

Abstract
There is limited research testing longitudinal models of how posttraumatic stress disorder (PTSD) severity leads to impaired relationship adjustment. The present study evaluated 2 potential mechanisms among a longitudinal sample of National Guard soldiers deployed to the Iraq War: (1) sensitivity to cues associated with punishment within intimate relationships and (2) sensitivity to cues associated with incentives in intimate relationships. Participants were surveyed by mail 1 year after an extended 16-month combat deployment and again 2 years later. Using a cross-lagged panel analysis with 2 mediators (relationship-specific threat and incentive sensitivity), findings indicated Time 1 PTSD symptom severity significantly eroded relationship adjustment over time through greater sensitivity to cues of relationship-related punishment, but not through incentive sensitivity. Additionally, findings indicated sensitivity to cues of relationship-related threats maintains symptoms of PTSD while sensitivity to cues of relationship-related incentives maintains relationship adjustment. Finally, PTSD symptoms significantly predicted erosion of relationship adjustment over time; however, associations from relationship adjustment to changes in PTSD severity over time were nonsignificant. Findings are discussed within the context of reinforcement sensitivity theory and emotional processing theory of PTSD.
Keywords: PTSD, couples, Reinforcement Sensitivity Theory, veterans, military families
Prior work suggests 12% to 20% of veterans returning from the wars in Iraq and Afghanistan screen positive for posttraumatic stress disorder (PTSD; Hoge et al., 2004; Schell & Marshall, 2008). Supportive family relationships, frequently with an intimate partner, can facilitate seeking mental health treatment and successful treatment response for those with PTSD symptoms (Evans, Cowlishaw, & Hopwood, 2009; Meis, Barry, Kehle, Erbes, & Polusny, 2010). However, the adjustment and stability of these important relationships is disrupted by the disorder itself (Taft, Watkins, Stafford, Street, & Monson, 2011). Empirical evidence demonstrating how PTSD erodes intimate relationships is vital to fortifying these relationships and supporting recovery from PTSD. The present work focuses on a central piece of this larger phenomenon: how symptoms of PTSD may erode veterans’ relationship adjustment, through veterans’ sensitivity to cues of punishment (relationship-related threat sensitivity) and cues of reward (relationship-related incentive sensitivity) within intimate relationships.
Sensitivity to Signals of Incentive and Threat
Several theories of behavior and personality coalesce around two fundamental and distinct action tendencies: approach and avoidance, sometimes referred to as appetitive and aversive motivation (Carver, Sutton, & Scheier, 2000). These tendencies are managed by various nervous system structures and systems. For approach tendencies, descriptions of potential underlying systems include, but are not limited to, the behavioral approach system (Gray, 1981), the behavioral engagement system (Depue, Krauss, & Spoont, 1987), and the behavioral activation system (Cloninger, 1987). For avoidance or withdrawal tendencies, proposed underlying systems include the behavioral inhibition system (Gray, 1981), fight-flight-freeze system (Gray & McNaughton, 2000), and withdrawal system (e.g., Davidson, 1988). Individual differences in the sensitivity of these systems exist and lead some individuals to be more or less highly engaged in the pursuit of potential incentives and avoidance of potential threats (Carver et al., 2000). Emotional experiences are linked to these action tendencies; high threat sensitivity is associated with negative affect, negative emotional experiences, and anxiety (Carver & White, 1994; Johnson, Turner, & Iwata, 2003); low incentive sensitivity is associated with symptoms of depression (e.g., Pinto-Meza et al., 2006) and high incentive sensitivity with impulsivity (e.g., Aluja & Blanch, 2011). For combat veterans with PTSD, sensitivities toward cues associated with punishment and reward within relationships likely develop prior to combat exposure; however, sensitivities are malleable with experience, learning, and environmental circumstances (Bijttebier, Beck, Claes, & Vandereycken, 2009; Hundt, Nelson-Gray, Kimbrel, Mitchell, & Kwapil, 2007; Shiner & Caspi, 2003).
Threat Sensitivity, PTSD, and Relationships
Prior studies support positive associations between PTSD symptom severity and threat sensitivity (e.g., Contractor, Elhai, Ractliffe, & Forbes, 2013; Maack, Tull, & Gratz, 2012; Pickett, Bardeen, & Orcutt, 2011). Emotional processing theory (Foa & Kozak, 1986; Foa, Ehlers, Clark, Tolin, & Orsillo, 1999) suggests PTSD symptoms are associated with shifts in worldview, including beliefs the world is a dangerous place and one cannot tolerate distress. Avoidance of trauma reminders, a central component of PTSD, maintains symptoms by preventing emotional processing of the trauma memory. Shifts in worldview, efforts to avoid trauma reminders, and hypervigilance, while trauma specific, are consistent with experiences of greater sensitivity to cues of punishment within one’s environment (Contractor et al., 2013).
Within the context of intimate relationships, threat sensitivity has been linked to rejection sensitivity, increases in negative attitudes about social bonds, and a focus on avoidance of negative outcomes in relationships, such as conflict (Gable, 2006; Laurenceau, Klienman, Kaczynski, & Carver, 2010). Although not isomorphic, Carver and Scheier’s (1998) description of emotional regulation may have utility in understanding the influence of threat sensitivity on relationships. Among those with greater threat sensitivity, a focus on cues of relationship-related punishment may lead to problematic or counterproductive relationship behavior to avoid such punishment, including disengagement and avoidance. These behaviors may reduce the opportunity for conflict resolution and closeness as individuals make efforts to increase the distance between their present circumstances and cues of relationship-related punishment (i.e., a discrepancy-enlarging loop; Carver & Scheier, 1998). This is consistent with prior cross-sectional work establishing avoidance in relationships as a pathway through which PTSD leads to poor family functioning (Creech, Benzer, Liebsack, Proctor, & Taft, 2013) and with research linking threat sensitivity to emotional withdrawal, maladaptive efforts to avoid aversive internal experiences, destructive behaviors, and emotional regulation difficulties (Bolger & Zuckerman, 1995; Hannan & Orcutt, 2013; Maack et al., 2012; Pickett et al., 2011; Tull, Gratz, Latzman, Kimbrel, & Lejuez, 2010).
Incentive Sensitivities, PTSD, and Relationships
The literature examining associations between incentive sensitivities and symptoms of PTSD is less consistent and largely inconclusive (Contractor, Elhai, Ractliffe, & Forbes, 2013; Maack et al., 2012; Pickett et al., 2011). Prior work has hypothesized that PTSD symptoms of dysphoric mood or emotional numbing may be associated with a diminished sensitivity for incentive cues, reduced capacity for positive emotional states in response to incentives, and lower incentive expectation (Pickett et al., 2011). Within intimate relationships, individuals with reduced sensitivity to incentives cues may be less motivated to seek relationship-related pleasurable experiences (e.g., closeness, affection), causing individuals to fail to pursue closeness and intimacy. Within intimate relationships, increased sensitivity to signals of relationship-related incentives have been associated with greater desire for relationships with others, greater reward responsiveness, lower anxiety after a conflict discussion, and greater overall relationship functioning (Berry, Willingham, & Thayer, 2000; Laurenceau et al., 2010; Meyer, Olivier, & Roth, 2005). However, research has yet to examine how threat and incentive sensitivities, as manifested within intimate relationships, function as pathways through which PTSD erodes relationship adjustment.
