

Abstract
Purpose:
To record central corneal thickness and corneal diameter in preterm and term newborns within first week of their birth and in preterm neonates at term age.
Methods:
Babies born at ≤34 weeks of gestation period (n = 100), term babies who have a gestation period of >37 weeks (n = 100) and preterm neonates at term age (38-42 weeks) who were born at ≤34 weeks (n = 100) were included in this hospital based observational descriptive study. Corneal diameter was taken by Castroviejo Calipers. Central corneal thickness was measured using portable ultrasonic pachymeter (Pachette 3). Refractive status of the eyes was measured using streak Wellch Allyn retinoscope under cyclopentolate cycloplegia.
Results:
Measure of central corneal thickness and corneal diameter in preterm newborns was found to be 633.5 ± 2.8 μm and 8.1 ± 0.6 mm, in full term newborns it was 555.1 ± 2.7 μm and 9.5 ± 0.6 mm, and in preterm neonates at term age, it was 563.5 ± 2.5 μm and 9.6 ± 0.5 mm, respectively. Mean central corneal thickness was found to be more in preterm newborns 633.5 um then term newborns 555.1 um and the difference was statistically significant (P =0.001). Mean corneal diameter was found to be maximum (9.6 mm) in preterm neonates at term age.
Conclusion:
Preterm babies have thick corneas and small corneal diameters. This study is useful with respect to the analysis of glaucoma in children and using preterm corneas as donor corneas in penetrating keratoplasty.
Keywords: Corneal diameter, corneal thickness, newborn
The cornea of preterm is different from a term newborns in parameters like corneal thickness, diameter and refractive power. Central corneal thickness (CCT) measurement plays an important role in diagnosis and treatment of various eye disorders. The number of preterm births has risen significantly in recent times with advanced medical care. Still there is very scant data on the central corneal thickness of premature and full term newborns during the neonatal period. A few studies such as Autzen and Bjørnstrøm[1] (13 premature infants), Kirwan et al.[2] (35 premature infants), and more recently by De Silva et al.[3] (56 premature infants), Uva et al.[4] (33 premature infants), Gunay et al.[5] (100 premature infants) and Jethani et al.[6] (85 premature infants) have presented their findings on the CCT in premature children.
The aim of this study is to record central corneal thickness and corneal diameter in preterm and term newborns within the first week of their birth and in preterm neonates at term age. There is very little literature about corneal thickness in preterm newborns worldwide and no study (to the best of the research knowledge) in India has been conducted for central corneal thickness and corneal diameter in preterm and term newborns and preterm neonates at term age.
Methods
The current study is a Hospital based observational descriptive study which has been carried out at “Department of Ophthalmology and Department of Pediatrics and Neonatology” in a tertiary care centre from November 2013 to March 2015. The study was approved by the ethical committee of the institution.
There were 3 groups of participants. They were as follows: Group A, with 100 preterm newborns; Group B, with 100 full term newborns; Group C, with 100 preterm neonates as they reached term age. Preterm and term newborns within first week of their birth and preterm neonates at term age underwent one time examination for this study.
The non-invasive nature of the procedure was explained to the parents and appropriate consent was obtained from them. All selected preterm and term babies fulfilling the inclusion criteria were subjected to detailed birth and postnatal history. Mother's antenatal history was recorded. Those not fulfilling the inclusion criteria have been excluded.
Inclusion criteria
All the subjects with following characteristics have been included in the study:
Group A: Babies born at ≤34 weeks of gestation period
Group B: Term babies who have a gestation period of >37 weeks
Group C: Preterm babies at term age (38-42 weeks) who were born at ≤34 weeks
Clinically stable babies who are not carrying any major symptom which can make the study biased towards it
Parental consent to record data.
Exclusion criteria
All the subjects with the following characteristics have been excluded from the study:
Babies with any congenital ocular abnormalities
Babies with congenital glaucoma
Babies with congenital cataract
Babies with retinopathy of prematurity.
Eye speculum was applied and paracaine drop was instilled in the eye. The right eye was examined first and then the left. Corneal diameter was taken by Castroviejo Calipers. Central corneal thickness was measured using portable ultrasonic pachymeter. The DGH 555 Ultrasonic Pachymeter (Pachette 3) is an ultrasonic pachymeter that uses echo spike techniques to measure the thickness of the cornea. An average of three pachymetry readings were taken. The reference point here was the centre of the undilated pupil. Refractive status of the eyes was measured using streak Wellch Allyn retinoscope under cyclopentolate cycloplegia. All the measurements were recorded by the same investigator.
Finally, once the recording was done, the data sheet was prepared for the statistical software (SPSS) to run and compute various statistical tests. The results thus obtained have been presented in a graphical and tabular manner in the report.
