
| Yes | 44 | 19.0 (12.7~25.2) | |
| No | 5 | 7.0 (4.4~9.6) | |
| BCR-ABL1 FISH | 0.006 | ||
| Complex signal patterns | 36 | 5.0 (2.4~7.6) | |
| single patterns | 16 | 15.0 (8.3~21.7) | |
| Cytogenetic abnormalities | 0.001 | ||
| t (9;22) | 11 | 27 (14.5~39.5) | |
| ACAs | 11 | 6 (1.7~10.3) |
Abbreviations: LDH lactic dehydrogenase, CR complete remission, PR partial remission
Table 5.
Multivariate analysis of risk factors for OS in BCR-ABL1 positive ALL
| Prognostic parameters (yes) | HR for OS (95% CI) | P value |
|---|---|---|
| CR + PR | 0.45 (0.13–1.54) | 0.201 |
| Complex BCR-ABL1 signal patterns | 0.44 (0.14–1.35) | 0.152 |
| ACAs | 0.16 (0.05–0.55) | 0.004 |
Discussion
Traditional drug resistance in BCR-ABL1 positive patients caused by mutations in the tyrosine kinase domain of BCR-ABL1 or quiescent leukemic stem cells sheltered in unexposed region of BM has been widely accepted [6, 8]. Disease relapse and resistance restrain the clinical outcomes of CML and ALL patients, urging us to explore pathogenesis of leukemia. ACAs caused by genomic instability in leukemic cells are inevitable in progression of leukemia, and its prognostic significance in the setting of TKIs remains largely unexplored. Even under the TKI treatments (imatinib monotherapy or imatinib in combination with low-dose cytarabine or interferon), the frequency of these ACAs in CML increases the probability from chronic phase to blast phase and confers poor survival, which has been proved in a randomized CML study IV with 1151 cases [15]. Several gene mutations or other fusion genes, such as P53, RB, GATA-2 and AML1-EVI-1 fusion genes, cause the fatal blast crisis and lead to a shorter OS time in CML patients [11, 16–18]. Conversely, though some studies have reported that there is a significantly higher rate of complete cytogenetic response (CCyR) at 6 months (p = 0.02) for CML patients without ACAs, the cumulative CCyR and major molecular response (MMR) rates are not different between patients with and without ACAs. Similarly, MR4.0 and MR4.5 rates are similar in both groups, indicating that ACAs at diagnosis do not significantly impact transformation-free survival, failure-free survival, event-free survival or OS in CML-CP patients [19].
Recently, Nicholas J. Short et al. [9] have shown that +der(22)t(9;22) and/or − 9/9p in the absence of high hyperdiploidy are independent factors for worse relapse-free survival (RFS) (HR 2.03 [95% CI 1.08–3.30], p = 0.03) and OS (HR 2.02 [95% CI 1.10–3.71], p = 0.02) in Philadelphia+ ALL patients receiving chemotherapy in combination with a TKI treatment (imatinib or dasatinib). To date, monitoring the expression of BCR-ABL1 fusion gene by q-PCR and identifying ABL kinase mutations by sequencing have been employed as effective means to predict disease relapse and resistance in CML and ALL patients. However, these technologies can not detect ACAs in patients. At diagnosis, the presence of clonal ACAs may be observed in 5% of CML-CP patients, ~ 30% of AP patients and ~ 80% of patients with blast crisis [20]. Conventional karyotyping analysis can identify some obvious ACAs but not subtle changes. DCDF-FISH not only confirms the presence of t(9;22), but also identifies deletions on the derivative chromosome 9 (−der 9 t(9;22)), three- or more-way variant t(9;22), gain of an additional Philadelphia chromosome (+der 22 t(9;22)) or other abnormalities [13]. Jain et al. [21] have analyzed 1076 CML patients with positive BCR-ABL1 using a commercially available BCR-ABL1 dual-color, dual-fusion probe. Typical dual-fusion signals are seen in 74% of cases. Atypical signal patterns are seen in 26% of cases. 1F1R2G (4%), 1F2R1G (2.5%) and 1F1R1G (11%) represent derivative deletions in chromosome 9 sequence, chromosome 22 sequence, or both, respectively. 3F1R1G (6.5%) usually represents gain of an additional Philadelphia chromosome; and 1F2R2G (1%) represents a three- or four-way variant translocation. More than one signal pattern are seen in 1% of cases. In the present study, our results indicated that complex BCR-ABL1 signal patterns were more frequently found in CML-BP (52.9%) and BCR-ABL1 positive ALL (30.8%) patients, while they were rarely detected in CML-CP (2.1%) patients. There were only six types of signals observed in CML-CP patients, while 12 and 10 types of signals were found in ALL and CML-BP patients, respectively, suggesting that ALL and CML-BP patients possessed more heterogeneous BCR-ABL1 cloned cells and ACAs.
