

Abstract
Purpose:
Cancer contributes substantially to the life expectancy gap between US Blacks and Whites, and racial cancer disparities remain stubborn to eradicate. Disparities vary geographically, suggesting that they are not inevitable.
Methods:
We examined the relationship between housing discrimination and the size of cancer disparities across large US metropolitan statistical areas (MSAs). We measured MSA level cancer disparities using Centers for Disease Control data. We estimated mortgage discrimination for each MSA using the Home Mortgage Disclosure Act database, and MSA racial segregation using US Census data. We mapped patterns of housing discrimination and cancer disparities and measured the associations between these place-based factors and cancer disparities across MSAs.
Results:
Black-to-White cancer mortality disparities (rate ratios) vary geographically, ranging from 1.50 to 0.86; 88% of mortality ratios are above 1, indicating higher mortality for Blacks. In areas with greater mortgage discrimination, the gap between Black and White cancer mortality rates is larger (r=0.32, p=0.001). This relationship persists in sex-specific analyses (males: r=0.37, p<0.001, females: r=0.23, p=0.02) and in models controlling for confounders. In contrast, segregation is inconsistently associated with disparities. Adjusting for incidence disparities attenuates, but does not eliminate, the correlation between mortgage discrimination and mortality disparities (r=0.22–0.24), implying that cancer incidence and survival each account for part of the mortality disparity.
Conclusion:
Mortgage discrimination is associated with larger Black-to-White cancer mortality disparities. Some areas are exceptions to this trend. Examination of these exceptions, and policies related to housing discrimination, may offer novel strategies for explaining and eliminating cancer disparities.
Keywords: cancer disparities, cancer mortality, mortgage discrimination, housing discrimination, mortality disparities
Precis for use in the Table of Contents:
We identify structural racism in housing as an important contributor to cancer mortality disparities across the United Sates. Additionally, we find that some of this relationship is explained by disparities in incidence.
INTRODUCTION
Despite decades of research, cancer disparities remain stubborn to eradicate. Between 1990 and 2012, Black to White differential mortality widened for colorectal, breast, and prostate cancer.1 By 2012, Blacks were 2.4 times more likely than Whites to die of prostate cancer, 1.4–1.5 times more likely to die of colorectal cancer, and 1.4 times more likely to die of breast cancer.1 Racial cancer disparities represent a substantial proportion of the overall mortality disparity between Blacks and Whites and are a major consideration in the provision of clinical care and public health practice and policy. In 2010, cancer accounted for 17% of the life expectancy gap between Black and White populations, second only to heart disease for women, and for men, third, also after homicide.2
Racial cancer disparities vary in magnitude geographically.3–5 This variation suggests that disparities are not inevitable and may be in part the product of modifiable place-specific characteristics. Better understanding this geographic variation could lead to new strategies to reduce disparities by, for example, leveraging successful programs or policies from places with small disparities to places where they are larger.
Housing discrimination and other forms of structural racism have been proposed as contributors to racial cancer disparities.6–9 Housing discrimination may limit high quality housing availability to individuals of a given race, and may be a marker for structural racism more broadly, for example, in education or criminal justice.8,10 Housing discrimination can take several forms, including biased mortgage lending, discrimination in renting, and racial segregation. Any of these forms of housing discrimination might account for geographic disparities in cancer mortality via reduced access to quality health care, healthy and affordable food, and safe places for physical activity, as well as increased exposure to environmental hazards.8 Additionally, some have argued that housing discrimination causes greater stress, which itself can lead to lesser emotional wellbeing and adverse biology, such as greater allostatic load.11
Two elements of housing discrimination, mortgage lending bias and racial segregation, can be measured objectively from publicly available databases. The federal Home Mortgage Disclosure Act of 1975 requires transparency in mortgage lending data, including the applicant’s race and income and whether the application was approved or denied. Segregation can be measured from US Census Data. The goal of this study was to determine whether biased mortgage lending and/or segregation were associated with cancer mortality disparities among the 100 largest US metropolitan areas. Given differences in the cancer mix between males and females, we also undertake sex-specific analyses. Models examine identified relationships while controlling for socioeconomic factors to determine whether associations are robust to confounding. Further, as cancer mortality can be influenced by both incidence and survival after diagnosis, we also examined available data for cancer incidence disparities, to isolate the influence of each factor.
