

Abstract
Rotator cuff disease is one of the most common causes of shoulder pain, yet controversy still exists regarding treatment of “irreparable” tears. Nonoperative management, including physical therapy and steroid injections, should be reserved for those without significant pain or functional impairment. Debridement may be used for low-demand patients, and should be performed with partial cuff repair, subacromial decompression, and/or acromioplasty to maximize outcomes. Biceps tenotomy and/or tenodesis have been shown to reduce postoperative pain and improve satisfaction when performed in conjunction with rotator cuff repairs, with no difference in functional outcome comparatively. Tendon transfers have been advocated with the potential benefit to improve function and decrease pain. More recently, extracellular matrix and human-derived dermal allografts have been used off-label as patch grafts in irreparable tears. Superior capsular reconstructive techniques and subacromial balloon spacers serve a similar function by acting to depress the humeral head in a cuff-deficient shoulder, however long-term data is needed before widespread adoption of these procedures. Finally, reverse shoulder arthroplasty serves as a salvage option for low demand elderly patients.
Key words: Rotator cuff tear, Treatment Options, Irreparable rotator cuff tear, massive rotator cuff tear
Introduction
Rotator cuff tears (RCT) are one of the most commonly treated orthopaedic pathologies, yet controversy exists regarding the management of these injuries. Acute traumatic tears in younger patients should be treated operatively to improve long-term function. However, management of tears that are large, chronic, degenerative, and not amenable to repair by standard means is heavily debated. These “irreparable” tears provide an ongoing challenge for the orthopaedic surgeon, with reported treatment failure rates as high as 40% for massive RCTs.1
Authors have attempted to classify these tears based on their size and location.2 Cofield et al. described a massive tear as greater than 5 cm,3 while others consider a massive rotator cuff tear to be one involving two or more tendons.4 Posterosuperior tears involve the supraspinatus and infraspinatus and are more common than anterosuperior tears, which involve the supraspinatus and subscapularis tendons (Figure 1A).5 The size and reparability of a tear are not always related, nor are they mutually exclusive descriptions. A massive tear is not necessarily irreparable, and an irreparable tear does not mean it is massive in size, however usually this is the case. Although the precise definition of an irreparable tear is still debatable, it can be defined surgically as a tear in which direct tendon-to-bone repair and healing is not possible, and as described by Warner et al. as the inability to achieve a direct repair of the native tendon to the humerus despite mobilizing the soft tissues.6 Goutallier described fatty degeneration of the rotator cuff through CT scans and graded the muscle quality with stages 0-IV (Table 1) .7 Irreparable RCTs are generally defined as stage III and IV, although this has been questioned.8 The true determination of an irreparable rotator cuff tear, however, is defined during surgery.
Some studies have analyzed the acromiohumeral index (AHI) to determine whether a RCT is repairable. An AHI of less than 5.8 mm has been associated with decreased likelihood of a repairable tear.9 Recent literature has elucidated additional independent predictors of irreparability including: chronic pseudoparalysis, large mediolateral tear size, positive tangent sign, high grade fatty degeneration of the supraspinatus, and three or four tendon tears.9 Some authors report that up to 30% of total RCTs can be classified as irreparable. 3,6,9 This review will provide an overview of diagnosis and treatment options for irreparable RCTs.
Clinical evaluation
Irreparable rotator cuff tears are unpredictable with respect to their clinical presentation. The spectrum of pain and functional disability varies widely. A shoulder may function well in the setting of a painless tear, whereas a small painful tear may result in substantial shoulder dysfunction and disability. The physical exam should begin with inspection of both upper extremities including the back and scapula with the shoulders and back exposed. The supraspinatus and infraspinatus fossae should be examined for atrophy which could signify chronic degeneration. Table 2 details the diagnostic meaneuvers and tests commonly used to determine the function of each muscle and/or tendon of the rotator cuff.10,11 It has been suggested that the belly press test specifically tests the superior subscapularis fibers while the lift-off test includes the upper and lower subscapularis fibers, however this is debatable.12
Imaging of the shoulder should include a standard set of four X-rays including a true anterior-posterior (grashey) view which can identify pathology of the glenohumeral joint and superior humeral migration, and a standard AP view for acromioclavicular (AC) joint pathology.11 The axillary view assesses the position of the humeral head within the glenoid in the anterior- to-posterior direction. The scapular-Y view allows assessment of the suprascapular outlet as well as the humeral head position relative to the glenoid. Acromial morphology is also clearly delineated on this view. The AHI measures 7 to 14 mm in healthy shoulders on the true AP view.13
Magnetic resonance imaging (MRI) is useful for evaluating rotator cuff tears as well as examining the muscle bellies on T1- weighted sagittal oblique cuts. CT arthrography may be used in the setting of a contraindication to an MRI study.7 Ultrasound has shown to be a valuable technique in detecting rotator cuff tears, with moderate to excellent (72-100%) accuracy in detecting fatty degeneration.14 Though a cost-efficient option, ultrasound is highly operator dependent and requires experience for its proper use.
