

Abstract
Context
Comprehensive injury-prevention training (plyometric, agility, balance, and core-stability exercises) has been shown to decrease sport-related injury. The relationship between trunk control and sport-related injury has been emphasized; however, the isolated effects of core-muscle training are unclear.
Objective
To investigate the effect of a simple 8-week core-muscle–training program on the neuromuscular control of the lower limb and trunk during jump landing and single-legged squatting.
Design
Controlled laboratory study.
Setting
Laboratory.
Patients or Other Participants
Seventeen female collegiate basketball players were randomly divided into training (n = 9; age = 19.7 ± 0.9 years) and control (n = 8; age = 20.3 ± 2.5 years) groups.
Intervention(s)
The training group completed the core-muscle–training program in addition to daily practice, and the control group performed only daily practice. Kinematic and kinetic data during a drop-jump test and single-legged squat were acquired using a 3-dimensional motion-analysis system.
Main Outcome Measure(s)
Three-dimensional hip, knee, and trunk kinematics; knee kinetics; and isokinetic muscle strength were measured at the pretraining and posttraining phases.
Results
For the drop-jump test, the maximal trunk-flexion angle increased (P = .008), and peak knee-valgus moment (P = .008) decreased in the training group. For the single-legged squat, the peak trunk-flexion angle increased (P = .04), and the total amount of trunk lateral-inclination angle (P = .02) and peak knee-valgus moment (P = .008) decreased in the training group. We observed no changes in the control group.
Conclusions
A consecutive 8-week core-muscle–training program improved lower limb and trunk biomechanics. These altered biomechanical patterns could be favorable to preventing sport-related injuries.
Keywords: anterior cruciate ligament injury, drop-jump test, single-legged squat
Key Points
Simple core-muscle training improved neuromuscular control of the trunk and lower limbs in collegiate female basketball players.
Performing this training program may reduce the risk of noncontact anterior cruciate ligament injuries in these athletes.
Core-muscle training seems to be an essential element to incorporate in an anterior cruciate ligament injury-prevention program, but more research is needed to determine whether this training program sufficiently reduces the incidence of anterior cruciate ligament injuries in this population.
Sex differences in the incidence of anterior cruciate ligament (ACL) injury have been widely recognized, with female athletes experiencing an incidence several times higher than male athletes during sport activities.1,2 The actual mechanism of ACL injury is still unclear; however, using the model-based, image-matching technique, Koga et al3 showed that extreme knee valgus and tibial internal rotation was likely the inciting mechanism at the time of noncontact injury. Hewett et al2 reported that greater knee-valgus angle and moment during a jump-landing task were risk factors for ACL injury and demonstrated a relationship between the ACL injury mechanism and knee valgus. Hewett et al4 suggested that 4 neuromuscular imbalances contributed to ACL injury in female athletes: ligament dominance, quadriceps dominance, leg dominance, and trunk dominance. Ligament dominance was defined as the neuromuscular imbalance responsible for valgus collapse. Supporting muscular groups do not adequately contract and absorb the ground reaction forces. Quadriceps dominance referred to the tendency to stabilize the knee joint primarily using the quadriceps. Landing from a jump with less knee flexion increases the potential to sustain an ACL injury. Leg dominance was defined as side-to-side asymmetry of the lower extremities, including muscle recruitment, strength, and flexibility. Trunk dominance described the inability to precisely control the trunk in 3-dimensional space. Unlike anatomic factors, these factors can theoretically be modified by appropriate interventions, so recent researchers have emphasized the importance of ACL injury prevention and reported the efficacy of prevention programs.
Most ACL injury-prevention programs have successfully reduced the risk of ACL injury. In their meta-analysis, Taylor et al5 observed a reduction in all ACL injuries (odds ratio = 0.61) and noncontact ACL injuries (odds ratio = 0.35) when the incidence was expressed relative to player-seasons. In another meta-analysis, Lopes et al6 found that ACL injury-prevention programs might improve biomechanics related to the quadriceps- and ligament-dominance theories. Most of these neuromuscular-training programs for ACL injury prevention consist of multiple components, such as plyometrics, balance, agility, flexibility, and strengthening, to address various aspects of neuromuscular control.7–11 Steffen et al12 noted that an ACL injury-prevention program performed with a high level of compliance resulted in a decreased risk of ACL injury. To increase athletes' adherence to a prevention program, the specific elements in the neuromuscular training that contribute to the reduced risk of ACL injury need to be clarified, and more efficient programs must be developed.
Core-stability exercise is one of the most favored components that are frequently included in ACL injury-prevention programs. Given that the dynamic motion of the trunk and hip joint affects knee-joint biomechanics during physical activities, neuromuscular-control deficits in the trunk and hip joint might increase the ACL injury risk.13–17 In their cohort study, Zazulak et al13 demonstrated that core stability predicted ACL injury in female athletes. Khayambashi et al17 reported that hip-abduction and external-rotation muscle strength predicted noncontact ACL injury in competitive athletes. Knee-valgus motion seemed to have resulted in a complex kinetic chain from the trunk to the pelvis and the lower limb. For ACL injury prevention, increasing trunk and pelvic stability was considered to reduce the ACL injury risk.
From these findings, we hypothesized that core-muscle training modifies the neuromuscular control of the trunk and lower limb, leading to a decreased risk of ACL injury. Therefore, the purpose of our study was to investigate the effect of a single application of simple core-muscle training on neuromuscular control of the lower limb and trunk during jump landing and single-legged squatting in female collegiate basketball players.