METHODS
Data sources
This study examines metropolitan statistical area (MSA) level associations and all measures are constructed at the MSA level. MSAs are areas comprised of an urban core, containing at least 50,000 inhabitants, including a core county as well as surrounding counties. We examined 100 MSAs in this study. Cancer incidence and mortality rates (total, sex-specific, and race-specific) for MSAs across the US were obtained from CDC Wonder for 2009–2013.12 Mortality data originate from death records, as processed by the National Vital Statistics System at the National Center for Health Statistics, and represent deaths for which the underlying cause of death was cancer. Incidence data originate from the CDC National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology and End Results program. Rates are calculated using the US 2000 standard population for age adjustment and are based on the residence of the individual at the time of death (for mortality) or diagnosis (for incidence). Housing discrimination measures were also examined at the MSA level. Mortgage discrimination was measured using the Home Mortgage Disclosure Act database for 2007–2011, and racial segregation measures were derived from US Census Bureau 2010 population data.
Measures
To measure cancer disparities, we computed the mortality rate ratio (MRR) or incidence rate ratio (IRR), dividing the Black age-adjusted rate by the White age-adjusted rate for each MSA. All sites of invasive cancer were included, for the population ages 25 and older. We also explored rates by sex given differences in the cancer mix for males and females.
We employed a recent measure of mortgage discrimination.13 This measure is estimated by calculating the odds of denial of a mortgage application for Black applicants as compared to White applicants in the MSA, using a logistic regression model. We examined two MSA-level measures of segregation for comparison, given the many commonly used measures. The dissimilarity index [range 0 to 1] measures how unevenly a particular racial group (here, Black/African Americans) is distributed over a region (here, MSA), across a set of subunits (here, census tracts) using Census population data. The Black isolation index [range 0–1] indicates the potential of an interaction between members of the same racial group (here, Black), as opposed to members of other racial groups (here, White), again using Census data. For both measures, a higher score indicates a greater level of segregation. MSAs in this study had an average of 470 tracts (min 94, max 4701).
Analysis
We first examined geographic patterns of mortgage discrimination, segregation and cancer disparities. Mortgage discrimination and segregation measures were mapped using a quintile classification system, such that one fifth of MSAs are included in each color category, ranging from high (red) to low (blue). Cancer mortality disparities (rate ratios) were mapped using a similar color scheme, with the break point for the lowest category (blue) adjusted such that it included all ratios of 1 or below, indicating areas where Blacks have an equal or lower mortality rate as compared to Whites. To facilitate comparison between maps of mortality and incidence disparities, additional maps were created using pure quintile break points, so that metropolitan areas can be directly compared across measures based on the group in which they are included. We further explored the distribution of each housing discrimination measure (mortgage discrimination, isolation, dissimilarity) using a series of correlation plots and histograms.
We examined correlations among housing discrimination measures, and between these measures and cancer mortality disparities. Correlations were weighted based on the size of each MSA’s Black population.14 We then estimated a set of models to determine whether the relationship between housing discrimination measures and cancer mortality disparities persisted when controlling for socioeconomic factors and segregation measures. Models were weighted by the size of the Black population, following the approach in correlation analysis. To determine whether relationships between housing discrimination and cancer mortality disparities could be fully or partially explained by incidence disparities, we calculated weighted partial correlations between housing discrimination and cancer mortality disparities, while controlling for cancer incidence disparities.14 Correlations reported used original variables, but results using log transformed variables do not change conclusions and result in only minor numerical differences. Statistical analyses were completed in SAS 9.415 and Stata SE 1516 and mapping was undertaken in Esri ArcMap 10.6.1.17 This study was conducted in accordance with local IRB policies on research exclusively employing public databases.
Role of the funding source
The funding sources were not involved in the design or conduct of the research.
RESULTS
Geographic Variation in Cancer Mortality Disparities and Housing Discrimination
Black-to-White cancer mortality disparities vary substantially across MSAs (Figure 1, panel a). Areas in red have the highest mortality for Blacks compared to Whites; areas in blue have equal or lower mortality for Blacks. The MRRs range from 1.50 in Madison, WI to 0.86 in Scranton, PA. Among all MSAs, 88% have MRRs above 1, indicating higher mortality for Blacks. The areas with MRRs<1 are concentrated in the Northeast, Southwest and Florida.
Figure 1. Geographic variation in structural racism and Black-to-White cancer mortality disparities across US metropolitan areas.
