

Abstract
Spleen is typically injured in blunt abdominal trauma. Spleen injuries make 42% of all blunt abdominal injuries. The aim of this study was to perform a retrospective assessment of the cases of acute and subacute isolated traumatic spleen ruptures.
A retrospective study performed on 50 patients, whose cause of death was isolated spleen rupture and bleeding into the abdominal cavity.
An acute spleen rupture was diagnosed in 47 cases, whereas the rest 3 cases demonstrated a subacute rupture. In cases of acute spleen rupture, the mean weight of spleen was 309.6 g, whereas in 3 cases of subacute rupture the mean weight of the organ achieved 710 g. The mean weight of spleen in the control group with no spleen rupture was 144.7 g.
Recording of the cases of isolated acute and subacute traumatic spleen ruptures and morphological assessment of them are important in forensic pathology science and in clinical practice as well.
Keywords: blunt trauma, forensic science, injury, intoxication, pathology, spleen rupture
1. Introduction
Spleen is the most frequently injured intra-abdominal organ. It is determined by its anatomic features. Spleen lies in the left hypochondrium between the 9th and 11th ribs. Usually, it is 10 to 12 cm in length, 7 to 8 cm in width, 3 to 4 cm in depth, and weighs approximately 150 to 200 g.[1,2] It can considerably expand and tighten rather quickly, and normally it does not come out from beneath the costal arch. A normal-sized spleen is usually entirely covered by the rib cage; thus, it can be palpated only while inhaled or in case of its at least three-time enlargement. When intra-abdominal pressure increases, its soft consistence, sinusoid structure, and fragile fibroelastic capsule determine its exposure to injuries. Spleen consists of an irregularly spaced connective tissue and is slightly thicker in the region of hilum. Trabeculae, septums of connective tissue, emanate from the capsule into the splenic parenchyma. Splenic artery is the largest truncus coeliacus branch. This anatomic feature demonstrates the intensity of spleen circulation. Intraorganic segmental circulation makes possible the partial resection of spleen. Generally, there are 2 or 3 segments of spleen.[2]
Spleen is typically injured in blunt abdominal trauma.[3] Spleen injuries make 42% of all blunt abdominal injuries.[4]
Spleen can rupture in 2 ways depending on its capsule injury. In the process of trauma, transcapsular spleen rupture may happen. In such case, spleen capsule and parenchyma rupture simultaneously and blood effuses into peritoneal cavity. It usually leads to acute blood loss and immediate death. Another possible way of spleen rupture is subcapsular rupture. It involves an initial formation of subcapsular hematoma, which enlarges several hours or days increasing the subcapsular pressure and finally induces capsular rupture.[5] Due to its mechanism, subcapsular rupture is also called a two-stage rupture.
Macroscopic/gross view is important in evaluating the consequences of a blunt abdominal trauma.[6] If the rupture was two-stage, then postmortem dissection shows spleen surrounded with adhesions. It is common to observe the rupture on internal, or visceral, surface of the organ. Transcapsular injury can reach the hilum or diaphragmatic surface of the organ. Slight spleen tears are often multiple, Y-, H-, and L-letter shaped.[3,5] Microscopic examination is performed to differentiate/distinguish an intact before trauma spleen rupture from pathologically changed and fragile organ.[4,7] Microscopic view is also important in exploring whether the rupture was indeed antemortem and in evaluating time after injury as well.[5,6] Spleen fragility is usually determined by the quantitative dominance of the white pulp. Normally, microscopic specimen of the rupture shows hemorrhage and neutrophil infiltration in the area of rupture. In case of pathology amyloidosis, lymphoid tissue proliferation, tumor cells can be found.[7] Perisplenic adhesions, capsule cicatrisation, demonstrate past trauma or rupture.[8]
2. Methods
2.1. Study design and data source
A retrospective study was performed on 50 patients, whose cause of death was an isolated spleen rupture and bleeding into the abdominal cavity. The research was designed as a retrospective cohort study and was approved by the Ethics Committee of Vilnius regional biomedical research. An informed consent was signed by the research subjects’ representatives. The data, regarding postmortem investigation of the victims between 2013 and 2016 years, were obtained from Lithuanian State Forensic Medicine Service database. The data concerning the patients with an isolated spleen rupture as the cause of death were collected from the central health e-database of Lithuania (www.esveikata.lt). This Lithuanian health dataset included demographic data of the patients, diagnoses, and information regarding the cause of death. All decedents received full autopsies. In every case, there was information provided from the law enforcement agencies, including scene of the incident, time of death, and the presumable death mechanism.