Results
The demographic profiles of the three groups were recorded.
The mean age of the preterm babies was found to be 31.7 ± 2.3 weeks while mean weight was found to be 1420 ± 600 grams. Amongst term age newborns, mean age was 38.4 ± 2.3 weeks and mean weight was 2880 ± 500 grams. The mean age of the preterm neonates at term age was found to be 39.8 ± 1.5 weeks, while mean weight was found to be 1740 ± 700 grams [Table 1].
Table 1.
The post conceptional age (in weeks) and weight (in grams) distribution of the three groups
| Groups | Age in weeks | Weight in grams | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Group A: Preterm Newborns (n=100) | 31.7 | 2.3 | 1420 | 600 |
| Group B: Term Newborns (n=100) | 38.4 | 2.3 | 2880 | 500 |
| Group C: Preterm Neonates at term age (n=100) | 39.8 | 1.5 | 1740 | 700 |
Mean central corneal thickness was found to be maximum 633.5 um in preterm newborns and minimum in term newborns 555.1 um and the difference was statistically significant too (P = 0.001). Mean corneal diameter was found to be maximum 9.6 mm in preterm neonates at term age and minimum in preterm newborns 8.1 mm and the difference was statistically significant too (P =0.001) [Table 2].
Table 2.
Central corneal thickness and corneal diameter at birth in preterm newborn vs term newborn vs preterm neonates at term age
| GROUPS | Mean Central corneal thickness (um) | Mean corneal diameter (mm) |
|---|---|---|
| Group A: Preterm Newborns (n=100) | 633.5±2.8 μm | 8.1±0.6 mm |
| Group B: Term Newborns (n=100) | 555.1±2.7 μm | 9.5±0.6 mm |
| Group C: Preterm Neonates at term age (n=100) | 563.5±2.5 μm | 9.6±0.5 mm |
| Group A vs Group B | Group A vs Group B | |
| P | 0.001 | 0.003 |
| Group B vs Group C | Group B vs Group C | |
| P | 0.115 | 0.010 |
| Group C vs Group A | Group C vs Group A | |
| P | 0.001 | 0.001 |
The term newborns had the highest overall refraction while the preterm neonates at term age had the lowest refraction. Amongst the 3 groups, the refraction was not very much varying for right eye, left eye and on the overall basis. Thus, it was found that refraction of preterm newborns, full term newborn, and preterm neonates at term age was found to be similar and they are hypermetropic [Table 3 and Fig. 1].
Table 3.
Refractive errors at birth in preterm neonates vs term newborn vs preterm neonates at term age
| GROUPS | Right Eye | Left Eye | Overall |
|---|---|---|---|
| Group A: Preterm Newborns (n=100) | +2.40±1.53 | +2.38±1.45 | +2.39±1.43 |
| Group B: Term Newborns (n=100) | +2.54±1.44 | +2.53±1.07 | +2.53±1.39 |
| Group C: Preterm Neonates at term age (n=100) | +2.03±1.03 | +2.02±1.06 | +2.03±0.99 |
| Group A vs Group B | Group B vs Group C | Group C vs Group A | |
| P | 0.253 | 0.002 | 0.020 |
Figure 1.
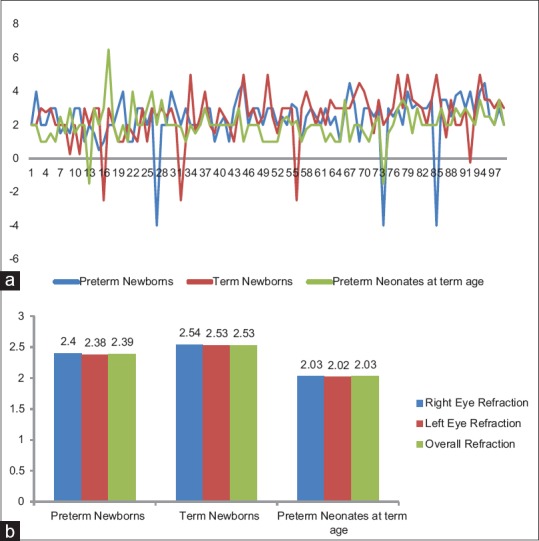
(a) Distribution chart for refractive errors at birth in preterm vs term newborn vs preterm neonates at term age. (b) Distribution chart for variation of refractive errors between right and left eye at birth in preterm vs term newborn vs preterm neonates at term age
Discussion
The preterm newborns have a thicker and smaller cornea. In our study, measure of central corneal thickness and corneal diameter in preterm newborns was found to be 633.5 ± 2.8 μm and 8.1 ± 0.6 mm respectively. Measure of central corneal thickness and corneal diameter in full term newborns was found to be 555.1 ± 2.7 μm and 9.5 ± 0.6 mm, respectively. There was no significant difference found between the right eye and left eye measurements.
