

Abstract
Epididymal fusional anomalies have been found to be associated with conditions of testicular maldescent with the several studies investigating this association reporting several variations in epididymal anatomy and epididymal-testicular fusion. To our knowledge, a single case of an isolated lower epididymal pole with a normal vas deferens, dubbed “Epididymal Polar Dissociation”, has been reported in the literature. In this report, we report the second case of epididymal polar dissociation discovered in a 17-year-old during surgical management of left testicular torsion.
Keywords: Epididymis, Fusion, Polar dissociation, Testicular torsion
Introduction
Epididymal fusional anomalies have long been associated with cryptorchidism as well as inguinal hernias and hydrocele.1 Documented variations of normal epididymal anatomy have been reported in studies investigating these associations, each of which proposes a classification scheme based on the prevalent variations in the study sample.1,2 None of the classifications, however, describe an anomaly whereby the cauda epididymis, and a normal nonatretic vas deferens, is isolated from the remainder of the epididymal body with no communication between the two structures, a previously undescribed anomaly first reported by McCain et al., in 2014 and dubbed “epididymal polar dissociation”.3 No other case has been since reported in the literature. In this article, we report the second case of epididymal polar dissociation discovered in a 17-year-old patient during the surgical exploration and management of left testicular torsion.
Case presentation
Our patient is a 17-year-old male with no previous history of medical illness who presented to our institution complaining of sudden-onset severe pain in the groin of a few hours’ duration. The patient reported similar episodes in the past which resolved spontaneously. On physical examination, the patient was found to have a tender high-riding left testicle but no remarkable findings. Testicular torsion was suspected, and a Doppler ultrasound was performed which revealed a 2.9 x 3.9 × 4.6 cm left testicle with no identifiable Doppler color flow, a heterogenous echotexture and a vertical orientation with respect to the right testicle, as seen in Fig. 1. The right testicle, however, had a normal Doppler color flow echotexture and orientation. Urgent surgical exploration was performed. After successful detorsion of the left testis, inspection revealed that a caput epididymis arising from the cranial pole of the testis with the corpus epididymis coursing caudally along its posterior aspect. The cauda epididymis, with a normal nonatretic vas deferens arising from its termination, existed separately from the remainder of the epididymal body with no apparent communication between the two structures. Fig. 2 demonstrates the intraoperative findings. A normal right testicle was found during the right hemiscrotal exploration. Bilateral testicular fixation was performed and the patient was discharged on the second post-operative day.
Fig. 1.

Doppler ultrasound of the left testis demonstrating compromised blood flow.
Fig. 2.
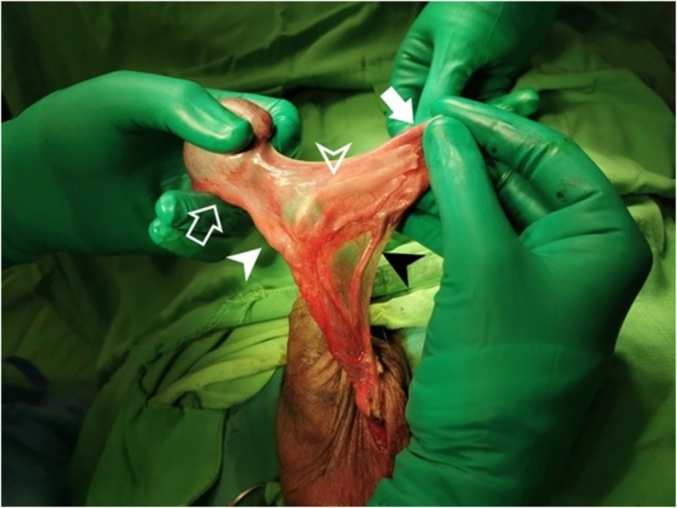
Intraoperative photo demonstrating the anatomic variation.
(Clear arrow: superior pole of the epididymis. Solid arrow: Lower pole of the epididymis. Clear arrowhead: vas deferens. White arrowhead: spermatic cord. Black arrowhead: vascular bundle of the lower epididymal pole).
