

Abstract
Introduction
The purpose of our present study was to assess the prognostic impact of FDG PET-CT after induction chemotherapy for patients with inoperable non-small-cell lung cancer (NSCLC).
Material and methods
This retrospective study included 50 patients with inoperable stage II/III NSCLC from January 2012 to July 2015. They were treated for curative intent with induction chemotherapy, followed by concomitant chemoradiation therapy or sequential radiation therapy. FDG PET-CT scans were acquired at initial staging (PET1) and after the last cycle of induction therapy (PET2). Five parameters were evaluated on both scans: SUVmax, SUVpeak, SUVmean, TLG, MTV, and their respective deltas. The prognostic value of each parameter for overall survival (OS) and progression-free survival (PFS) was evaluated with Cox proportional-hazards regression models.
Results
Median follow-up was 19 months. PET1 parameters, clinical and histopathological data were not predictive of the outcome. TLG2 and ΔTLG were prognostic factors for OS. TLG2 was the only prognostic factor for PFS. For OS, log-rank test showed that there was a better prognosis for patients with TLG2< 69g (HR = 7.1, 95%CI 2.8–18, p = 0.002) and for patients with ΔTLG< -81% after induction therapy (HR = 3.8, 95%CI 1.5–9.6, p = 0.02). After 2 years, the survival rate was 89% for the patients with low TLG2 vs 52% for the others. We also evaluated a composite parameter considering both MTV2 and ΔSUVmax. Patients with MTV2> 23cc and ΔSUVmax> -55% had significantly shorter OS than the other patients (HR = 5.7, 95%CI 2.1–15.4, p< 0.01).
Conclusion
Post-induction FDG PET might be an added value to assess the patients’ prognosis in inoperable stage II/III NSCLC. TLG, ΔTLG as well as the association of MTV and ΔSUVmax seemed to be valuable parameters, more accurate than clinical, pathological or pretherapeutic imaging data.
Introduction
Non-small cell lung cancer (NSCLC) is one of the most frequent malignancies in Western countries and represents a leading cause of death by cancer [1]. If surgery is recommended in early stages, it is generally associated with radiation therapy and chemotherapy for patients with locally advanced disease [2]. Patients presenting with inoperable stage II/III NSCLC can benefit from induction chemotherapy before radiation therapy or before concomitant chemoradiation therapy.
Induction chemotherapy allows to start the treatment earlier, while preparing (chemo)-radiation therapy. It causes a reduction of tumoral volume and thus a narrowing of the fields of irradiation, which enables to reduce both volume and dose of radiation of the Organs at Risk (OAR), and to assess tumoral chemosensitivity of the primary tumor and nodal metastases.
Over the past few years, FDG PET-CT has proven its use for diagnosing [3], staging, evaluating tumor response [4] and has shown its potential as a prognostic imaging biomarker in lung cancer. Several studies have shown the prognostic implications of changes in standardized uptake value (SUV) and suggested that FDG PET-CT could predict the response to chemoradiation [5,6], induction chemotherapy [7] and radiation therapy alone [8,9]. A meta-analysis revealed that high tumoral uptake at staging could result in a worse prognosis, especially in early stages [10]. However, metabolic parameters in patients with NSCLC after induction therapy lead to controversial results in terms of prognostic evaluation [11,12]. Volume-based indices were useful for predicting therapy response after induction chemotherapy, however, that study concerned a majority of patients who underwent curative intent surgery [13]. The purpose of our present study is to assess the prognostic impact of FDG PET-CT after induction chemotherapy for patients with inoperable NSCLC.
Material & methods
Population and treatment
This retrospective study, approved by the institutional review board (approval number 1708B), included 50 patients from January 2012 to July 2015. Thirty-five of these patients were followed at the Henri Becquerel Cancer Centre whereas 15 of them were followed in other centres for a multi-centre trial (initiated by the Henri Becquerel Cancer Centre) in which patients with hypoxic tumoral areas could benefit from dose escalation radiotherapy (RTEP-5 NCT01576796)[14]. All these 50 patients’ clinical and imaging data were available and searchable in our centre. Patients provided written informed consent for their data and scans to be published anonymously.
Patients with inoperable stage II or III NSCLC, according to the 7th edition of the International Union Against Cancer staging system, treated for curative intent with induction chemotherapy, followed by concomitant chemo-radiation therapy or sequential radiation therapy, were included. The 15 patients from the RTEP-5 study were included regardless of the hypoxic status of their tumor.
Patients who would have surgery after induction chemotherapy or presenting with metastases—at initial staging or after induction chemotherapy—were excluded.
Induction therapy consisted in 1 to 6 cycles of platinum-based chemotherapy. The following radiation therapy delivered 66 to 70 Gy in 33 to 35 daily fractions of 2 Gy, associated or not to concomitant chemotherapy.
All patients underwent FDG PET-CT scans at initial staging and before radiation therapy.