Present Study
We examined how PTSD symptom severity, measured among veterans recently returned from the Iraq War (Time 1), may lead to changes in veterans’ relationship adjustment 2 years later (Time 2), through relationship-related threat and incentive sensitivity. We used a longitudinal cross-lagged panel design, hypothesizing that Time 1 PTSD symptom severity would lead to poorer relationship adjustment through greater relationship-related threat sensitivity (Primary Hypothesis 1; H1; see red [dark gray] solid lines in Figure 1) and poorer relationship-related incentive sensitivity (Primary Hypothesis 2; H2).
Figure 1.
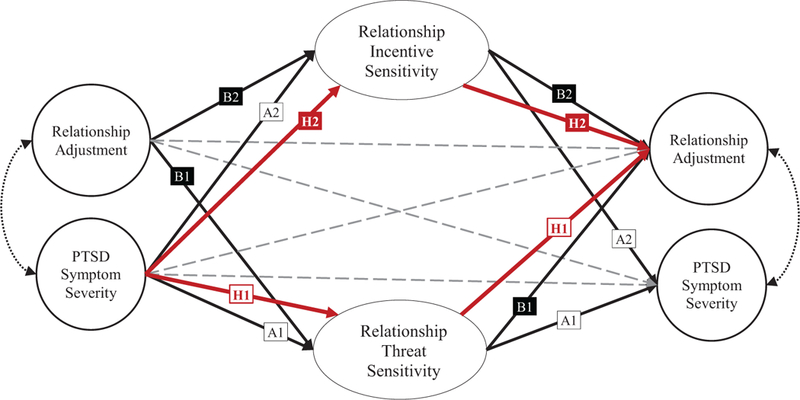
Hypothesized indirect pathways from Time 1 to Time 2. H1 = Hypothesis 1: indirect pathway from PTSD severity to poorer relationship adjustment through relationship threat sensitivity (red [dark gray] solid lines). H2 = Hypothesis 2: indirect pathway from PTSD severity to poorer relationship adjustment through lower relationship incentive sensitivity (red [dark gray] solid lines). A1 = Exploratory Objective A1: testing associations between relationship threat sensitivity and changes in PTSD symptom over time. A2 = Exploratory Objective A2: testing associations between relationship incentive sensitivity and changes in PTSD symptom over time. B1 = Exploratory Objective B1: testing associations between relationship threat sensitivity and changes in relationship adjustment over time. B2 = Exploratory Objective B2: testing associations between relationship incentive sensitivity and changes in relationship adjustment over time. PTSD = posttraumatic stress disorder. See the online article for the color version of this figure.
The study design also allows for exploring associations between relationship-related sensitivities and (A) changes in PTSD symptoms over time (Exploratory Objectives A1 and A2; see black solid lines in Figure 1) and (B) changes in relationship adjustment over time (Exploratory Objectives B1 and B2; see black solid lines in Figure 1). Relationship-related sensitivities may be associated with maintaining functioning over time for relationship adjustment and PTSD symptom severity. For example, PTSD symptoms at Time 1 may be associated with greater threat sensitivity, including within intimate relationships. Greater relationship-related threat sensitivity may contribute to fueling threat vigilance and avoidance behaviors broadly and, consequently, PTSD symptoms. Alternatively, poor relationship adjustment may be associated with reduced sensitivity to relationship-related incentive cues. This blunted sensitivity may maintain relationship distress by limiting the ability of positive interactions to buffer the effects of relationship conflict and strain on relationship adjustment.
Lastly, prior work examining potential reciprocal relationships between relationship adjustment and PTSD symptom severity over time is limited and conflicting, with some work indicating associations are bidirectional (Evans et al., 2009) and other suggesting the effects are unidirectional, such that PTSD symptoms erode relationship adjustment, while the alternative pathway (relationship adjustment → PTSD severity) is nonsignificant (Erbes, Meis, Polusny, Compton, & MacDermid Wadsworth, 2012). The design of the present study design allows us to also examine these effects over time (Exploratory Objective C; see dotted lines in Figure 1).
Method
Participants and Procedures
Participants were drawn from a longitudinal cohort study of National Guard soldiers deployed to Iraq for Operation Iraqi Freedom (OIF) from March of 2006 to July of 2007 (Ferrier-Auerbach, Erbes, Polusny, Rath, & Sponheim, 2010). Time 1 data were drawn from mailed surveys obtained 1 year after soldiers’ return from deployment. All Time 1 responders were mailed surveys 2 years later (Time 2, i.e., 3 years after return from deployment). At both time points, we used standard mailed survey methodology to optimize response rates (Dillman, Smyth, & Christian, 2014). Participants were sent an initial survey packet, containing a cover letter (informed consent document), survey, postage paid return envelope, and $20 incentive. At 2-week intervals, nonrespondents were mailed a postcard reminder, second survey, and a third survey, using overnight (United Parcel Service Priority Mail) mail. Unique participant identification numbers were attached to each survey to link returned surveys to participants’ identifiable information through a crosswalk file, accessible only to study staff.
Response rates were 49.3% (n = 953) at Time 1 and 59.1% at Time 2 (n = 563). At Time 1, compared to nonresponders, there were no significant differences on ethnicity, gender, or PTSD symptom severity. Time 1 survey responders were significantly older, more likely to be married, less likely to be of enlisted rank than nonresponders (Polusny et al., 2011). At Time 2, there were no significant differences between responders and nonresponders on PTSD symptoms or gender. Compared to nonresponders, Time 2 survey responders were older (33.56 vs. 31.37 years old on average), F(1, 941) = 16.11, p < .001), more educated, F(1, 947) = 16.79, p < .001, more likely to be White (89.51% vs. 84.47%), χ2(N = 1) = 5.21, p = .022), and in longer intimate relationships, F(1, 753) = 10.10, p < .002.
For the present set of analyses, we included those individuals who completed Time 1 surveys and were in intimate relationships. As the dependent variable was relationship adjustment, we then excluded the 106 participants were not in intimate relationships at Time 2, leaving a final sample of 771 participants at Time 1 and 453 at Time 2. Of note, veterans were only surveyed at Time 2 if they had completed Time 1 surveys. Consequently, all 453 Time 2 participants had completed Time 1 surveys. On average, participants were 33 years old at Time 1 (M = 32.87, SD = 8.18). Most (76.2%) had attended some college or obtained a college degree (associate’s or bachelor’s); 3.9% had advanced degrees. Many had been in intimate relationships for 5 or more years at Time 1 (47.2%; 2–5 years = 24.5%; 6 months to 2 years = 19.7%; 0 to 6 months = 8.6%). Most were male (92.2%), enlisted (85.2%), and White (88.6%; 3.4% Black, 4.2% Hispanic American, 2.5% Native American or American Indian, 1.7% Asian American). The majority also had children or stepchildren (56.4%) and were married or living with an intimate partner (67.0%). Nearly half the sample (49.8%) reported at least one prior deployment, with 23.7% reporting a prior OIF or Operation Enduring Freedom deployment. Participants reported high rates of experiences consistent with combat, including receiving hostile or incoming fire (98.7%), participating in combat missions or patrols (88.1%), encountering land mines or booby traps (80.5%), being attacked by terrorists or civilians (76.4%), witnessing someone from their unit or an ally seriously injured or killed (45.1%), firing a weapon at the enemy (38.5%), and killing or believing they killed an enemy soldier (24.1%). At Time 1, 20.0% of the sample reported seeking mental health care since their return from deployment. At Time 2, 40.9% had sought mental health care since the previous survey.