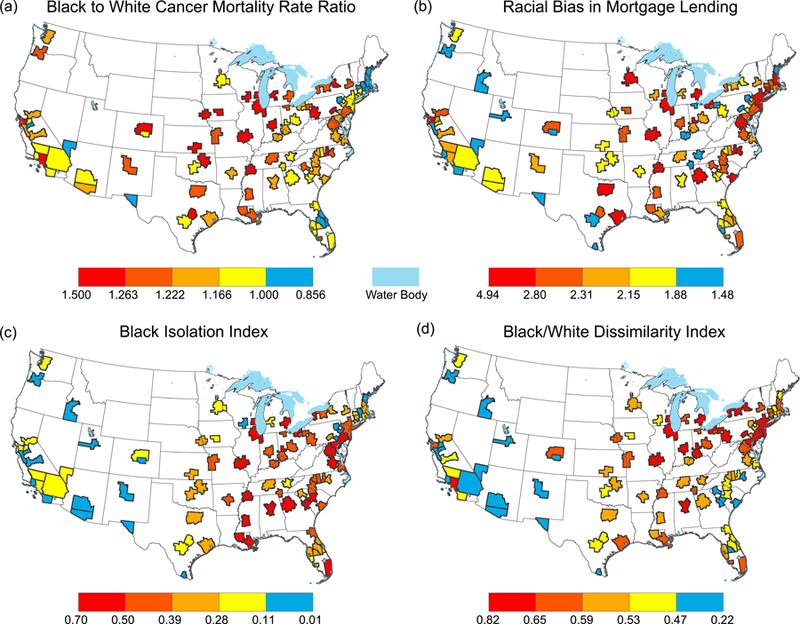
Shown are the spatial distributions of (panel a) cancer mortality disparities and three measures of structural racism in housing: (panel b) Racial Bias in Mortgage Lending, (panel c) Black isolation, and (panel d) dissimilarity. Category breaks on all maps represent quantiles, such that one fifth of the metropolitan areas shown are represented by each color. However, to enhance interpretation, the lowest category (blue) for mortality disparities is adjusted such that blue areas represent places where Blacks have equal or lower mortality than Whites. In contrast, metropolitan areas where Blacks have higher mortality rates than Whites are shown in shades of red and yellow, with the darkest red indicating the largest disparity between Blacks and Whites. Of the 100 largest US metropolitan areas, information was available for all metropolitan areas for structural racism measures, and for all but 3 for mortality.
Housing discrimination also varies geographically (Fig 1, panels b-d). For each map, areas with the highest values are depicted in red; lowest values are in blue. Mortgage discrimination (panel b) ranges from a low of 1.46 in El Paso, TX to a high of 4.94 in Milwaukee, WI. In no MSA were Blacks at an advantage for securing a mortgage loan. Mortgage discrimination is higher in the Midwest, Northeast, and parts of the South, and lower in the West. Two segregation measures are presented. For each measure, a higher value implies a greater degree of racial segregation. The Black isolation index (panel c) is higher in the Midwest and Eastern US and lower in the West and Southwest, ranging from a low of 0.01 in Provo-Orem, UT, to a high of 0.70 in Detroit, MI. The dissimilarity index (panel d) ranges from a low of 0.22 in Provo-Orem, UT, to a high of 0.82 in Milwaukee, WI. Dissimilarity is highest in the Midwest, Northeast, and parts of the South, and lowest in the West and parts of the Southeast.
Mortgage discrimination is correlated (Figure 2) with both dissimilarity (r=0.55, p<0.001) and isolation (r=0.55, p<0.001). Correlations indicate that mortgage discrimination is positively associated with, but does not duplicate, segregation metrics. Black isolation correlates, as expected, with dissimilarity (r=0.57, p<0.001). Figure 2 displays the distributions of each housing discrimination measure and their relationships. Each plot illustrates a correlation between two variables, with the histograms on each axis representing the distribution of each single variable. As illustrated, the distributions of isolation and dissimilarity are quite different, despite the fact that they both correlate with mortgage discrimination at r=0.55. Black isolation is distributed across the range of values from 0 to 1, while dissimilarity is more normally distributed.
Figure 2. Distributions and correlations of housing discrimination measures.
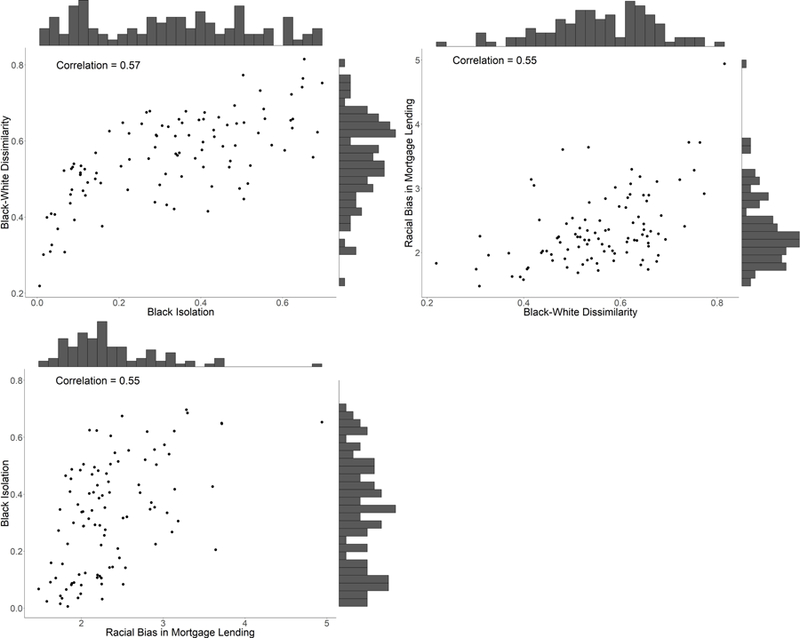
Each scatter plot illustrates a correlation between two housing discrimination variables, with the histograms on each axis representing the distribution of each single variable.