Tumor heterogeneity originates from multiple genetic and epigenetic diversities, leading to clonal evolution and drug resistance. CML-BP patients with simultaneous ACAs show lower response rates and a shorter failure time of imatinib mesylate (STI571) treatment [22]. BCR-ABL1 independent gene mutations (33% of patients had somatic mutations in addition to BCR-ABL1, including ASXL1, DNMT3A, RUNX1 and TET2, revealing that most mutations were part of the Ph-positive clones) are frequently found in Ph-negative and Ph-positive clones of CML patients and may be considered as important cofactors in the clonal evolution of CML [23]. Moreover, BCR-ABL1 compound mutations and other ABL1 tyrosine kinase inhibitors (TKIs) can also confer high-level resistance to imatinib [24]. Several research groups have also screened relapse-related gene mutations, including RAS and CREBBP/NT5C2 mutations in ALL patients [25, 26]. However, the correlation between clonal evolution and FISH signal patterns has not been well established in BCR-ABL1 positive patients. Therefore, we monitored the evolution of FISH signal patterns in BCR-ABL1 positive ALL patients. A total of five clonal evolution patterns related to disease progression were observed, and various sensitive or drug resistant subclones were found in patients receiving TKI treatment and chemotherapy. Therefore, we believed that monitoring the BCR-ABL1 signal patterns using FISH could also be a effective way to predict the disease progression and relapse for BCR-ABL1 positive ALL patients. Regrettably, we only evaluated 200 cells which might be missed some small clones. Moreover, due to the incomplete data and retrospective analysis, there is maybe not just five modes involved clone evolution. In the future, we will prospectively explain its incidence and clinical significance in the larger size of patients. Because we did not monthly check the BCR-ABL1 using FISH in CML-CP patients subsequently and due to the small sample size of CML-BP patients, we only evaluated the treatment response in BCR-ABL1 positive ALL patients and survival time in CML-BP and ALL patients. Our results indicated that patients with complex BCR-ABL1 signal patterns, ACAs and without achieving CR + PR had a poor OS time. In addition, among 30 ALL patients with no split phase, nine patients with complex BCR-ABL1 pattern had poorer OS time than patients with single BCR-ABL1 pattern (9.6 vs 28.3 months, p = 0.026). So, we think ACAs by karyotyping and FISH by DCDF probes could be well used complimentary to select more poor-risk patients. FISH analysis would be specially helpful for those patients with no split phase. Conversely, ACAs might identify poor-risk patients within the group of single-pattern patients. Due to the limited number of patients, we only observed ACAs was the independent prognostic factor for OS. Furthermore, our data also indicated CML-CP patients once progressed to blast phase, had similarly poor survival with BCR-ABL1 positive ALL patients (median OS is 10.0 vs.13.0 months, p = 0.984) even under the background of TKI treatment (Fig. 4b). Receiving hematopoietic stem cell transplantation or next generation of TKI as soon as possible might overcome the poor prognostic effect.
Conclusions
Taken together, our results suggested that signal patterns of BCR-ABL1 identified by FISH could predict disease progression and OS in BCR-ABL1 positive acute leukemia. Of course, our study had some limitations, such as the small sample size of CML-BP patients. Moreover, we did not analyze the correlation among the results of BCR-ABL1 FISH, q-PCR and sequencing which might be related to relapse or resistance to TKI-based therapy [26]. These questions need to be further answered in larger number of patients.