PET-CT imaging
FDG PET-CT scans were acquired at initial staging (PET1) and between the end of the last cycle of induction therapy and the beginning of (chemo-) radiation therapy (PET2). For the 35 patients treated in Rouen, PET-CT scans were performed on a Biograph Sensation 16 Hi-Rez device (Siemens Medical Solutions, Erlangen, Germany, 29 patients), GE 710 (GE, 5 patients) and mCT 40 (Siemens, 1 patient). For the 15 remaining patients from the multi-centre trial, PET-CT scans were acquired on Gemini GXL (Philips, 2 patients), Biograph mCT 40 (Siemens, 5 patients), Biograph mCT (Siemens, 1 patient), Discovery ST (GE, 1 patient), Gemini TOF (Philips, 3 patients), Discovery ST 4 (GE, 1 patient), GE 690 (GE, 1 patient) and Biograph (Siemens, 1 patient). Patients were asked to fast for at least 6 hours before the time of 18F-FDG administration to ensure that the serum glucose and serum insulin levels were low. An activity of 3.5 to 5 MBq/kg of 18F-FDG was injected after 20 minutes of rest. Sixty minutes later (±10 min), the acquisition began with non-injected CT in the cephalocaudal direction. The images were acquired with the patients’ arms positioned over the head while breathing freely. The PET data were then acquired in the caudocephalic direction using a whole-body protocol (3 min per bed position). The delay between injection and acquisition was standardized to 60 minutes in order to obtain a normalized counting rate for all patients. Protocols of acquisition and reconstruction were inherent to each nuclear medicine department and the same for a given device. They followed EANM procedure guidelines [15].
PET-CT analysis
PET1 and PET2 were analysed using a Planet Onco workstation (PlanetOnco, v.2.0; DOSISoft®). All lesions (primary tumor and involved lymph nodes) with significant uptake were considered, which allowed to determine 5 main parameters: SUVmax, SUVmean, SUVpeak (defined as the average SUV within a 1 cc spherical region of interest centred on a high uptake part of the tumor), metabolic tumor volume (MTV) using a 41% of SUVmax threshold and total lesion glycolysis (TLG), defined as the product of MTV by SUVmean. The response to induction therapy was assessed by calculating the deltas for each parameter, with:
In addition, CT data were also analysed with Telemis-Medical PACS interface (TM v.2.70) by measuring the summed lesions diameter as used in RECIST 1.1 [4].
Patients follow-up and statistical analysis
The follow-up consisted in routine clinical evaluation and systematic imaging revaluation (FDG PET-CT or CT) at 3 and 12 months after the end of treatment, and then periodically. The follow-up duration was the time between the end of radiation therapy and the last day of clinical or imaging evaluation, or the date of death.
Time to progression was defined as the time between the end of radiation therapy and the date of local or metastatic recurrence assessed through any imaging modality.
Clinical data, such as performance status, age and weight loss, as well as histological subtypes and tumoral stage were collected. Statistical analyses were realized with MedCalc software. Predictive factors for overall survival (OS) and progression free survival (PFS) were analysed using univariate and multivariate analyses. Receiver operator characteristics curves were used to determine a cut-off value for parameters whose p-value was less than 0.05 in multivariate analysis. OS and PFS were graphically represented using the Kaplan-Meier method. A log-rank test was used to compare groups for each independent factor and a p-value< 0.05 was considered as a statistically significant difference.
Results
Clinical data are summarized in Table 1.
Table 1. Population characteristics.
| Patients | 50 |
|---|---|
| Age (years) | Mean : 63 (+/-9) Range : 37–84 |
| Sex: | Number of patients |
| - M - F |
44 6 |
| Histology: | Number of patients |
| - Adenocarcinoma - Squamous cell carcinoma |
28 22 |
| Tumoral stage: | Number of patients |
| - IIA, IIB, IIIA - IIIB |
23 27 |
| Induction chemotherapy (1 to 6 cycles): | Number of patients (N) |
| - Platinum salt + Pemetrexed - Platinum salt + Gemcitabin - Platinum salt + Vinorelbin - Platinum salt + Taxanes |
17 3 18 12 |
| Post- induction treatment: | N |
| - Concomitant chemoradiation therapy - Radiation therapy |
37 13 |
| Follow-up (months) | Mean (+/- S.D.) : 21 (+/-11) Median : 19 Range : 2–45 |
| Events: | N |
| - Relapse - Death |
33 18 |
Fifty patients (44 men and 6 women) with a mean age of 63 years (+/- 9) were included in our study. Median follow-up was 19 months.
Twenty-eight (56%) of lung cancers were adenocarcinomas and 22 (44%) were squamous cell carcinomas.
Twenty-three cancers were staged as IIA, IIB or IIIA (46%) and 27 were staged as IIIB according to the UICC 7th edition of TNM classification of malignant tumors (2009).
Induction therapy consisted in 1 to 6 cycles chemotherapy associating platinum salts to vinorelbin (36%), pemetrexed (34%), taxanes (24%) or gemcitabin (6%).
After induction chemotherapy, 37 patients (74%) were treated with concomitant radiochemotherapy and 13 with radiation therapy alone. Patients undergoing radiation therapy alone had more cycles of induction therapy than patients treated with concomitant chemoradiation (4.0 vs 2.3, p< 0.001).
During the follow-up duration, 66% of our population showed local or metastatic relapse and 18 patients (36%) died, mainly from disease progression or toxicities of therapy.
Fig 1 illustrates the changes between PET1 and PET2.
Fig 1. Tumoral response.