Measures
PTSD symptoms.
PTSD symptom severity was assessed at Time 1 and Time 2, using the PTSD Checklist—Military Version (PCL-M; Weathers, Huska, & Keane, 1991). The PCL-M is a widely used instrument that consists of 17 Likert scale items, corresponding to Diagnostic and Statistical Manual of Mental Disorders (4th ed.) symptoms of PTSD. Response options range from 1 (not at all) to 5 (extremely). The measure has high test-retest reliability and internal consistency; validity of the instrument was established through correlates with other self-report instruments and gold-standard diagnostic interviews for PTSD (Ruggiero, Del Ben, Scotti, & Rabalais, 2003). A score above 50 and endorsement of “moderate” or greater on at least one symptom of reexperiencing, three symptoms of avoidance, and two symptoms of arousal was considered a positive screen for PTSD (Hoge et al., 2004). Alpha for the present sample were in the acceptable range (Time 1 α = .96; Time 2 α = .95).
Relationship adjustment.
An abbreviated version of the Dyadic Adjustment Scale (7 items; ADAS; Sharpley & Cross, 1982) was used to assess global relationship adjustment at both time points. The ADAS has demonstrated validity through correlates with couple beliefs, couple functioning, relationship status, relationship satisfaction, couple communication, conflict resolution, and cohesion (Hunsley, Pinsent, Lefebvre, James-Tanner, & Vito, 1995; Sharpley & Rogers, 1984). It also correlates at similar strengths as the original 32-item scale to relationship satisfaction, cohesion, and relationship functioning (Hunsley et al., 1995) and successfully discriminates distressed from nondistressed couples (Funk & Rogge, 2007). A score of 21.5 or below is considered a positive screen for clinically significant relationship strain (Funk & Rogge, 2007; present sample Time 1 α = .88; Time 2 α = .90). Items assess relationship happiness (0 to 6 scale), level of agreement with one’s intimate partner across various domains, frequency of positive shared activities, and positive communication on a 0 to 5 scale.
Relationship Incentive and Threat Sensitivity Scales (RITSS).
General predispositions, including individual traits and attitudes, are often poor predictors of specific behaviors (e.g., Epstein, 1979, 1980), driving recommendations that relationship specific traits and attitudes be used when examining relationship-specific behavior (Reis, Capobianco, & Tsai, 2002). For the present study, we administered the RITSS, an 11-item measure providing two relationship-specific sensitivity scales: Relationship Incentive Sensitivity (RIS) and Relationship Threat Sensitivity (RTS; Laurenceau et al., 2010). Items are scored on a 4-point Likert scale, ranging from very false (4) to very true (1). Higher scores on the RIS indicate greater tendencies to approach relationship-related incentives in intimate relationships (e.g., feeling connected). Higher scores on the RTS indicate greater motivation to avoid relationship-related threat (e.g., conflict).
Psychometric analyses examining scale validity indicate the RIS is significantly associated with affiliation, approach in friendships, and higher positive affect in men and women after positive relationship tasks. RIS scores correlate significantly with broad measures incentive sensitivity (behavioral activation system, drive and reward responsiveness) and inversely with attachment avoidance (Laurenceau et al., 2010). RIS scores demonstrate incremental validity in predicting relationship quality above and beyond global nondomain specific incentive and threat sensitivity scales. Validity analyses indicated RTS scores are significantly associated with avoidance and anxiety in relationships, rejection sensitivity in relationships, anxiety following aversive relationship tasks in women, and threat sensitivity. As expected, scores did not significantly associate with approach behavior in intimate relationships or other theoretically unrelated constructs (achievement motivation). As expected, RTS scores were negatively associated with relationship quality among women. Neither the RIS nor RTS significantly correlated with measures of social desirability. Finally, confirmatory factor analyses repeatedly supported a two-factor solution, consistent with the purported subscales (Laurenceau et al., 2010). Alphas for the present sample were adequate (Time 2 RIS α = .88; RTS α = .78).
Analytic Strategy
Hypothesized models were tested using structural equation modeling in Mplus (version 7; Muthén & Muthén, 1998–2012). Full information maximum likelihood estimation was used to obtain estimates for models tested, which performs optimally for data that are either Missing At Random or Missing Completely At Random (Peugh & Enders, 2004). Latent constructs were specified for each variable of interest. In examining change over time, it is important to first establish that the measurement of variables assessed repeatedly is consistent over time. Formal factorial invariance models (Meredith, 1993) were tested across Time 1 and Time 2 assessments of relationship adjustment and PTSD symptom severity. After establishing whether the measurement of constructs over time was consistent, we proceeded with testing our hypotheses and exploratory objectives. Model fit was evaluated by visual inspection of a series of goodness-of-fit indices: comparative fit index (CFI), Tucker-Lewis or nonnormed fit index, root-mean-square error of approximation (RMSEA), and standardized root-mean-square residual (SRMR). Guidelines suggest the following values are consistent with a desirable model fit: CFI ≥ .95, RMSEA ≤ .06, SRMR ≤ .08 (Hu & Bentler, 1999). We also evaluated the probability that the RMSEA was greater than .05 if the upper bound of the confidence interval exceeded .10 (Browne & Cudeck, 1993). Finally, we examined the pattern of associations among our model variables and the formal test of the indirect effects from PTSD symptoms at Time 1 to relationship adjustment at Time 2, through our mediating variables (relationship incentive sensitivity and relationship threat sensitivity), while controlling for Time 1 relationship adjustment scores.
Results
Based on established cutoffs described above, at Time 1, 14.1% of the sample screened positive for probable PTSD, 39.4% screened positive for clinically significant relationship distress, and 9.5% screened positive for both. Two years later (Time 2), 17.3% of the sample screened positive for probable PTSD, 37.4% for clinically significant relationship distress, and 11.5% for both probable PTSD and relationship distress. Correlations among latent variables are displayed in Table 1. We examined three formal factorial invariance models (i.e., configural, weak, and strong) of relationship adjustment and PTSD symptom change over time to identify the most parsimonious model of change in these constructs that also retained fit within acceptable limits. The strong invariance model (specifies the loading patterns, loading magnitudes, and intercepts to be equal across time) was the most parsimonious and demonstrated limited loss of fit across indices, χ2(N = 95) = 284.68, p < .001, CFI = .969, RMSEA = .057, 90% confidence interval (CI) [.050, .065], SRMR = .048; configural invariance model, χ2(N = 87) = 270.323, p < .001, CFI = .970, RMSEA = .059, 90% CI [.051, .067], SRMR = .046; weak invariance model, χ2(N = 92) = 280.01, p < .001, CFI = .969, RMSEA = .058, 90% CI [.050, .066], SRMR = .051. The structural model with standardized path coefficients was then estimated and is shown in Figure 2 in simplified form. The hypothesized structural model obtained adequate fit to the data, χ2(N = 79) = 222.74, p < .001, CFI = .946, RMSEA = .049, 90% CI [.041, .056], SRMR = .058.
Table 1.