Supplementary information
Additional file 1: Table S1. FISH signal details in BCR-ABL1 positive ALL patients.
Acknowledgements
Not applicable.
Abbreviations
- ACAs
Additional cytogenetic abnormalities
- ALL
Acute lymphoblastic leukemia
- AML
Acute myeloid leukemia
- CCyR
Complete cytogenetic response
- CML-BP
Chronic myeloid leukemia-blast phase
- CR
Complete remission
- DCDF
Dual color, dual fusion probe
- FISH
Fluorescence in situ hybridization
- LDH
Lactate dehydrogenase
- MMR
Major molecular response
- OS
Overall survival
- PR
Partial remission
- TKIs
Tyrosine kinase inhibitors
Authors’ contributions
ZZ and CZ designed and performed the research, and also interpreted the data and drafted the manuscript; JM, LS, GY and WL discussed the advice from reviewers and substantively revised it together; LF conducted the experimental design, analyzed and interpreted the data, and approved the final manuscript. All of the authors have read and approved the manuscript, and ensure that this is the case.
Funding
These work including the study design and execution, the collection, analysis, and interpretation of data and writing the manuscript were financially supported by grants from the National Natural Science Foundation of China (81760539, 81560036, 81560034), Science and Technology Cooperation Program of Jiangxi Province (20151BDH80043).
Availability of data and materials
The datasets supporting the conclusions of this manuscript are included within the article. Please contact author for raw data requests.
Ethics approval and consent to participate
The study was approved by Institutional Review Board from the first affiliated hospital of nanchang university and conducted in accordance with provision of the Declaration of Helsinki. Informed consent to participate in the study had been obtained from participants or their parents if the children were under 16.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Zhanglin Zhang and Zhiwei Chen contributed equally to this work.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s12885-019-6137-8.
References
- 1.Castagnetti F, Gugliotta G, Breccia M, Iurlo A, Levato L, Albano F, et al. The BCR-ABL1 transcript type influences response and outcome in Philadelphia chromosome-positive chronic myeloid leukemia patients treated frontline with imatinib. Am J Hematol. 2017;92:797–805. doi: 10.1002/ajh.24774. [DOI] [PubMed] [Google Scholar]
- 2.Radich JP, Kopecky KJ, Boldt DH, Head D, Slovak ML, Babu R. Detection of BCR-ABL fusion genes in adult acute lymphoblastic leukemia by the polymerase chain reaction. Leukemia. 1994;8:1688–1695. [PubMed] [Google Scholar]
- 3.Konoplev S, Yin CC, Kornblau SM, Kantarjian HM, Konopleva M, Andreeff M, et al. Molecular characterization of de novo Philadelphia chromosome-positive acute myeloid leukemia. Leuk Lymphoma. 2013;54:138–44. 2. doi: 10.3109/10428194.2012.701739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Steelman LS, Pohnert SC, Shelton JG, Franklin RA, Bertrand FE. McCubreyJA.JAK/STAT, Raf/MEK/ERK, PI3K/Akt and BCR-ABL in cell cycle progression and leukemogenesis. Leukemia. 2004;18:189–218. doi: 10.1038/sj.leu.2403241. [DOI] [PubMed] [Google Scholar]
- 5.Xie S, Lin H, Sun T, Arlinghaus RB. Jak2 is involved in c-Myc induction by Bcr-Abl. Oncogene. 2002;21:7137–7146. doi: 10.1038/sj.onc.1205942. [DOI] [PubMed] [Google Scholar]