Relationship of Cancer Mortality Disparities to Housing Discrimination
As expected from visual inspection of the maps, in areas where Blacks experience greater mortgage discrimination, they are also at a greater cancer mortality disadvantage (Table 1: r=0.32, p=0.001). This relationship persists when stratified by sex (males: r=0.37, p< 0.001; females: r=0.23, p=0.02). While these relationships are statistically significant, they are not absolute, as evidenced by some MSAs with lower cancer mortality disparities despite high levels of mortgage discrimination.
Table 1:
Correlations between measures of structural racism in housing and cancer mortality disparities (2009–2013) for large US metropolitan areas
| MRR | Black Isolation | Black to White Dissimilarity | Racial Bias in Mortgage Lending | |||
|---|---|---|---|---|---|---|
| Corr | P-value | Corr | P-value | Corr | P-value | |
| All | 0.19 | 0.06 | 0.12 | 0.24 0.28 |
0.32 | 0.001 |
| Females | 0.12 | 0.25 | 0.11 | 0.23 | 0.02 | |
| Males | 0.31 | 0.002 | 0.13 | 0.21 | 0.37 | <0.001 |
Note: MRR=Mortality Rate Ratio. MRRs are calculated for ages 25+; bold indicates statistical significance at alpha=0.05.
In contrast, segregation measures are inconsistently associated with the cancer mortality disparity. In areas where Blacks experience greater isolation (segregation), Black men die of cancer at a higher rate (r=0.31, p=0.002), but this is not true for women (r=0.12, p=0.25), and the overall relationship (for women and men combined) is of borderline significance (r=0.19, p=0.06). Dissimilarity is not correlated significantly with mortality disparities (r=0.12, p=0.24).
Accounting for Confounding
We then examined whether observed associations between mortgage discrimination and cancer disparities are robust to confounding factors using a series of multivariate models. Table 2 presents the results of these models. Mortgage discrimination is significantly associated with cancer mortality disparities when controlling for MSA-level socioeconomic factors (median household income, proportion unemployed, proportion with a high school education) for females (coef=0.05, p-value=0.005) and males (coef=0.09, p-value<0.001). For males, the association persists when controlling for both segregation measures simultaneously (coef=0.07, p-value=0.003) and in a final model controlling for socioeconomic factors and segregation measures (coef=0.05, p-value=0.041). Adjusting for SES or segregation did not attenuate the relationship between racial bias and cancer mortality disparities.
Table 2:
Multivariate models examining associations between mortgage discrimination and cancer mortality disparities (2009–2013) for large US metropolitan areas
| Unadjusted | Adjusted for SES | Adjusted for Segregation | Adjusted for SES and Segregation | |||||
|---|---|---|---|---|---|---|---|---|
| Coef | P-value | Coef | P-value | Coef | P-value | Coef | P-value | |
| All | 0.06 | 0.001 | 0.07 | <0.001 | 0.06 | 0.007 | 0.05 | 0.034 |
| Females | 0.04 | 0.021 | 0.05 | 0.005 | 0.05 | 0.053 | 0.04 | 0.134 |
| Males | 0.08 | <0.001 | 0.09 | <0.001 | 0.07 | 0.003 | 0.05 | 0.041 |
Note: bold indicates statistical significance at alpha=0.05. SES variables include MSA median household income, proportion unemployed and proportion without a high school diploma. Segregation variables include isolation and similarity.
Accounting for Cancer Incidence Disparities
Black to White cancer mortality disparities could be attributable to higher cancer incidence among Blacks, poorer survival among Blacks, or both. This distinction is important as it may point to different solutions in clinical care, public health practice, and/or policy-making. Cancer survival data are not consistently available at the MSA level, but cancer incidence data is available. We determined whether and to what extent incidence explains observed relationships between housing discrimination and cancer mortality disparities; that portion of the relationship that was not explained by incidence would presumably be attributable to cancer survival.
