

Abstract
Background:
Although high density lipoprotein (HDL) modulates many cell types in the cardiovascular system, little is known about HDL in the kidney. We assessed urinary excretion of apolipoprotein AI (apoAI), the main protein in HDL.
Methods:
We enrolled 228 children with various kidney disorders and 40 controls. Urinary apoAI, albumin and other markers of kidney damage were measured using ELISA, apoAI isoforms with Western blot, and renal biopsies stained for apoAI.
Results:
Patients followed in nephrology clinic had elevated urinary apoAI vs. controls (median 0.074 ug/mg; Interquartile Range (IQR): 0.0160–0.560, vs. 0.019 ug/mg; IQR: 0.004–0.118, p<0.001). Patients with tubulopathies, renal dysplasia/congenital anomalies of the kidney and urogenital tract, glomerulonephritis, and nephrotic syndrome (NS) in relapse had greatest elevations (p≤0.01). Patients with NS in remission, nephrolithiasis, polycystic kidney disease, transplant or hypertension were not different from controls. Although all NS in relapse had higher apoAI excretion than in remission (0.159 vs 0.0355 ug/mg, p=0.01), this was largely driven by patients with focal segmental glomerulosclerosis (FSGS). Many patients, especially with FSGS, had increased urinary apoAI isoforms. Biopsies from FSGS patients showed increased apoAI staining at proximal tubule brush border, compared to diffuse cytoplasmic distribution in minimal change disease.
Conclusion:
Children with kidney disease have variably increased urinary apoAI depending on underlying disease. Urine apoAI is particularly elevated in diseases affecting proximal tubules. Kidney disease is also associated with HMW apoAI isoforms in urine, especially FSGS. Whether abnormal urinary apoAI is a marker or contributor to renal disease awaits further study.
Keywords: Apolipoprotein AI, high density lipoprotein, nephrotic syndrome, focal segmental glomerulosclerosis, Fanconi syndrome, Dent disease
Introduction
Lipoproteins, including very low density lipoprotein (VLDL), low density lipoprotein (LDL), and high density lipoproteins (HDL) are most closely linked to pathophysiology of cardiovascular disease (CVD) and are therapeutically targeted in CVD [1–5]. Recently, the pathophysiologic importance of lipoproteins, specifically HDL, has expanded beyond CVD to include various disorders such as sepsis, cancer, diabetes, and immunological diseases [6–9]. This is because HDL, and its main protein, apolipoprotein AI (apoAI), provide beneficial effects in different types of cells by a variety of mechanisms, which include increasing cellular cholesterol efflux, reducing oxidative stress and inflammatory cytokine response, increasing insulin secretion, and regulation of cellular apoptosis, differentiation, and proliferation [6–13].
Traditionally, the kidneys have not been regarded as major lipoprotein targets because the glomerular filtration barrier limits passage of most lipid particles and plasma proteins. However, HDL is not synthesized as an intact particle but assembled and remodeled from its constituent lipids, apolipoproteins, and enzymes in the circulation. Metabolism of HDL also proceeds by metabolism of its individual components rather than removal of the holoparticle. The size of the predominant protein component of HDL, apoAI, is 28 kDa, which is approximately half the size of albumin, suggesting it can cross the filtration barrier and interact with the renal parenchyma. We recently showed that normal apoAI, apoAI mimetic, and normal HDL protect against podocyte injury in vitro and lessen glomerular injury and proteinuric kidney damage in vivo [14]. However, disorders which disrupt apoAI/HDL structure or function may permit filtration of potentially harmful apoAI/HDL. Indeed, abnormal apoAI/HDL prevailing in diseases such as diabetes, Alport syndrome, and allograft failure, has been shown to damage kidney cells and reduce kidney function. In these circumstances, interventions which improve apoAI/HDL functionality benefit renal cells and lessen progressive renal damage through mechanisms which include modulation of inflammatory, immune, and fibrotic pathways [6, 15–19].
Once filtered, apoAI is reabsorbed by tubular epithelial cells expressing receptors (cubilin/megalin) and transporters for apolipoproteins and HDL, including ATP-binding cassette transporter-A1 (ABCA1), -G1 (ABCG1), and scavenger receptor-BI (SRBI) [20–25]. Deficiency or disruption of the transporters or receptors affects tubular handling of apoAI. For example, cubilin deficiency and proximal tubular reabsorption failure due to Fanconi syndrome increases urinary excretion of apoAI [21, 23]. Cubilin-deficient mice have reduced proximal tubule uptake and increased urinary loss of apoAI and albumin in association with decreased plasma levels of apoAI and HDL3 along with hypoalbuminemia [22]. Several studies have documented apoAI/HDL in urine of adults with kidney disease although the pathobiological significance of these observations is unclear [26–28]. Early stages of renal injury and impaired glomerular filtration rate (GFR) are associated with serum elevation of other HDL components, including apolipoprotein AIV and the enzyme lecithin cholesterol acyltransferase (LCAT) [26, 27, 29]. Elevation in urinary apoAI has also been suggested as a potential marker of calcium oxalate nephrolithiasis, as well as bladder cancer [28, 30]. Interestingly, a recent proteomic study assessing biomarkers of recurrent focal and segmental glomerulosclerosis (FSGS) after renal transplant, described a modified isoform of apoAI in urine that differentiated recurrent from non-recurrent FSGS [31]. In the current study, we therefore aimed to quantitate and characterize urinary apolipoprotein AI in children across a spectrum of kidney diseases and compared to healthy children.
Subjects and methods
Subjects.
Two hundred twenty-eight patients, age 3–18 years, seeking care in the Vanderbilt Pediatric Nephrology Clinic were enrolled. The demographic, clinical, laboratory features, and biopsy data were collected from the electronic medical record. Patients were grouped by clinical diagnosis. Thirteen patients with non-classifiable abnormalities were excluded from analysis. Forty healthy controls were recruited from a general pediatric setting. Exclusion criteria for controls included history of kidney disease or hypertension, acute illness, or medications other than vitamins, contraceptives, antihistamines, inhaled steroids or bronchodilators. The study was approved by the Institutional Review Board at Vanderbilt University Medical Center. A waiver of consent was granted for patients who submitted urine as part of their routine care. Controls were consented and asked to provide a urine sample for study purposes.
Analysis of urine and kidney biopsies.
Urine samples were aliquoted into 1.5 mL samples and immediately stored at −80°C until analysis. Urine levels of creatinine and total protein were measured by commercially available colorimetric assays (Quantichrome DICT-500, Thermo Fisher 22662). ApoAI, albumin, alpha-1-microglobulin (α1M), and kidney injury molecule-1 (KIM-1) were measured using commercially available ELISA kits (R&D DAPA10, Thermo Fischer EHALB, Abcam ab108884, R&D DKM100, respectively) according to the manufacturers’ instructions. All urinary measurements were expressed as a ratio to urine creatinine.