These results were similar with that of the previous researchers. In Turkey, the overall mean central corneal thickness was found to be 647.7 ± 63.9 μm for babies having gestation period of 25-34 weeks i.e. preterm newborns.[7] Similarly, in England, for full term newborns, the mean central corneal thickness was measured to be 581 ± 4.7 μm.[8] Also, with respect to corneal diameter study in Saudi Arabia by KU al-Umran et al. showed that corneal diameter ranged between 7.7 mm in preterm newborns and 10 mm in full term babies.[9,10]
In our study, the central corneal thickness and corneal diameter in preterm neonates at term age was obtained and it was found to be 563.5 ± 2.5 μm and 9.6 ± 0.5 mm respectively.
Moreover, there was no significant difference in central corneal thickness and corneal diameter of preterm neonates at term age and full term newborns. This clearly shows that preterm babies catch up with the term babies in the parameters like central corneal thickness and corneal diameter. This is similar to parameters such as weight and length of the preterm babies, which also is nearly the same in preterm babies at term age to that of the full term.
Studies in Ireland by Kirwan et al. have shown that central corneal thickness in preterm newborns decreases from 691 um at 31 weeks to 605 um at 38 weeks along with a significant increase in horizontal corneal diameter of 8.0 mm at 31 weeks to 8.9 mm at 38 weeks. These parameters further changed to central corneal thickness of 564 μm and corneal diameter 9.6 mm at 39-41 weeks age i.e., their term age.[2] The change in the 2 corneal parameters seem to be related to each other and began immediately after birth.
De Silva et al.[3] in Italy conducted a study on the thickness development in premature infants, and it was concluded that central corneal thickness decreased from 794 to 559 μm from preterm newborns at term age to term newborns. Uva et al. reported a mean CCT of 599 ± 36 μ in premature newborns and 576 ± 26 μ in full term newborns.[4] Jethani et al. did a comparison of central corneal thickness on the basis of post-gestational age which showed a mean thickness of 620.7 ± 88.8 and 574.4 ± 78.3 μ in the <260 days and >260 days age groups respectively.[6]
Our data of 633.5 ± 2.8 μm and for preterm is similar to reported by Jethani et al.,[6] but lower than the studies by Autzen and Bjørnstrøm,[1] Kirwan et al.[2] De Silva et al.[3] and Gunay et al.[5] Gunay et al. and Uva et al. also correlated birth weight and CCT. Their study on premature children suggested that the birth weight was negatively correlated with CCT.[4,5]
Intraocular pressure measurement in glaucoma is related to the corneal thickness. Thicker corneas give a false high measurement of intra ocular pressure. Moreover, preterm newborns are associated with increased corneal hydration at birth. So, while diagnosing congenital glaucoma in a neonate, knowledge of this increased thickness would be of great significance. Although the increased corneal thickness increases the IOP recorded, there is also increased corneal hydration which may lead to ease of corneal deformation or applanation. Moses et al.[11] described underestimation of IOP in oedematous corneas due to increased applanation and corneal deformation.
Acar et al. recorded the intraocular pressure and central corneal thickness in healthy premature infants. The mean IOP was 16.8 ± 2.9 mm Hg and the mean CCT, 590 ± 58.2 μm.[12] IOP and CCT values were found to be higher in infants with lower PCA. Higher IOP values in these infants was associated with higher CCT values. Similarly, follow-up of a diagnosed glaucoma in preterm newborns would have to be done keeping in view of this change of corneal thickness up till term age.
The use of donor cornea of a preterm in corneal transplantation was always considered to be difficult. This is basically due to the increased thickness of the cornea of preterm newborns. Preterm newborns used as donor corneas in penetrating keratoplasty yield refractive errors with myopic shift because of the steep corneal configuration in preterm newborns. The surgical difficulties are encountered because of thick cornea of these preterm babies. The knowledge of this increased thickness would help in clinical implications of the use of such corneas in penetrating keratoplasty.
It was found in our study that refraction in the preterm newborns, full term newborn preterm neonates at term age was found to be similar and they are hypermetropic. However, Snir et al.[13] found that full term infants are usually hypermetropic, whereas premature babies, with or without previous retinopathy of prematurity (ROP), more often have myopia and astigmatism. The risk of myopia increases in the presence of ROP, and its magnitude increases with a decrease in the age of prematurity and an increase in severity of the residua of ROP. Babies developing ROP are considered to have anterior segment arrest. It is possible that their corneal thickness remains thicker and do not come to normal value at term age.