66-year-old patient with T2N2 (Stage IIIA) left upper lobe squamous cell carcinoma. At baseline (a), tumor SUVmax was 12 g/ml, MTV 13 cc and TLG 89 g. After 2 cycles of carboplatin-paclitaxel (b), SUVmax was 8.2 g/ml (ΔSUVmax = -33%), MTV 2.4 cc (ΔMTV = -82%) and TLG 11.3 g (ΔTLG = -87%). After 45 months, the patient was still alive and showed no sign of recurrence.
In univariate analysis, none of the following parameters was significant to predict the outcome of the population: performance status (p = 0.2), age (p = 0.38), histologic subtype (p = 0.86), pre-radiation weight loss (p = 0.07), the number of cycles of induction chemotherapy (p = 0.58), the association of concomitant chemotherapy during radiation (p = 0.85) or a locally advanced (IIIB) disease (p = 0.11).
Furthermore, lesion diameters used in RECIST 1.1 were measured using CT data to assess the response to the induction therapy. Twenty-six patients had a stable disease (52%), 23 showed a partial response (46%) and the remaining patient (2%) had a progressive disease. There was no statistically significant correlation between the response to induction chemotherapy and the outcome (for PFS: p = 0.08, for OS: p = 0.07).
Table 2 details information for each parameter of interest in PET1 and PET2, and the response to treatment with the delta of each parameter. Many parameters, mainly extracted from PET2 data, were significant to predict OS or PFS in univariate analysis. However, when considering overall survival, no parameter extracted from PET1 data was significant.
Table 2. PET data and univariate analysis.
| Mean (+/- Standard Deviation) | Median | Range | PFS | OS | |
|---|---|---|---|---|---|
| PET1 | |||||
| SUVmax1 | 16 (+/-8) | 14 | 4–50 | p = 0.52 | p = 0.79 |
| SUVmean1 | 8 (+/-5) | 7 | 2–31 | p = 0.39 | p = 0.54 |
| SUVpeak1 | 14 (+/-7) | 11 | 3–47 | p = 0.53 | p = 0.79 |
| MTV1 | 73 (+/-65) | 54 | 5–333 | p = 0.0004 | p = 0.75 |
| TLG1 | 613 (+/-643) | 399 | 28–3216 | p = 0.02 | p = 0.55 |
| PET2 | |||||
| SUVmax2 | 9 (+/-9) | 8 | 2–50 | p = 0.31 | p = 0.004 |
| SUVmean2 | 5 (+/-5) | 3 | 1–31 | p = 0.46 | p = 0.01 |
| SUVpeak2 | 7 (+/-8) | 6 | 0–47 | p = 0.28 | p = 0.001 |
| MTV2 | 30 (+/- 28) | 22 | 2–140 | p = 0.056 | p = 0.03 |
| TLG2 | 160 (+/- 294) | 75 | 3–1967 | p = 0.02 | p< 0.001 |
| Response | |||||
| ΔSUVmax | -40% (+/- 31%) | -43% | -93%−+26% | p = 0.41 | p< 0.001 |
| ΔSUVmean | -43% (+/-30%) | -48% | -93%−+18% | p = 0.87 | p = 0.04 |
| ΔSUVpeak | -45% (+/- 31%) | -48% | -100%−+19% | p = 0.27 | p< 0.001 |
| ΔMTV | -45% (+/- 48%) | -54% | -94%−+164% | p = 0.85 | p = 0.052 |
| ΔTLG | -67% (+/- 36%) | -76% | -99%−+106% | p = 0.36 | p = 0.001 |
| Δ Σ lesion diameters | -28% (+/-22%) | -26% | -72%−+37% | p = 0.08 | p = 0.07 |
In multivariate analysis (see Table 3), only TLG2 was an independent parameter for PFS, and both TLG2 and ΔTLG were independent factors for OS.
Table 3. Multivariate analysis.
| PFS | OS | Cut-off value | Sensitivity | Specificity | AUC | |
|---|---|---|---|---|---|---|
| TLG1 | p = 0.90 | |||||
| MTV1 | p = 0.06 | |||||
| SUVmax2 | p = 0.25 | |||||
| SUVmean2 | p = 0.42 | |||||
| SUVpeak2 | p = 0.15 | |||||
| MTV2 | p = 0.09 | |||||
| TLG2 | p = 0.02 | p = 0.02 | PFS: 97g OS: 69g |
51.5% 88.9% |
82.4% 59.4% |
0.688 0.766 |
| ΔSUVmax | p = 0.27 | |||||
| ΔSUVmean | p = 0.63 | |||||
| ΔSUVpeak | p = 0.84 | |||||
| ΔTLG | p = 0.03 | -81% | 83% | 56% | 0.736 | |
| Composite parameter | p = 0.01 | MTV2 < 23 cc or ΔSUVmax < -55% VS MTV2 > 23 cc and ΔSUVmax > -55% |
72% | 81% | 0.771 |
Another parameter was analyzed: a composite considering both ΔSUVmax and MTV2 to isolate a subgroup of bad responders with low ΔSUVmax and high MTV2. P-values for this composite parameter were inferior to 0.05 in uni- and multivariate analysis, when considering overall survival. ROC curves analyses determined a threshold for each statistically significant parameter in order to separate the population into two groups.