Correlations Among Latent Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Time 1 PTSD checklist | — | |||||
| 2. Time 1 relationship adjustment | −.43 | — | ||||
| 3. Time 2 sensitivity to threats in relationships | .28 | −.05 | — | |||
| 4. Time 2 sensitivity to incentives in relationships | −.30 | .46 | .24 | — | ||
| 5. Time 2 PTSD checklist | .77 | −.33 | .31 | −.31 | — | |
| 6. Time 2 relationship adjustment | −.38 | .52 | −.08 | .60 | − .47 | — |
Note. PTSD = posttraumatic stress disorder.
Figure 2.

Structural model. Values represent standardized path coefficients. Solid lines represent statistically significant pathways (p < .01). Dashed lines represent nonsignificant pathways. PTSD = posttraumatic stress disorder.
Primary Hypothesis 1: Time 1 PTSD Severity → Relationship Threat Sensitivity → Time 2 Relationship Adjustment
Consistent with expectations, after accounting for all other pathways in the model, Time 1 PTSD symptom severity was significantly associated with greater Time 2 relationship threat sensitivity. Relationship threat sensitivity was, in turn, associated with changes in relationship adjustment from Time 1 to Time 2. The formal test of the indirect effect from Time 1 PTSD symptom severity to changes in relationship adjustment through relationship threat sensitivity was statistically significant (β = −.04, p = .012).
Primary Hypothesis 2: PTSD Severity → Relationship Incentive Sensitivity → Relationship Adjustment
Contrary to expectations, PTSD symptom severity at Time 1 failed to significantly predict poorer relationship incentive sensitivity at Time 2. However, Time 2 relationship incentive sensitivity was significantly associated with changes in relationship adjustment from Time 1 to Time 2. The indirect test of the pathway from Time 1 PTSD symptom severity to change in relationship adjustment over time, through relationship incentive sensitivity, was marginally significant (β = −.05, p = .096).
Exploratory Objective A: Time 1 PTSD Severity → (A1) Relationship Threat Sensitivity/(A2) Relationship Incentive Sensitivity → Time 2 PTSD Severity
Tests of the indirect effect from Time 1 PTSD symptom severity to Time 2 PTSD symptom severity through increased relationship threat sensitivity were statistically significant (β = .04, p = .004). However, the indirect path from PTSD Time 1 to Time 2 PTSD through decreased relatiositivity was nonsignificant. See Table 2.
Table 2.
Total, Indirect, and Direct Standardized Effects
| Effect | β | p | 95% CI |
|---|---|---|---|
| Total | −.21 | .000 | [−.28, −.13] |
| Direct | −.13 | .004 | [−.20, −.06] |
| Total indirect | −.08 | .004 | [−.13, −.04] |
| Hypothesis 1: Time 1 PTSD severity → Sensitivity to relationship threat cues → Time 2 relationship adjustment | −.04 | .012 | [−.06, −.01] |
| Hypothesis 2: Time 1 PTSD severity → Sensitivity to relationship incentive cues → Time 2 relationship adjustment | −.05 | .096 | [−.09, .00] |
| Exploratory indirect paths | |||
| Time 1 PTSD severity→ Sensitivity to relationship threat cues → Time 2 PTSD severity | .04 | .004 | [.02, .06] |
| Time 1 PTSD severity→ Sensitivity to relationship incentive cues → Time 2 PTSD severity | .02 | .105 | [.00, .04] |
| Time 1 relationship adjustment → Sensitivity to relationship threat cues → Time 2 relationship adjustment | −.01 | .346 | [−.03, .01] |
| Time 1 relationship adjustment → Sensitivity to relationship incentive cues → Time 2 relationship adjustment | .14 | .000 | [.10, .19] |
Note. CI = confidence interval; PTSD = posttraumatic stress disorder.
Exploratory Objective B: Time 1 Relationship Adjustment → (B1) Relationship Threat Sensitivity/(B2) Relationship Incentive Sensitivity → Time 2 Relationship Adjustment
Time 1 Relationship Adjustment scores predicted Time 2 Relationship Adjustment scores indirectly through decreased incentive sensitivity (β = .14, p < .001), but not through increased threat sensitivity.
Exploratory Objective C: Bidirectional Associations Between PTSD Symptom Severity and Relationship Adjustment
After accounting for all other pathways in the model, moderate to large stability coefficients remained that were statistically significant (i.e., Time 1 Relationship Adjustment → Time 2 Relationship Adjustment; Time 1 PTSD severity → Time 2 PTSD severity). Additionally, Time 1 PTSD symptom severity directly, significantly predicted Time 2 Relationship Adjustment. However, the alternative pathway, Time 1 Relationship Adjustment to Time 2 PTSD symptom severity was not statistically significant.
Discussion
We sought to improve our understanding of the link between PTSD and relationship adjustment among Iraq War veterans through a longitudinal, cross-lagged panel analysis of relationship adjustment and PTSD symptom severity. We examined two hypothesized indirect pathways through which symptoms of PTSD would lead to poorer relationship adjustment 2 years later: (H1) higher threat sensitivity and (H2) lower incentive sensitivity within intimate relationships. We also tested exploratory pathways mediating stability in relationship adjustment (Exploratory Objective A) and PTSD severity (Exploratory Objective B), and examined bidirectional relations between PTSD and relationship adjustment (Exploratory Objective C).
Primary Hypothesis 1: Sensitivity to Relationship Threat Cues
Results supported our first hypothesis. PTSD symptom severity at Time 1 led to changes in relationship adjustment 2 years later through predicting greater threat sensitivity within intimate relationships, such as concerns about making mistakes in relationships, sensitivity to a partner’s anger or criticism, and anxiety about negative things that may happen in one’s relationship. Broad shifts in worldview among those with PTSD (Foa & Kozak, 1986; Foa et al., 1999) along with PTSD-related symptoms of hypervigilance and avoidance may elevate or exacerbate preexisting threat sensitivities within intimate relationships. Threat sensitivity, broadly, has been linked to problems with emotional regulation difficulties, including nonacceptance of negative emotions, perceived lack of access to strategies assisting with emotion regulation, limited emotional clarity, and problems engaging in both goal-directed behavior and impulsive behavior when experiencing distress (Hannan & Orcutt, 2013; Tull et al., 2010). Relatedly, threat sensitivity is linked to avoidance of aversive internal experiences (experiential avoidance; Maack et al., 2012; Pickett et al., 2011). Both poor emotional regulation and experiential avoidance provide pathways between severity of PTSD and threat sensitivity (Hannan & Orcutt, 2013; Maack et al., 2012; Pickett et al., 2011).
Threat sensitivity specifically within relationships is likely toxic through stimulating maladaptive cognitive biases and problematic relationship behavior, including those associated with experiential avoidance and poor emotional regulation. The literature on social avoidance motivation within interpersonal relationships indicates a focus on avoidance goals fuels biased attention toward negative experiences in relationships and cognitive biases toward interpreting neutral social interactions as negative (Elliot et al., 2006; Gable, 2006; Gable et al., 2000; Strachman & Gable, 2006). This chronic negative focus likely erodes satisfaction and closeness in relationships over time (Impett et al., 2010). Maladaptive behaviors may include reductions in necessary risk taking to address relationship issues and to be emotionally vulnerable, consistent with work finding avoidance mediates PTSD and relationship adjustment associations (Creech et al., 2013), as well as increases in rates of impulsive and destructive relationship behavior, consistent with robust associations between PTSD and both emotional and physical relationship abuse (Taft et al., 2011).