Western blots were performed for every patient with elevated urinary apoAI and a random sampling of patients from each group without elevated apoAI, including 14/14 patients with nephrotic syndrome (NS) relapse, 10/44 transplant patients, 6/18 glomerulonephritis (GN) patients, 17/19 patients with dysplasia / congenital anomalies of the kidney and urogenital tract (CAKUT), 12/24 patients with tubulopathies, 19/30 patients with NS remission, 1/4 polycystic kidney disease (PCKD) patients, 5/35 stone patients, and 8/40 controls. Western Blots were done using commercially available SDS-PAGE gels with MOPS SDS buffer. Protein concentration was measured as above, and a fixed amount of 20 ug total protein was loaded per well. Whole urine was centrifuged, boiled, then loaded into the gel. Molecular weight markers (Bio-Rad) were used in each gel. Proteins were transferred to nitrocellulose membranes and probed with anti-apoAI (mouse monoclonal Santa Cruz sc-376818 plus anti-mouse HRP secondary antibody Promega W4021).
From patients with available biopsies for review, two patients with FSGS and two with minimal change disease (MCD) were randomly selected along with kidney tissue from a normal adult control. Three micrometer sections were stained for apoAI. Briefly, paraffin sections were heated in 0.01 mol/L sodium citrate buffer (pH 6.0) and endogenous peroxidase quenched with fresh 0.3% hydrogen peroxidase / methanol. After blocking, sections were incubated with rabbit anti-apoAI (1:10000 Novus biology, Littleton, CO) in a humidified chamber at 4°C overnight, followed by incubation with a HRP-conjugated secondary antibody. Diaminobenzidine was used as a chromogen with hematoxylin as a counterstain. Slides treated with nonspecific antisera instead of primary antibody were used as negative control, and known positive tissues were used as positive controls. All slides were examined without knowledge of the diagnosis.
Statistical analysis.
The demographic and clinical characteristics of subjects are summarized using medians and lower and upper quartiles, as well as means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Wilcoxon rank sum and Kruskal-Wallis tests were used to compare urine apoAI and albumin levels between groups. Bonferroni correction was applied to p values when doing pairwise comparisons between different diagnoses. Multivariable linear regression with robust standard errors were used when comparing urinary apoAI among clinic patients and controls to control for potential confounding factors, such as age, race and sex. The regression model was pre-specified based on knowledge of potential effect of factors and consideration of not over-fitting, and only subjects with complete data (not missing any included covariate value) were included in the modeling. Spearman ρ correlation coefficients were obtained between urinary apoAI and other markers. Logarithmic transformation was used for skewed data for graphs as indicated. A two-sided p value <0.05 was considered statistically significant. All analyses were performed using R. version 3.5.0 (https://www.R-project.org).
Results
Demographic and baseline characteristics.
The demographic and clinical characteristics, primary diagnoses, and measured urinary markers are summarized in Table 1. On average, the controls were older and more likely to be female and black than clinic patients. There was no difference in urinary apoAI between white and non-white controls (p=0.577). Nine different disease entities are represented, comprised of nephrolithiasis and/or mineral abnormality (n=35), tubulopathy (n=24), PCKD (n=4), CAKUT (n=19), GN (n=18), transplant (n=44), NS relapse (n=14), NS remission (30), and hypertension (HTN) (40), along with 40 controls.
Table 1:
Demographics and clinical characteristics of controls and clinic patients.
| Controls (n=40) | Clinic Patients (n=228) | |
|---|---|---|
| Sex | ||
| Female | 68% (27) | 42% (95) |
| Male | 32% (13) | 58% (133) |
| Race* | ||
| White | 55% (21) | 77% (166) |
| Black | 42% (16) | 19% (41) |
| Asian | 0% (0) | 4% (8) |
| Latino | 3% (1) | 0% (1) |
| Age (years) | 13.5 17.0 18.0 15.3±3.4 |
8.0 13.0 16.0 11.9±4.4 |
| Ethnicity* | ||
| Hispanic | 5% (2) | 11% (24) |
| Non-Hispanic | 95% (37) | 89% (199) |
| Primary Diagnosis | ||
| Nephrolithiasis and/or mineral abnormality (stones) | 15% (35) | |
| Tubulopathy | 11% (24) | |
| - Proximal | (11) | |
| - Distal | (7) | |
| - Acute interstitial nephritis | (6) | |
| Polycystic kidney disease | 2% (4) | |
| Dysplasia/CAKUT | 8% (19) | |
| Glomerulonephritis | 8% (18) | |
| - Hypocomplementemic | (5) | |
| - IgA Nephropathy/Henoch-Schonlein Purpura Nephropathy | (5) | |
| - Microscopic vasculitis | (2) | |
| - Alport Syndrome | (1) | |
| - Persistent proteinuria | (5) | |
| Transplant | 19%. (44) | |
| - Stable with normal creatinine | (19) | |
| - Stable with elevated creatinine | (22) | |
| - Acute T cell rejection | (1) | |
| - Chronic allograft nephropathy | (2) | |
| Nephrotic syndrome relapse | 6% (14) | |
| - Minimal change disease | (11) | |
| - FSGS | (3) | |
| Nephrotic syndrome remission | 13% (30) | |
| - Minimal change disease | (22) | |
| - FSGS | (8) | |
| Hypertension | 18% (40) | |
| ACE inhibitor or Angiotensin Receptor Blocker | ||
| Yes | 0% (0) | 32% (73) |
| No | 100% (40) | 68% (155) |
| Diabetes | ||
| Yes | 0% (0) | 5% (12) |
| No | 100% [40] | 95% [216] |
| GFR Schwartz (mL/min/1.73 m2]** | 88.0 95.0 127.0 108.6±37.5 (n=11) |
50.2 77.5 91.0 73.2±29.6 (n=182) |
| Urine albumin/creatinine [ACR] [mg/g] | 3.7 9.2 23.2 19.2±25.8 |
7.03 22.9 143.1 120.0±228.5 |
| Urine apoAI/creatinine [ug/mg] | 0.004 0.019 0.118 0.125±0.294 |
0.016 0.074 0.560 1.255±4.088 |
| Urine α1M/creatinine [ug/mg] | 0.330 0.942 2.045 1.41±1.52 (n=15) |
1.954 9.040 41.64 27.1±39.9 (n=148) |
| Urine KIM-l/creatinine [ng/mg] | 0.166 0.238 0.857 0.56±0.60 (n=15) |
0.207 0.587 1.582 1.76±3.51 (n=148) |
a b c represent the lower quartile a, the median b, and the upper quartile c for continuous variables, x ± s represents mean±SD. N is the number of non-missing values. Numbers after proportions are frequencies.
Race and ethnicity are provided for patients whose charts contained these data.
GFR was calculated for patients with serum creatinine measured and documented within 6 months of the study visit.