When considering PFS, TLG2 was the only independent predictive parameter with a cut-off value of 97 g. A log-rank test revealed that there was a better prognosis for the 30 patients with low TLG2 (HR = 2.8, 95%CI 1.3–5.9, p = 0.002). After 12 months, 97% of the patients with low TLG2 showed no relapse versus 56% in the group of 20 patients with high TLG2. After 24 months, they were respectively 67% in the first group vs 34% in the second one.
For OS, ROC curves showed cut-off values of -81% for ΔTLG and 69 g for TLG2. A log-rank test showed that there was a better prognosis for patients with low TLG2 (HR = 7.1, 95%CI 2.8–18, p = 0.002) and for patients with a high decrease of TLG after induction therapy (HR = 3.8, 95%CI 1.5–9.6, p = 0.02). After 12 months, 91% of the 21 patients with high decrease of TLG were alive versus 76% of the remaining 29 patients, and 89% of the patients with low TLG2 survived versus 52% for the patients with high TLG2. Survival curves using the Kaplan-Meier method are represented in Fig 2.
Fig 2. FDG PET parameters and survival curves.
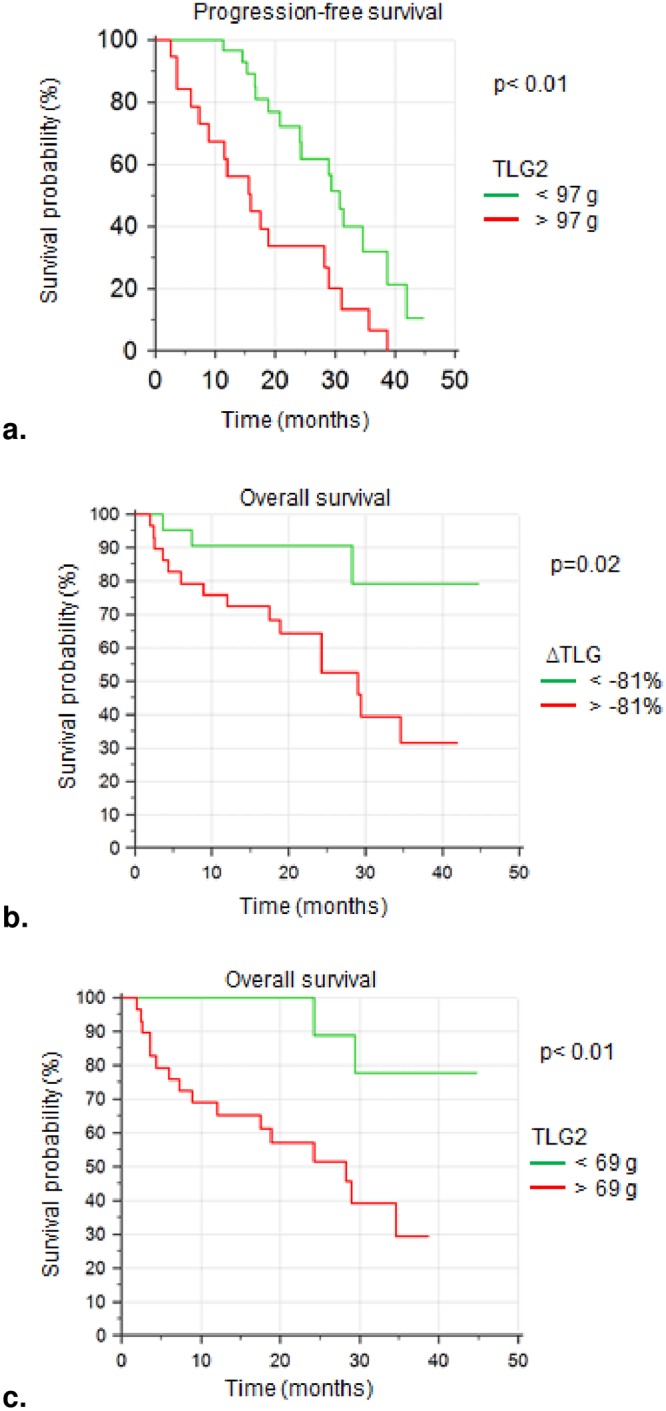
Survival curves using the Kaplan-Meier method. (a) PFS was longer for patients with low TLG2 (HR = 2.8, 95%CI 1.3–5.9, p< 0.01). After 2 years, the survival rate was 67% for the 30 patients with low TLG2 vs 34% for the 20 others. Median survival was respectively reached at 31 and 16 months. (b) 21 patients with high decrease of TLG after therapy (ΔTLG < -81%) showed longer OS (HR = 3.8, 95%CI 1.5–9.6, p = 0.02). After 1 year and after 2 years, survival rates for the 21 good responders were 91% versus 76% and 59% for the 29 bad responders. Median survival was not reached for good responders and was 29 months for the others. (c) Survival curves showed longer OS for patients with low TLG2 (HR = 7.1, 95%CI 2.8–18, p< 0.01). After 2 years, the survival rate was 89% for the 21 patients with low TLG2 (median survival not reached) vs 52% for the other 29 patients (median survival at 28 months).