Management options
Nonoperative treatment
The mainstay of nonoperative management for irreparable RCTs is physical therapy, non-steroidal anti-inflammatory medication (NSAIDs) if able to tolerate, and possibly corticosteroid injections. Physical therapy focuses on deltoid reconditioning (Figure 1B) and periscapular strengthening of secondary shoulder stabilizers such as the pectoralis major and latissimus dorsi.15-17 In a study from the Reading Shoulder Unit, Levy et al. described a nonoperative rehabilitation program for patients with massive RCTs in which patients underwent a program focusing on anterior deltoid strengthening. They experienced a success rate of 82%, and Constant scores increased from 26 to 60 at a minimum of 9 months following treatment and forward flexion increased from 40° to 160°.18 Success using this protocol, however, is based upon having an intact and functional subscapularis. A later study demonstrated a lower success rate of 40% in elderly patients with irreparable RCTs who underwent the anterior deltoid rehabilitation program, suggesting some variability in the efficacy of this home treatment modality.4,19 Subacromial corticosteroid injections as well as NSAIDs may be helpful in alleviating pain in conjunction with physical therapy, but offer only short-term effects on shoulder pain and function.20 Due to questionable effect on intact tendons, lack of proven long-term benefit, and potential for increased postoperative infection risk if shoulder arthroplasty is required in the future, repeated steroid injections are not recommended.20,21
Many patients with RCTs experience significant levels of pain despite nonoperative management. Rockwood et al. published a series of 57 patients with irreparable RCTs treated with a modified Neer acromioplasty, subacromial decompression, and open debridement of massive tears of the supraspinatus and infraspinatus without attempt at partial repair. At 6.5-year followup, 83% of patients had a satisfactory result and 17% of patients had an unsatisfactory result in terms of function and pain relief. Poor results were associated with a weak or dysfunctional anterior deltoid or previous acromioplasty or attempt at rotator cuff repair.22
Further studies have found that debridement performed without attempt at rotator cuff repair offers only temporary pain resolution and less functional improvement compared to partial repair. Melillo et al. concluded that improvement in pain following debridement is short-lived and patients frequently have recurrent pain and continued poor function.23 In a 2010 prospective randomized study comparing functional outcomes following debridement vs. partial repair in 42 patients with massive RCT, both treatments offered significant improvement. Partial RCR offered slightly better functional outcome than debridement despite a 52% structural failure rate in repair.24 A cadaveric study by Oh et al. in 2012 found that partial repair, specifically posterior fixation, was important in restoring glenohumeral kinematics following massive RCT.17 In a 2012 prospective randomized clinical trial, Iagulli et al. found no significant difference in University of California Los Angeles (UCLA) functional outcome scores between partial compared to complete repair of massive RCT at a mean follow-up time of 2 years, demonstrating the potential for functional improvement through partial repair.25 Due to the potential for improved functional outcome using partial repair, contrasted to the recurrence of pain following debridement without partial repair, an attempt at repair is preferred over debridement alone.
Table 1.
Goutallier clasification for rotator cuff disease.
| Goutallier stage | CT findings |
|---|---|
| Stage 0 | Normal muscle (no fat) |
| Stage I | Fatty streaks in muscle |
| Stage II | More muscle than fat |
| Stage III | Equal amounts muscle and fat |
| Stage IV | Less muscle than fat |
Table 2.
Physical exam tests for rotator cuff disease.
| Muscle tested | Diagnostic maneuver or test |
| Supraspinatus | Resisted forward flexion in scapular plane with thumb up10 |
| Infraspinatus | Resisted external rotation with shoulder adducted |
| Subscapularis | Abdominal compression test, lift off test, bear hug test11 |
| Teres minor | Resisted external rotation with elbow flexed 90 degrees and shoulder elevated to 90 degrees in scapular plane |
Figure 1.