METHODS
Participants
Seventeen female basketball players who belonged to 1 collegiate team were recruited from Hirosaki University. We randomly distributed participants to either the training group (n = 9) or the control group (n = 8) using block randomization, which provided a better guarantee that both groups would be of nearly equal size (Table 1). The block length was set at 4 to limit a possible imbalance and to avoid predictability toward the end of the sequence in a block. The allocation in each block was defined using Excel (version 2013; Microsoft Corp, Redmond, WA). The training group was instructed to add the core-muscle–training program to regular practice, and the control group was instructed to maintain regular practice. Volunteers who had a history of substantial traumatic injury or any clinical symptoms in the lower limbs were excluded. We observed no differences in the demographic data between groups (Table 1). All participants provided written informed consent, and the Hirosaki University Graduate School of Medicine Review Board approved the study.
Table 1.
Anthropometric Data of the Training (n = 9) and Control (n = 8) Groups (Mean ± SD)
| Characteristic |
Group |
U Value |
P Value |
|
| Training |
Control |
|||
| Age, y | 19.7 ± 0.9 | 20.3 ± 2.5 | 35.5 | .96 |
| Height, cm | 160.6 ± 4.9 | 158.8 ± 2.9 | 29.0 | .54 |
| Mass, kg | 54.7 ± 5.6 | 52.5 ± 2.9 | 28.5 | .48 |
Training Program
The simple core-muscle–training program was designed to consist of only 3 components from the Federation Internationale de Football Association 11+ (FIFA11+) program: bench, side bench, and Nordic hamstrings (Table 2; Figure 1).18–20 The training group participated in the program 4 times or more each week for 8 weeks. The training volume was 2 sets of the core-muscle–training program performed before each regular practice. Training intensity was set to 2 or 3 levels and increased according to the degree of each participant's achievement. Before the training, an orthopaedic surgeon (S.S.) instructed participants how to perform each exercise using appropriate and safe postures, and he monitored the training at least once each week. We determined participants' training compliance through weekly self-reported questionnaires.
Table 2.
Figure 1.
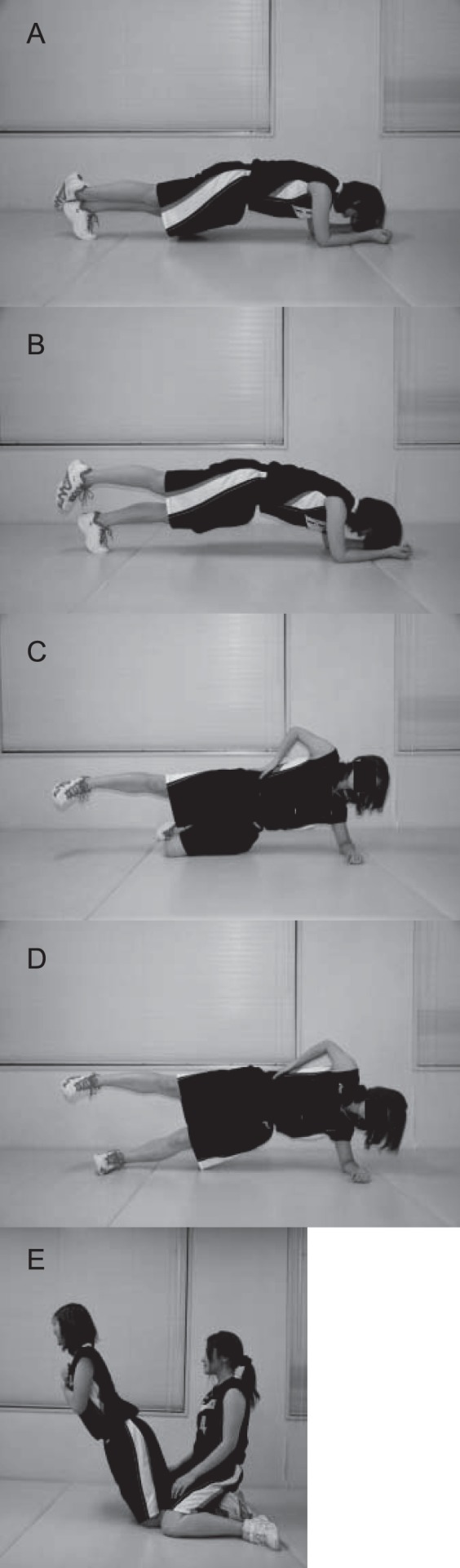
A–E. Core-muscle–training program.