Figure 3 presents overall cancer MRRs and IRRs, using quintiles. Cancer incidence disparities vary geographically, distributed similarly to mortality disparities. Compared to mortality disparities, incidence disparities are smaller and less often present. Of the MSAs, 59% have IRRs above 1. Incidence disparities range from a low of 0.60 in McAllen TX to a high of 1.41 in Madison, WI.
Figure 3. Geographic variation in Black-to-White cancer incidence and mortality disparities across US metropolitan areas.
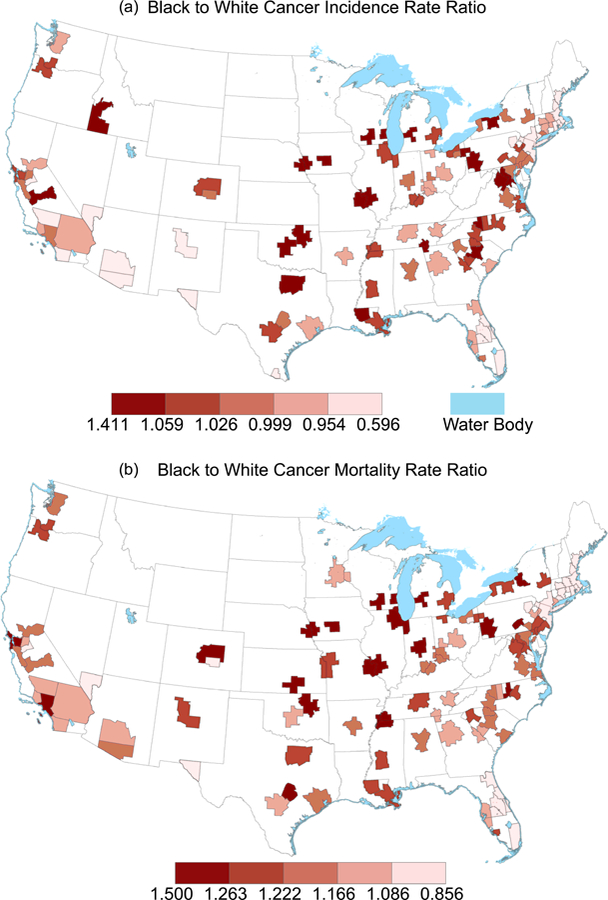
Shown are the spatial distributions of Black to White disparities in cancer incidence (panel a) and mortality (panel b). Quantile breaks are used on both maps, such that one fifth of each map is in each color category, to illustrate the relationship between large cancer mortality and incidence disparities across US metropolitan areas. Of the 100 largest US metropolitan areas, information was available for all but 3 areas for mortality, and all but 5 areas for incidence.
Black individuals living in areas with greater mortgage discrimination (r=0.25, p-value=0.02) and isolation (r=0.23, p-value=0.02) experience a greater relative cancer incidence burden (Table 3). This relationship is driven by strong and significant correlations among men (mortgage bias: r=0.36, p<0.001; isolation: r=0.33, p=0.001). Housing discrimination is not related to the incidence disparity among women (r=0.15, p-value=0.15), and dissimilarity shows no significant correlation (r=−0.06, p-value=0.59).
Table 3:
Correlations between measures of structural racism in housing and cancer incidence disparities (2009–2013) for large US metropolitan areas
| IRR | Black Isolation | Black to White Dissimilarity | Racial Bias in Mortgage Lending | |||
|---|---|---|---|---|---|---|
| Corr | P-value | Corr | P-value | Corr | P-value | |
| All | 0.23 | 0.02 | −0.06 | 0.59 | 0.25 | 0.02 |
| Females | 0.17 | 0.11 | −0.15 | 0.15 | 0.15 | 0.15 |
| Males | 0.33 | 0.001 | 0.08 | 0.43 | 0.36 | <0.001 |
Note: IRR=Incidence Rate Ratio. IRRs are calculated for ages 25+; bold indicates statistical significance at alpha=0.05.
To determine whether observed relationships between housing discrimination and cancer mortality disparities could be explained by disparities in incidence, we calculated partial correlation coefficients (Table 4). Controlling for incidence disparities attenuates, but does not eliminate, the relationship between mortgage discrimination and mortality disparities overall (r=0.24, p=0.02), and in sex specific analyses (males: r=0.22, p=0.04; females: r=0.22, p=0.04). This finding implies that Black individuals living in areas with higher mortgage discrimination experience a greater disadvantage in both cancer incidence and survival.