- 6.Soverini S, Gnani A, Colarossi S, Castagnetti F, Abruzzese E, Paolini S, et al. Philadelphia-positive patients who already harbor imatinib-resistant Bcr-Abl kinase domain mutations have a higher likelihood of developing additional mutations associated with resistance to second- or third-line tyrosine kinase inhibitors. Blood. 2009;114:2168–2171. doi: 10.1182/blood-2009-01-197186. [DOI] [PubMed] [Google Scholar]
- 7.Branford S, Rudzki Z, Walsh S, Parkinson I, Grigg A, Szer J, et al. Detection of BCR-ABL mutations in patients with CML treated with imatinib is virtually always accompanied by clinical resistance, and mutations in the ATP phosphate-binding loop (P-loop) are associated with a poor prognosis. Blood. 2003;102:276–283. doi: 10.1182/blood-2002-09-2896. [DOI] [PubMed] [Google Scholar]
- 8.Graham SM, Jorgensen HG, Allan E, Pearson C, Alcorn MJ, Richmond L, et al. Primitive, quiescent, Philadelphia-positive stem cells from patients with chronic myeloid leukemia are insensitive to STI571 in vitro. Blood. 2002;99:319–325. doi: 10.1182/blood.V99.1.319. [DOI] [PubMed] [Google Scholar]
- 9.Short NJ, Kantarjian HM, Sasaki K, Ravandi F, Ko H, Cameron Yin C, et al. Poor outcomes associated with +der(22)t(9;22) and −9/9p in patients with Philadelphia chromosome-positive acute lymphoblastic leukemia receiving chemotherapy plus a tyrosine kinase inhibitor. Am J Hematol. 2017;92:238–243. doi: 10.1002/ajh.24625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.King RL, Naghashpour M, Watt CD, Morrissette JJ, Bagg A. A comparative analysis of molecular genetic and conventional cytogenetic detection of diagnostically important translocations in more than 400 cases of acute leukemia, highlighting the frequency of false-negative conventional cytogenetics. Am J Clin Pathol. 2011;135:921–928. doi: 10.1309/AJCPJCW6BY0CNIHD. [DOI] [PubMed] [Google Scholar]
- 11.Kim TD, Turkmen S, Schwarz M, Koca G, Nogai H, Bommer C, et al. Impact of additional chromosomal aberrations and BCR-ABL kinase domain mutations on the response to nilotinib in Philadelphia chromosome-positive chronic myeloid leukemia. Haematologica. 2010;95:582–588. doi: 10.3324/haematol.2009.014712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bakshi SR, Brahmbhatt MM, Trivedi PJ, Shukla SN, Shah PM. Atypical D-FISH patterns of BCR/ABL gene rearrangements in 169 chronic myeloid leukemia patients. J Assoc Genet Technol. 2006;32:164–167. [PubMed] [Google Scholar]
- 13.Primo D, Tabernero MD, Rasillo A, Sayagues JM, Espinosa AB, Chillon MC, et al. Patterns of BCR/ABL gene rearrangements by interphase fluorescence in situ hybridization (FISH) in BCR/ABL+ leukemias: incidence and underlying genetic abnormalities. Leukemia. 2003;17:1124–1129. doi: 10.1038/sj.leu.2402963. [DOI] [PubMed] [Google Scholar]
- 14.Lee DS, Kim EC, Yoon BH, Kim WH, Yoon JH, Cho HI. Can minor bcr/abl translocation in acute leukemia be discriminated from major bcr/abl by extra-signal FISH analysis? Haematologica. 2001;86:991–992. [PubMed] [Google Scholar]
- 15.Fabarius A., Leitner A., Hochhaus A., Muller M. C., Hanfstein B., Haferlach C., Gohring G., Schlegelberger B., Jotterand M., Reiter A., Jung-Munkwitz S., Proetel U., Schwaab J., Hofmann W.-K., Schubert J., Einsele H., Ho A. D., Falge C., Kanz L., Neubauer A., Kneba M., Stegelmann F., Pfreundschuh M., Waller C. F., Spiekermann K., Baerlocher G. M., Lauseker M., Pfirrmann M., Hasford J., Saussele S., Hehlmann R. Impact of additional cytogenetic aberrations at diagnosis on prognosis of CML: long-term observation of 1151 patients from the randomized CML Study IV. Blood. 2011;118(26):6760–6768. doi: 10.1182/blood-2011-08-373902. [DOI] [PubMed] [Google Scholar]