Motion Analysis
Trial data were collected with a 3-dimensional motion-analysis system (Vicon Motion Systems Ltd, Oxford, United Kingdom) using 7 infrared cameras. Kinematic data were sampled at 120 Hz and recorded digitally on a personal computer with a dual Pentium III processor (Intel Corp, Santa Clara, CA) with a base frequency of 1 GHz. The ground reaction force was collected at 1200 Hz using a calibrated and leveled force plate (model OR6-6-1; AMTI, Watertown, MA) embedded in the floor and synchronized with the motion-analysis system for simultaneous collection. Thirty-five retroreflective markers with a 25-mm diameter were placed on the following anatomic landmarks: front of the head, back of the head, right back of the head, seventh cervical vertebrae, 10th thoracic vertebrae, clavicle, sternum, right scapula, acromioclavicular joint, lateral epicondyle of the humerus, thumb and fifth finger sides of the wrist, head of the second metacarpal, anterior-superior iliac spine, posterior-superior iliac spine, midthigh, lateral epicondyle of the femur, middle of the shank, lateral malleolus of the ankle, heel, and head of the second metatarsal. We recorded the 3-dimensional marker trajectories according to Plug-in Gait (Vicon Motion Systems) marker placement and calculated the kinematic and kinetic variables using Plug-in Gait in Vicon Workstation (version 4.6; Vicon Motion Systems). We used inverse-dynamics analyses to calculate external joint moments from the kinematic data and ground reaction force with Plug-in Gait. Marker-trajectory data were filtered using the Woltring smoothing spline in the cubic mode.21 The force-plate data filtered through a low-pass Butterworth digital filter at a cutoff frequency of 12 Hz. All kinetic data were normalized to body weight (in kg) and height (in m). Kinematic and kinetic data of the lower limb and trunk were evaluated during the drop-jump test (DJT)22 and single-legged squat (SLS). To perform the DJT, participants dropped directly from a 31-cm high box that had reflective markers placed on the corners and immediately attempted a maximal vertical jump. Kinematic and kinetic data from initial contact on the floor to toe-off were operationally defined as the stance phase. To perform the SLS, participants were instructed to flex the knee joint gradually from single-legged standing with upright posture to a depth from which they were able to return to the starting position smoothly while holding their hands on their hips and focusing straight ahead during the squat. A trial was considered invalid if the other limb was held in front of the body during the squat, touched the ground, or caused loss of balance. To exclude the effects of fatigue, participants rested after each trial and performed SLS using both the right and left limbs. They performed 3 trials after practicing several times, and the average of the right- and left-side data for the DJT and SLS was used for statistical analysis. To avoid any coaching effects, we provided neither information about the lower limb or trunk position or alignment nor any specific technical instruction to the participants. Kinematic and kinetic data were evaluated during the entire stance phase from initial contact to toe-off. Kinematic data of the maximal flexion-extension, adduction-abduction, and internal-external–rotation angles of the hip; the maximal flexion-extension and varus-valgus angles of the knee; the maximal flexion-extension angle of the trunk; and the total amount of right to left lateral inclination angle of the trunk during the stance phase were calculated for each trial. In this study, trunk-flexion angle and lateral-inclination angle were defined as the thorax angle with respect to the perpendicular axis in the sagittal and transverse planes, respectively. The kinetic data were measured as the peak knee-valgus moment during 1 trial of DJT and SLS. The first peak knee-valgus moment after initial contact and the time between initial contact and the first peak of knee-valgus moment were also calculated in the DJT.
Isokinetic Muscle-Strength Measurement
Hip-flexor and -abductor, knee-flexor and -extensor, and trunk-extensor and -flexor strength were assessed using the Kin-Com 500 H (Chattex Corp, Chattanooga, TN). All strength values were evaluated as isokinetic peak torque concentric contractions.23 Angular velocity was set at 60°/s and 120°/s in the measurements of hip- and knee-muscle strength and 20°/s and 40°/s in the measurement of trunk-muscle strength, according to the protocol that was established in advance. Participants lay on a table, and hip-flexor and -abductor strength were measured in the supine and lateral positions, respectively. We fixed the pelvis to the table with a dedicated belt and attached a measuring pad to the distal femur during the hip-strength test. For the knee-muscle–strength test, participants were seated, and the measuring pad was attached to the calf to measure knee-flexor strength and to the anterior distal tibia to measure knee-extensor strength. To avoid hip and femur movement, the thigh was fixed to the seat during the measurement of knee-flexor and -extensor strength. For the trunk-muscle–strength test, participants were seated, and the rotation axis of the lever was adjusted to the L5-S1 level. The measuring pad was attached to the manubrium to measure trunk-flexor strength and the scapular spine to measure trunk-extensor strength. The pelvis was fixed to the seat. To exclude the influence of lower limb muscle contraction, we attached a dedicated pad to the anterior tibia and instructed participants to raise both feet off the ground. All muscle-strength data were normalized to body weight (in kg). A minimum 30- to 60-second rest period was provided between efforts to allow muscle recovery.24 The best curve as determined by the highest peak was recorded. Strength was measured in both limbs, and the average of the right and left limbs was calculated.
Statistical Analysis
All kinematic and kinetic data and isokinetic muscle strength were measured at 2 points: pretraining and posttraining. Comparisons between pretraining and posttraining in each group were performed with the Wilcoxon signed-rank test, and groups were compared using the Mann-Whitney U test with the α level set at .05. The normality of the variables was determined using Kolmogorov-Smirnov statistics. We used nonparametric statistics and described the results of kinematic, kinetic, and isokinetic muscle strength by the median and interquartile range (IQR) because some variables were nonnormally distributed. All statistical analyses were conducted using SPSS (version 16.0; SPSS Inc, Chicago, IL).
RESULTS
The training group performed the 8-week core-muscle–training program an average of 4.7 times per week. During this training period, we observed no incidence of acute or overuse lower limb injury. No differences between groups before the intervention were found for any kinematic, kinetic, or isokinetic strength measurements.