While separate from reinforcement sensitivity theory, Carver and Scheier (1998) argued that behavior is a series of attempts to achieve or maintain homeostatic relationships between one’s current status and desired goal/values (e.g., intimacy and affiliation) or antigoals (e.g., trauma exposure, emotional flooding, and feelings of vulnerability or abandonment). Among an individual with PTSD, symptoms and prior trauma histories may shift perceptions of the distance between one’s present state and trauma-related antigoals within one’s intimate relationship, causing a discrepancy-enlarging loop through which an individual works to maximize the discrepancy between his or her current condition and the antigoal, through avoidance and maladaptive relationship behavior.
Primary Hypothesis 2: Sensitivity to Relationship Incentive Cues
Our findings failed to support our second hypothesis, that symptoms of PTSD would erode relationship adjustment over time through attenuated sensitivity to cues of relationship rewards. Prior work has suggested that affective blunting may be a major cause of poor relationship adjustment among those with symptoms of PTSD (e.g., Cook, Riggs, Thompson, Coyne, & Sheikh, 2004; Erbes, Meis, Polusny, & Compton, 2011). While sensitivity to relationship-related incentives was associated with relationship adjustment, it was not significantly associated with Time 1 PTSD symptom severity, when all other variables were included in the model. Initial zero-order associations indicated moderately sized correlations between PTSD severity and poorer relationship-related incentive sensitivity. Consequently, it may be that the association between PTSD severity and relationship incentive sensitivity is best accounted for by co-occurring global relationship strain (i.e., a spurious association) than by a direct predictive relationship from PTSD symptom severity to poorer sensitivity to incentive cues. Further work is needed to determine if this pattern is robust to replication.
Exploratory Indirect Effects
Time 1 PTSD symptom severity significantly predicted Time 2 PTSD symptom severity through greater sensitivity to relationship-related threat cues. The alternative indirect pathway from Time 1 PTSD to Time 2 PTSD through sensitivity to incentive cues in relationships was not statistically significant. Conversely, Time 1 Relationship Adjustment predicted Time 2 Relationship Adjustment through sensitivity to cues of relationship-related incentive, but not through sensitivity to cues of relationship-related punishment. While RITSS variables were assessed at only a single time point (Time 2), this pattern of associations suggests that sensitivity to cues of punishment in intimate relationships is important to understanding the course of PTSD symptoms over time, potentially through maintaining or exacerbating avoidance and hypervigilance symptoms, while incentive sensitivity is more central in understanding fluctuations in relationship adjustment, perhaps through increasing motivation to work at seeking and approaching cues of relationship-related incentives. This finding adds to the literature tying orientation toward approaching social goals to the frequency of positive social events (Gable, 2006) and increased relationship satisfaction, with the latter association mediated by positive emotions (Impett et al., 2010).
Reciprocal Relations Between PTSD Severity and Relationship Adjustment Over Time
Lastly, our findings contribute to the literature examining reciprocal relations between PTSD symptoms and relationship adjustment over time. PTSD symptom severity at Time 1 predicted declines in relationship adjustment over the following 2 years. However, associations examining the alternative pathway, that relationship adjustment at Time 1 predicts changes in PTSD symptom severity 2 year later, were nonsignificant. These findings are consistent with prior work among community (vs. clinical) samples finding that while PTSD symptoms predict declines in relationship adjustment and social support, relationship adjustment does not significantly predict changes in PTSD severity over time (Erbes et al., 2012; King, Taft, King, Hammond, & Stone, 2006). Prior work among participants in treatment trials has found the alternative, that relationship functioning does predict changes in PTSD symptom severity over time (Evans et al., 2009; Tarrier, Sommerfield, & Pilgrim, 1999). These conflicting findings may reflect important differences due to the two types of samples or may suggest that relationship adjustment leads to declines in symptoms of PTSD through enhancing responsivity to treatment, rather than relationship adjustment leading directly to declines in PTSD severity.
Implications
To the best of our knowledge, this is the first published report demonstrating the importance of reinforcement sensitivity in understanding intimate relationship adjustment among returning veterans exposed to combat. Problems in intimate relationships and families are too often prominent among returning veterans’ mental health concerns (Sayers, Farrow, Ross, & Oslin, 2009). Our findings provide longitudinal evidence that elevated sensitivity to cues of relationship-related threats provide a unique pathway through which PTSD symptoms erode relationship adjustment, while sensitivity to cues of relationship incentives can maintain relationship adjustment, despite symptoms of PTSD. This is an important step in improving the sophistication of both theory and interventions geared toward bolstering relationship adjustment among those with PTSD symptoms.
Our findings suggest effective interventions for improving relationship adjustment among returning veterans with PTSD symptoms may be those focused both on encouraging veterans to (1) approach cues of relationship-related goals, through planned positive activities, and (2) despite distress, approach important activities they may perceive as linked to potential punishment (vulnerability, conflict) in a productive way. The success of the first goal is likely independent of symptoms of PTSD. Consistent with Carver and Scheier’s (1998) concept of a discrepancy-reducing loop, if these activities improve contact between an individual and relationship-related goals (i.e., intimacy and affiliation), the frequency of positive feelings, frequency of approach behaviors, and ultimately, relationship adjustment may improve. This may prove a valuable place to start an intervention, as our data indicate that changes in PTSD symptom severity are not necessarily required, prior to improving relationship adjustment, through this pathway. This strategy is consistent with approaches in classic behavioral couple therapy and integrative behavioral couple therapy (Erbes, Polusny, MacDermid, & Compton, 2008; Jacobson & Christensen, 1996), as well as strategies within two emerging cognitive-behavioral couple therapies for PTSD (cognitive-behavioral conjoint therapy for PTSD, CBCT; Monson et al., 2012; Structured Approach Therapy, SAT; Sautter, Glynn, Arseneau, Cretu, & Yufik, 2014).
The second goal is consistent with promoting activity regulated by the Behavioral Inhibition System (BIS; Gray & McNaughton, 2000). The BIS acts as a defensive approach system, detecting conflicts between approach and avoidance, and inhibiting both approach and avoidance, while conducting a risk assessment (Gray & McNaughton, 2000). This system then suppresses or further activates whichever neuropsychological system is appropriate. The role of this system within intimate relationships is understudied and in need of future research, but recent work suggests this system is not largely influenced by symptoms of PTSD (r = .03, ns; Hannan & Orcutt, 2013). Consequently, there may be promise in strategies designed to encourage veterans to approach relationship-related threat cues, despite sensitivity to these cues.
Strategies could include those based in mindfulness, including within Acceptance and Commitment Therapy (Hayes, Strosahl, & Wilson, 2012), dialectical behavior therapy (Linehan, 2015), and acceptance strategies within Integrative Behavioral Couples Therapy (Jacobson & Christensen, 1996). CBCT and SAT are also particularly relevant (Monson et al., 2012; Sautter et al., 2014), as both interventions include assisting couples in understanding links between avoidance, PTSD, and problems in intimate relationships and explicitly target avoidance behaviors in relationships as a path to recovery. While relatively untested, Emotionally Focused Couple Therapy may also prove relevant to addressing these goals in treatment (Johnson, 2002).