2.2. Identification of cases
The study involved 50 cases with isolated spleen ruptures in total, of them 42 died suddenly without receiving any medical treatment and 8 patients were hospitalized before death. All the cases were defined according to the International Classification of Diseases. Cases of isolated spleen rupture and bleeding into the abdominal cavity, cases with/without fractured ribs, and cases of blunt abdominal trauma with/without bruising of the soft tissues were chosen as enrollment criteria. Cases of blunt abdominal trauma with multiple ruptures of several visceral organs were excluded from the analysis. The circumstances of all the cases were determined as accidental or as homicide.
2.3. Statistical analysis
The data collected were processed using R software. The Shapiro–Wilk test was used to determine whether the data were normally distributed. Chi-square test and Fisher exact test were performed to intercompare the groups of acute and subacute spleen rupture. Spearman's correlation coefficients were assessed. A weak correlation was defined as r < 0.39; a moderate correlation with r values from 0.40 to 0.69; and a strong correlation with r > 0.70. In addition, 95% confidence intervals were calculated. Differences with P < 0.05 were considered significant.
2.4. Histological methods
Histological sections were cut and prepared for the routine light microscopy. Histomorphological features of the clot were examined using hematoxylin and eosin (H&E) staining. Perls’ Prussian blue reaction was used to detect ferric iron and Masson's Trichrome staining for collagen fibers.
The H&E staining consists of several stages: removing of paraffin, staining, and dehydration. Sections are deparaffinated by keeping them sequentially in absolute alcohol, 96% and 70% ethanol and distilled water for a certain time. After that specimens are stained with hematoxylin solution and then continuously irrigated with flowing water. Afterward, eosin–floxin solution is applied. Finally, specimens are quickly sequentially dehydrated in 70%, 90%, and absolute alcohol and enclosed with covering material. Nucleus and other DNA/RNA containing structures are dyed in blue–violet color, whereas cytoplasm and matrix in different pink tints.
3. Results
3.1. Cases of an acute isolated spleen rupture
The number of autopsies performed from 2013 to 2016 was 25,072. During this period, there were 50 cases of isolated traumatic spleen ruptures and in 3 of them subacute spleen ruptures was diagnosed.
The mean age of the research subjects (n = 50) was 44 years. The youngest victim was 29-year-old and the eldest was 75-year-old; 74% were men and 26% were women. The mean age of men was 42.19 ± 9.84 years; the mean age of women was 50.62 ± 9.75 years. Statistically significant difference was found between the mean age of male and female (P = .01).
The mean height of the decedents was 174 cm, the shortest was 158 cm, and the tallest was 190 cm. The mean weight of spleen was 309.6 g, the lightest weight was 64 g, and the heaviest weight was 1460 g. The mean weight of spleen was 336.19 ± 328.25 g in male group and 236 ± 165.62 g in female group (Fig. 1). No statistically significant difference was found between the mean weight of spleen in male and female groups (P = .17). The mean length of spleen was 14 ± 3.9 cm; a statistically significant correlation was observed between length and weight of the spleen (r = 0.77, P < .05) (Fig. 2).
Figure 1.
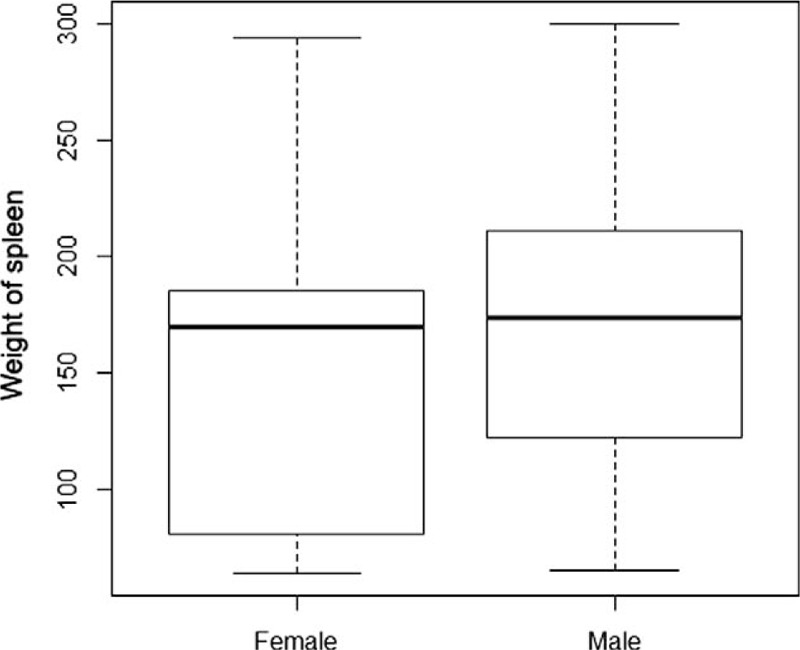
The mean weight of spleen.