Drop-Jump Test
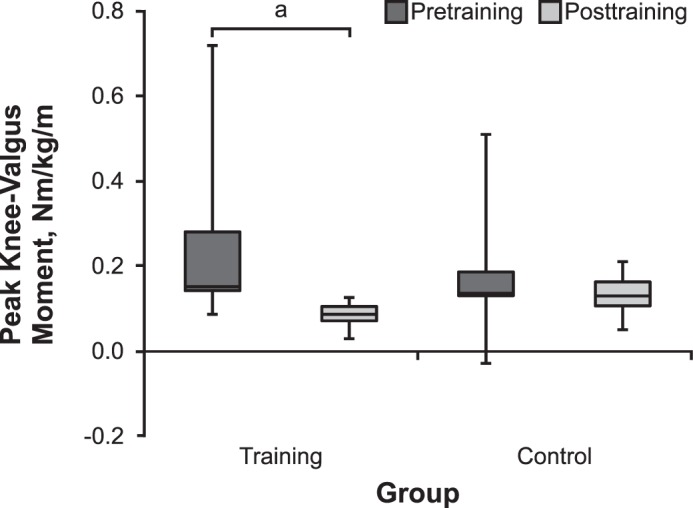
We found no change in the maximal hip-flexion, hip-adduction, or hip internal-rotation angle or knee-flexion or knee-valgus angle between pretraining and posttraining in the groups (Figures 2 and 3; Table 3). In the training group, the maximal trunk-flexion angle increased from 37.7° (IQR = 30.5°–46.2°) at pretraining to 47.7° (IQR = 44.0°–52.0°) at posttraining (P = .008). We demonstrated no change in the control group from pretraining (32.5°; IQR = 23.7°–45.1°) to posttraining (40.2°; IQR = 33.5°–46.4°; P = .48; Table 3). The total trunk lateral-inclination angle during the stance phase was not different in the training group from pretraining (3.2°; IQR = 1.4°–3.6°) to posttraining (1.7°; IQR = 1.6°–2.4°; P = .17) or in the control group from pretraining (3.1°; IQR = 2.4°–5.0°) to posttraining (3.2°; IQR = 2.2°–3.9°; P = .58), but it was smaller in the training group than in the control group at posttraining (P = .03; Figure 4). In the training group, the peak knee-valgus moment decreased from 0.46 Nm/kg/m (IQR = 0.23–0.55 Nm/kg/m) at pretraining to 0.16 Nm/kg/m (IQR = 0.09–0.38 Nm/kg/m) at posttraining (P = .008). In contrast, we noted no change from pretraining (0.20 Nm/kg/m; IQR = 0.18–0.48 Nm/kg/m) to posttraining (0.30 Nm/kg/m; IQR = 0.23–0.46 Nm/kg/m) in the control group (P = .78; Figure 5). In the training group, the first peak of knee-valgus moment after initial contact decreased from 0.27 Nm/kg/m (IQR = 0.23–0.46 Nm/kg/m; average = 51 ± 15 milliseconds after initial contact) at pretraining to 0.06 Nm/kg/m (IQR = 0.01–0.18 Nm/kg/m; average = 26 ± 3 milliseconds after initial contact) at posttraining (P = .008; Figure 6). No difference was evident in the control group from pretraining (0.20 Nm/kg/m; IQR = 0.05–0.29 Nm/kg/m; average = 25 ± 5 milliseconds after initial contact) to posttraining (0.17 Nm/kg/m; IQR = 0.05–0.30 Nm/kg/m; average 28 ± 8 milliseconds after initial contact; P = .89; Figure 6).
Figure 2.

Pretraining and posttraining kinematics (mean ± standard deviation) of the training group in the drop-jump test. A, Hip flexion-extension angle. B, Hip adduction-abduction angle. C, Hip internal-external–rotation angle. D, Knee flexion-extension angle. E, Knee varus-valgus angle. F, Trunk flexion-extension angle.
Figure 3.

Pretraining and posttraining kinematics (mean ± standard deviation) of the control group in the drop-jump test. A, Hip flexion-extension angle. B, Hip adduction-abduction angle. C, Hip internal-external–rotation angle. D, Knee flexion-extension angle. E, Knee varus-valgus angle. F, Trunk flexion-extension angle.
Table 3.
Peak Values of Kinematic Data for the Drop-Jump Test
| Variable |
Training Group, ° |
Control Group, ° |
||||
| Median (Interquartile Range) |
P Value |
Median (Interquartile Range) |
P Value |
|||
| Pretraining |
Posttraining |
Pretraining |
Posttraining |
|||
| Hip | ||||||
| Flexion | 74.0 (71.1–79.8) | 78.7 (76.7–82.5) | .44 | 82.6 (78.6–87.7) | 83.1 (78.7–86.2) | .78 |
| Adduction | 2.2 (−1.7–3.1) | 1.0 (−1.4–2.7) | .44 | 0.4 (−1.1–1.2) | 0.7 (−0.8–1.9) | .07 |
| Internal rotation | 8.0 (5.6–10.3) | 4.8 (4.0–7.5) | .09 | 7.3 (0.8–11.8) | 4.4 (1.8–8.7) | .40 |
| Knee | ||||||
| Flexion | 96.5 (92.6–99.9) | 99.1 (94.3–101.3) | .37 | 100.7 (95.6–106.7) | 104.7 (94.9–107.8) | .89 |
| Valgus | 5.8 (3.9–6.6) | 2.6 (1.9–5.8) | .11 | 5.3 (4.0–5.9) | 6.6 (3.6–9.2) | .40 |
| Trunk | ||||||
| Flexion | 37.7 (30.5–46.2) | 47.7 (44.0–52.0) | .008a | 32.5 (23.7–45.1) | 40.2 (33.5–46.4) | .48 |
Indicates difference (P < .05).
Figure 4.
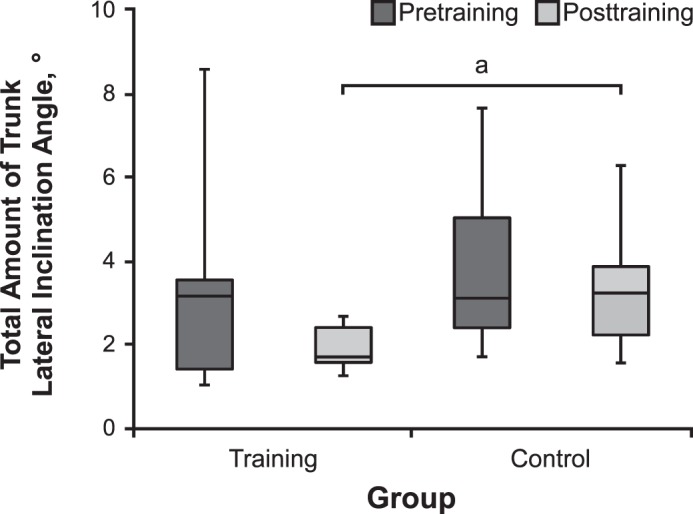
The total amount of trunk lateral inclination angle in the drop-jump test (median value with interquartile range). a P < .05.
Figure 5.