Renal disease is associated with increased urinary apoAI that varies among different diseases.
Compared to the control group, the clinic patients cohort showed significantly elevated levels of urinary apoAI (median 0.074; IQR: 0.016 – 0.560 vs. 0.019 ug/mg; IQR: 0.004 – 0.118, p=0.001) (Figure 1A). Patients seen for evaluation of isolated hypertension had urinary apoAI levels that did not differ from controls (0.017 ug/mg; IQR: 0.003 – 0.096 vs. 0.019 ug/mg; IQR: 0.004 – 0.118, p<0.001); exclusion of these patients did not affect the significantly increased urinary apoAI in clinic patients (median 0.098; IQR: 0.023 – 0.65 vs. 0.019 ug/mg; IQR: 0.004 – 0.118, p<0.001) (Figure 1A). Urinary apoAI levels differed among the various renal diseases (Figure 2). Compared to controls, urinary apoAI was higher in patients with tubulopathies, renal dysplasia / CAKUT, GN, and NS in relapse (all adjusted p<0.01). In contrast, urinary apoAI was not different between controls and children with NS in remission, stones or mineral derangements, PCKD, or transplants.
Figure 1.
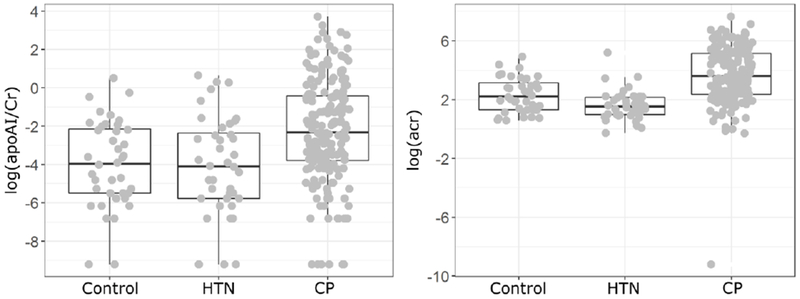
A. Urinary excretion of apoAI in clinic patients (CP) and controls.
CP does not include hypertension patients seen in clinic. Wilcoxon rank sum test p=0.0001. The lower quartile, median, and upper quartile are shown by the Boxplot. The whisker was extended to 1.5 times of Interquartile Range (IQR). For those with apoAI=0, a value of 0.0001 was assigned for logarithmic transformation shown as the minimum in the graph. B. Urinary excretion of albumin in CP and controls. Wilcoxon rank sum test p <0.0001. For those with ACR=0, a value of 0.0001 was assigned for logarithmic transformation shown as the minimum in the graph.
Figure 2. Urinary apoAI differentiated by disease classification.
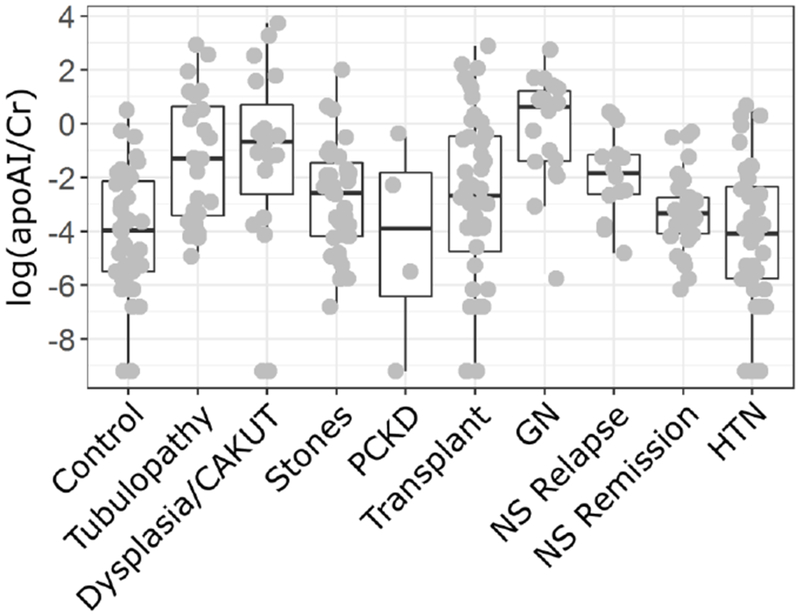
Wilcoxon rank sum test p=0.0001. The lower quartile, median, and upper quartile are shown by the boxplot. The whisker was extended to 1.5 times of Interquartile Range (IQR). For those with apoAI=0, a value of 0.0001 was assigned for logarithmic transformation shown as the minimum in the graph.
As expected, urinary albumin was elevated in clinic patients compared to controls (median 23.9; IQR: 7.03 – 143.1 vs. 9.16 mg/g; IQR: 3.70 – 23.2, p<0.001, Figure 1B). Since albuminuria is regarded to be a strong marker of progressive chronic kidney disease, we assessed whether urinary apoAI excretion correlated with urine albumin:creatinine ratio (ACR). Urinary apoAI correlated moderately with albumin when considering all diseases (Spearman’s Rho 0.56, p<0.001), but the degree of correlation varied considerably by disease. The strongest correlation was seen in patients with dysplasia / CAKUT (Spearman’s Rho 0.788, p≤0.001) while the weakest was in NS relapse (Spearman’s Rho 0.147, p=0.616). There was a modest negative correlation between urinary apoAI and GFR (Spearman Rho −0.282, p<0.001). The correlation of urinary apoAI with established markers of tubular injury/dysfunction was moderate with urinary α1M (Spearman Rho 0.42, p<0.001) and weak with urinary KIM-1 (Spearman Rho 0.29, p≤0.001).
Proximal but not distal tubulopathy is associated with elevated urinary apoAI.
Within the tubulopathy group, patients with disorders principally affecting proximal tubules including Fanconi syndrome, Dent disease, Lowe syndrome and cystinosis, had higher urinary apoAI levels than patients with primarily distal tubule dysfunction including distal renal tubular acidosis (RTA), diabetes insipidus, and Bartter syndrome (p=0.004, Figure 3). Notably, the median urinary apoAI in patients with acute interstitial nephritis (AIN) was not different from controls (0.16 ug/mg vs. 0.02 ug/mg, p=0.1) and much lower than in the patients with long-standing proximal tubule dysfunctions (2.85 ug/mg p=0.01).
Figure 3: Urinary apoAI in patients with renal tubulopathies.