Table 4:
Partial correlation coefficients between measures of structural racism and cancer mortality disparities (2009–2013), while controlling for incidence disparities, for large US metropolitan areas
| Black Isolation | Racial Bias in Mortgage Lending | |||
|---|---|---|---|---|
| Corr | P-value | Corr | P-value | |
| All | 0.04 | 0.68 | 0.24 | 0.02 |
| Females | −0.01 | 0.96 | 0.22 | 0.04 |
| Males | 0.13 | 0.22 | 0.22 | 0.04 |
Note: bold indicates statistical significance at alpha=0.05
However, adjusting for the incidence disparity fully attenuates the relationship between isolation and mortality disparities for men. This finding implies that the greater cancer mortality burden experienced by Black men living in more segregated areas is primarily due to a larger disadvantage in incidence, rather than poorer cancer survival. Adjusted analyses were not performed using the dissimilarity metric, as it was not significantly associated with mortality disparities in unadjusted analyses.
DISCUSSION
This study documents substantial geographic variation in cancer mortality disparities and housing discrimination among the largest US MSAs. In MSAs with higher levels of mortgage discrimination, Blacks are at a greater cancer mortality disadvantage compared to Whites. This relationship persists when adjusting for socioeconomic factors known to be related to breast cancer mortality disparities.18 The relationship between mortgage discrimination and cancer mortality disparities is attenuated, but not eliminated, when adjusting for incidence disparities, implying that both incidence and survival are factors relevant to the relationship between mortgage discrimination and cancer mortality disparities. Measures of segregation are inconsistently associated with cancer disparities, although Black men living in areas with greater isolation experience significantly greater cancer incidence and mortality. Much of the existing literature on racial disparities focuses on poorer survival among racial groups once the cancer is diagnosed, with less focus on incidence or prevention (other than tobacco reduction).18,19 Our findings suggest that cancer incidence, mortality, and survival disparities warrant attention.
There are plausible mechanisms by which mortgage discrimination might cause greater cancer incidence or poorer survival among Blacks. A higher chance of mortgage application denial for Black applicants tends to reduce Black home ownership and increase the likelihood of renting. Renting results in a reduced ability to accumulate home equity – a primary source of wealth – which may limit resources available to offset the financial burden of cancer. Neighborhoods with higher proportions of renters have higher levels of residential instability, which can weaken social ties and limit social support.20 Lack of social support adversely affects cancer survival.21 High levels of housing discrimination could also indicate more pervasive discriminatory norms in other sectors (e.g. criminal justice, labor). Higher stress levels induced by structural racism in multiple sectors could lead to deleterious coping behaviors, including alcohol abuse, tobacco use and unhealthy eating, and social stressors themselves have been linked to more aggressive forms of cancer.22,23 Only two small, local studies have previously related biased mortgage lending to cancer outcomes.13,24
We did not find segregation to be consistently associated with cancer disparities. A few prior studies have related segregation to site-specific cancer disparities nationally, with mixed results.3,4,25,26 While segregation may result from housing discrimination, it is different from other forms of housing discrimination as it may also reflect individual choices to live in a community that shares a racial identity.27 The “enclave” effect may partially balance the adverse effects of racial segregation, through social support or other health-promoting mechanisms.28 The competing effects of health harm and benefit garnered from living in racially or ethnically homogenous places may provide an explanation for mixed results observed.
Further, it is important to note differences among housing discrimination measures used. Mortgage discrimination is consistently associated with cancer disparities, while segregation is not. Segregation reflects both the effects of housing discrimination and personal housing choices, making interpretation complex.27 The mortgage discrimination measure is distinct from segregation measures as it is a measure of discrimination in a system, rather than a measure of the spatial distribution of individuals, by race and/or ethnicity, across a metropolitan area. For this reason, mortgage discrimination may offer a more “pure” measure of housing discrimination.
In this study, Black men living in areas with greater segregation (isolation) were found to experience greater cancer mortality disparities, but there was no relationship for women. Further, this relationship is explained by incidence disparities, suggesting that factors strongly associated with cancer incidence may play an important role. These gender differences should be further explored and may be due in part to causal factors associated with sex-specific cancer sites (e.g. prostate) or to gendered behavioral responses to racial segregation that affect cancer risk. We speculate that potential linkages between Black isolation and cancer incidence disparities affecting males and females differently could include patterns of tobacco use, fresh fruit and vegetable consumption, activity levels, health care seeking behaviors, and exposure to stressors or hazardous environmental contaminants based on occupation or social interactions, among other factors.8 Further, dissimilarity was not associated with mortality disparities; it is possible that this measure may not capture, as compared to Black isolation, the effects of particular environments within an MSA where Black residents live, instead measuring whether populations are distributed evenly across the MSA. This finding deserves further exploration in future work.