- 16.Beck Z, Kiss A, Toth FD, Szabo J, Bacsi A, Balogh E, et al. Alterations of P53 and RB genes and the evolution of the accelerated phase of chronic myeloid leukemia. Leuk Lymphoma. 2000;38:587–597. doi: 10.3109/10428190009059278. [DOI] [PubMed] [Google Scholar]
- 17.Zhang SJ, Ma LY, Huang QH, Li G, Gu BW, Gao XD, et al. Gain-of-function mutation of GATA-2 in acute myeloid transformation of chronic myeloid leukemia. Proc Natl Acad Sci U S A. 2008;105:2076–2081. doi: 10.1073/pnas.0711824105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mitani K, Ogawa S, Tanaka T, Miyoshi H, Kurokawa M, Mano H, et al. Generation of the AML1-EVI-1 fusion gene in the t(3;21)(q26;q22) causes blastic crisis in chronic myelocytic leukemia. EMBO J. 1994;13:504–510. doi: 10.1002/j.1460-2075.1994.tb06288.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Alhuraiji A, Kantarjian H, Boddu P, Ravandi F, Borthakur G, DiNardo C, et al. Prognostic significance of additional chromosomal abnormalities at the time of diagnosis in patients with chronic myeloid leukemia treated with frontline tyrosine kinase inhibitors. Am J Hematol. 2018;93:84–90. doi: 10.1002/ajh.24943. [DOI] [PubMed] [Google Scholar]
- 20.Luatti S, Castagnetti F, Marzocchi G, Baldazzi C, Gugliotta G, Iacobucci I, et al. Additional chromosomal abnormalities in Philadelphia-positive clone: adverse prognostic influence on frontline imatinib therapy: a GIMEMA working party on CML analysis. Blood. 2012;120:761–767. doi: 10.1182/blood-2011-10-384651. [DOI] [PubMed] [Google Scholar]
- 21.Jain PP, Parihar M, Ahmed R, Abraham A, Vishwabandya A, George B, et al. Fluorescence in situ hybridization patterns of BCR/ABL1 fusion in chronic myelogenous leukemia at diagnosis. Indian J Pathol Microbiol. 2012;55:347–351. doi: 10.4103/0377-4929.101742. [DOI] [PubMed] [Google Scholar]
- 22.O'Dwyer M. E. The impact of clonal evolution on response to imatinib mesylate (STI571) in accelerated phase CML. Blood. 2002;100(5):1628–1633. doi: 10.1182/blood-2002-03-0777. [DOI] [PubMed] [Google Scholar]
- 23.Schmidt M, Rinke J, Schafer V, Schnittger S, Kohlmann A, Obstfelder E, et al. Molecular-defined clonal evolution in patients with chronic myeloid leukemia independent of the BCR-ABL status. Leukemia. 2014;28:2292–2299. doi: 10.1038/leu.2014.272. [DOI] [PubMed] [Google Scholar]
- 24.Khorashad JS, Kelley TW, Szankasi P, Mason CC, Soverini S, Adrian LT, et al. BCR-ABL1 compound mutations in tyrosine kinase inhibitor-resistant CML: frequency and clonal relationships. Blood. 2013;121:489–498. doi: 10.1182/blood-2012-05-431379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oshima K, Khiabanian H, da Silva-Almeida AC, Tzoneva G, Abate F, Ambesi-Impiombato A, et al. Mutational landscape, clonal evolution patterns, and role of RAS mutations in relapsed acute lymphoblastic leukemia. Proc Natl Acad Sci U S A. 2016;113:11306–11311. doi: 10.1073/pnas.1608420113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ding LW, Sun QY, Mayakonda A, Tan KT, Chien W, Lin DC, et al. Mutational profiling of acute lymphoblastic leukemia with testicular relapse. J Hematol Oncol. 2017;10:65. doi: 10.1186/s13045-017-0434-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. FISH signal details in BCR-ABL1 positive ALL patients.
Data Availability Statement
The datasets supporting the conclusions of this manuscript are included within the article. Please contact author for raw data requests.