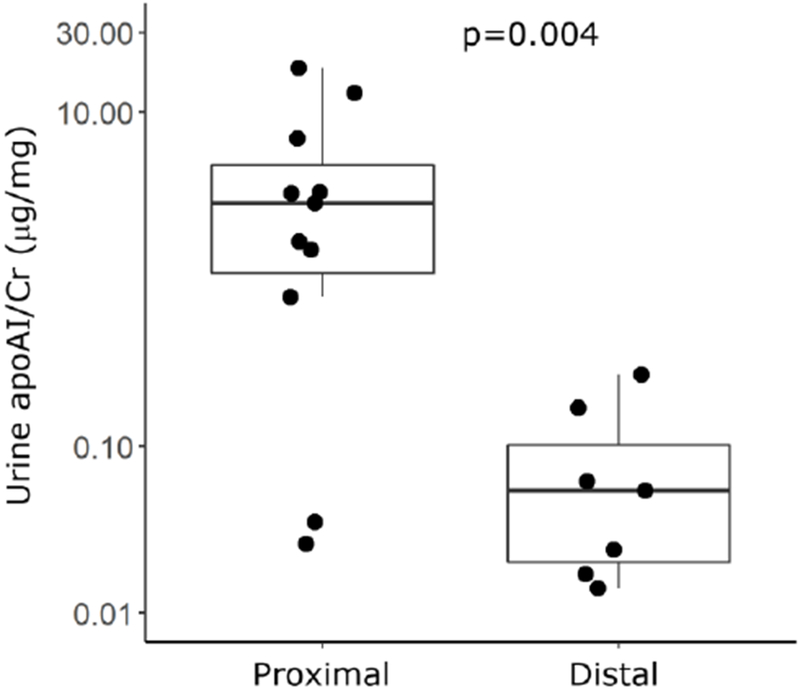
Wilcoxon rank sum test p=0.004. The lower quartile, median, and upper quartile are shown by the boxplot. The whisker was extended to 1.5 times of Interquartile Range (IQR).
Urinary apoAI is different in MCD vs. FSGS
Urinary apoAI was increased in NS in relapse compared to NS in remission or normal controls (Figure 2). Within the NS relapse group, there was a notable difference in median apoAI excretion in MCD vs. FSGS even though urinary ACR was markedly increased in both. Patients with FSGS had much higher median urinary apoAI in relapse compared to remission (1.42 vs. 0.037 ug/mg, p=0.01) (Figure 4). Patients with MCD did not show this increase in apoAI excretion in relapse vs. remission (0.083 vs. 0.032 ug/mg, p=0.08) (Figure 4).
Figure 4:
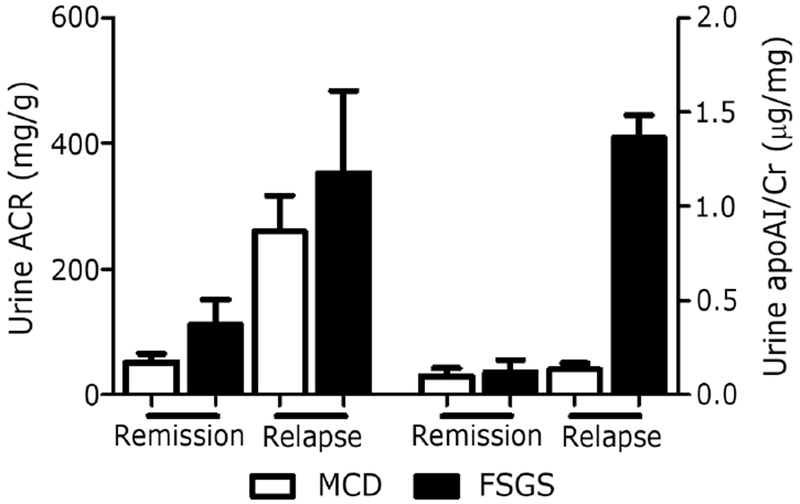
Urinary albumin and apoAI in Minimal Change Disease (MCD) and Focal Segmental Glomerulosclerosis (FSGS) in relapse and remission.
Renal distribution of apoAI differs in MCD and FSGS
Renal tissue biopsies from four patients with MCD or FSGS revealed a different pattern of apoAI staining than that seen in normal kidney tissues (Figure 5). In normal kidney, apoAI protein expression was focalized in the cytoplasm of proximal tubules. Compared to the normal kidney, apoAI staining was increased in proximal tubules in biopsies of both MCD and FSGS. Further, apoAI distribution was changed. In MCD, apoAI still showed diffuse cytoplasmic distribution, similar to that observed in controls. By contrast, in FSGS, apoAI staining appeared not only in the cytoplasm, but was also strongly concentrated at the brush border of the apical membrane of proximal tubules.
Figure 5:
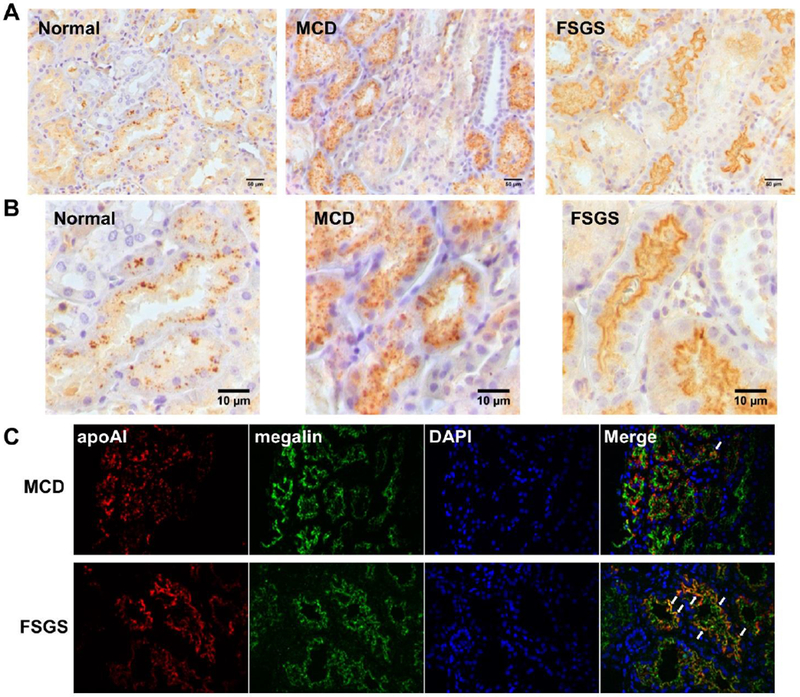
(A) ApoAI staining in kidneys from a control patient (adult kidney donor), a patient with minimal change disease (MCD), and a patient with focal segmental glomerulosclerosis (FSGS). (B) higher magnification showing localization of apoAI in the proximal brush border in the FSGS sample. (C) Fluorescent staining colocalizing apoAI with megalin, which is specifically expressed on the brush border of proximal tubules. The colocalization is especially prominent in the proximal tubule brush border of patients with FSGS compared to MCD (arrow). The MCD patient shown had urinary albumin to creatinine ratio (ACR) of 656.4 mg/g, urinary apoAI to creatinine ratio of 0.008 ug/mg, and serum creatinine of 0.57 mg/dL (GFR>100) while the FSGS patient had ACR of 588.5 mg/g, urinary apoAI to creatinine ratio of 1.538 ug/mg, and a serum creatinine of 0.57 mg/dL (GFR>100) in measurements closest to the time of biopsy.