Future Research and Limitations
While our longitudinal design assists in addressing the weaknesses of prior work, the present study has several limitations. Our data cannot examine predisposing factors prior to deployment, such as mental health diagnoses, PTSD symptoms, personality traits, or preexisting threat/incentive sensitivities. Preexisting sensitivity to cues associated with punishment and reward may be a shared cause, placing individuals at risk for both PTSD and difficulty in relationships, rather than these sensitivities being influenced by symptoms of PTSD. However, these sensitivities are likely malleable (Bijttebier et al., 2009; Hundt, Nelson-Gray, Kimbrel, Mitchell, & Kwapil, 2007; Shiner & Caspi, 2003) and, thus, may be shifted or altered by trauma exposure, PTSD symptoms, or both.
Also, while survey response rates were within acceptable limits for survey research, our findings may be less generalizable to those of certain groups or with certain demographic factors. Small average differences were found indicating that nonresponders were less likely to be White (5% difference) and, on average, were 2 years younger. On average, they were also somewhat less educated (0.32 points on an 8-point scale) and in somewhat shorter relationships (0.23 points different on a 4-point scale). Findings may apply less to individuals with these characteristics, although group differences were not large. We were also unable to consider the role of gender due to limited numbers of female veterans in the sample.
The RITSS (Laurenceau et al., 2010) is a relatively new measure, and to the best of our knowledge, it is the only established measure assessing incentive and threat sensitivity within romantic relationships. While the initial psychometric work underlying this measure is thorough and encouraging, additional published work is needed to further replicate its reliability and validity. Additionally, the measure does not differentiate between threat sensitivity (and associated fear) and approach-avoidance conflict (and associated anxiety; i.e., BIS; Gray & McNaughton, 2000). Our data are also limited by their reliance on self-report instruments solely from veterans. Future work is needed to consider our findings within a dyadic or multilevel context (e.g., actor-partner interdependence model) in order to consider how one dyad member’s reinforcement sensitives may differentially or jointly influence his or her own and his or her partner’s relationship outcomes. Impett and colleagues (2010) found that it took only one partner with a high avoidance goals for the relationship satisfaction of both dyad members to decline. Additionally, it is possible that veterans’ reinforcement sensitivities would predict PTSD symptoms differently if PTSD was assessed by gold-standard, clinician-administered structured interviews or if reinforcement sensitives were measured through observing couple interactions. Finally, others argue that accurate assessment of reinforcement sensitivity requires primarily neural rather than questionnaire-based methods (DeYoung, 2010; Smillie, 2008a, 2008b). These are all important areas for future research.
A few additional findings are also of note. First, we found notable stability over time in symptoms of PTSD (direct unique path, β = .73). Associations and indirect effects with the other model variables, did not account for this robust relation. This may be due to the relationship-specific nature of all other variables in the model. Second, we found high rates of veterans’ screening positive for relationship discord among our sample (approaching 40% at both time points). Continuing to understand the source of these notable levels of strain is critical to supporting returning veterans and their families.
Contributor Information
Laura A. Meis, Center for Chronic Disease Outcomes Research, Minneapolis Veterans Affairs (VA) Health Care System, Minneapolis, Minnesota, and Department of Medicine, University of Minnesota
Christopher R. Erbes, Center for Chronic Disease Outcomes Research, Minneapolis VA Health Care System, and Department of Psychiatry, University of Minnesota
Paul A. Arbisi, Minneapolis VA Health Care System and Department of Psychiatry, University of Minnesota
David S. DeGarmo, College of Education, University of Oregon
Mark D. Kramer, Minneapolis Veterans Affairs Health Care System, Minneapolis, Minnesota
Shannon M. Kehle-Forbes, Center for Chronic Disease Outcomes Research, Minneapolis VA Health Care System, and Department of Medicine, University of Minnesota
Sandra L. Shallcross, Department of Psychiatry, Hennepin County Medical Center, Minneapolis, Minnesota
Melissa A. Polusny, Center for Chronic Disease Outcomes Research, Minneapolis VA Health Care System, and Department of Psychiatry, University of Minnesota.
References
- Aluja A, & Blanch A. (2011). Neuropsychological Behavioral Inhibition System (BIS) and Behavioral Approach System (BAS) assessment: A shortened sensitivity to punishment and sensitivity to reward questionnaire version (SPSRQ-20). Journal of Personality Assessment, 93, 628–636. 10.1080/00223891.2011.608760 [DOI] [PubMed] [Google Scholar]
- Berry DS, Willingham JK, & Thayer CA (2000). Affect and personality as predictors of conflict and closeness in young adult friendships. Journal of Research in Personality, 34, 84–107. 10.1006/jrpe.1999.2271 [DOI] [Google Scholar]
- Bijttebier P, Beck I, Claes L, & Vandereycken W. (2009). Gray’s Reinforcement Sensitivity Theory as a framework for research on personality-psychopathology associations. Clinical Psychology Review, 29, 421–430. [DOI] [PubMed] [Google Scholar]
- Bolger N, & Zuckerman A. (1995). A framework for studying personality in the stress process. Journal of Personality and Social Psychology, 69, 890–902. 10.1037/0022-3514.69.5.890 [DOI] [PubMed] [Google Scholar]
- Browne MYC, & Cudeck RR (1993). Alternative ways of assessing model fit In Bollen KA & Long JS (Eds.), Testing structural equation models (pp. 136–162). Newberry Park, CA: Sage. [Google Scholar]
- Carver CS, & Scheier MF (1998). On the self-regulation of behavior. New York, NY: Cambridge University Press; 10.1017/CBO9781139174794 [DOI] [Google Scholar]
- Carver CS, Sutton SK, & Scheier MF (2000). Action, emotion, and personality: Emerging conceptual integration. Personality and Social Psychology Bulletin, 26, 741–751. 10.1177/0146167200268008 [DOI] [Google Scholar]
- Carver CS, & White T. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. Journal of Personality and Social Psychology, 67, 319–333. 10.1037/0022-3514.67.2.319 [DOI] [Google Scholar]
- Cloninger CR (1987). A systematic method of clinical description and classification of personality variants: A proposal. Archives of General Psychiatry, 44, 573–588. [DOI] [PubMed] [Google Scholar]
- Contractor AA, Elhai JD, Ractliffe KC, & Forbes D. (2013). PTSD’s underlying symptom dimensions and relations with behavioral inhibition and activation. Journal of Anxiety Disorders, 27, 645–651. 10.1016/j.janxdis.2013.07.007 [DOI] [PubMed] [Google Scholar]