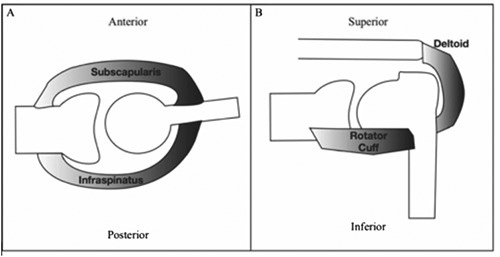
Glenohumeral joint force couples in the transverse plane (A) and coronal plane (B). Anterosuperior rotator cuff tears decrease posterior forces on the humerus, while posteropsuperior rotator cuff tears decrease anterior forces on the humerus (A). Both predispose to laxity in the saggital plane. An insufficient supraspinatus muscle or tendon leads to superior laxity and upward migration of the humeral head. Conditioning the deltoid (B) can restore downward forces on the humerus to minimize such laxity and improve joint kinematics and function.
Biceps tenotomy/tenodesis
Although once thought to be a superior stabilizer of the humeral head,26 the long head of the biceps tendon has been shown to have minial effect on shoulder function or stability,27,28 and is a common source of shoulder pain.29 Failure to address the biceps tendon has been associated with persistent pain and reduced satisfaction following RCR in some studies.29 In a series of 307 patients, Walch performed a biceps tenotomy on patients with irreparable RCT with 2-14 year follow up. All patients had equivalent passive shoulder range of motion on the ipsilateral shoulder and the contralateral “well” shoulder, and an increased Constant score from 48.4 to 67.6 after tenotomy. 87% of patients were either satisfied or very satisfied with surgery.30 Boileau et al. treated 39 irreparable RCTs with a biceps tenotomy and 33 irreparable RCTs with tenodesis. At 35 months, 75% of patients were satisfied with their surgical outcome, and Constant score increased from 46.3 to 66.5, showing similar results to the study by Walch.31 There were no significant differences in satisfaction or Constant scores between tenotomy and tenodesis.
There is currently no consensus regarding performing biceps tenotomy versus tenodesis. In a meta-analysis by Slenker et al., the authors found an 8% rate of cosmetic deformity in the tenotomy group with no clinical differences between groups in terms of satisfaction with the procedure.32 In a prospective cohort study performed by Koh et al., biceps tenotomy was associated with a higher rate of popeye deformity and biceps cramping than tenodesis.33 This same finding was reported in another retrospective cohort study.34 However, neither of these studies found any significant difference in functional outcome scores. Zhang et al. found that tenotomy and tenodesis were equal and effective for treatment of long head biceps lesions in irreparable RCTs, but that tenotomy required shorter surgical time and resulted in faster pain relief.35 A downside of performing tenotomy is that in the rare case that the biceps becomes symptomatic, later tenodesis is not possible.
Tendon transfers
Numerous tendon transfers for the treatment of irreparable RCTs have been proposed. Tendon transfers are used with the intended benefit of providing coverage to the humeral head and improving function.
Latissimus dorsi transfer
The latissimus dorsi muscle has multiple actions on the shoulder including extension, internal rotation, and adduction. The tendon is useful for transfer as it has 33.9 cm of excursion and has a predictable insertion anterior to the teres major tendon and 7 mm lateral.36 Latissimus dorsi tendon transfers (LDTT) are utilized in patients with refractory pain and weakness with an otherwise normal joint space and an irreparable posterosuperior rotator cuff defect. More recently, Elhassan et. al demonstrated the low risk of nerve compression and feasibility of LDTT for irreparable subscapularis tendon repairs.37 For proper use, superior migration of the humeral head must be minimal with an AHI greater than 5 mm. Improvement in external rotation is thought to be due to either tenodesis effect or active muscle contraction, but EMG studies have shown conflicting evidence regarding muscle activation after LDTT.38,39
LDTT can either be performed with a single-incision or two-incision technique. 40,41 Arthroscopic-assisted techniques for LDTT have recently been developed, providing smaller surgical incisions, improved visualization, lower infection rate, and preservation of the deltoid origin, theoretically facilitating faster rehabilitation. 42 Poor outcomes following LDTT have been associated with subscapularis dysfunction, teres minor dysfunction, glenohumeral osteoarthritis, and AC joint arthritis.43 Outcomes after LDTT in properly selected patients show significant pain relief and satisfaction, however, functional improvement is much less predictable. Complications following this procedure are rare, with a recent review article reporting a complication rate of 7.3%, the most common being tendon rupture.42
Pectoralis major transfer
The pectoralis major muscle acts on the shoulder by aiding in flexion, internal rotation, and adduction. This procedure is indicated for patients with weakness caused by anterosuperior RCTs with subscapularis tear. Pectoralis major transfers were first described by Wirth and Rockwood for irreparable tears of the subscapularis and later modified by Resch who described transferring the upper two thirds of the tendon under the conjoined tendon to more closely reproduce the anatomy of the subscapularis. 44,45 This technique later evolved into transfer of the entire pectoralis tendon under the conjoined tendon.46
Trapezius transfer