Renal injury affects urinary apoAI subtype
Complementing the elevated levels of urinary apoAI measured by ELISA (Figure 1), Western blots also showed larger apoAI (28 kDa) bands in urine of clinic patients but not in normal controls. In addition, high molecular weight (HMW) subtypes of apoAI were present in urine from many patients with kidney disease. These HMW subtypes were associated with higher ACR and higher urinary apoAI (p<0.001) but not GFR (p=0.16). The HMW apoAI species were especially prominent in patients with FSGS in relapse (Figure 6). Although most patients with proximal tubulopathies and glomerulonephritis also had HMW apoAI forms, these bands were much less prominent than those seen in relapsing FSGS patients. Most patients with dysplasia / CAKUT, transplant and stones did not have HMW apoAI bands.
Figure 6. Western blots for urinary apoAI in patients with Minimal Change Disease (MCD) or Focal Segmental Glomerulosclerosis (FSGS) in relapse and remission.
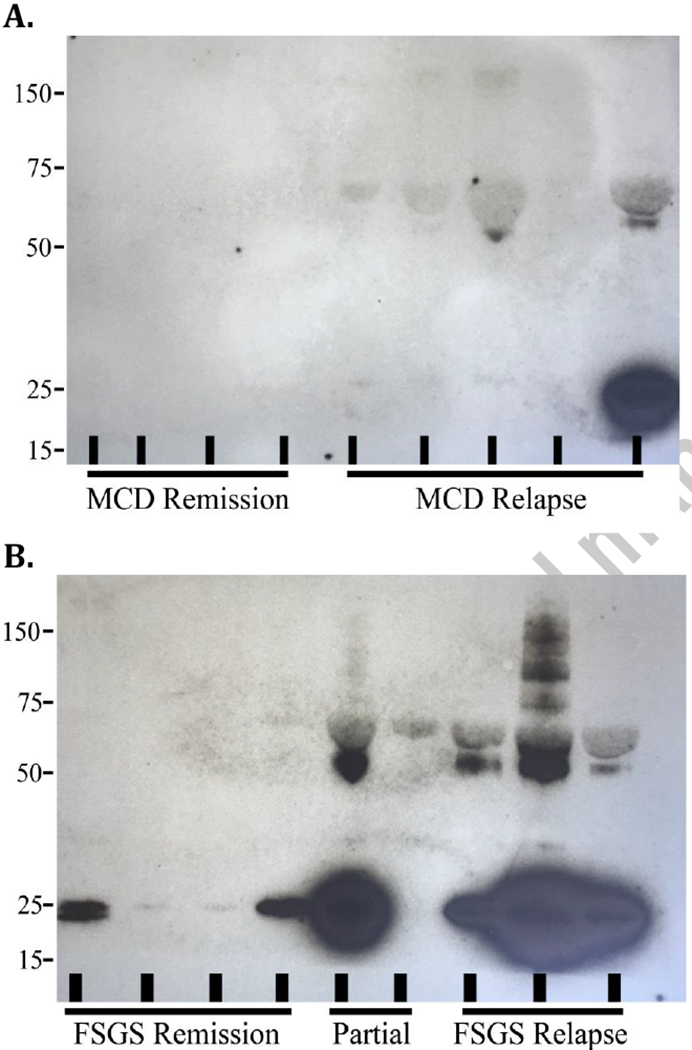
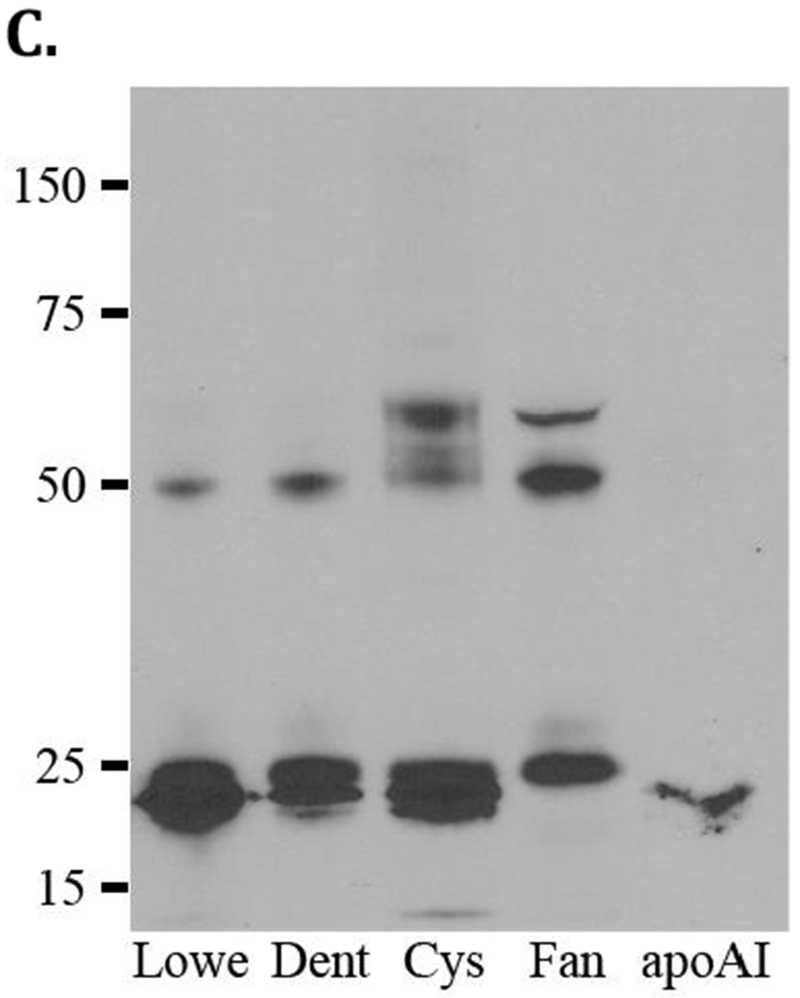
Each lane is a sample from a single patient with the diagnosis specified. A. Patients with MCD in remission and relapse. B. Patients with FSGS in remission and relapse. Partial remission includes patients with biopsy-proven FSGS and ongoing chronic kidney disease without nephrotic-range proteinuria. C. Patients with proximal tubulopathies including Lowe syndrome (Lowe), Fanconi syndrome (Fan), Dent disease (Dent), and cystinosis (Cys) along with a positive control (apoAI). The lower bands represent apoAI in its authentic, unmodified form. The larger bands, we believe, represent modified forms of the apoAI protein. We hypothesize that the detrimental urinary environment created by diseased kidneys favors the generation of oxidized lipids and lipoproteins that crosslink to produce high molecular weight subpopulations.