Figure 2.
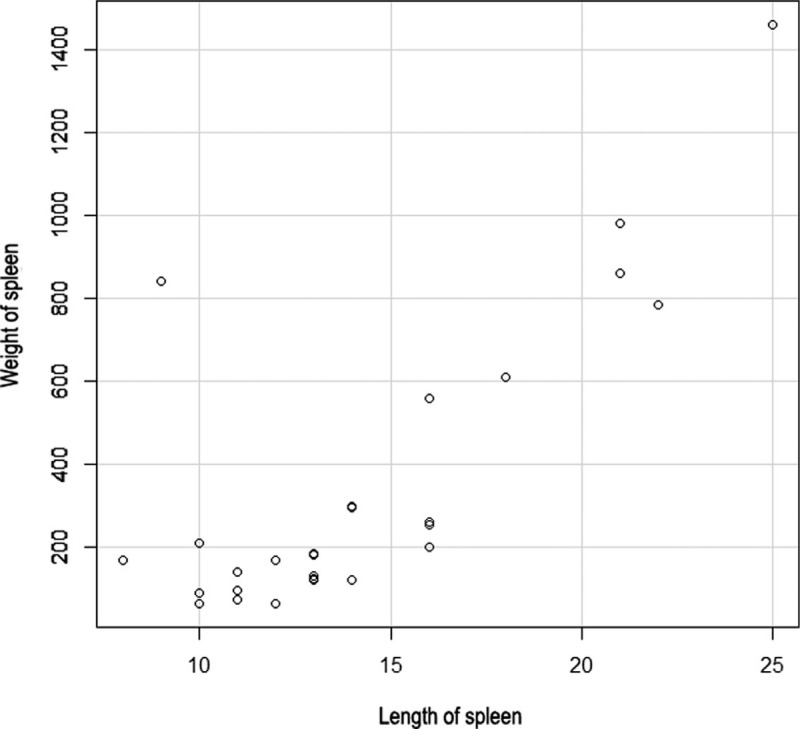
Correlation between length and weight of spleen.
The mean volume of blood in abdominal cavity was 1872 mL, the lowest volume found was 1000 mL, and the biggest was 4500 mL. The mean volume of blood in abdominal cavity was 1876.94 ± 1137.05 mL in male and 1858.85 ± 1003.56 mL in female groups. No statistically significant difference was found between the mean volume of blood found in abdominal cavity in male and female groups (P = 0.96).
In 84% of the cases, victims died immediately with no medical assistance provided, whereas the rest were hospitalized and died at the hospital.
The mean age of victims, who died immediately, was 43.37 ± 9.85 years, and the mean age of those hospitalized was 49.87 ± 12.24 years. No statistically significant difference was found between the mean age of the victims in these 2 groups (P = .19).
In the group of victims, who did not receive medical aid, the mean age of men was 44.25 ± 8.22 years and the mean age of women was 55.50 ± 14.05 years. No statistically significant difference was found between the mean age of men and women in the group (P = .23). The mean weight of spleen in men of the same group was 206.50 ± 39.48 g and in women was 319.75 ± 182.92 g. No statistically significant difference was found between the mean weight of spleen in men and women in the group (P = .31). The mean volume of blood in abdominal cavity of men was 2000 ± 1080 mL, and of women was 1250 ± 288 mL. No statistically significant difference was found between the mean volume of blood in abdominal cavity of men and women in the group of victims, who died immediately (P = 0.26).
In the group of subjects, who were hospitalized before death, the mean age of men was 41.94 ± 10.11 and the mean age of women was 48.44 ± 7.16 years. No statistically significant difference was found between the mean age of men and women in the group (P = .04). The mean weight of spleen in men of the same group was 352.40 ± 345.05 g and in women was 198.78 ± 153.41 g. No statistically significant difference was found between the mean weight of spleen in men and women in the group (P = .06). The mean volume of blood found in abdominal cavity of men was 1861 ± 1159 mL and of women was 2129 ± 1100 mL. No statistically significant difference was found between the mean volume of blood in abdominal cavity of men and women in the group of victims, who died in hospital (P = .53).