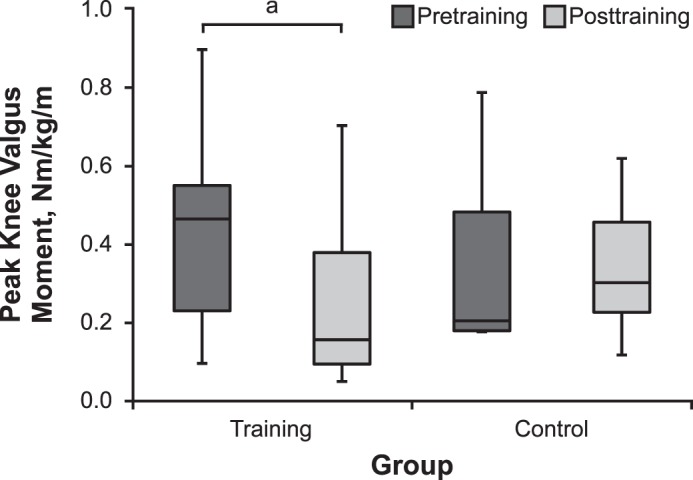
The peak knee-valgus moment in the drop-jump test (median value with interquartile range). a P < .05.
Figure 6.

The knee-valgus moment from initial contact to the floor to toe-off (A, training group; B, control group) and the first peak of knee valgus moment in the drop-jump test (C, median value with interquartile range). a P < .05.
Single-Legged Squat Test
In the training group, we observed increases in the maximal hip-flexion angle from 61.6° (IQR = 56.1°–67.9°) at pretraining to 69.1° (IQR = 63.7°–77.1°) at posttraining (P = .04), knee-flexion angle from 74.5° (IQR = 66.8°–82.9°) at pretraining to 82.5° (IQR = 76.2°–84.7°) at posttraining (P = .04), and trunk-flexion angle from 22.3° (IQR = 15.6°–30.8°) at pretraining to 32.2° (IQR = 27.8°–38.2°) at posttraining (P = .04). Decreases occurred in the maximal hip internal-rotation angle from 14.0° (IQR = 11.7°–15.3°) at pretraining to 6.7° (IQR = 3.7°–8.1°) at posttraining (P = .008), knee-valgus angle from 5.0° (IQR = 2.0°–6.1°) at pretraining to 2.2° (IQR = 0.9°–3.2°) at posttraining (P = .008), and trunk lateral-inclination angle from 6.5° (IQR = 3.9°–7.4°) at pretraining to 4.3° (IQR = 4.0°–4.6°) at posttraining (P = .02). However, no change occurred in the control group (Table 4; Figure 7). The peak knee-valgus moment decreased from 0.15 Nm/kg/m (IQR = 0.14–0.28 Nm/kg/m) at pretraining to 0.09 Nm/kg/m (IQR = 0.07–0.11 Nm/kg/m) at posttraining in the training group (P = .008) but did not change in the control group from pretraining (0.14 Nm/kg/m; IQR = 0.13–0.19 Nm/kg/m) to posttraining (0.13 Nm/kg/m; IQR = 0.11–0.16 Nm/kg/m; P = .89; Figure 8).
Table 4.
Peak Values of Kinematic Data in Single-Legged Squat
| Variable |
Training Group, ° |
Control Group, ° |
||||
| Median (Interquartile Range) |
P Value |
Median (Interquartile Range) |
P Value |
|||
| Pretraining |
Posttraining |
Pretraining |
Posttraining |
|||
| Hip | ||||||
| Flexion | 61.6 (56.1–67.9) | 69.1 (63.7–77.1) | .04a | 65.9 (60.0–68.1) | 61.3 (54.2–65.9) | .33 |
| Adduction | 22.1 (21.0–22.9) | 21.8 (20.8–24.1) | .59 | 21.2 (21.0–22.9) | 19.4 (18.0–21.8) | .78 |
| Internal rotation | 14.0 (11.7–15.3) | 6.7 (3.7–8.1) | .008a | 8.8 (7.7–12.7) | 10.9 (5.7–13.6) | .26 |
| Knee | ||||||
| Flexion | 74.5 (66.8–82.9) | 82.5 (76.2–84.7) | .04a | 74.4 (67.4–79.1) | 74.7 (67.4–79.1) | .16 |
| Valgus | 5.0 (2.0–6.1) | 2.2 (0.9–3.2) | .008a | 2.9 (2.0–4.4) | 3.4 (2.6–6.2) | .67 |
| Trunk | ||||||
| Flexion | 22.3 (15.6–30.8) | 32.2 (27.8–38.2) | .04a | 23.6 (14.2–28.0) | 25.3 (19.2–31.1) | .21 |
Indicates difference (P < .05).
Figure 7.
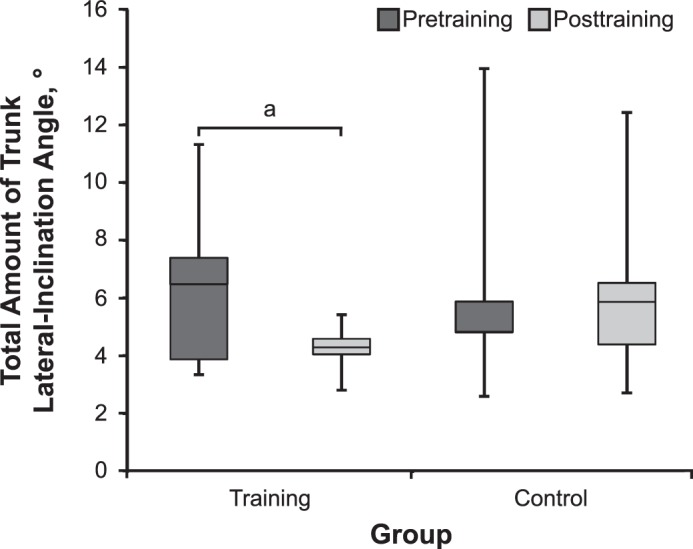
The total amount of trunk lateral-inclination angle in the single-legged squat (median value with interquartile range). a P < .05.
