

Dear Editor:
A kind of herbs, aconite is known for cardiac toxicity [1,2]. Hemodynamic support using extracorporeal life support (ECLS) may be good method if failed conventional resuscitation. We report two experiences using ECLS in aconite intoxication.
A 47-year-old man, who had taken 20 herbal tablets containing aconite, visited the emergency room because of chest discomfort. An initial electrocardiography (ECG) showed persistent multifocal ventricular tachycardia (Figure 1). He repeatedly became pulseless and unconscious. All conventional resuscitation methods including antiarrhythmic medicines, chest compression, and electric cardioversion failed to maintain a stable condition. After 10 minutes of resuscitation, extracorporeal membrane oxygenation (ECMO) was inserted immediately. A 15-F arterial and 22-F venous catheter were percutaneously inserted into the right femoral vessels. The initial flow rate was set at 2 L/min. Although ventricular tachyarrhythmia occurred frequently on the first hospital day, soon after, the vital signs were stabilized. ECG showed a normal sinus rhythm after 33 hours of ECLS. The ECLS was removed on hospital day 2. He was discharged on hospital day 10.
Figure 1.
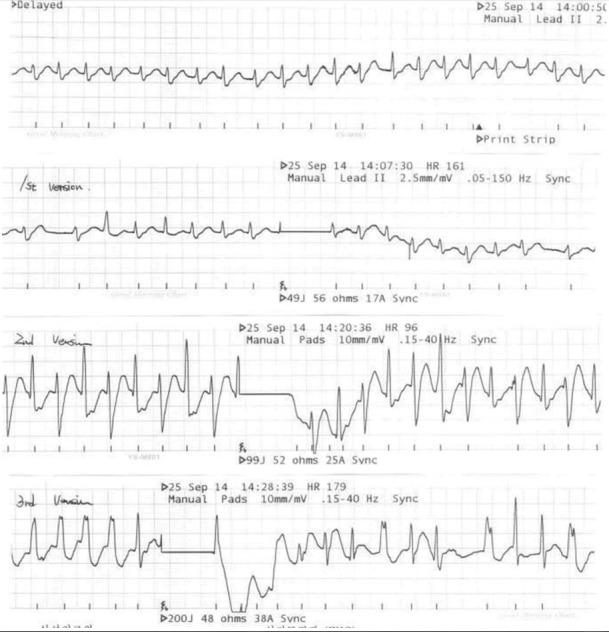
Initial and post-cardioversion electrocardiography: persistent multifocal ventricular tachycardia.
Other case, a 31-year-old man, ingested an unknown number of tablets containing aconite and had difficulty in moving and chest discomfort, was referred to Samsung Medical Center. The initial ECG showed an irregular rhythm with a narrow QRS (Figure 2). Despite conventional resuscitation, the ventricular tachycardia was sustained. After a few minutes, a 15-F arterial and 22-F venous catheter were inserted. The patient’s vital signs were stabilized and ECG rhythm regained normal sinus rhythm after 9 hours of ECLS support. The ECLS was removed on hospital day 2. He was discharged on hospital day 7.
Figure 2.
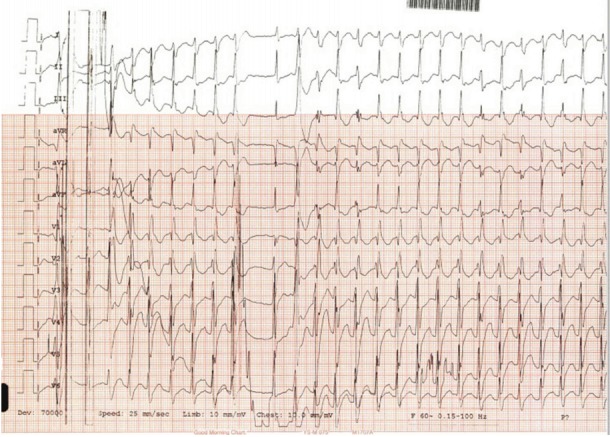
Electrocardiography upon arrival at the emergency room: persistent multifocal ventricular tachycardia with right bundle branch block pattern.
Aconite induces refractory ventricular arrhythmia. The symptoms of poisoning appear 10 minutes to 3 hours after aconite is ingested [3,4]. When cardiogenic shock are refractory to medical treatment, it is most important to maintain blood pressure and tissue oxygenation by the use of a percutaneous cardiopulmonary bypass [5]. During the clearance of aconite from the body, ECMO may substitute heart function [6]. Our report shows that ECLS was an effective modality for repetitive life-threatening arrhythmia due to aconite poisoning. We believe that ECPR is a viable alternative to traditional cardiopulmonary resuscitation for patients with acute aconite intoxication.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Chan TY. Aconitum alkaloid poisoning because of contamination of herbs by aconite roots. Phytother Res. 2016;30:3–8. doi: 10.1002/ptr.5495. [DOI] [PubMed] [Google Scholar]
- 2.Chan TY, Tomlinson B, Tse LK, Chan JC, Chan WW, Critchley JA. Aconitine poisoning due to Chinese herbal medicines: a review. Vet Hum Toxicol. 1994;36:452–5. [PubMed] [Google Scholar]
- 3.Chen X, Wu R, Jin H, Gao R, Yang B, Wang Q. Successful rescue of a patient with acute aconitine poisoning complicated by polycystic renal hemorrhage. J Nippon Med Sch. 2015;82:257–61. doi: 10.1272/jnms.82.257. [DOI] [PubMed] [Google Scholar]
- 4.Friese J, Gleitz J, Gutser UT, Heubach JF, Matthiesen T, Wilffert B, et al. Aconitum sp. alkaloids: the modulation of voltage-dependent Na+ channels, toxicity and antinociceptive properties. Eur J Pharmacol. 1997;337:165–74. doi: 10.1016/s0014-2999(97)01268-5. [DOI] [PubMed] [Google Scholar]
- 5.Lin CC, Chan TY, Deng JF. Clinical features and management of herb-induced aconitine poisoning. Ann Emerg Med. 2004;43:574–9. doi: 10.1016/j.annemergmed.2003.10.046. [DOI] [PubMed] [Google Scholar]
- 6.de Lange DW, Sikma MA, Meulenbelt J. Extracoporeal membrane oxygenation in the treatment of poisoned patients. Clin Toxicol (Phila) 2013;51:385–93. doi: 10.3109/15563650.2013.800876. [DOI] [PubMed] [Google Scholar]