The lower trapezius tendon transfer was originally described to increase function in patients with brachial plexus palsy.47 Elhassan et al. more recently described its use as an alternative treatment for patients with a posterosuperior deficient rotator cuff.47 In a biomechanical study, the pull of the trapezius external rotation moment arm was significantly higher with the humerus in 0° of adduction than the latissimus dorsi tendons.48 A 2016 case series of irreparable RCTs treated with lower trapezius transfer augmented by Achilles allograft found that 32 of 33 patients had significant improvement in pain, subjective shoulder function, DASH scores, and ROM at an average follow- up time of 47 months. Greatest gains in ROM were observed in patients with >60º of preoperative flexion.49 Another biomechanical study comparing the latissimus transfer to the trapezius transfer showed superiority of the trapezius transfer in restoring glenohumeral kinematics and force coupling.50
Scaffold devices
Over the past decade there have been multiple attempts at biologic and non-biologic augments to rotator cuff tendon healing. Mammalian derived extracellular matrix (ECM) and human derived dermal allograft (GraftJacket, Arthroflex) are currently approved for use by the FDA, although recent AAOS clinical guidelines have recommended against the use of xenograft for augmentation of rotator cuff repair.51 In a study of 16 patients with massive retracted RCT, Bond et al. used a GraftJacket (Wright Medical Technology, Arlington, TN) dermal allograft to repair the rotator cuff tendon stump to the greater tuberosity with suture anchors. Fifteen of 16 patients were satisfied with the procedure and UCLA scores improved from 18.4 to 30.4 postoperatively, Constant scores increased from 53.8 to 84.0 and there were no complications reported.51 However, due to the lack of a control group in their study, this remains controversial. In a biomechanical study, Mura used a synthetic patch graft to bridge the gap after simulated supraspinatus, infraspinatus, and subscapularis defects. Abduction torque was increased in the supraspinatus by 61%, infraspinatus by 68% or subscapularis by 80%.52 In a clinical study by Gupta et al. using human dermal allograft, they found significant improvement in patient pain, range of motion, strength, and overall shoulder function.53 One must bear in mind that the use of augments and scaffolding devices to bridge a defect is currently used “off-label”, and clinical studies have had mixed results regarding efficacy.
Superior capsule reconstruction
Superior capsule reconstruction (SCR) has been suggested for managing irreparable rotator cuff tears by reconstructing the superior capsule in rotator cuff-deficient shoulders.7,23,54 Mihata et al. first described this in a biomechanical study.55 8 mm thick fascia lata (FL) autograft was used to reconstruct the superior capsule of the glenohumeral joint; medially the graft is attached to the superior glenoid and laterally attached to the greater tuberosity.56 In a clinical study of 24 patients with large or massive irreparable RCT, ASES scores improved from 23.5 to 92.9 postoperatively and 84% of patients were free from graft tear at a mean of 34 month follow up. In a 2016 follow-up paper, Milhata et al. found that shoulder stabilization was optimized when the graft was placed at 10 to 30º of glenohumeral abduction, and that an 8mm thick graft provided significantly greater stability compared to a 4mm-thick graft.57
Graft material and vascularity characteristics are import considerations for SCR. Despite early enthusiasm for acellular dermal matrix (ADM) allografts for SCR, early reports have shown significant retear rates, however patients still show clinical improvement in pain and function.58 Mihata et al. biomechanically compared the efficacy of superior capsular reconstruction restoration of superior glenohumeral stability using FL autograft against ADM allograft. In their study, the ADM allograft was shown to have 15% less strength, and only partially restored superior glenohumeral stability, whereas FL allografting completely restored superior stability.59 Studies to improve graft vascularity have emerged as well as a recent cadaveric study demonstrated the feasibility of performing SCR with vascular dermal autograft tissue.60
Balloon interpositioned arthroplasty
In 2012, Savarese and Romeo described arthroscopic implantation of a biodegradable spacer between the acromion and the humeral head for the treatment of irreparable RCTs.61 The spacer is designed to create a physical barrier between tissues and to widen the subacromial space to facilitate deltoid action.62,63 Senekovic et al. reported results of a subacromial spacer with an associated biceps tenotomy and found that 85% of the patients showed a clinically significant improvement of at least 15 points in Constant score, while 62% showed at least 25 points of improvement at five-year follow- up.62 Deranlot et al. described, in a series of 37 patients (39 shoulders), a significant improvement of the Constant score from 45 preoperatively to 76 at a mean of 33 months follow-up. In their study, 92% of the shoulders also underwent a long head of biceps tenotomy.64 While this may serve as an eventual time saving, low-cost option, and satisfactory early clinical results have been shown,65-67 more clinical data is necessary before routine use of the spacer can be recommended.