Figure 8.
The peak knee-valgus moment in the single-legged squat (median value with interquartile range). a P < .05.
Isokinetic Strength
Isokinetic peak torque increased in the training group for all muscles tested except the knee extensors. The peak torque of the hip flexor at 60°/s was 1.15 Nm/kg (IQR = 1.01–1.24 Nm/kg) at pretraining and 1.33 Nm/kg (IQR = 1.14–1.42 Nm/kg) at posttraining (P = .01), the hip abductor at 120°/s was 0.65 Nm/kg (IQR = 0.61–0.79 Nm/kg) at pretraining and 0.73 Nm/kg (IQR = 0.71–0.85 Nm/kg) at posttraining (P = .02), the knee flexor at 60°/s was 1.22 Nm/kg (IQR = 1.16–1.30 Nm/kg) at pretraining and 1.38 Nm/kg (IQR = 1.23–1.40 Nm/kg) at posttraining (P = .03) and at 120°/s was 1.08 Nm/kg (IQR = 1.03–1.30 Nm/kg) at pretraining and 1.26 Nm/kg (1.12–1.32 Nm/kg) at posttraining (P = .049), the trunk extensor at 40°/s was 4.27 Nm/kg (IQR = 3.40–4.85 Nm/kg) at pretraining and 4.67 Nm/kg (IQR = 4.41–5.08 Nm/kg) at posttraining (P = .04), and the trunk flexor at 20°/s was 2.27 Nm/kg (IQR = 1.78–3.47 Nm/kg) at pretraining and 3.33 Nm/kg (IQR = 2.89–3.89 Nm/kg) at posttraining (P = .01) and at 40°/s was 2.27 Nm/kg (IQR = 1.78–2.74 Nm/kg) at pretraining and 3.35 Nm/kg (IQR = 2.72–4.10 Nm/kg) at posttraining (P = .008; Table 5). However, in the control group, we observed no change in isokinetic muscle strength between pretraining and posttraining. After the core-muscle training, the peak torque of the knee flexors at 60°/s (P = .02) and 120°/s (P = .046) and the trunk flexors at 20°/s (P = .02) was higher in the training than in the control group.
Table 5.
Isokinetic Muscle Strength
| Variable |
Angular Velocity, °/s |
Training Group, Nm/kg |
Control Group, Nm/kg |
||||
| Median (Interquartile Range) |
P Value |
Median (Interquartile Range) |
P Value |
||||
| Pretraining |
Posttraining |
Pretraining |
Posttraining |
||||
| Hip | |||||||
| Flexion | 60 | 1.15 (1.01–1.24) | 1.33 (1.14–1.42) | .01b | 1.24 (1.12–1.35) | 1.22 (1.14–1.36) | .18 |
| 120 | 1.13 (1.00–1.14) | 1.16 (1.10–1.38) | .21 | 1.12 (0.95–1.40) | 1.12 (1.02–1.43) | .18 | |
| Abduction | 60 | 0.78 (0.70–0.92) | 0.92 (0.81–0.94) | .05 | 0.96 (0.85–1.06) | 1.00 (0.86–1.06) | .12 |
| 120 | 0.65 (0.61–0.79) | 0.73 (0.71–0.85) | .02b | 0.79 (0.67–0.96) | 0.78 (0.69–1.01) | .06 | |
| Knee | |||||||
| Extension | 60 | 2.17 (1.63–2.23) | 2.03 (1.86–2.05) | >.99 | 1.89 (1.52–2.08) | 1.74 (1.53–2.06) | .67 |
| 120 | 1.77 (1.42–1.81) | 1.71 (1.65–1.76) | .95 | 1.42 (1.16–1.77) | 1.42 (1.13–1.73) | .94 | |
| Flexion | 60 | 1.22 (1.16–1.30) | 1.38 (1.23–1.40)a | .03b | 1.16 (1.08–1.29) | 1.20 (1.11–1.24) | .24 |
| 120 | 1.08 (1.03–1.30) | 1.26 (1.12–1.32)a | .049b | 1.07 (0.98–1.19) | 1.09 (1.05–1.12) | .26 | |
| Trunk | |||||||
| Extension | 20 | 4.46 (4.10–5.04) | 4.89 (3.78–4.80) | .14 | 4.06 (3.53–4.75) | 4.08 (3.78–4.80) | .26 |
| 40 | 4.27 (3.40–4.85) | 4.67 (4.41–5.08) | .04b | 3.58 (3.09–4.71) | 4.12 (3.32–4.68) | .09 | |
| Flexion | 20 | 2.27 (1.78–3.47) | 3.33 (2.89–3.89)a | .01b | 2.58 (2.15–3.31) | 2.36 (2.18–2.63) | .78 |
| 40 | 2.27 (1.78–2.74) | 3.35 (2.72–4.10) | .008b | 2.84 (2.46–3.35) | 2.66 (2.57–3.16) | .16 | |
Greater than the control group (P < .05).
Indicates difference between pretraining and posttraining (P < .05).
DISCUSSION
Our most interesting finding was that performing simple core-muscle training resulted in neuromuscular-control changes in the trunk and lower limbs.
Neuromuscular Control of the Trunk
We demonstrated that lateral trunk motion decreased during the SLS after core-muscle training. The relationship between neuromuscular control of the trunk and ACL injury has been emphasized. Zazulak et al13,14 reported that factors related to core stability predicted ACL injury. In a cohort study using video analysis, Hewett et al15 showed that trunk control in the coronal plane was an important component of ACL injury. Landing with greater lateral trunk motion makes the ground reaction force vector move laterally and increases the lever arm in reference to the knee-joint center. Therefore, knee-valgus moment rises and eventually leads to ACL injury.25
Participants who performed the core-muscle–training program also displayed increased trunk-flexion angles during the DJT and SLS and increased hip- and knee-flexion angles during the SLS, indicating that core-muscle training improved neuromuscular control (Figure 9). Researchers have reported that neuromuscular control of the trunk in the sagittal plane also plays an important role in knee-joint biomechanics. Kulas et al26 found that hamstrings-muscle and knee anterior shear forces depended on a trunk-adaptation strategy. Nagano et al27 and Blackburn and Padua28 indicated that trunk flexion during cutting and landing maneuvers was related to increasing hip- and knee-flexion angles, so increasing trunk flexion in these maneuvers might reduce the ACL injury risk.