This study has limitations. We focused only on disparities between Black and White populations. We focused specifically on structural racism in housing because of the importance of housing in shaping residential neighborhood exposures that are known to influence health. However, other types of structural racism – particularly in sectors such as justice, labor and education – should be examined. This is an ecological analysis, not an analysis of individual level data. Therefore, caution is required when generalizing conclusions to the individual level.
This study has several strengths. Data used are objectively measured – originating from cancer registry, vital statistics, census, and Home Mortgage Disclosure Act records – and offer broad coverage of the US Black population. US Census American Community Survey 2013 data indicates that 75% of the US Black population resides in one of the largest 100 metropolitan areas. In addition, few prior studies have examined structural racism and cancer. We employed a novel measure of mortgage discrimination to quantify a form of housing discrimination that is amenable to modification through policy change. Further, our intentional choice to employ straightforward statistical analyses emphasized clear relationships of interest, while revealing important exceptions.
The influence of housing discrimination on cancer disparities could be targeted in at least two ways. By identifying exceptions to primary relationships observed, policies might be identified to mitigate the effects of such discrimination. This potential is evidenced by several MSAs (Boston, MA; New York City, NY; Hartford, CT) where high levels of mortgage discrimination are not accompanied by large disparities. However, in the long term, it would be preferable to address the problem of housing discrimination directly. Approaches could include housing mobility programs that specifically target public health improvement29 or provide counseling to voucher recipients,30 or policies that target mortgage discrimination itself, including borrower-focused policies such as requiring a “loan price tag” or loan comparison report to empower applicants.31
We identify housing discrimination as an important and largely unexplored factor that may influence racial cancer disparities in the United States. Our finding that MSAs with higher levels of housing discrimination experience larger racial cancer disparities suggests that future work should explore the causal relation between housing discrimination and racial disparities in cancer mortality. A recent position statement from the American Association for Cancer Research, American Cancer Society, American Society of Clinical Oncology, and National Cancer Institute argued that variation in disparities across the US indicates an important role for system-level factors and social determinants of health in explaining cancer health disparities.32 This study supports that assertion, indicating that housing discrimination is an important factor to consider in future work that seeks to explain and ultimately eliminate cancer disparities.
Acknowledgments:
This work was funded in part by the National Cancer Institute/National Institutes of Health, through grants R01-CA214805 (PI: Beyer) and R01-CA170945 (PI: Nattinger) and in part by the Advancing a Healthier Wisconsin Endowment at the Medical College of Wisconsin.
Research Support: This work was funded in part by the National Cancer Institute/National Institutes of Health, through grants R01-CA214805 and R01-CA170945 and in part by the Advancing a Healthier Wisconsin Endowment at the Medical College of Wisconsin.
Footnotes
Conflict of interest statement: The authors have no conflicts of interest to report.
References
- 1.DeSantis C, Naishadham D, Jemal A. Cancer statistics for African Americans, 2013. CA Cancer J Clin 2013;63(3):151–166. [DOI] [PubMed] [Google Scholar]
- 2.Kochanek KD, Arias E, Anderson RN. How did cause of death contribute to racial differences in life expectancy in the United States in 2010? NCHS Data Brief 2013;(125):1–8. http://www.ncbi.nlm.nih.gov/pubmed/24152376. [PubMed] [Google Scholar]
- 3.Benjamins MR, Hunt BR, Raleigh SM, Hirschtick JL, Hughes MM. Racial Disparities in Prostate Cancer Mortality in the 50 Largest US Cities. Cancer Epidemiol 2016;44:125–131. [DOI] [PubMed] [Google Scholar]
- 4.Whitman S, Orsi J, Hurlbert M. The racial disparity in breast cancer mortality in the 25 largest cities in the United States. Cancer Epidemiol 2012;36(2):e147–e151. [DOI] [PubMed] [Google Scholar]
- 5.Desantis CE. Breast Cancer Statistics , 2017 , Racial Disparity in Mortality by State 2017;67(6):439–448. doi: 10.3322/caac.21412. [DOI] [PubMed] [Google Scholar]
- 6.Gee GC, Ford CL. Structural racism and health inequities. Du Bois Rev Soc Sci Res Race 2011;8(01):115–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Williams DR, Mohammed SA. Racism and health: Pathways and scientific evidence. Am Behav Sci 2013;57(8):1199–1216. doi: 10.1177/0002764213487340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet 2017;389(10077):1453–1463. doi: 10.1016/S0140-6736(17)30569-X. [DOI] [PubMed] [Google Scholar]
- 9.Chae DH, Clouston S, Hatzenbuehler ML, et al. Association between an internet-based measure of area racism and black mortality. PLoS One 2015;10(4):e0122963. doi: 10.1371/journal.pone.0122963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lukachko A, Hatzenbuehler ML, Keyes KM. Structural racism and myocardial infarction in the United States. Soc Sci Med 2014;103:42–50. doi: 10.1016/j.socscimed.2013.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. J Inf 2006;96(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention. United States Cancer Statistics: Public Information Data https://wonder.cdc.gov/cancer.HTML. Published 2016.