Reverse total shoulder arthroplasty
Rotator cuff tear arthropathy (RCTA) may develop as a consequence of severe rotator cuff deficiency due to altered glenohumeral kinematics.68 Reverse total shoulder implant is the ideal arthroplasty implant for RCTA. This implant improves function of the rotator cuff deficient shoulder in three important ways: the center of rotation of the glenohumeral joint is medialized which converts the superior shear force at the baseplate-bone interface into a compressive force, the humeral is distalized which tightens the deltoid thus improving its lever arm, and a semi-constrained articulation limits translation and converts the superior-directed pull of the deltoid into a rotational motion at the glenosphere. The deltoid fibers become the sole abductors and elevators of the glenohumeral joint and thus lose their ability to rotate the humerus. Patients with external rotation weakness may require a tendon transfer to improve external rotation strength, but this remains controversial. Simovitch showed that patients with an intact teres minor tendon retained external rotation compared to those with absent tendons or fatty infiltration.69 Although RTSA is best indicated for RCTA, there have been reports regarding its efficacy in the treatment of massive irreparable RCTs in the absence of glenohumeral arthritis. Mulieri et al. showed improvement of ASES scores from 33.3 to 75.4, Simple Shoulder Test (SST) scores from 1.6 to 6.5 and significant pain improvement based on the visual analogue scale (VAS). Most patients had significant clinical improvement and predictable improvement in pain.70
Conclusions
Irreparable rotator cuff tears can be a challenging treatment for the orthopaedic surgeon. While no singular treatment exists that is the gold standard, many options exist. Treatment depends on a patient’s functional status as well as the skill and procedural familiarity of the surgeon. Tendon transfer is common with the lower trapezius tendon gaining popularity. Salvage options for continued pain and decreased function include reverse total shoulder arthroplasty and hemiarthroplasty in rare cases. Superior capsular reconstruction using fascia lata autograft have shown promise, but longterm clinical studies are necessary before definitive conclusions can be drawn.
Funding Statement
Funding: none.
References
- 1.Chung SW, Kim JY, Kim MH, et al. Arthroscopic repair of massive rotator cuff tears: outcome and analysis of factors associated with healing failure or poor postoperative function. Am J Sports Med 2013;41:1674-83. [DOI] [PubMed] [Google Scholar]
- 2.Patte D. Classification of rotator cuff lesions. Clin Orthop Relat Res 1990:81-6. [PubMed] [Google Scholar]
- 3.Cofield RH, Parvizi J, Hoffmeyer PJ, et al. Surgical repair of chronic rotator cuff tears. A prospective long-term study. J Bone Joint Surg Am 2001;83-A:71-7. [DOI] [PubMed] [Google Scholar]
- 4.Oh JH, Park MS, Rhee SM. Treatment Strategy for Irreparable Rotator Cuff Tears. Clin Orthop Surg 2018;10:119-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Omid R, Heckmann N, Wang L, et al. Biomechanical comparison between the trapezius transfer and latissimus transfer for irreparable posterosuperior rotator cuff tears. J Shoulder Elbow Surg 2015;24:1635-43. [DOI] [PubMed] [Google Scholar]
- 6.Warner JJ. Management of massive irreparable rotator cuff tears: the role of tendon transfer. Instr Course Lect 2001;50:63-71. [PubMed] [Google Scholar]
- 7.Goutallier D, Postel JM, Bernageau J, et al. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994:78-83. [PubMed] [Google Scholar]
- 8.Burkhart SS, Barth JR, Richards DP, et al. Arthroscopic repair of massive rotator cuff tears with stage 3 and 4 fatty degeneration. Arthroscopy 2007;23:347-54. [DOI] [PubMed] [Google Scholar]
- 9.Kim IB, Jung DW, Suh KT. Prediction of the Irreparability of Rotator Cuff Tears. Arthroscopy. 2018. [DOI] [PubMed] [Google Scholar]