The mean weight of spleen in the control group with no spleen rupture (n = 250) was 144.7 g, median weight was 120 g, minimal weight was 80.5 g, and maximum weight was 505 g (Fig. 3). The mean age of the group was 58.55 years. The mean weight of spleen was 146.75 ± 78.25 g in male group and 139.38 ± 84.72 g in female group. No statistically significant difference was found between the mean weight of spleen in 2 gender groups (P = .52).
Figure 3.
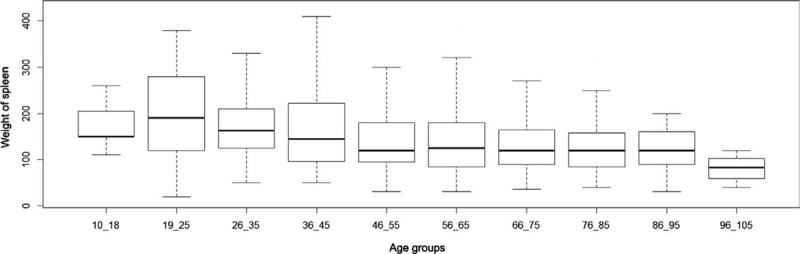
The mean weight of spleen in control group.
3.2. Cases of subacute spleen rupture
A 31-year-old man was found dead at home. The external examination of the body revealed no external mechanical injury. However, 1830 mL of liquid blood and dark red blood clots in the abdominal cavity was found during internal inspection. The spleen was of 18 × 15 × 7 cm size and weighed 840 g. There was a 12-cm-length rupture of the capsule and parenchyma, located on the diaphragmatic surface of the organ. Furthermore, adhesions were detected between superior anterior border of the spleen and the diaphragm. The spleen capsule was thicker than normal in the area of adherence. Blood ethanol concentration was 0.92%.
A 50-year-old woman was found dead at home. External examination of the corpse revealed a subcutaneous bruise on the right part of the loin. During internal inspection, 2475 mL of liquid blood and dark red blood clots was found in the peritoneal cavity. The spleen was of 16 × 10 × 5 cm size and weighed 560 g. A 6-cm-length rupture of the capsule and parenchyma was found in the region of the hilum. The sides of the rupture were covered with clotted blood, granular tissue, and fibrin. Internal spleen surface was adhered to omentum, and the capsule was strained in the region of the hilum. Blood ethanol concentration was 1.69%.
A 49-year-old man was found dead at home. No external mechanical injury was found during the external examination. Internal inspection revealed 1550 mL of liquid blood and solitary blood clots in the abdominal cavity. The spleen capsule was wrinkled, size 15 × 6 × 2 cm, weight 365 g. There was a 5-cm-length rupture at the hilum of the spleen. The sides of the rupture had irregular borders, covered with solid dark purple blood clots. The surrounding tissue was multicolored, whitish purple, and granular fibrinous tissue areas were observed. Blood ethanol concentration was 2.53%.
Findings of macroscopic and microscopic observation of the ruptured area include the following: granular tissue with plenty of hemosiderin and an abundant infiltration of hemosiderophages in the projection of the rupture and granular tissue hyalinization patchily (Figs. 4 and 5). Pathology diagnosis includes a two-stage spleen rupture. An initial rupture was diagnosed microscopically 3 to 5 days before death and the second one shortly before death. The mean weight of spleen in the group of subacute spleen rupture was 710 g.
Figure 4.
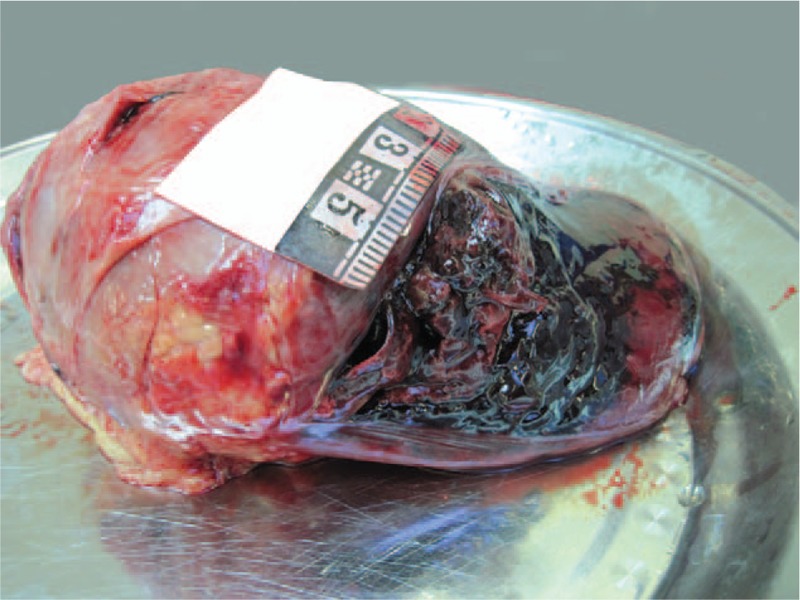
Blunt abdominal trauma, 600 g spleen with subacute bleeding.