We also used a composite parameter considering both ΔSUVmax and MTV2. Using the ROC curves, we determined a cut-off value for ΔSUVmax (-55%) and for MTV2 (23 cc). We were then able to isolate a subgroup of 19 patients with high MTV2 and low decrease of SUV after induction chemotherapy. When we compared the OS for this subgroup (Group B) to the OS of the 31 remaining patients (Group A), the log-rank test showed that OS was significantly longer for Group A vs Group B (HR = 5.7, 2.1–15.4, p< 0.001). After 12 months, survival rates were 97% for Group A vs 53% for Group B. After 24 months, they were 89% for Group A vs 41% for Group B (Fig 3).
Fig 3. Overall survival using the composite parameter.

Group A: 31 patients with low MTV2 or high decrease of SUVmax after induction therapy. Group B: 19 patients with high MTV2 (> 23 cc) and low decrease of SUVmax (ΔSUVmax> -55%). Median survival was not reached in Group A and was 17.5 months in Group B. HR = 5.7, 95%CI 2.1–15.4, p< 0.001.
Discussion
We have shown that post-induction PET (PET2) could be an added value to assess the patients’ prognosis in inoperable stage II/III NSCLC. First, it allows the evaluation of response to induction chemotherapy, informs about the tumor chemosensitivity and about the estimation of the prognosis, thanks to the ΔTLG. Then, it seems that post-induction TLG (TLG2) is predictive of the outcome independently from pretherapeutic data.
In our study, data extracted from PET2 appeared to be more accurate than RECIST criteria or than clinical and histopathological data to assess the patients’ outcome.
We did not isolate any metabolic or volumetric parameter issued from pretherapeutic FDG PET (PET1) as a predictive factor for survival, in opposition to what is commonly found when reviewing the literature [10, 16–19]. Even though a few studies did not find any correlation between baseline uptake and survival [20], our hypothesis to explain these surprising results might be that our study considered a limited series of patients and could lack of power to show significant association between PET1 data and the population’s outcome. In that case, we can only assume that the parameters obtained with PET2 might predict the outcome with more reliability than those obtained with PET1. Of course, this should be studied in a prospective study with a larger cohort of patients.
The current standard for patients with locally advanced NSCLC includes a baseline FDG PET-CT followed by induction chemotherapy. A CT acquisition is then realized in position of treatment to prepare the radiotherapy which is to follow, concomitant or not to chemotherapy. Yet, this procedure only enables an assessment of morphologic tumor response, whereas PET-CT can determine both anatomic and metabolic tumor responses.
A recently published study showed that an early metabolic response using PERCIST 1.0 or EORTC criteria was more sensitive and accurate than with RECIST 1.1 criteria [21]. In addition, FDG PET may reveal and locate metastatic lesions, and identify patients with progressive disease. For instance, a phase II trial proposing dose escalation radiotherapy to 18F-MISO positive lesions in patients with NSCLC (RTEP-5 NCT01576796) showed that 9/79 patients (11%) were excluded because of metastatic progression on post-induction FDG PET [14]. These findings were also highlighted in one of the studies evaluating FDG PET after induction therapy, with 17% of patients with metastatic evolution after neoadjuvant therapy [22].
In addition to re-staging the disease and avoiding useless and potentially harmful treatment, PET2 could identify a population at high risk of relapse using prognostic parameters.
Among the tools assessed in our study, the composite parameter seems to be interesting to predict the outcome by isolating a subgroup of patients with the highest risk of progression.
Ho Yun Lee and S. M. Eschmann studies have used ΔSUVmax to distinguish between good responders to induction chemotherapy from bad responders [23,24]. In our study, the cut-off value for ΔSUVmax was -55%, in coherence to what was determined in those two studies (-50% and -60%, respectively).
Furthermore, post-induction volumetric indices were found to be prognostic tools regarding survival [13] or pathological response [25].
Once combined, ΔSUVmax and MTV2 became a significant tool in the multivariate analysis when considering overall survival. However, the use of this hybrid parameter has to be confirmed in a prospective or a cohort study.
A recently published study showed that ΔSUVmax was also an interesting parameter as well as ΔMTV, between baseline PET and interim PET after induction chemotherapy, to predict complete response after concurrent chemo-radiation therapy in patients with head and neck cancer [26].
Even though our results seem promising, our study suffers from a few limitations.
We retrospectively included patients who had benefited from curative-intent radiotherapy and undergone post-induction chemotherapy FDG PET. That limited the number of patients in our study since we did not include all the patients with inoperable NSCLC who had undergone neo-adjuvant chemotherapy. These facts have certainly impacted on the statistical power, which may have reduced the significance of other potential prognostic parameters. Moreover, we are not able to determine the amount of patients with progressive disease, since metastatic evolution or a too large tumor generally contra-indicate radiation therapy.
In addition, this retrospective recruitment lead to heterogeneity in induction chemotherapy, in both quantitative and qualitative aspects. However, the number of cycles of induction chemotherapy had no significant impact on the deltas (ΔSUVmax, ΔTLG, ΔSUVpeak, ΔSUVmean) or on the outcome.
Also, even though we did show that a locally advance disease (stage III B) was not a significant parameter to predict the outcome, we did not study if the involvement of lymph nodes was a valuable parameter to assess the patients’ prognosis because, since they had all been treated by induction chemotherapy because of an important tumoral mass, only four of them (8%) were N0 according to the TNM classification.