Discussion
We find that children with kidney disease have variably increased urinary apoAI, which depends on the underlying disease. Of note, only modest correlation with albuminuria or GFR was observed. Tubulopathies, especially those involving the proximal tubule, had the highest apoAI excretion. At 28 kDa, apoAI is less than half the size of albumin (68 kDa) and is therefore predicted to easily cross the glomerular filtration barrier. The minimal or absent urinary apoAI in children with normal kidneys indicates complete tubular reabsorption consistent with the current understanding that the cubilin/megalin complex in the proximal tubules binds and endocytoses low molecular weight proteins, including apoAI [21]. In line with this understanding, children with dysfunction of the proximal tubule, e.g. Fanconi syndrome, Dent disease, Lowe Syndrome and cystinosis, were found to have significantly elevated urinary apoAI (Figures 2 and 3). Our data also indicate that acquired and chronic progressive kidney damage involving the proximal tubules leads to increased urinary apoAI. Thus, children with dysplasia / CAKUT had significantly elevated urine apoAI levels compared to controls. In contrast, diseases involving primarily distal tubules, i.e. distal RTA and Bartter syndrome, did not have elevated apoAI excretion. These results complement our unpublished studies characterizing tubular handling of apoAI. We studied two tubular injury models: diphtheria toxin (DT) transgenic mouse expressing the human DT receptor in proximal tubular epithelial cells and in which DT injection causes acute tubular injury, and the folic acid injury model, where injected folic acid forms crystals in the distal nephron with distal tubular injury. Compared to baseline, mice with DT-induced proximal tubular injury had doubling in urine apoAI excretion, reduced proximal tubule expression of cubilin, and localization of apoAI to the apical membrane. By contrast, folic acid injury caused only subtle change in urinary apoAI. These observations and our current data provide strong support that the proximal, but not distal, tubule is critical in renal handling of apoAI.
Previously, elevated urinary apoAI was reported in patients with nephrolithiasis and was even suggested as a possible marker of renal stone disease [28]. We found no increase in urinary apoAI in 38 patients with active kidney stones, history of kidney stones, and/or active urine mineral derangements, such as hyperuricemia, hypercalcemia or hypocitraturia. Elevated urinary apoAI was not seen in patients with nephrocalcinosis alone, but was observed in the context of nephrocalcinosis with proximal tubule dysfunction, i.e. Dent disease, reiterating the link between the proximal tubules and increased urinary apoAI excretion. Of note, the previous study linking nephrolithiasis and elevated urinary apoAI was in hospitalized adult patients who underwent surgical intervention for stones [28]. This clinical scenario infers acute obstruction with possible infection. Our population included children seen for routine care, who were neither acutely obstructed nor infected. Our results do not support utility of urinary apoAI to identify children with stone disease.
In addition to proximal tubular dysfunction, our results indicate that disruption of the glomerular filtration barrier that characterizes glomerular disease, including GN and NS, increases urinary apoAI (Figure 3). However, the pattern of apoAI excretion and the relationship to the “gold-standard” marker of glomerular disruption, namely, albuminuria is noteworthy. Children with active NS had greater urinary apoAI than controls or patients with NS in remission, a result that was largely driven by increased urinary apoAI in patients with FSGS. Thus, although relapse in patients with MCD and FSGS caused a comparable degree of albuminuria, FSGS patients had significantly higher urinary apoAI levels than those with MCD. Children with MCD had similar urinary apoAI as controls, even in relapse. There was little correlation with ACR among patients in relapse (Spearman’s Rho 0.147, p=0.62). The dissociation between apoAI and ACR was observed not only in NS but, to varying degrees, in all disorders represented in our population. These results suggest potentially distinct pathways for tubular uptake of filtered albumin and apoAI. Filtered albumin is taken up by high-affinity, high capacity megalin-cubilin receptor complex and endocytosis involving the neonatal Fc receptor [32]. Megalin-cubilin is also the primary pathway for salvage of filtered apoAI. However, the role of other lipoprotein transporters, such as ABCA1, ABCG1 and SR-BI, present along the nephron is currently unknown. How these pathways are altered by renal injury is currently not understood, but may significantly affect the urinary protein profile in renal disease.
Aside from increased quantity of urinary apoAI, our data also show that urine of patients with certain renal diseases contains irregular HMW forms of apoAI. This may be critical since modification in the apoAI/FIDL structure and composition reflected by changes in the molecular weight not only causes loss of their protective actions but also converts the lipoproteins into potentially toxic biological agents [33–35]. While many children with renal disease in our population had HMW bands, all children with relapsed NS due to FSGS excreted multiple HMW forms of apoAI. These are interesting observations since cross-linking of apoAI produces HMW dimers and trimers with impaired functionality, including decreased ability to bind lipopolysaccharides, efflux cellular cholesterol, and to inhibit cytokine response [35]. It is therefore possible that appearance of HMW species in urine of patients with renal disease reflects a detrimental environment, e.g. high oxidative stress favoring generation of oxidized lipids / lipoproteins that crosslink to produce subpopulations of larger size. Whether the composition and modification of apoAI-HMW species observed in subjects with other kidney diseases are like those seen in patients with FSGS can be addressed in future studies.
Although excretion of these HMW apoAI forms was noted during relapse but not remission of FSGS, it did not parallel the quantity of urinary apoAI nor the quantity of albuminuria. These findings are interesting in view of a proteomic analysis of plasma and urine samples in patients with recurrent FSGS post-transplantation [31]. The authors reported the presence of a modified apoAI with a slightly higher molecular weight than authentic apoAI that differentiated recurrent FSGS from non-recurrence with a sensitivity of 93% and a specificity of 98%. Nearly every patient with recurrence had the modified apoAI in their urine, while none had it present in the serum. Our findings complement these data and suggest the intriguing possibility that the intrarenal milieu in FSGS promotes apoAI modification, and this modified apoAI then appears in the urine. Whether it has a pathogenic role in renal injury remains to be determined.
Differences in renal handling of apoAI between FSGS and MCD are further illustrated by the differences in localization of apoAI observed in our pilot study of renal biopsies. Compared to normal kidney, MCD and FSGS have more apoAI in proximal tubules (Figure 5). This observation suggests that increased filtered apoAI in NS is taken up by the tubules. In MCD, the apoAI is more diffusely distributed within the cytoplasm of the proximal tubule cells. By contrast, in FSGS, apoAI expression appeared not only in the cytoplasm, but was also strongly concentrated at the brush border of the apical membrane. This finding suggests the possibility that FSGS, but not MCD, is associated with impairment in the normal tubular structure / function which impedes normal uptake of filtered apoAI, reflected by the abnormal tubular distribution of apoAI together with increased urinary loss of apoAI. Interestingly, evidence of tubular injury has been observed in patients with FSGS, e.g. increased tubular apoptosis was described in renal biopsies from children with FSGS [36]. It is also possible that FSGS in relapse provides a conducive environment for crosslinking of apoAI into HMW forms that contribute to differences in tubular handling between the two diseases. Whether these findings can be used to differentiate FSGS and MCD requires further study. Clearly, study of additional patient biopsies to confirm these preliminary observations is warranted.