Figure 5.
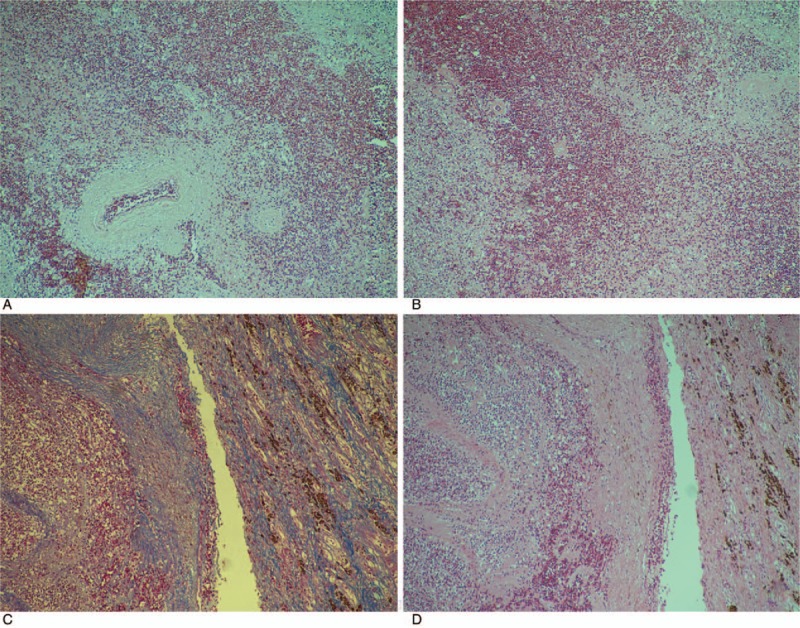
The microscopic view of spleen with subacute bleeding.
4. Discussion
The research had certain limitations as described below. First, all the subjects derived from Lithuanian population and the obtained parameters do not represent the situation of the global population. Second, the study involved a limited number of female patients. Third, the selected subjects were mostly middle-aged and older. The study did not involve individuals of the pediatric age.
According to the results of the study, the mean age of men, who died due to acute spleen rupture, was 42.19 ± 9.84 years; the mean age of women was 50.62 ± 9.75 years. A statistically significant difference between the gender groups (P = .01) was found. The mean weight of spleen was 336.19 ± 328.25 g in male group and 236 ± 165.62 g in female group. However, there was no statistically significant difference between the mean weight of spleen in these 2 groups (P = .17). There was also no statistically significant difference found between the mean volume of blood found in abdominal cavity in male and female groups (P = .96).
In the study of the standard dimensions of the normal spleen in Iranian population from the Razavi Khorasan Province, the weight of the spleen varied from 1 to 720 with mean value of 123.87 g.[26] The mean weight of spleen was 128.51 ± 86.09 g in male group and 107.23 ± 65.45 g in female group, which was consistent to the present study findings. The spleen dimensions were significantly higher in men than in women.
The mean length of spleen in Bangladeshi people was 9.66 cm (range: 5–13 cm).[27] The average width and thickness of spleen were 3.06 cm (range: 1.5–5.5 cm) and 6.22 cm (range: 3.5–9.5 cm), respectively.