Figure 9.

Maximal knee-flexion phase in the drop-jump test. Hip-, knee-, and trunk-flexion angles were greater and knee-in alignment improved from, A, pretraining, to, B, posttraining.
These trunk kinematic changes in the coronal and sagittal planes seem to result from core strengthening. Nakase et al29 investigated the effect of part 2 of the FIFA11+ program using positron emission tomography. Part 2 of the FIFA11+ program includes the bench, sideways bench, and hamstrings training that we used as a reference when developing our simple core-muscle–training program. They demonstrated that the abdominal rectus, gluteus medius, and gluteus minimus were activated after part 2 of the FIFA11+. Therefore, it was reasonable for the training group to demonstrate increased isokinetic strength of the muscles surrounding the hip joint and trunk (ie, core muscles).
Knee-Valgus Moment
The peak knee-valgus moment during the DJT was reduced after core-muscle training in our study. In a cohort study, Hewett et al2 noted that female athletes with a greater knee-valgus angle and moment during a jump-landing task increased their risk of ACL injury. In a model-based image-matching study, Koga et al3 showed that sudden knee-valgus loading and noncontact ACL injury occurred approximately 40 milliseconds after initial contact. The first peak knee-valgus moment was recorded within 60 milliseconds after initial contact for most of our participants during the DJT. Given that increased knee-valgus moment immediately after initial contact might be a risk factor for ACL injury, producing the kinetic change that decreased the first peak knee-valgus moment after initial contact in the training group seems to be the most suitable way to reduce the risk of noncontact ACL injury during a landing maneuver. A decreased knee-valgus moment immediately after initial contact seemed to be caused by decreased lateral trunk motion or increased trunk-, hip-, and knee-flexion angles. That is, core-muscle training improved the feedforward mechanism in the jump-landing maneuver.
The Role of Core-Muscle Training in an ACL Injury-Prevention Program
Whereas some ACL injury-prevention programs have effectively decreased the incidence of ACL injury,7–10 they have several problems. First, these programs comprise many types of training exercises, which makes accomplishing them in daily practice difficult for amateur athletes, who were limited by daily practice time. Second, it is unclear which training actually contributed to the reduced incidence of ACL injury. To encourage clinicians to use ACL injury-prevention programs, researchers need to develop effective and efficient programs that can be performed in a shorter time. In our study, the time required for core-muscle training was 10 minutes or less, and participant compliance was excellent. Clinicians, coaches, and athletic trainers should consider incorporating this core-muscle training into the warm-up program of daily practice as one of the most essential elements and should recommend that players perform the exercises at home. We clearly demonstrated that core-muscle training can potentially improve the neuromuscular control of the trunk and lower limbs; however, we do not know whether performing only these 3 training exercises sufficiently reduces the incidence of ACL injuries. To develop an effective ACL injury-prevention program, we need to determine the mechanism by which training other than core-muscle training may decrease the incidence of ACL injuries.
LIMITATIONS
Our study had limitations. First, we studied only female basketball players. We do not know whether this core-muscle training will produce the same training effect in male athletes or athletes in other sports. Second, this study included only a limited number of participants and was not adequately powered to perform all statistical analyses. We included nonnormally distributed variables at a certain rate. Using a parametric test to compare normally distributed variables was ideal; however, given that measured kinematic, kinetic, and isokinetic muscle-strength variables in the same task included normally and nonnormally distributed data, we used a nonparametric analysis to compare the 2 groups by consolidating the statistical methods. Moreover, a risk of type 1 error existed because we performed multiple comparisons for kinematic, kinetic, and isokinetic muscle-strength variables among an inadequate number of participants. However, given that all participants belonged to 1 team and performed the same regular practice, the kinematic and kinetic changes in the training group might have been achieved by the simple core-muscle training. Third, the 8-week training duration of this study might not have been long enough to evaluate the training effects. However, Pfile et al30 reported that a 4-week training program of core-stability and plyometric exercises resulted in biomechanical changes at the knee and hip joints during a drop vertical jump. Whereas we believed that our training program lasted long enough for us to evaluate the effects on biomechanics during the DJT and SLS, the training effects need to be evaluated over a longer training duration, or a more extensive prospective study with a larger sample size needs to be conducted to demonstrate whether this core-muscle–training program can reduce the incidence of ACL injuries.
CONCLUSIONS
Neuromuscular control of the lower limb and trunk in the DJT and SLS, as well as isokinetic muscle strength, was modified after 8 weeks of core-muscle training in collegiate female basketball players. Therefore, the risk of noncontact ACL injury might be reduced.
ACKNOWLEDGMENTS
We thank Eiki Tsushima, PhD, Hirosaki University School of Health Science, for providing assistance with the statistical analysis.