If a large prospective study confirmed the reliability of PET2 to identify a population at risk, we could imagine a change of treatment with a more personalized approach for these particular patients.
Several clinical trials are in process to evaluate the feasibility and the impact of adaptive therapy in NSCLC. For example, hypoxic lesions are known to be radio-resistant. Thus, escalation dose radiotherapy could be considered for these patients, in order to improve their survival. A phase II study of total dose increase in hypoxic lesions showed that dose escalation was feasible [14]. A survival analysis must then be conducted in a phase III clinical trial.
Furthermore, persistence of hypermetabolism in NSCLC during radiation therapy is highly predictive of relapse [27]. Currently ongoing trials study the impact on survival of escalation dose radiotherapy in these patients (RTEP7 NCT02473133, NCT01507428) [28,29].
Bad responders to chemotherapy could benefit from a switch to another line of chemotherapy as showed in a clinical trial of neoadjuvant chemotherapy [30]. Or, an alternative treatment associated to radiotherapy, such as immunotherapy [31,32], could be considered. Indeed, abscopal responses have been reported by physicians treating patients with non-small-cell lung cancer with ipilimumab combined with radiation [33].
The benefit of immunotherapy, such as anti-PD1 or anti-PD-L1 antibodies, in NSCLC will be assessed in ongoing or in future studies (NCT02768558, NCT0257843) [34,35]. In addition, a phase I trial has already evaluated the safety and tolerability of an immunocytokin (Selectikine) associated to radiotherapy [36].
The fact that PET2 potentially identified a subgroup of patients at high risk of relapse might lead to therapeutic prospective studies to improve their prognosis.
Conclusion
Post-induction FDG PET might be an added value to assess the patients’ prognosis in inoperable stage II/III NSCLC. TLG and ΔTLG seemed to be valuable parameters and more accurate than clinical, pathological or pretherapeutic imaging data.
Moreover, the combination of volumetric and metabolic changes using a composite parameter (associating post-induction MTV and ΔSUVmax) seems to be an interesting tool to identify the patients with the highest risk of relapse after radiation therapy.
Supporting information
(XLSX)
Data Availability
All relevant data are within the manuscript and Supporting Information files.
Funding Statement
The authors received no specific funding for this work.
References
- 1.Boyle P, Ferlay J. Cancer Incidence and Mortality in Europe, 2004. Ann Oncol. 2005;16(3):481–8. 10.1093/annonc/mdi098 [DOI] [PubMed] [Google Scholar]
- 2.Farray D, Mirkovic N, Albain KS, Multimodality Therapy for Stage III Non-Small-Cell Lung Cancer. J Clin Oncol. 2005;23(14):3257–69. 10.1200/JCO.2005.03.008 [DOI] [PubMed] [Google Scholar]
- 3.Jerusalem G, Hustinx R, Beguin Y, Fillet G.The Value of Positron Emission Tomography (PET) Imaging in Disease Staging and Therapy Assessment. Ann Oncol. 2002;13 Suppl 4:227–34. [DOI] [PubMed] [Google Scholar]
- 4.Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors. J Nucl Med. 2009;50 Suppl 1:122S–50S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Calais J, Thureau S, Dubray B, Modzelewski R, Thiberville L, Gardin I, et al. Areas of High 18F-FDG Uptake on Preradiotherapy PET/CT Identify Preferential Sites of Local Relapse after Chemoradiotherapy for Non-Small Cell Lung Cancer. J Nucl Med. 2015;56(2):196–203. 10.2967/jnumed.114.144253 [DOI] [PubMed] [Google Scholar]
- 6.Machtay M, Duan F, Siegel BA, Snyder BS, Gorelick JJ, Reddin JS, et al. Prediction of Survival by [18F]fluorodeoxyglucose Positron Emission Tomography in Patients with Locally Advanced Non-Small-Cell Lung Cancer Undergoing Definitive Chemoradiation Therapy: Results of the ACRIN 6668/RTOG 0235 Trial. J Clin Oncol. 2013;31(30):3823–30. 10.1200/JCO.2012.47.5947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abramyuk A, Tokalov S, Zöphel K, Koch A, Szluha Lazanyi K, Gillham C, et al. Is Pre-Therapeutical FDG-PET/CT Capable to Detect High Risk Tumor Subvolumes Responsible for Local Failure in Non-Small Cell Lung Cancer?. Radiother Oncol. 2009;91(3):399–404. 10.1016/j.radonc.2009.01.003 [DOI] [PubMed] [Google Scholar]