- 10.Lee CK, Itoi E, Kim SJ, et al. Comparison of muscle activity in the empty-can and full-can testing positions using 18 F-FDG PET/CT. J Orthop Surg Res 2014;9:85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.O’Kane JW, Toresdahl BG. The evidenced- based shoulder evaluation. Curr Sports Med Rep 2014;13:307-13. [DOI] [PubMed] [Google Scholar]
- 12.Tokish JM, Decker MJ, Ellis HB, et al. The belly-press test for the physical examination of the subscapularis muscle: electromyographic validation and comparison to the lift-off test. J Shoulder Elbow Surg 2003;12:427-30. [DOI] [PubMed] [Google Scholar]
- 13.Weiner DS, Macnab I. Superior migration of the humeral head. A radiological aid in the diagnosis of tears of the rotator cuff. J Bone Joint Surg Br 1970;52:524-7. [PubMed] [Google Scholar]
- 14.Mall NA, Kim HM, Keener JD, et al. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. J Bone Joint Surg Am 2010;92:2623-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ainsworth R. Physiotherapy rehabilitation in patients with massive, irreparable rotator cuff tears. Musculoskeletal Care 2006;4:140-51. [DOI] [PubMed] [Google Scholar]
- 16.Ainsworth R, Lewis JS. Exercise therapy for the conservative management of full thickness tears of the rotator cuff: a systematic review. Br J Sports Med 2007;41:200-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Oh JH, McGarry MH, Jun BJ, et al. Restoration of shoulder biomechanics according to degree of repair completion in a cadaveric model of massive rotator cuff tear: importance of margin convergence and posterior cuff fixation. Am J Sports Med 2012;40:2448-53. [DOI] [PubMed] [Google Scholar]
- 18.Levy O, Mullett H, Roberts S, Copeland S. The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears. J Shoulder Elbow Surg 2008;17:863-70. [DOI] [PubMed] [Google Scholar]
- 19.Yian EH, Sodl JF, Dionysian E, Schneeberger AG. Anterior deltoid reeducation for irreparable rotator cuff tears revisited. J Shoulder Elbow Surg 2017;26:1562-5. [DOI] [PubMed] [Google Scholar]
- 20.Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev. 2003:CD004016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singh JA, Sperling JW, Schleck C, et al. Periprosthetic infections after total shoulder arthroplasty: a 33-year perspective. J Shoulder Elbow Surg 2012;21:1534-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rockwood CA, Williams GR, Burkhead WZ. Débridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-66. [DOI] [PubMed] [Google Scholar]
- 23.Melillo AS, Savoie FH, Field LD. Massive rotator cuff tears: debridement versus repair. Orthop Clin North Am 1997;28:117-24. [DOI] [PubMed] [Google Scholar]
- 24.Berth A, Neumann W, Awiszus F, Pap G. Massive rotator cuff tears: functional outcome after debridement or arthroscopic partial repair. J Orthop Traumatol 2010;11:13-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Iagulli ND, Field LD, Hobgood ER, et al. Comparison of partial versus complete arthroscopic repair of massive rotator cuff tears. Am J Sports Med 2012;40:1022-6. [DOI] [PubMed] [Google Scholar]
- 26.Warner JJ, McMahon PJ. The role of the long head of the biceps brachii in superior stability of the glenohumeral joint. J Bone Joint Surg Am 1995;77:366-72. [DOI] [PubMed] [Google Scholar]
- 27.Yamaguchi K, Riew KD, Galatz LM, et al. Biceps activity during shoulder motion: an electromyographic analysis. Clin Orthop Relat Res 1997:122-9. [DOI] [PubMed] [Google Scholar]
- 28.Levy AS, Kelly BT, Lintner SA, et al. Function of the long head of the biceps at the shoulder: electromyographic analysis. J Shoulder Elbow Surg 2001;10:250-5. [DOI] [PubMed] [Google Scholar]
- 29.Virk MS, Cole BJ. Proximal Biceps Tendon and Rotator Cuff Tears. Clin Sports Med 2016;35:153-61. [DOI] [PubMed] [Google Scholar]
- 30.Walch G, Edwards TB, Boulahia A, et al. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: clinical and radiographic results of 307 cases. J Shoulder Elbow Surg 2005;14:238-46. [DOI] [PubMed] [Google Scholar]
- 31.Boileau P, Baqué F, Valerio L, et al. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am 2007;89:747-57. [DOI] [PubMed] [Google Scholar]