In another research, in Kumaon Region of Uttarakhand, contrary to findings in the present study, the spleen weight in females was bigger than in males (153.9 g vs 149.17 g, respectively).[28]
In the study performed by Caglar et al., the range of spleen weight in males was 48 to 720 g, with a mean weight 209 ± 111.7 g. Furthermore, in the mentioned study spleen weight significantly correlated with the height of individuals.[29]
Despite the fact that the spleen is not a vital organ, it performs several important functions. First of all, its immune role as it is the biggest secondary lymphoid organ, which contains 25% of the whole lymphatic tissue of the body.[18] Consequently, a severe sepsis is more likely to occur after splenectomy. Another significant function is the removal of the aged red blood cells and platelets (splenectomy is one of the possible ways of managing platelet deficiency). These cells can also be stored in the spleen. The 1/3 part of the body storage of thrombocytes is found in the spleen. Therefore, in cases of hemorrhagic shock the spleen can shrink and emit a certain amount of blood, which compensates anemia, though partially.[2]
Spleen can be injured under the compressive or tractive forces. Compressive injury manifests as the disruption of the organ. However, due to the spleen intraperitoneal position it can also be separated from its vascular pedicle by traction.[3,19] Moreover, in the process of trauma the sharp bend of a fractured rib can cut open the spleen capsule and cause the rupture of parenchyma. Nevertheless, spleen more often ruptures because of an increased intra-abdominal pressure in the process of a blunt trauma, when a hit is to the region of the spleen. Road traffic accidents, fall from height, violence (hit to the region of the spleen), and sports-related injuries commonly cause spleen trauma, gunshot injuries—less frequently.[4,7]
The rupture is likely to happen immediately or several days/weeks after the trauma. Tissue plasticity plays a significant role in the process of a blunt abdominal trauma: a kick to the thorax can leave minimal subcutaneous bruises, whereas the abdominal organs (liver and spleen) may be seriously damaged due to the dense structure.[6] A pathological rupture is also possible, for instance, in splenomegalic patients. The common reasons of spleen enlargement: malaria, EBV infection, liver diseases, blood cancer (lymphoma, leukemia), angiosarcoma, and amyloidosis.[7,8,20] In general, pathological rupture is rare; it happens in 0.1% to 0.5% of cases.[8] There are 3 possible mechanisms of this rupture: spleen capsule straining from within in splenomegalic patients, outside pressing of the capsule while coughing, vomiting, defecating (due to increased intraabdominal pressure), occlusion of the feeding vessel with consequent spleen necrosis and blood issues.[8,13]
Fractured ribs and increased intraabdominal pressure during resuscitation can cause spleen rupture. It happens in about 0.3% of all resuscitated patients.[6,21] Usually, these patients suddenly die due to the loss of significant amount of blood.[3]
A delayed rupture can be present in about 14% of all spleen ruptures.[22] A rupture is considered as delayed, if it happens >7 days after the trauma. According to other authors, spleen must be damaged ≥ 2 days before the capsule rupture.[23] In 75% of the cases, a delayed rupture happens within 2 weeks and in 90% of the cases within 4 weeks after the trauma.[24] If there is a high-energy trauma (e.g., motorcycle accident), the rupture is more likely to involve both spleen capsule and parenchyma, and induce an acute intra-abdominal bleeding. In case of a less-energy trauma (e.g., violence), a subcapsular hematoma appears and starts enlarging. Finally, when the capsule fails to resist the pressure under it and ruptures it induces a subacute bleeding.[3,25] In process of getting abdominal injury, a considerable part of patients, about 23%, are inebriated. Consequently, the diagnostic process becomes more complicated. Children are likely to traumatize in a more specific way—falling on the bicycle handlebar while riding. At the moment of falling, an increased intraabdominal pressure can cause spleen rupture.[25]
Acute spleen rupture prevalently happens during blunt abdominal trauma because of suddenly increased intraabdominal pressure. It suggests that external body injuries may not always be seen. However, traumatized patients usually complain about pain in the left upper part of abdomen, as well as in the region of left shoulder (Kehr's symptom). Therefore, these clinical symptoms are first to be evaluated suspecting spleen injury. Moreover, confusion, dizziness, disorientation, blurry vision, pallor, tachycardia, hypotension, and loss of consciousness are pathognomic signs denoting intensive internal bleeding and developing hemorrhagic shock.[9–12] In addition, it is essential to use more accurate investigation methods like instrumental examination, particularly focused abdominal sonography for trauma (FAST), abdominal CT, and diagnostic peritoneal lavage (DPL). CT is usually performed with hemodynamically stable patients and helps to detect active extravasation, visualize retroperitoneum and diaphragm injuries. Fractured ribs, bones of pelvis girdle, and vertebral column are commonly diagnosed along with spleen rupture.[13] USG is the method of choice in case of instability.[13,14] DPL is the second-choice instrumental method useful in diagnosing a hollow organ injury.