- 8.Na F, Wang J, Li C, Deng L, Xue J, Lu Y.Primary Tumor Standardized Uptake Value Measured on F18-Fluorodeoxyglucose Positron Emission Tomography Is of Prediction Value for Survival and Local Control in Non-Small-Cell Lung Cancer Receiving Radiotherapy: Meta-Analysis. J Thorac Oncol. 2014;9(6):834–42. 10.1097/JTO.0000000000000185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Borst GR, Belderbos JS, Boellaard R, Comans EF, De Jaeger K, Lammertsma AA, et al. Standardised FDG Uptake: A Prognostic Factor for Inoperable Non-Small Cell Lung Cancer. Eur J Cancer. 2005;41(11):1533–41. 10.1016/j.ejca.2005.03.026 [DOI] [PubMed] [Google Scholar]
- 10.Paesmans M, Berghmans T, Dusart M, Garcia C, Hossein-Foucher C, Lafitte JJ, et al. Primary Tumor Standardized Uptake Value Measured on Fluorodeoxyglucose Positron Emission Tomography Is of Prognostic Value for Survival in Non-Small Cell Lung Cancer: Update of a Systematic Review and Meta-Analysis by the European Lung Cancer Working Party for the International Association for the Study of Lung Cancer Staging Project. J Thorac Oncol. 2010;5(5):612–9. 10.1097/JTO.0b013e3181d0a4f5 [DOI] [PubMed] [Google Scholar]
- 11.Dooms C, Verbeken E, Stroobants S, Nackaerts K, De Leyn P, Vansteenkiste J. Prognostic Stratification of Stage IIIA-N2 Non-Small-Cell Lung Cancer after Induction Chemotherapy: A Model Based on the Combination of Morphometric-Pathologic Response in Mediastinal Nodes and Primary Tumor Response on Serial 18-Fluoro-2-Deoxy-Glucose Positron Emission Tomography. J Clin Oncol. 2008;26(7):1128–34. 10.1200/JCO.2007.13.9550 [DOI] [PubMed] [Google Scholar]
- 12.Tanvetyanon T, Eikman EA, Sommers E, Robinson L, Boulware D, Bepler G. Computed Tomography Response, but Not Positron Emission Tomography Scan Response, Predicts Survival after Neoadjuvant Chemotherapy for Resectable Non-Small-Cell Lung Cancer. J Clin Oncol. 2008;26(28):4610–6. 10.1200/JCO.2008.16.9383 [DOI] [PubMed] [Google Scholar]
- 13.Soussan M, Chouahnia K, Maisonobe JA, Boubaya M, Eder V, Morère JF, et al. Prognostic Implications of Volume-Based Measurements on FDG PET/CT in Stage III Non-Small-Cell Lung Cancer after Induction Chemotherapy. Eur J Nucl Med Mol Imaging. 2013;40(5):668–76. 10.1007/s00259-012-2321-7 [DOI] [PubMed] [Google Scholar]
- 14.Vera P, Thureau S, Chaumet-Riffaud P, Modzelewski R, Bohn P, Vermandel M, et al. Phase II Study of a Radiotherapy Total Dose Increase in Hypoxic Lesions Identified by F-Miso PET/CT in Patients with Non-Small Cell Lung Carcinoma (RTEP5 Study). J Nucl Med. 2017;58(7):1045–1053. 10.2967/jnumed.116.188367 [DOI] [PubMed] [Google Scholar]
- 15.Boellaard R, Delgado-Bolton R, Oyen WJ, Giammarile F, Tatsch K, Eschner W, et al. FDG PET/CT: EANM Procedure Guidelines for Tumour Imaging: Version 2.0. Eur J Nucl Med Mol Imaging. 2015;42(2):328–54. 10.1007/s00259-014-2961-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Berghmans T, Dusart M, Paesmans M, Hossein-Foucher C, Buvat I, Castaigne C, et al. Primary Tumor Standardized Uptake Value (SUVmax) Measured on Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) Is of Prognostic Value for Survival in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review and Meta-Analysis (MA) by the European Lung Cancer Working Party for the IASLC Lung Cancer Staging Project. J Thorac Oncol. 2008;3(1):6–12. 10.1097/JTO.0b013e31815e6d6b [DOI] [PubMed] [Google Scholar]
- 17.Hyun SH, Ahn HK, Ahn MJ, Ahn YC, Kim J, Shim YM, et al. Volume-Based Assessment With 18F-FDG PET/CT Improves Outcome Prediction for Patients With Stage IIIA-N2 Non-Small Cell Lung Cancer. AJR Am J Roentgenol. 2015;205(3):623–8. 10.2214/AJR.14.13847 [DOI] [PubMed] [Google Scholar]
- 18.Chen HH, Chiu NT, Su WC, Guo HR, Lee BF. Prognostic Value of Whole-Body Total Lesion Glycolysis at Pretreatment FDG PET/CT in Non-Small Cell Lung Cancer. Radiology. 2012;264(2):559–66. 10.1148/radiol.12111148 [DOI] [PubMed] [Google Scholar]
- 19.Im HJ, Pak K, Cheon GJ, Kang KW, Kim IJ, Chung JK, et al. Prognostic Value of Volumetric Parameters of (18)F-FDG PET in Non-Small-Cell Lung Cancer: A Meta-Analysis. Eur J Nucl Med Mol Imaging. 2015. February;42(2):241–51. 10.1007/s00259-014-2903-7 [DOI] [PubMed] [Google Scholar]
- 20.Hoang JK, Hoagland LF, Coleman RE, Coan AD, Herndon JE 2nd, Patz EF Jr. Prognostic Value of Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography Imaging in Patients with Advanced-Stage Non-Small-Cell Lung Carcinoma. J Clin Oncol. 2008;26(9):1459–64. 10.1200/JCO.2007.14.3628 [DOI] [PubMed] [Google Scholar]