- 32.Slenker NR, Lawson K, Ciccotti MG, et al. Biceps tenotomy versus tenodesis: clinical outcomes. Arthroscopy 2012;28:576-82. [DOI] [PubMed] [Google Scholar]
- 33.Koh KH, Ahn JH, Kim SM, Yoo JC. Treatment of biceps tendon lesions in the setting of rotator cuff tears: prospective cohort study of tenotomy versus tenodesis. Am J Sports Med 2010;38:1584-90. [DOI] [PubMed] [Google Scholar]
- 34.De Carli A, Vadalà A, Zanzotto E, et al. Reparable rotator cuff tears with concomitant long-head biceps lesions: tenotomy or tenotomy/tenodesis? Knee Surg Sports Traumatol Arthrosc 2012;20:2553-8. [DOI] [PubMed] [Google Scholar]
- 35.Zhang Q, Zhou J, Ge H, Cheng B. Tenotomy or tenodesis for long head biceps lesions in shoulders with reparable rotator cuff tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc 2015;23:464-9. [DOI] [PubMed] [Google Scholar]
- 36.Herzberg G, Urien JP, Dimnet J. Potential excursion and relative tension of muscles in the shoulder girdle: relevance to tendon transfers. J Shoulder Elbow Surg 1999;8:430-7. [DOI] [PubMed] [Google Scholar]
- 37.Elhassan B, Christensen TJ, Wagner ER. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: an anatomic study. J Shoulder Elbow Surg 2014;23:492-9. [DOI] [PubMed] [Google Scholar]
- 38.Iannotti JP, Hennigan S, Herzog R, et al. Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. Factors affecting outcome. J Bone Joint Surg Am 2006;88:342-8. [DOI] [PubMed] [Google Scholar]
- 39.Irlenbusch U, Bernsdorf M, Born S, et al. Electromyographic analysis of muscle function after latissimus dorsi tendon transfer. J Shoulder Elbow Surg 2008;17:492-9. [DOI] [PubMed] [Google Scholar]
- 40.Habermeyer P, Magosch P, Rudolph T, et al. Transfer of the tendon of latissimus dorsi for the treatment of massive tears of the rotator cuff: a new singleincision technique. J Bone Joint Surg Br 2006;88:208-12. [DOI] [PubMed] [Google Scholar]
- 41.Gerber C, Vinh TS, Hertel R, Hess CW. Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff. A preliminary report. Clin Orthop Relat Res 1988:51-61. [PubMed] [Google Scholar]
- 42.Memon M, Kay J, Quick E, et al. Arthroscopic-Assisted Latissimus Dorsi Tendon Transfer for Massive Rotator Cuff Tears: A Systematic Review. Orthop J Sports Med 2018;6:232596-7118777735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gerber C, Rahm SA, Catanzaro S, et al. Latissimus dorsi tendon transfer for treatment of irreparable posterosuperior rotator cuff tears: long-term results at a minimum follow-up of ten years. J Bone Joint Surg Am 2013;95:1920-6. [DOI] [PubMed] [Google Scholar]
- 44.Wirth MA, Rockwood CA. Operative treatment of irreparable rupture of the subscapularis. J Bone Joint Surg Am 1997;79:722-31. [DOI] [PubMed] [Google Scholar]
- 45.Resch H, Povacz P, Ritter E, Matschi W. Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon. J Bone Joint Surg Am 2000;82:372-82. [DOI] [PubMed] [Google Scholar]
- 46.Galatz LM, Connor PM, Calfee RP, et al. Pectoralis major transfer for anteriorsuperior subluxation in massive rotator cuff insufficiency. J Shoulder Elbow Surg 2003;12:1-5. [DOI] [PubMed] [Google Scholar]
- 47.Elhassan B, Bishop A, Shin A. Trapezius transfer to restore external rotation in a patient with a brachial plexus injury. A case report. J Bone Joint Surg Am 2009;91:939-44. [DOI] [PubMed] [Google Scholar]
- 48.Hartzler RU, Barlow JD, An KN, Elhassan BT. Biomechanical effectiveness of different types of tendon transfers to the shoulder for external rotation. J Shoulder Elbow Surg 2012;21:1370-6. [DOI] [PubMed] [Google Scholar]
- 49.Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior- superior rotator cuff tear. J Shoulder Elbow Surg 2016;25:1346-53. [DOI] [PubMed] [Google Scholar]
- 50.Omid R, Cavallero MJ, Granholm D, et al. Surgical anatomy of the lower trapezius tendon transfer. J Shoulder Elbow Surg 2015;24:1353-8. [DOI] [PubMed] [Google Scholar]
- 51.Bond JL, Dopirak RM, Higgins J, et al. Arthroscopic replacement of massive, irreparable rotator cuff tears using a GraftJacket allograft: technique and preliminary results. Arthroscopy 2008;24:403-9. [DOI] [PubMed] [Google Scholar]