Two-stage spleen rupture cases are rarer than the acute, although their lethal outcome is more frequent due to the complicated diagnostics.[15,16]
Indications for conservative treatment of parenchymal organs are nonsevere injury, hemodynamic stability, abdominal trauma without multiple ruptures of several organs, no anticoagulant therapy, and successfully performed angioembolization.[14] However, nonoperative management (NOM) is a complex, multidisciplinary strategy that starts with careful clinical observation and constant strict monitoring by means of repeated laboratory tests and radiological imaging.[30,31] After assigning nonoperative treatment, patient must be followed up for at least 72 hours. According to Cirocchi et al systematic review, NOM represented the gold-standard treatment for American Association for the Surgery of Trauma (AAST) grades I and II in 21 nonrandomized studies and was associated with decreased mortality in severe splenic trauma (AAST grades III–V) (4.78% vs 13.5% in NOM and OM, respectively).[27] About 60% of all adult patients and up to 95% of children having spleen rupture are successfully conservatively treated.[17] Nevertheless, the main risk of NOM is the possibility of sudden delayed hemorrhage that could be immediately fatal, before emergency surgery can be performed.[31] Surgical treatment (suturing, spleen resection, splenectomy) is commonly performed with unstable patients, suffering from a serious injury.[14] Due to the profuse bleeding of spleen hemodynamically, unstable patients are usually treated with splenectomy.[2] Comparing to laparotomy, laparoscopic spleen removal is prevalent. Urgent surgery is performed in up to 40% of all cases.[17]
5. Conclusion
In cases of acute spleen rupture, the mean weight of spleen was 309.6 g, whereas in 3 cases of subacute rupture the mean weight of the organ achieved 710 g. The mean weight of spleen in control group with no spleen rupture was 144.7 g. Acute and subacute spleen rupture dating, and morphological evaluation of their properties are found to be important and applicable in clinical practice and forensic pathology.
Author contribution
Investigation: Dmitrij Fomin, Sigitas Chmieliauskas, Vidas Petrauskas, Alina Sumkovskaja, Karolina Ginciene, Eleonora Jurolaic.
Supervision: Sigitas Laima, Jurgita Stasiuniene.
Sigitas Chmieliauskas orcid: 0000-0001-9104-9835.
Footnotes
Abbreviations: AAST = American Association for the Surgery of Trauma, CT = computed tomography, DNA/RNA = deoxyribonucleic acid/ribonucleic acid, DPL = diagnostic peritoneal lavage, FAST = focused abdominal sonography for trauma, H&E = hematoxylin and eosin, NOM = nonoperative management, USG = ultrasonography.
How to cite this article: Fomin D, Chmieliauskas S, Petrauskas V, Sumkovskaja A, Ginciene K, Laima S, Jurolaic E, Stasiuniene J. Traumatic spleen rupture diagnosed during postmortem dissection. Medicine. 2019;98:40(e17363).
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest to disclose.
References
- [1].Dolinak D, Matshes EW, Lew EO. Blunt Force Injury. Forensic Pathology: Principles and Practice. 2005;Burlington, MA: Elsevier, Chapter 5. [Google Scholar]
- [2].Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 7th ed2014;Philadelphia, PA: Lippincott Williams & Wilkins, 256–262. [Google Scholar]
- [3].Biswas G. Review of Forensic Medicine and Toxicology. 2012;London: Jaypee, 204-228. [Google Scholar]
- [4].Spitz WU, Spitz DJ. Blunt Force Injury. Spitz and Fisher's Medicolegal Investigation of Death: Guidelines for the Application of Pathology to Crime Investigation. 4th ed.Springfield, IL: Charles C Thomas; 2006;Chapter 10. [Google Scholar]
- [5].Elsevier, Siegel J, Saukko P. Encyclopedia of Forensic Sciences. 2nd ed2013;8–9. [Google Scholar]
- [6].Simon LV, Bhimji SS. Blunt Force Trauma. Treasure Island, FL: StatPearls Publishing; 2018. [PubMed] [Google Scholar]