Our study has several limitations, including the observational nature of examining “all comers” at a single center. Additional studies with a larger number of patients with specific diseases are needed. We are also limited by the heterogeneity of disease severity and treatment within each disease type and the variable time between diagnosis and urinary apoAI measurement. Nevertheless, the differences in the quantity and quality of urinary apolipoproteins among different kidney diseases generate many hypotheses regarding urinary apolipoproteins as potential markers or even mediators of renal injury.
In conclusion, children with kidney disease have increased urinary apoAI that varies among diseases. Urine apoAI is particularly elevated in proximal tubulopathies, dysplasia and proteinuric glomerular diseases, but only modestly parallels the magnitude of albuminuria. Further, certain diseases, most notably FSGS, excrete high molecular weight forms of apoAI that are not linked to the concentration of apoAI. These findings suggest the potential utility of measuring urinary apoAI to identify abnormal renal handling of lipoproteins and reflecting renal disease.
Acknowledgments and grant funding:
This research was supported by the following grants: NIH 1P01HL116263, NIH UL1 TR002243, and NIH UL1 TR000445.
We thank the clinical and nursing staff in the Vanderbilt Pediatric Nephrology Clinic and the Adolescent Clinic, who were key in sample collection. The authors also acknowledge the expert technical assistance of Cathy Xu.
Footnotes
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of a an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
Conflict of interest
The authors have no conflicts of interest to disclose.
Compliance with ethical standards
The study was approved by the Institutional Review Board at Vanderbilt University Medical Center. A waiver of consent was granted for patients who submitted urine as part of their routine care. Controls were consented and asked to provide a urine sample for study purposes.
References
- 1.Khera AV, Demler OV, Adelman SJ, Collins HL, Glynn RJ, Ridker PM, Rader DJ, Mora S (2007) Cholesterol Efflux Capacity, High-Density Lipoprotein Particle Number, and Incident Cardiovascular Events: An Analysis From the JUPITER Trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin). Circulation 135:2494–2504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rohatgi A, Khera A, Berry JD, Givens EG, Ayers CR, Wedin KE, Neeland IJ, Yuhanna IS, Rader DR, de Lemos JA, Shaul PW (2014) HDL cholesterol efflux capacity and incident cardiovascular events. N Engl J Med 371:2383–2393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhou L, Li C, Gao L, Wang A (2015) High-density lipoprotein synthesis andmetabolism (Review). Mol Med Rep 12:4015–4021 [DOI] [PubMed] [Google Scholar]
- 4.Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, Wood AM, Lewington S, Sattar N, Packard CJ, Collins R, Thompson SG, Danesh J (2009) Major lipids, apolipoproteins, and risk of vascular disease. JAMA 302:1993–2000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R (2010) Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 376:1670–1681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Annema W, von Eckardstein A (2013) High-density lipoproteins. Multifunctional but vulnerable protections from atherosclerosis. Jpn Circ J 77:2432–2448 [DOI] [PubMed] [Google Scholar]
- 7.Tall AR, Yvan-Charvet L (2015) Cholesterol, inflammation and innate immunity. Nat Rev Immunol 15:104–116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zamanian-Daryoush M, Lindner D, Tallant TC, Wang Z, Buffa J, Klipfell E, Parker Y, Hatala D, Parsons-Wingerter P, Rayman P, Yusufishaq MS, Fisher EA, Smith JD, Finke J, DiDonato JA, Hazen SL (2013) The cardioprotective protein apolipoprotein A1 promotes potent anti-tumorigenic effects. J Biol Chem 288:21237–21252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rye KA, Barter PJ, Cochran BJ (2016) Apolipoprotein A-I interactions with insulin secretion and production. Curr Opin Lipidol 27:8–13 [DOI] [PubMed] [Google Scholar]
- 10.Kontush A, Chantepie S, Chapman MJ (2003) Small, dense HDL particles exert potent protection of atherogenic LDL against oxidative stress. Arterioscler Thromb Vasc Biol 23:1881–1888 [DOI] [PubMed] [Google Scholar]
- 11.Monette JS, Hutchins PM, Ronsein GE, Wimberger J, Irwin AD, Tang C, Sara JD, Shao B, Vaisar T, Lerman A, Heinecke JW (2016) Patients With Coronary Endothelial Dysfunction Have Impaired Cholesterol Efflux Capacity and Reduced HDL Particle Concentration. Circ Res 119:83–90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.de Souza JA, Vindis C, Negre-Salvayre A, Rye KA, Couturier M, Therond P, Chantepie S, Salvayre R, Chapman MJ, Kontush A (2010) Small, dense HDL 3 particles attenuate apoptosis in endothelial cells: pivotal role of apolipoprotein A-I. J Cell Mol Med 14:608–620 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Saleheen D, Scott R, Javad S, Zhao W, Rodrigues A, Picataggi A, Lukmanova D, Mucksavage ML, Luben R, Billheimer J, Kastelein JJ, Boekholdt SM, Khaw KT, Wareham N, Rader DJ (2015) Association of HDL cholesterol efflux capacity with incident coronary heart disease events: a prospective case-control study. Lancet Diabetes Endocrinol 3:507–513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tsuchida Y, Zhong J, Otsuka T, Dikalova A, Pastan I, Anantharamaiah GM, Linton MF, Yancey PG, Ikizler TA, Fogo AB, Yang H, Kon V (2019) Lipoprotein Modulation of Proteinuric Renal Injury. Lab Invest. doi: 10.1038/s41374-019-0253-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Moreira RS, Irigoyen M, Sanches TR, Volpini RA, Camara NO, Malheiros DM, Shimizu MH, Seguro AC, Andrade L (2014) Apolipoprotein A-I mimetic peptide 4F attenuates kidney injury, heart injury, and endothelial dysfunction in sepsis. Am J Physiol Regul Integr Comp Physiol 307:R514–524 [DOI] [PubMed] [Google Scholar]