- Cook JM, Riggs DS, Thompson R, Coyne JC, & Sheikh JI (2004). Posttraumatic stress disorder and current relationship functioning among World War II ex-prisoners of war. Journal of Family Psychology, 18, 36–45. 10.1037/0893-3200.18.136 [DOI] [PubMed] [Google Scholar]
- Creech SK, Benzer JK, Liebsack BK, Proctor S, & Taft CT (2013). Impact of coping style and PTSD on family functioning after deployment in Operation Desert Shield/Storm returnees. Journal of Traumatic Stress, 26, 507–511. 10.1002/jts.21823 [DOI] [PubMed] [Google Scholar]
- Davidson RJ (1988). EEG measures of cerebral asymmetry: Conceptual and methodological issues. International Journal of Neuroscience, 39, 71–89. 10.3109/00207458808985694 [DOI] [PubMed] [Google Scholar]
- Depue RA, Krauss SP, & Spoont MR (1987). A two-dimensional threshold model of seasonal bipolar affective disorder In Magnusson D. & Ohman A. (Eds.), Psychopathology: An interactional perspective (pp. 95–123). Orlando, FL: Academic Press. [Google Scholar]
- DeYoung CG (2010). Personality neuroscience and the biology of traits. Social and Personality Psychology Compass, 4, 1165–1180. 10.1111/j.1751-9004.2010.00327.x [DOI] [Google Scholar]
- Dillman DA, Smyth JD, & Christian LM (2014). Internet, phone, mail, and mixed mode surveys: The tailored design method (4th ed). Hoboken, NJ: Wiley. [Google Scholar]
- Elliot AJ, Gable SL, & Mapes RR (2006). Approach and avoidance motivation in the social domain. Personality and Social Psychology Bulletin, 32, 378–391. 10.1177/0146167205282153 [DOI] [PubMed] [Google Scholar]
- Epstein S. (1979). The stability of behavior: I. On predicting most of the people much of the time. Journal of Personality and Social Psychology, 37, 1097–1126. 10.1037/0022-3514.37.7T097 [DOI] [Google Scholar]
- Epstein S. (1980). The stability of behavior: II. Implications for psychological research. American Psychologist, 35, 790–806. 10.1037/0003-066X.35.9.790 [DOI] [Google Scholar]
- Erbes CR, Meis LA, Polusny MA, & Compton JS (2011). Couple adjustment and PTSD symptoms in National Guard veterans of the Iraq war. Journal of Family Psychology, 25, 479–487. 10.1037/a0024007 [DOI] [PubMed] [Google Scholar]
- Erbes CR, Meis LA, Polusny MA, Compton JS, & MacDermid Wadsworth S. (2012). An examination of PTSD symptoms and relationship functioning in U. S. soldiers of the Iraq War over time. Journal of Traumatic Stress, 25, 187–190. 10.1002/jts.21689 [DOI] [PubMed] [Google Scholar]
- Erbes CR, Polusny MA, MacDermid S, & Compton J. (2008). Couple therapy with combat veterans and their partners. Journal of Clinical Psychology: In Session, 64, 972–983. 10.1002/jcpl.20521 [DOI] [PubMed] [Google Scholar]
- Evans L, Cowlishaw S, & Hopwood M. (2009). Family functioning predicts outcomes for veterans in treatment for chronic posttraumatic stress disorder. Journal of Family Psychology, 23, 531–539. 10.1037/a0015877 [DOI] [PubMed] [Google Scholar]
- Ferrier-Auerbach AG, Erbes CR, Polusny MA, Rath M, & Sponheim S. (2010). Predictors of emotional distress reported by soldiers in the combat zone. Journal of Psychiatric Research, 44, 470–476. 10.1016/j.jpsychires.2009.10.010 [DOI] [PubMed] [Google Scholar]
- Foa EB, Ehlers A, Clark DM, Tolin DF, & Orsillo SM (1999). The Posttraumatic Cognitions Inventory (PTCI): Development and validation. Psychological Assessment, 11, 303–314. 10.1037/1040-3590.11.3.303 [DOI] [Google Scholar]
- Foa EB, & Kozak MJ (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99, 20–35. [PubMed] [Google Scholar]
- Funk JL, & Rogge RD (2007). Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the Couples Satisfaction Index. Journal of Family Psychology, 21, 572–583. 10.1037/0893-3200.21.4.572 [DOI] [PubMed] [Google Scholar]
- Gable SL (2006). Approach and avoidance social motives and goals. Journal of Personality, 74, 175–222. 10.1111/j.1467-6494.2005.00373.x [DOI] [PubMed] [Google Scholar]
- Gable SL, Reis HT, & Elliot AJ (2000). Behavioral activation and inhibition in everyday life. Journal of Personality and Social Psychology, 78, 1135–1149. 10.1037/0022-3514.78.6T135 [DOI] [PubMed] [Google Scholar]
- Gray JA (1981). A critique of Eysenck’s theory of personality In Eysenck HJ (Ed.), A model forpersonality (pp. 246–276). Berlin, Germany: Springer-Verlag; 10.1007/978-3-642-67783-0_8 [DOI] [Google Scholar]
- Gray JA (1987). Perspectives on anxiety and impulsivity: A commentary. Journal of Research in Personality, 21, 493–509. 10.1016/0092-6566(87)90036-5 [DOI] [Google Scholar]
- Gray JA, & McNaughton N. (2000). The neuropsychology of anxiety. Oxford, UK: Oxford University Press. [Google Scholar]
- Hannan SM, & Orcutt HK (2013). Emotion dysregulation as a partial mediator between reinforcement sensitivity and posttraumatic stress symptoms. Personality and Individual Differences, 55, 574–578. 10.1016/j.paid.2013.04.028 [DOI] [Google Scholar]
- Hayes SC, Strosahl KD, & Wilson KG (2012). Acceptance and commitment therapy: The process and practice of mindful change (2nd ed). New York, NY: Guilford Press. [Google Scholar]
- Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, & Koffman RL (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine, 351, 13–22. 10.1056/NEJMoa040603 [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Hundt NE, Nelson-Gray RO, Kimbrel NE, Mitchell JT, & Kwapil TR (2007). The interaction of reinforcement sensitivity and life events in the prediction of anhedonic depression and mixed anxiety-depressive symptoms. Personality and Individual Differences, 43, 1001–1012. 10.1016/j.paid.2007.02.021 [DOI] [Google Scholar]
- Hunsley J, Pinsent C, Lefebvre M, James-Tanner S, & Vito D. (1995). Construct validity of the short forms of the Dyadic Adjustment Scale. Family Relations, 44, 231–237. 10.2307/585520 [DOI] [Google Scholar]
- Impett EA, Gordon AM, Kogan A, Oveis C, Gable SL, & Keltner D. (2010). Moving toward more perfect unions: Daily and long-term consequences of approach and avoidance goals in romantic relationships. Journal of Personality and Social Psychology, 99, 948–963. 10.1037/a0020271 [DOI] [PubMed] [Google Scholar]
- Jacobson NS, & Christensen A. (1996). Integrative couple therapy: Promoting acceptance and change. New York, NY: Norton. [Google Scholar]
- Johnson SM (2002). Emotionally focused couple therapy with trauma survivors: Strengthening attachment bonds. New York, NY: Guilford Press. [Google Scholar]
- Johnson S, Turner R, & Iwata N. (2003). BIS/BAS levels and psychiatric disorder: An epidemiological study. Journal of Psychopathology and Behavioral Assessment, 25, 25–36. 10.1023/A:1022247919288 [DOI] [Google Scholar]
- Jordan BK, Marmar CR, Fairbank JA, Schlenger WE, Kulka RA, Hough RL, & Weiss DS (1992). Problems in families of male Vietnam veterans with posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 60, 916–926. 10.1037/0022-006X.60.6.916 [DOI] [PubMed] [Google Scholar]