- [7].Al-Kindi H, Devi L, George M. Splenic pathology in traumatic rupture of the spleen: a five year study. Oman Med J 2009;2:81–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Gedik E, Girgin S, Aldemir M. Non-traumatic splenic rupture: report of seven cases and review of the literature. World J Gastroenterol 2008;43:6711–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].National Confidential Enquiry into Perioperative Deaths (NCEPOD). Trauma: Who Cares? London: NCEPOD; 2007. Available at: https://www.ncepod.org.uk/2007t.html Accessed December 20, 2018. [Google Scholar]
- [10].Myers J. Focused assessment with sonography for trauma (FAST): the truth about ultrasound in blunt trauma. J Trauma 2007;62:S28. [DOI] [PubMed] [Google Scholar]
- [11].Livingston DH, Lavery RF, Passannante MR, et al. Admission or observation is not necessary after a negative abdominal computed tomographic scan in patients with suspected blunt abdominal trauma: results of a prospective, multi-institutional trial. J Trauma 1998;44:273–80. [DOI] [PubMed] [Google Scholar]
- [12].Isenhour JL, Marx J. Advances in abdominal trauma. Emerg Med Clin North Am 2007;25:713–33. [DOI] [PubMed] [Google Scholar]
- [13].Ruffolo DC. Delayed splenic rupture: understanding the threat. J Trauma Nurs 2002;9:34–40. [DOI] [PubMed] [Google Scholar]
- [14].Jansen JO, Yule SR, Loudon MA. Investigation of blunt abdominal trauma. BMJ 2008;7650:938–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].McGrath A, Whiting D. Recognising and assessing blunt abdominal trauma. Emerg Nurse 2015;22:18–24. [DOI] [PubMed] [Google Scholar]
- [16].Riezzo I, Di Battista B, De Salvia A, et al. Delayed splenic rupture: dating the sub-capsular hemorrhage as a useful task to evaluate causal relationships with trauma. Forensic Sci Int 2014;234:64–71. [DOI] [PubMed] [Google Scholar]
- [17].Bradburn EH, Frankel HL. Diagnosis and management of splenic trauma. J Lancaster Gen Hosp 2010;4:124–9. [Google Scholar]
- [18].Maung AA, Kaplan LJ. Management of Splenic Injury in the Adult Trauma Patient. Philadelphia, PA: Wolters Kluwer Health; 2014. [Google Scholar]
- [19].Hodder & Stoughton Ltd., Payne-James J, Jones R, Karch SB, et al. Forensic Medicine. 13th ed2011;98–110. [Google Scholar]
- [20].Aubrey-Bassler FK, Sowers N. 613 cases of splenic rupture without risk factors or previously diagnosed disease: a systematic review. BMC Emerg Med 2012;12:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Stallard N, Findlay G, Smithies M. Splenic rupture following cardiopulmonary resuscitation. Resuscitation 1997;2:171–3. [DOI] [PubMed] [Google Scholar]
- [22].Lokhvitskii SV, Afendulov SA. Two-stage splenic rupture. Klin Khir 1990;4:35–7. [PubMed] [Google Scholar]
- [23].Kluger Y, Paul DB, Raves JJ, et al. Delayed rupture of the spleen-myths, facts, and their importance: case reports and literature review. J Trauma 1994;4:568–71. [PubMed] [Google Scholar]
- [24].Gaharaj PV. Forensic Medicine. 2003;India: Orient Longman, 107–130. [Google Scholar]
- [25].Farhat GA, Abdu RA, Vanek VW. Delayed splenic rupture: real or imaginary? Am Surg 1992;58:340–5. [PubMed] [Google Scholar]
- [26].Mohammadi S, Hedjazi A, Sajjadian M, et al. Morphometric Study of Spleen in Iranian Cadavers from Razavi-Khorasan Province. Bangladesh Med Res Counc Bull 2016;42:61–6. [Google Scholar]
- [27].Chowdhury AI, Sultana SZ, Mannan S. Morphometric study of splenic volume in Bangladeshi cadaver. Mymensingh Med J 2012;21:445–9. [PubMed] [Google Scholar]
- [28].Chandra Prakash D, Deopa Thakkar HK. Study of internal organ weight and its correlation to body weight in Kumaon region of Uttarakhand. J Indian Acad Forensic Med 2013;35:29–32. [Google Scholar]
- [29].Caglar V, Kumral B, Uygur R, et al. Study of volume, weight and size of normal pancreas, spleen and kidney in adults autopsies. Forensic Med Anat Res 2014;2:63–9. [Google Scholar]
- [30].Grover SA, Barkun AN, Sackett DL. Does this patient have splenomegaly? JAMA 1993;270:2218–21. [PubMed] [Google Scholar]
- [31].Cirocchi R, Boselli C, Corsi A, et al. Is non-operative management safe and effective for all splenic blunt trauma? A systematic review. Crit Care 2013;17:R185. [DOI] [PMC free article] [PubMed] [Google Scholar]