Discussion
Fusional anomalies of the epididymis and testis may be expected due to the complexity of their embryogenesis. Several factors are implicated in the mechanism behind fusional anomalies, chiefly of which are the hormonal and mechanical elements responsible for normal testicular descent into the scrotum, given the established associations between fusional anomalies and cryptorchidism, inguinal hernias and hydrocele.1 On a similar vein, epididymal fusional disorders have also been theorized to be due to intrauterine hormonal disturbances.4 Furthermore, vascular accidents may lead to fusional anomalies. During mesonephric involution, the blood supply of the vas deferens transitions from the dorsal aorta to the internal iliac artery.2 Accidents sustained during this process may account for segmental epididymal or vasal atresia and, therefore, fusional anomalies.4
Classifications of epididymal anomalies have been proposed in the several studies of which Caterino et al.’s is the most recent and most exhaustive. In their classification, 3 groups of anomalies are described based on the degree of nonunion: normal anatomy, minor anomalies and major anomalies. Normal anatomy is defined either by contiguity between the head, body and tail or the detachment of the body. Minor anomalies are defined as either the disconnection of the body and tail or of the body and part of the epididymal head. Lastly, major anomalies are defined by either the disconnection of the head and body, the complete separation of the epididymis from the testis with the presence or absence of a mesentery between the two, or the complete separation and atrophy of the epididymis.1 The documented fusional anomalies in the literature fall into one of the eight types. No classification describes an anomaly where a superior epididymal pole is found attached to the testis and a lower epididymal pole, with a normal nonatretic vas deferens arising from its termination, is found isolated from the remainder of the epididymis with no communication seen between the two structures. Coined as “epididymal polar dissociation” by McCain et al. in their description of this previously undocumented variant, this fusional anomaly is exceptionally rare, with our case being the second of its nature.
The classical prevalence of epididymal anomalies among patients with cryptorchidism was found to be 36%.4 More recently, minor anomalies were found to have a 42.2% prevalence among patients with cryptorchidism versus a 5.6% prevalence in control patients and major anomalies a 9.3% by 1.6% prevalence in patients with cryptorchidism and controls respectively.1 Fusional and ductal anomalies have been associated with infertility as well with ductal anomalies having an incidence of 10–27% patients with infertility as compared to 0.5%–1% of normal patients.5 In Merksz et al.’s study, the authors report that 612 out of 1386 cryptorchidism cases were found to have anomalies that did not permit sperm passage into the vas deferens.2 The presence of a fusional anomaly, however, is not correlated with reduced fertility. Kraft et al. investigated the histological content of undescended testes and compared it to their normal descended counterparts to determine if associated epididymal fusional anomalies are predictive of reduced histological content. They conclude that though epididymal anomalies are associated with smaller testicle size and higher pre-operative position, no significant abnormalities in germ cell or adult dark spermatogonia content present.5
Conclusion
Fusional anomalies have long been described in studies investigating their association with cryptorchidism. Though several rare variations have been reported, with several classifications describing these anomalies, cases of epididymal polar dissociation remain to be exceedingly rare. Being familiar with the different variations, both rare and common, is essential to avoid unwanted injuries during the surgical exploration and management of testicular disorders.
Declarations of interest
None.
Contributor Information
Imad Matta, Email: imad.f.matta@gmail.com.
Elie Ghabi, Email: elieghabi@gmail.com.
Rana Abi Tayeh, Email: rana_abitayeh@hotmail.com.
Edward Assaf, Email: assaf.edward@gmail.com.
Walid Al Hajj Obeid, Email: waobeid@stgeorgehospital.org.
References
- 1.Caterino S., Lorenzon L., Cavallini M., Cavaniglia D., Ferro F. Epididymal‐testicular fusion anomalies in cryptorchidism are associated with proximal location of the undescended testis and with a widely patent processus vaginalis. J Anat. 2014;225(4):473–478. doi: 10.1111/joa.12222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Merksz M., Toth J. Testicular-epididymal fusion abnormality in undescended testis. Int Urol Nephrol. 1987;19(2):179–187. doi: 10.1007/BF02550471. [DOI] [PubMed] [Google Scholar]
- 3.McCain S., McCain S., Mark D., Brown R. Case reports in urology; 2014. Epididymal Polar Dissociation: A Previously Undescribed Anatomical Variant. 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mollaeian M., Mehrabi V., Elahi B. Significance of epididymal and ductal anomalies associated with undescended testis: study in 652 cases. Urology. 1994;43(6):857–860. doi: 10.1016/0090-4295(94)90152-x. [DOI] [PubMed] [Google Scholar]
- 5.Kraft K.H., Mucksavage P., Canning D.A., Snyder H.M., III, Kolon T.F. Histological findings in patients with cryptorchidism and testis-epididymis nonfusion. J Urol. 2011;186(5):2045–2049. doi: 10.1016/j.juro.2011.07.037. [DOI] [PubMed] [Google Scholar]