- 21.Shang J, Ling X, Zhang L, Tang Y, Xiao Z, Cheng Y, et al. Comparison of RECIST, EORTC Criteria and PERCIST for Evaluation of Early Response to Chemotherapy in Patients with Non-Small-Cell Lung Cancer. Eur J Nucl Med Mol Imaging. 2016;43(11):1945–53. 10.1007/s00259-016-3420-7 [DOI] [PubMed] [Google Scholar]
- 22.Hellwig D, Graeter TP, Ukena D, Georg T, Kirsch CM, Schäfers HJ. Value of F-18-Fluorodeoxyglucose Positron Emission Tomography after Induction Therapy of Locally Advanced Bronchogenic Carcinoma. J Thorac Cardiovasc Surg. 2004;128(6):892–9. 10.1016/j.jtcvs.2004.07.031 [DOI] [PubMed] [Google Scholar]
- 23.Lee HY, Lee HJ, Kim YT, Kang CH, Jang BG, Chung DH, et al. Value of Combined Interpretation of Computed Tomography Response and Positron Emission Tomography Response for Prediction of Prognosis after Neoadjuvant Chemotherapy in Non-Small Cell Lung Cancer. J Thorac Oncol. 2010;5(4):497–503. 10.1097/JTO.0b013e3181d2efe7 [DOI] [PubMed] [Google Scholar]
- 24.Eschmann SM, Friedel G, Paulsen F, Reimold M, Hehr T, Dittmann H, et al. Repeat 18F-FDG PET for Monitoring Neoadjuvant Chemotherapy in Patients with Stage III Non-Small Cell Lung Cancer. Lung Cancer. 2007; 55(2):165–71. 10.1016/j.lungcan.2006.09.028 [DOI] [PubMed] [Google Scholar]
- 25.Soussan M, Cyrta J, Pouliquen C, Chouahnia K, Orlhac F, Martinod E, et al. Fluorine 18 Fluorodeoxyglucose PET/CT Volume-Based Indices in Locally Advanced Non-Small Cell Lung Cancer: Prediction of Residual Viable Tumor after Induction Chemotherapy. Radiology. 2014;272(3):875–84. 10.1148/radiol.14132191 [DOI] [PubMed] [Google Scholar]
- 26.Kim KR, Shim HJ, Hwang JE, Cho SH, Chung IJ, Park KS, et al. The Role of Interim FDG PET-CT after Induction Chemotherapy as a Predictor of Concurrent Chemoradiotherapy Efficacy and Prognosis for Head and Neck Cancer. Eur J Nucl Med Mol Imaging. 2017. September 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vera P, Mezzani-Saillard S, Edet-Sanson A, Ménard JF, Modzelewski R, Thureau S, et al. FDG PET during Radiochemotherapy Is Predictive of Outcome at 1 Year in Non-Small-Cell Lung Cancer Patients: A Prospective Multicentre Study (RTEP2). Eur J Nucl Med Mol Imaging. 2014;41(6):1057–65. 10.1007/s00259-014-2687-9 [DOI] [PubMed] [Google Scholar]
- 28.Study of Interest of Personalized Radiotherapy Dose Redistribution in Patients With Stage III NSCLC—ClinicalTrials.gov
- 29.Study of Positron Emission Tomography and Computed Tomography in Guiding Radiation Therapy in Patients With Stage III Non-Small Cell Lung Cancer—ClinicalTrials.gov
- 30.Chaft JE, Dunphy M, Naidoo J, Travis WD, Hellmann M, Woo K, et al. Adaptive Neoadjuvant Chemotherapy Guided by (18)F-FDG PET in Resectable Non-Small Cell Lung Cancers: The NEOSCAN Trial. J Thorac Oncol. 2016. April;11(4):537–44. 10.1016/j.jtho.2015.12.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Seyedin SN, Schoenhals JE, Lee DA, Cortez MA, Wang X, Niknam S, et al. Strategies for Combining Immunotherapy with Radiation for Anticancer Therapy. Immunotherapy. 2015;7(9):967–980. 10.2217/imt.15.65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tang C, Wang X, Soh H, Seyedin S, Cortez MA Krishnan S, et al. Combining Radiation and Immunotherapy: A New Systemic Therapy for Solid Tumors? Cancer Immunol Res. 2014;2(9):831–8 10.1158/2326-6066.CIR-14-0069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Golden EB, Demaria S, Schiff PB, Chachoua A, Formenti SC.An Abscopal Response to Radiation and Ipilimumab in a Patient with Metastatic Non-Small Cell Lung Cancer. Cancer Immunol Res. 2013;1(6):365–72. 10.1158/2326-6066.CIR-13-0115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cisplatin and Etoposide Plus Radiation Followed By Nivolumab/Placebo For Locally Advanced NSCLC—ClinicalTrials.gov
- 35.Anti-PD-L1 in Stage IIIA(N2) NSCLC—ClinicalTrials.gov
- 36.van den Heuvel MM, Verheij M, Boshuizen R, Belderbos J, Dingemans AM, De Ruysscher D, et al. NHS-IL2 Combined with Radiotherapy: Preclinical Rationale and Phase Ib Trial Results in Metastatic Non-Small Cell Lung Cancer Following First-Line Chemotherapy J Transl Med. 2015;13:32 10.1186/s12967-015-0397-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(XLSX)
Data Availability Statement
All relevant data are within the manuscript and Supporting Information files.