- King DW, Taft C, King LA, Hammond C, & Stone ER (2006). Directionality of the association between social support and posttraumatic stress disorder: A longitudinal investigation. Journal of Applied Social Psychology, 36, 2980–2992. 10.1111/j.0021-9029.2006.00138.x [DOI] [Google Scholar]
- Laurenceau J, Klienman BM, Kaczynski KJ, & Carver CS (2010). Assessment of relationship-specific incentive and threat sensitivities: Predicting satisfaction and affect in adult intimate relationships. Psychological Assessment, 22, 407–419. [DOI] [PubMed] [Google Scholar]
- Linehan MM (2015). DBT skills training manual (2nd ed). New York, NY: Guilford Press. [Google Scholar]
- Maack DJ, Tull MT, & Gratz KL (2012). Experiential avoidance mediates the association between behavioral inhibition and posttraumatic stress disorder. Cognitive Therapy and Research, 36, 407–416. 10.1007/s10608-011-9362-2 [DOI] [Google Scholar]
- Meis LA, Barry RA, Kehle SM, Erbes CR, & Polusny MA (2010). Relationship adjustment, PTSD symptoms, and treatment utilization among coupled National Guard soldiers deployed to Iraq. Journal of Family Psychology, 24, 560–567. 10.1037/a0020925 [DOI] [PubMed] [Google Scholar]
- Meredith W. (1993). Measurement invariance, factor analysis, and factorial invariance. Psychometrika, 58, 525–543. 10.1007/BF02294825 [DOI] [Google Scholar]
- Meyer B, Olivier LE, & Roth D. (2005). Please don’t leave me! BIS/BAS, attachment styles, and responses to a relationship threat. Personality and Individual Differences, 38, 151–162. 10.1016/j.paid.2004.03.016 [DOI] [Google Scholar]
- Monson CM, Fredman SJ, Macdonald A, Purkay-Martin ND, Resick PA, & Schnurr PP (2012). Effect of cognitive-behavioral couple therapy for PTSD: A randomized controlled trial. Journal of the American Medical Association, 308, 700–709. 10.1001/jama.2012.9307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2012). Mplus user’s guide (7th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Myers CE, Vanmeenen KM, & Servatius RJ (2012). Behavioral inhibition and PTSD symptoms in veterans. Psychiatry Research, 196, 271–276. 10.1016/j.psychres.2011.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peugh JL, & Enders CK (2004). Missing data in educational research: A review of reporting practices and suggestions for improvement. Review of Educational Research, 74, 525–556. 10.3102/00346543074004525 [DOI] [Google Scholar]
- Pickett SM, Bardeen JR, & Orcutt HK (2011). Experiential avoidance as a moderator of the relationship between behavioral inhibition system sensitivity and posttraumatic stress symptoms. Journal of Anxiety Disorders, 25, 1038–1045. 10.1016/jjanxdis.2011.06.013 [DOI] [PubMed] [Google Scholar]
- Pinto-Meza A, Caseras X, Soler J, Puigdemont D, Perez V, & Torrubia R. (2006). Behavioral inhibition and behavioral activation systems in current and recovered major depression participants. Personality and Individual Differences, 40, 215–226. 10.1016/j.paid.2005.06.021 [DOI] [Google Scholar]
- Polusny MA, Kehle SM, Nelson NW, Erbes CR, Arbisi PA, & Thuras P. (2011). Longitudinal effects of mild traumatic brain injury and posttraumatic stress disorder comorbidity on postdeployment outcomes in National Guard soldiers deployed to Iraq. Archives of General Psychiatry, 68, 79–89. 10.1001/archgenpsychiatry.2010.172 [DOI] [PubMed] [Google Scholar]
- Reis HT, Capobianco A, & Tsai FF (2002). Finding the person in personal relationships. Journal of Personality, 70, 813–850. 10.1111/1467-6494.05025 [DOI] [PubMed] [Google Scholar]
- Ruggiero KJ, Del Ben K, Scotti JR, & Rabalais AE (2003). Psychometric properties of the PTSD Checklist—Civilian Version. Journal of Traumatic Stress, 16, 495–502. 10.1023/A:1025714729117 [DOI] [PubMed] [Google Scholar]
- Sautter FJ, Glynn SM, Arseneau JR, Cretu JB, & Yufik T. (2014). Structured approach therapy for PTSD in returning veterans and their partners: Pilot findings. Psychological Trauma: Theory, Research, Practice, and Policy, 6(Suppl. 1), S66–S72. 10.1037/a0036762 [DOI] [Google Scholar]
- Sayers SL, Farrow VA, Ross J, & Oslin DW (2009). Family problems among recently returned military veterans referred for a mental health evaluation. Journal of Clinical Psychiatry, 70, 163–170. 10.4088/JCP.07m03863 [DOI] [PubMed] [Google Scholar]
- Schell TL, & Marshall GN (2008). Survey of individuals previously deployed for OEF/OIF In Tanielian T. & Jaycox LH (Eds.), Invisible wounds of war: Psychological and cognitive injuries, their consequences, and service to assist recovery (pp. 87–115). Santa Monica, CA: RAND. [Google Scholar]
- Sharpley CF, & Cross DG (1982). A psychometric evaluation of the Spanier Dyadic Adjustment Scale. Journal of Marriage and the Family, 44, 739–741. 10.2307/351594 [DOI] [Google Scholar]
- Sharpley CF, & Rogers HJ (1984). Preliminary validation of the Abbreviated Spanier Dyadic Adjustment Scale: Some psychometric data regarding a screening test of marital adjustment. Educational and Psychological Measurement, 44, 1045–1049. 10.1177/0013164484444029 [DOI] [Google Scholar]
- Shiner R, & Caspi A. (2003). Personality differences in childhood and adolescence: Measurement, development, and consequences. Journal of Child Psychology and Psychiatry, 44, 2–32. 10.1111/1469-7610.00101 [DOI] [PubMed] [Google Scholar]
- Smillie LD (2008a). The conceptualisation, measurement and scope of reinforcement sensitivity in the context of a neuroscience of personality. European Journal of Personality, 22, 411–425. 10.1002/per.687 [DOI] [Google Scholar]
- Smillie LD (2008b). What is reinforcement sensitivity? Neuroscience paradigms for approach-avoidance process theories of personality. European Journal of Personality, 22, 359–384. 10.1016/j.paid.2004.09.013 [DOI] [Google Scholar]
- Strachman A, & Gable SL (2006). What you want (and do not want) affects what you see (and do not see): Avoidance social goals and social events. Personality and Social Psychology Bulletin, 32, 1446–1458. 10.1177/0146167206291007 [DOI] [PubMed] [Google Scholar]
- Taft CT, Watkins LE, Stafford J, Street AE, & Monson CM (2011). Posttraumatic stress disorder and intimate relationship problems: A meta-analysis. Journal of Consulting and Clinical Psychology, 79, 22–33. 10.1037/a0022196 [DOI] [PubMed] [Google Scholar]
- Tarrier N, Sommerfield C, & Pilgrim H. (1999). Relatives’ expressed emotion (EE) and PTSD treatment outcome. Psychological Medicine, 29, 801–811. 10.1017/S0033291799008569 [DOI] [PubMed] [Google Scholar]
- Tull MT, Gratz KL, Latzman RD, Kimbrel NA, & Lejuez CW (2010). Reinforcement sensitivity theory and emotion regulation difficulties: A multimodal investigation. Personality and Individual Differences, 49, 989–994. 10.1016/j.paid.2010.08.010 [DOI] [Google Scholar]
- Weathers FW, Huska J, & Keane T. (1991). The PTSD Checklist Military Version (PCL-M). Boson, MA: National Center for Posttraumatic Stress Disorder. [Google Scholar]