- 52.Mura N, O’Driscoll SW, Zobitz ME, et al. Biomechanical effect of patch graft for large rotator cuff tears: a cadaver study. Clin Orthop Relat Res 2003:131-8. [DOI] [PubMed] [Google Scholar]
- 53.Gupta AK, Hug K, Berkoff DJ, et al. Dermal tissue allograft for the repair of massive irreparable rotator cuff tears. Am J Sports Med 2012;40:141-7. [DOI] [PubMed] [Google Scholar]
- 54.Thorsness R, Romeo A. Massive Rotator Cuff Tears: Trends in Surgical Management. Orthopedics 2016;39: 145-51. [DOI] [PubMed] [Google Scholar]
- 55.Mihata T, Lee TQ, Watanabe C, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy 2013;29:459-70. [DOI] [PubMed] [Google Scholar]
- 56.Mihata T, McGarry MH, Pirolo JM, et al. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: a biomechanical cadaveric study. Am J Sports Med 2012;40:2248-55. [DOI] [PubMed] [Google Scholar]
- 57.Mihata T, McGarry MH, Kahn T, et al. Biomechanical Effect of Thickness and Tension of Fascia Lata Graft on Glenohumeral Stability for Superior Capsule Reconstruction in Irreparable Supraspinatus Tears. Arthroscopy 2016;32:418-26. [DOI] [PubMed] [Google Scholar]
- 58.Denard PJ, Brady PC, Adams CR, et al. Preliminary Results of Arthroscopic Superior Capsule Reconstruction with Dermal Allograft. Arthroscopy 2018;34:93-9. [DOI] [PubMed] [Google Scholar]
- 59.Mihata T, Bui CNH, Akeda M, et al. A biomechanical cadaveric study comparing superior capsule reconstruction using fascia lata allograft with human dermal allograft for irreparable rotator cuff tear. J Shoulder Elbow Surg 2017;26:2158-66. [DOI] [PubMed] [Google Scholar]
- 60.Stone MA, Carre A, Trasolini N, et al. Vascularized dermal autograft for the treatment of irreparable rotator cuff tears. J Shoulder Elbow Surg. 2018. [DOI] [PubMed] [Google Scholar]
- 61.Savarese E, Romeo R. New solution for massive, irreparable rotator cuff tears: the subacromial “biodegradable spacer”. Arthrosc Tech 2012;1:e69-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Senekovic V, Poberaj B, Kovacic L, et al. The biodegradable spacer as a novel treatment modality for massive rotator cuff tears: a prospective study with 5- year follow-up. Arch Orthop Trauma Surg 2017;137:95-103. [DOI] [PubMed] [Google Scholar]
- 63.Holschen M, Brand F, Agneskirchner JD. Subacromial spacer implantation for massive rotator cuff tears: Clinical outcome of arthroscopically treated patients. Obere Extrem 2017;12:38-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Deranlot J, Herisson O, Nourissat G, et al. Arthroscopic Subacromial Spacer Implantation in Patients With Massive Irreparable Rotator Cuff Tears: Clinical and Radiographic Results of 39 Retrospectives Cases. Arthroscopy 2017;33:1639-44 [DOI] [PubMed] [Google Scholar]
- 65.Moon AS, Patel HA, Ithurburn MP, et al. Subacromial Spacer Implantation for the Treatment of Massive Irreparable Rotator Cuff Tears: A Systematic Review. Arthroscopy 2019;35:607-14. [DOI] [PubMed] [Google Scholar]
- 66.Ricci M, Vecchini E, Bonfante E, et al. A clinical and radiological study of biodegradable subacromial spacer in the treatment of massive irreparable rotator cuff tears. Acta Biomed 2017;88:75-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Yallapragada RK, Apostolopoulos A, Katsougrakis I, Selvan TP. The use of a subacromial spacer-inspace balloon in managing patients with irreparable rotator cuff tears. J Orthop 2018;15:862-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Ishihara Y, Mihata T, Tamboli M, et al. Role of the superior shoulder capsule in passive stability of the glenohumeral joint. J Shoulder Elbow Surg.2014;23:642-8. [DOI] [PubMed] [Google Scholar]
- 69.Simovitch RW, Helmy N, Zumstein MA, Gerber C. Impact of fatty infiltration of the teres minor muscle on the outcome of reverse total shoulder arthroplasty. J Bone Joint Surg Am 2007;89:934-9. [DOI] [PubMed] [Google Scholar]
- 70.Mulieri P, Dunning P, Klein S, et al. Reverse shoulder arthroplasty for the treatment of irreparable rotator cuff tear without glenohumeral arthritis. J Bone Joint Surg Am 2010;92:2544-56. [DOI] [PubMed] [Google Scholar]