REFERENCES
- 1.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 2.Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1. Mechanisms and risk factors. Am J Sports Med. 2006;34(2):299–311. doi: 10.1177/0363546505284183. [DOI] [PubMed] [Google Scholar]
- 3.Koga H, Nakamae A, Shima Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38(11):2218–2225. doi: 10.1177/0363546510373570. [DOI] [PubMed] [Google Scholar]
- 4.Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing ACL injuries: current biomechanical and epidemiologic considerations. Update 2010. N Am J Sports Phys Ther. 2010;5(4):234–251. [PMC free article] [PubMed] [Google Scholar]
- 5.Taylor JB, Waxman JP, Richter SJ, Shultz SJ. Evaluation of the effectiveness of anterior cruciate ligament injury prevention programme training components: a systematic review and meta-analysis. Br J Sports Med. 2015;49(2):79–87. doi: 10.1136/bjsports-2013-092358. [DOI] [PubMed] [Google Scholar]
- 6.Lopes TJA, Simic M, Myer GD, Ford KR, Hewett TE, Pappas E. The effects of injury prevention programs on the biomechanics of landing tasks: a systematic review with meta-analysis. Am J Sports Med. 2017;46(6):1492–1499. doi: 10.1177/0363546517716930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27(6):699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 8.Heidt RS, Jr, Sweeterman LM, Carlonas RL, Traub JA, Tekulve FX. Avoidance of soccer injuries with preseason conditioning. Am J Sports Med. 2000;28(5):659–662. doi: 10.1177/03635465000280050601. [DOI] [PubMed] [Google Scholar]
- 9.Myklebust G, Engebretsen L, Braekken IH, Skjølberg A, Olsen OE, Bahr R. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13(2):71–78. doi: 10.1097/00042752-200303000-00002. [DOI] [PubMed] [Google Scholar]
- 10.Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med. 2005;33(7):1003–1010. doi: 10.1177/0363546504272261. [DOI] [PubMed] [Google Scholar]
- 11.Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J Strength Cond Res. 2005;19(1):51–60. doi: 10.1519/13643.1. [DOI] [PubMed] [Google Scholar]
- 12.Steffen K, Emery CA, Romiti M, et al. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med. 2013;47(12):794–802. doi: 10.1136/bjsports-2012-091886. [DOI] [PubMed] [Google Scholar]
- 13.Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35(7):1123–1130. doi: 10.1177/0363546507301585. [DOI] [PubMed] [Google Scholar]
- 14.Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. The effects of core proprioception on knee injury: a prospective biomechanical-epidemiological study. Am J Sports Med. 2007;35(3):368–373. doi: 10.1177/0363546506297909. [DOI] [PubMed] [Google Scholar]
- 15.Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417–422. doi: 10.1136/bjsm.2009.059162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Frank B, Bell DR, Norcross MF, Blackburn JT, Goerger BM, Padua DA. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am J Sports Med. 2013;41(11):2676–2683. doi: 10.1177/0363546513496625. [DOI] [PubMed] [Google Scholar]
- 17.Khayambashi K, Ghoddosi N, Straub RK, Powers CM. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: a prospective study. Am J Sports Med. 2016;44(2):355–361. doi: 10.1177/0363546515616237. [DOI] [PubMed] [Google Scholar]
- 18.Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337:a2469. doi: 10.1136/bmj.a2469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Longo UG, Loppini M, Berton A, Marinozzi A, Maffulli N, Denaro V. The FIFA 11+ program is effective in preventing injuries in elite male basketball players: a cluster randomized controlled trial. Am J Sports Med. 2012;40(5):996–1005. doi: 10.1177/0363546512438761. [DOI] [PubMed] [Google Scholar]
- 20.Fédération Internationale de Football Association. The “11+” Manual: A Complete Warm-up Programme to Prevent Injuries. 2018 http://www.yrsa.ca/pdf/Fifa11/11plus_workbook_e.pdf#search=%27FIFA+11+manual%27 Accessed December 14.
- 21.Woltering HJ. A FORTRAN package for generalized, cross-validatory spline smoothing and differentiation. Adv Eng Software. 1986;8(2):104–113. [Google Scholar]
- 22.Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2005;33(2):197–207. doi: 10.1177/0363546504266484. [DOI] [PubMed] [Google Scholar]
- 23.Farrell M, Richards JG. Analysis of the reliability and validity of the kinetic communicator exercise device. Med Sci Sports Exerc. 1986;18(1):44–49. [PubMed] [Google Scholar]
- 24.Parcell AC, Sawyer RD, Tricoli VA, Chinevere TD. Minimum rest period for strength recovery during a common isokinetic testing protocol. Med Sci Sports Exerc. 2002;34(6):1018–1022. doi: 10.1097/00005768-200206000-00018. [DOI] [PubMed] [Google Scholar]
- 25.Hewett TE, Myer GD. The mechanistic connection between the trunk, hip, knee, and anterior cruciate ligament injury. Exerc Sport Sci Rev. 2011;39(4):161–166. doi: 10.1097/JES.0b013e3182297439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kulas AS, Hortobágyi T, Devita P. The interaction of trunk-load and trunk-position adaptations on knee anterior shear and hamstrings muscle forces during landing. J Athl Train. 2010;45(1):5–15. doi: 10.4085/1062-6050-45.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nagano Y, Ida H, Akai M, Fukubayashi T. Relationship between three-dimensional kinematics of knee and trunk motion during shuttle run cutting. J Sports Sci. 2011;29(14):1525–1534. doi: 10.1080/02640414.2011.599038. [DOI] [PubMed] [Google Scholar]
- 28.Blackburn JT, Padua DA. Influence of trunk flexion on hip and knee joint kinematics during a controlled drop landing. Clin Biomech (Bristol, Avon) 2008;23(3):313–319. doi: 10.1016/j.clinbiomech.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 29.Nakase J, Inaki A, Mochizuki T, et al. Whole body muscle activity during the FIFA 11+ program evaluated by positron emission tomography. PLoS One. 2013;8(9):e73898. doi: 10.1371/journal.pone.0073898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pfile KR, Hart JM, Herman DC, Hertel J, Kerrigan DC, Ingersoll CD. Different exercise training interventions and drop-landing biomechanics in high school female athletes. J Athl Train. 2013;48(4):450–462. doi: 10.4085/1062-6050-48.4.06. [DOI] [PMC free article] [PubMed] [Google Scholar]