Limitation of our study includes small sample size and lack of follow up of preterm babies till term age as it was a one-time study. Moreover, it could have been more informative if IOP was also measured along with corneal measurements, but further studies for the same can be planned.
Conclusion
This study analyzes central corneal thickness and corneal diameter amongst preterm newborns, full term newborns and preterm neonates at term age.
Major results obtained from the study suggests that central corneal thickness at birth in preterm newborn is significantly more than term newborn and preterm neonates at term age. The corneal diameter at birth in preterm newborn is significantly less than term newborn and preterm neonates at term age. The central corneal thickness and corneal diameter in preterm neonates at term age is almost equivalent to term newborn.
This study is useful with respect to the analysis of glaucoma in children and using preterm corneas as donor corneas in penetrating keratoplasty. Preterm babies have the ability to catch up with the full term in various parameters, including but not limited to corneal thickness and corneal diameter. This finding could help in computing the gestational age of preterm newborns. Also, we suggest further study of corneal thickness in babies developing retinopathy of prematurity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Autzen T, Bjørnstrøm L. Central corneal thickness in premature babies. Acta Ophthalmol (Copenh) 1991;69:251–2. doi: 10.1111/j.1755-3768.1991.tb02720.x. [DOI] [PubMed] [Google Scholar]
- 2.Kirwan C, O’Keefe M, Fitzsimon S. Central corneal thickness and corneal diameter in premature infants. Acta Ophthalmol Scand. 2005;83(Suppl 6):751–3. doi: 10.1111/j.1600-0420.2005.00559.x. [DOI] [PubMed] [Google Scholar]
- 3.De Silva S, Parentin F, Michieletto P, Pensiero S. Corneal curvature and thickness development in premature infants. J Pediatr Ophthalmol Strabismus. 2011;48:25–9. doi: 10.3928/01913913-20100318-02. [DOI] [PubMed] [Google Scholar]
- 4.Uva MG, Reibaldi M, Longo A, Avitabile T, Gagliano C, Scollo D, et al. Intraocular pressure and central corneal thickness in premature and full-term newborns. J AAPOS. 2011;15:367–9. doi: 10.1016/j.jaapos.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 5.Gunay M, Celik G, Gunay BO, Dogru M, Gursoy T, Ovali HF. Central corneal thickness measurements in premature infants. Int J Ophthalmol. 2014;7:496–500. doi: 10.3980/j.issn.2222-3959.2014.03.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jethani J, Shah K, Jethani M. Evaluating the change in central corneal thickness in neonates (term and preterm) in Indian population and the factors affecting it. Indian J Ophthalmol. 2015;63:501–3. doi: 10.4103/0301-4738.162601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Murat G, Celik G, Gunay BO, Dogru M, Gursoy T, Ovali HF. Central corneal thickness measurements in premature infants. International J Ophthalmol. 2014;7(Suppl 3):496–500. doi: 10.3980/j.issn.2222-3959.2014.03.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pennie FC, Wood ICJ, Olsen C, White S, Charman WN. A longitudinal study of the biometric and refractive changes in full-term infants during the first year of life. Vision Res. 2001;41(Suppl 21):2799–810. doi: 10.1016/s0042-6989(01)00169-9. [DOI] [PubMed] [Google Scholar]
- 9.Al-Umran, Khaled U, Maurizio FP. Corneal diameter in premature infants. Br J Ophthalmol. 1992;76(Suppl 5):292–3. doi: 10.1136/bjo.76.5.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rushood AA, Zahrani MH, Khamis A, Rushood AA. Central corneal thickness in full-term Saudi newborns. Acta Ophthalmol. 2012;90(Suppl 5):355–8. doi: 10.1111/j.1755-3768.2012.02412.x. [DOI] [PubMed] [Google Scholar]
- 11.Moses RA. The Goldmann applanation tonometer. Am J Ophthalmol. 1958;46:865–9. doi: 10.1016/0002-9394(58)90998-x. [DOI] [PubMed] [Google Scholar]
- 12.Acar DE, Acar U, Tunay ZO, Ozdemir O, Dolgun A, Erdurmus M. The intraocular pressure and central corneal thickness in healthy premature infants. JAAPOS. 2015;19:108–11. doi: 10.1016/j.jaapos.2014.10.027. [DOI] [PubMed] [Google Scholar]
- 13.Snir M, Friling R, Weinberger D, Sherf I, Axer-Siegel R. Refraction and keratometry in 40 week old premature (corrected age) and term infants. Br J Ophthalmol. 2004;88(Suppl 7):900–4. doi: 10.1136/bjo.2003.037499. [DOI] [PMC free article] [PubMed] [Google Scholar]