- 16.Souza AC, Bocharov AV, Baranova IN, VIshnyakova TG, Huang YG, Wilkins KJ, Hu X, Street JM, Alvarex-Prats A, Mullick AE, Patterson AP, Remaley AT, Eggerman TL, Yuen PS, Star RA (2016) Antagonism of scavenger receptor CD36 by 5A peptide prevents chronic kidney disease progression in mice independent of blood pressure regulation. Kidney Int 89:809–822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Merscher-Gomez S, Guzman J, Pedigo CE, Lehto M, Aquillon-Prada R, Mendez A, Lassenius MI, Forsblom C, Yoo T, Villarreal R, Maiguel D, Johnson K, Goldberg R, Nair V, Randolph A, Kretzler M, Nelson RG, Burke GW 3rd, Groop PH, Fornoni A; FinnDiane Study Group (2013) Cyclodextrin protects podocytes in diabetic kidney disease. Diabetes 62:3817–3827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pedigo CE, Ducasa GM, Leclercq F, Sloan A, Mitrofanova A, Hashmi T, Molina-David J, Ge M, Lassenius MI, Forsblum C, Lehto M, Groop PH, Kretzler M, Eddy S, Martini S, Reich H, Wahl P, Ghiggeri G, Faul C, Burke GW 3rd, Kretz O, Huber TB, Mendez AJ, Merscher S, Fornoni A (2016) Local TNF causes NFATc1-dependent cholesterol-mediated podocyte injury. J Clin Invest 126:3336–3350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mitrofanova A, Molina J, Varona Santos J, Guzman J, Morales XA, Ducasa GM, Bryn J, Sloan A, Volosenco I, Kim JJ, Ge M, Mallela SK, Kretzler M, Eddy S, Martini S, Wahl P, Pastori S, Mendez AJ, Burke GW, Merscher S, Fornoni A (2018) Hydroxypropyl-beta-cyclodextrin protects from kidney disease in experimental Alport syndrome and focal segmental glomerulosclerosis. Kidney Int 94:1151–1159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hammad SM, Barth JL, Knaak C, Argraves WS (2000) Megalin acts in concert with cubilin to mediate endocytosis of high density lipoproteins. J Biol Chem 275:12003–12008 [DOI] [PubMed] [Google Scholar]
- 21.Nielsen R, Christensen EI, Birn H (2016) Megalin and cubilin in proximal tubule protein reabsorption: from experimental models to human disease. Kidney Int 89:58–67 [DOI] [PubMed] [Google Scholar]
- 22.Aseem O, Smith BT, Cooley MA, Wilkerson BA, Argraves KM, Remaley AT, Argraves WS (2014) Cubilin maintains blood levels of HDL and albumin. J Am Soc Nephrol 25:1028–1036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Heilskov GJ, Graciela C, Abdelmejid K, Henning N, Ilsø CE, Anthony N, Kragh MS(2008) A Pivotal Role of the Human Kidney in Catabolism of HDL Protein Components Apolipoprotein A-I and A-IV but not of A-II. Lipids 43:467–470 [DOI] [PubMed] [Google Scholar]
- 24.Yang H, Fogo AB, Kon V (2016) Kidneys: key modulators of high-density lipoprotein levels and function. Curr Opin Nephrol Hypertens 25:174–179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gomo ZA, Henderson LO (1988) High-density lipoprotein apolipoproteins in urine: II.Enzyme-linked immunoassay of apolipoprotein A-I. Clin Chem 34:1781–1786 [PubMed] [Google Scholar]
- 26.Kronenberg F, Kuen E, Ritz E, Konig P, Kraatz G, Lhotta K, Mann JF, Muller GA, Neyer U, Riegel W, Riegler P, Schwenger V, von Eckardstein A (2002) Apolipoprotein A-IV serum concentrations are elevated in patients with mild and moderate renal failure. J Am Soc Nephrol 13:461–469 [DOI] [PubMed] [Google Scholar]
- 27.Mack S, Coassin S, Vaucher J, Kronenberg F, Lamina C (2017) Evaluating the Causal Relation of ApoA-IV with Disease-Related Traits - A Bidirectional Two-sample Mendelian Randomization Study. Sci Rep 7:8734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zhu W, Liu M, Wang GC, Peng B, Yan Y, Che JP, Ma QW, Yao XD, Zheng JH(2014) Fibrinogen alpha chain precursor and apolipoprotein A-I in urine as biomarkers for noninvasive diagnosis of calcium oxalate nephrolithiasis: a proteomics study. Biomed Res Int 2014:415651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Calabresi L, Simonelli S, Conca P, Busnach G, Cabibbe M, Gesualdo L, Gigante M, Penco S, Veglia F, Franceschini G (2015) Acquired lecithin:cholesterol acyltransferase deficiency as a major factor in lowering plasma HDL levels in chronic kidney disease. J Intern Med 277:552–561 [DOI] [PubMed] [Google Scholar]
- 30.Li C, Li H, Zhang T, Li J, Liu L, Chang J (2014) Discovery of Apo-A1 as a potentialbladder cancer biomarker by urine proteomics and analysis. Biochem Biophys Res Commun 446:1047–1052 [DOI] [PubMed] [Google Scholar]
- 31.Lopez-Hellin J, Cantarell C, Jimeno L, Sanchez-Fructuoso A, Puig-Gay N, Guirado L, Vilarino N, Gonzalez-Roncero FM, Mazuecos A, Lauzurica R, Burgos D, Plumed JS, Jacobs-Cacha C, Jimenez C, Fernandez A, Fernandez-Alvarez P, Torregrosa V, Nieto JL, Meseguer A, Alonso A (2013) A form of apolipoprotein a-I is found specifically in relapses of focal segmental glomerulosclerosis following transplantation. Am J Transplant 13:493–500 [DOI] [PubMed] [Google Scholar]
- 32.Dickson LE, Wagner MC, Sandoval RM, Molitoris BA (2014) The proximal tubule and albuminuria: really! J Am Soc Nephrol 25:443–453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yoshifumi K, Tomoaki T, Shinichi M, Tohru A, Tatsumi M, Zensuke O (2013)Semiquantitative Analysis of Apolipoprotein A-I Modified by Advanced Glycation End Products in Diabetes Mellitus. J Clin Lab Anal 27:231–236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hewing B, Parathath S, Barrett T, Chung WK, Astudillo YM, Hamada T, Ramkhelawon B, Tallant TC, Yusufishaq MS, Didonato JA, Huang Y, Buffa J, Berisha SZ, Smith JD, Hazen SL, Fisher EA (2014) Effects of native and myeloperoxidase-modified apolipoprotein a-I on reverse cholesterol transport and atherosclerosis in mice. Arterioscler Thromb Vasc Biol 34:779–789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.May-Zhang LS, Yermalitsky V, Huang J, Pleasent T, Borja MS, Oda MN, Jerome WG, Yancey PG, Linton MF, Davies SS (2018) Modification by isolevuglandins, highly reactive gamma-ketoaldehydes, deleteriously alters high-density lipoprotein structure and function. J Biol Chem 293:9176–9187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Erkan E, Garcia CD, Patterson LT, Mishra J, Mitsnefes MM, Kaskel FJ, Devarajan P(2005) Induction of renal tubular cell apoptosis in focal segmental glomerulosclerosis: roles of proteinuria and Fas-dependent pathways. J Am Soc Nephrol 16:398–407 [DOI] [PubMed] [Google Scholar]