- 13.Beyer KMM, Zhou Y, Matthews K, Bemanian A, Laud PW, Nattinger AB. New spatially continuous indices of redlining and racial bias in mortgage lending: links to survival after breast cancer diagnosis and implications for health disparities research (manuscript submitted) [DOI] [PubMed] [Google Scholar]
- 14.Cohen J, Cohen P, West SG, Aiken LS. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences (3rd Ed.); 2003. http://ezproxy.massey.ac.nz/login?url=http://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,cookie,url,uid&db=psyh&AN=2002-18109-000&site=ehost-live.
- 15.SAS Institute. SAS 9.4 2013. [Google Scholar]
- 16.StataCorp. Stata: Release 15. Statistical Software 2017. [Google Scholar]
- 17.ESRI. ArcMap: Release 10.6.1 Redlands, CA: Environmental Systems Research Institute; 2018. [Google Scholar]
- 18.Nattinger AB, Wozniak EM, McGinley EL, Li J, Laud P, Pezzin LE. Socioeconomic Disparities in Mortality Among Women With Incident Breast Cancer Before and After Implementation of Medicare Part D. Med Care 2016:1. doi: 10.1097/MLR.0000000000000685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bigby JA HMD. Disparities across the Breast Cancer Continuum. Cancer Causes Control 2005;16(1):35–44. [DOI] [PubMed] [Google Scholar]
- 20.Sampson RJ, Groves WB. Community structure and crime: Testing social-disorganization theory. Am J Sociol 1989:774–802. [Google Scholar]
- 21.Kroenke CH, Kubzansky LD, Schernhammer ES, Holmes MD, Kawachi I. Social networks, social support, and survival after breast cancer diagnosis. J Clin Oncol 2006;24(7):1105–1111. doi: 10.1200/JCO.2005.04.2846. [DOI] [PubMed] [Google Scholar]
- 22.Zeigler-Johnson CM, Tierney A, Rebbeck TR, Rundle A. Prostate cancer severity associations with neighborhood deprivation. Prostate Cancer 2011;2011:846263. doi: 10.1155/2011/846263 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dietze EC, Sistrunk C, Miranda-Carboni G, O’Regan R, Seewaldt VL. Triple-negative breast cancer in African-American women: disparities versus biology. Nat Rev Cancer 2015;15(4):248–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zhou Y, Bemanian A, Beyer KMM. Housing Discrimination, Residential Racial Segregation, and Colorectal Cancer Survival in Southeastern Wisconsin. Cancer Epidemiol Biomarkers Prev [DOI] [PubMed] [Google Scholar]
- 25.Hayanga AJ, Zeliadt SB, Backhus LM. Residential segregation and lung cancer mortality in the United States. JAMA Surg 2013;148(1):37–42. [DOI] [PubMed] [Google Scholar]
- 26.Haas JS, Earle CC, Orav JE, et al. Racial segregation and disparities in breast cancer care and mortality. Cancer 2008;113(8):2166–2172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Eligon J Affluent and Black, and Still Trapped by Segregation. New York Times https://www.nytimes.com/2016/08/21/us/milwaukee-segregation-wealthy-black-families.html. Published August 20, 2016. [Google Scholar]
- 28.Eschbach K, Ostir GV, Patel KV, Markides KS, Goodwin JS Neighborhood context and mortality among older Mexican Americans: Is there a barrio advantage? Am J Public Health 2004;94(10):1807–1812. doi: 10.2105/AJPH.94.10.1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kruckenberg K, Tegeler P. Policy Brief July 2010 2010;(July):1–10. [Google Scholar]
- 30.Tegeler P The Need for a National Housing Mobility Infrastructure. In: Keels M, ed. URBAN AMERICA FORWARD: CIVIL RIGHTS ROUNDTABLE SERIES ; 2016:1–2. http://www.prrac.org/pdf/need_for_national_housing_mobility_infrastructure.pdf. [Google Scholar]
- 31.Bybee JR. Fair lending 2.0: A borrower-based solution to discrimination in mortgage lending. Univ Michigan J Law Reform 2009;45(1):113–154. [Google Scholar]
- 32.Polite BN, Adams-Campbell LL, Brawley OW, et al. Charting the future of cancer health disparities research: A position statement from the American Association for Cancer Research, the American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute. CA Cancer J Clin 2017. doi: 10.3322/caac.21404. [DOI] [PubMed] [Google Scholar]