

Abstract
Introduction
Recurrent pregnancy loss (RPL) is defined as three or more spontaneous pregnancy losses before the 20th week of gestation or fetal weight of < 500 gm from the last menstrual period. Vascular endothelial growth factor (VEGF) is essential for implantation, development of embryo and placental angiogenesis. Women with low VEGF level are believed to be at higher risk of RPL.
Objective
To measure the level of VEGF in women with RPL and compare it with women with 1 or more successful pregnancies.
Methods
This is a Case control study carried out in King George Medical University, Lucknow from August 2015 to 2016. Participants sample size was 60 women. Thirty women with 3 or more spontaneous abortions were included as cases, and 30 women with at least 1 successful term pregnancy were controls. Serum VEGF level was analyzed using ELISA kit. Main outcome measured: 1. Serum VEGF level in the two groups. 2. Serum VEGF level in different underlying etiologies in women with RPL.
Results
Mean VEGF level was 105.3 pg/mL in RPL cases, while it was 156.8 pg/mL in fertile controls. (p = 0.01). VEGF level was 86.2 pg/mL in patients with anatomical defects, 109 pg/mL in APLA syndrome, 85.1 pg/mL in hypothyroidism and 122.2 pg/mL in unexplained RPL.
Conclusion
The mean serum VEGF level was significantly lower in women with recurrent pregnancy loss compared with women with successful term pregnancy, implicating its role in maintaining pregnancy.
Keywords: Recurrent pregnancy loss, Vascular endothelial growth factor (VEGF), Antiphospholipid syndrome
Introduction
Recurrent pregnancy loss (RPL), also known as recurrent spontaneous abortions, is defined as three or more spontaneous pregnancy losses before the 20th week of gestation or fetal weight of < 500 gm from the last menstrual period [1, 2]. The American Society for Reproductive Medicine defines recurrent pregnancy loss as two or more failed clinical pregnancies confirmed by ultrasonography or histopathological examination. It is generally accepted that evaluation of couples should begin after 2 abortions. Incidence of RPL is 1% [3].
PRIMARY RECURRENT PREGNANCY LOSS is repeated abortion in which a pregnancy has never been carried to viability.
SECONDARY RECURRENT PREGNANCY LOSS is repeated abortion in which a live birth has occurred at some time [1].
Many etiological factors have been implicated as a cause of recurrent pregnancy, and the main factors being [2, 4] Chromosomal anomalies (3.5–5%) like balanced translocations and single gene defects; Anatomical defects (12–16%)including incomplete müllerian fusion, cervical incompetence, synechiae, fibroids and adenomyosis; Endocrine abnormalities (17–20%) such as PCOS, diabetes, thyroid and prolactin disorders; and Immunological factors (20–50%) like antiphospholipid syndrome (APS) and antithyroid antibody [1–6].
Other causes such as Alloimmunopathology, inherited thrombophilias (Factor V Leiden and others), infections (genital mycoplasmas, toxoplasma, rubella) and environmental exposures (smoking, heavy alcohol or caffeine consumption) have been proposed but not established [1–6].
Vascular endothelial growth factor (VEGF), also known as vascular permeability factor (VPF), is an angiogenic cytokine secreted by vascular smooth muscle cells, corpus luteum, endometrium and placenta. It is essential for oocytes maturation, proliferation of trophoblasts, implantation and development of the embryo, the angiogenesis and vasculogenesis. It regulates the integrity of endothelial cells during embryogenesis, and hence contributes to optimal vascular shape and function and participates in placentation by increasing angiogenesis, vascular permeability and trophoblast invasion, which are required for successful implantation [5, 7, 8].
Polymorphism in VEGF gene is associated with altered serum levels of VEGF protein.
Due to involvement of VEGF in angiogenesis and association of recurrent pregnancy loss with uteroplacental insufficiency and implantation defects, it is believed that women carrying low expression alleles and hence lower blood levels of VEGF are at higher risk of spontaneous abortion [5, 7–9].
Therefore in our study, we aim to measure the serum VEGF level in non-pregnant women with three or more spontaneous abortions and compare the level with women who had 1 or more successful term pregnancy (and no abortions) and evaluate the difference between the two groups. The serum VEGF level was assessed in relation to number of abortions and underlying etiology.
Aims and Objectives
To assess the level of vascular endothelial growth factor (VEGF) in cases of recurrent pregnancy loss (RPL) and compare it with women with one or more successful term pregnancies.
To evaluate the underlying etiology in patients with Recurrent Pregnancy Loss.
To compare the level of VEGF in women with unexplained RPL, and compare it with other underlying causes of RPL and to assess if a difference exists between them.
Methodology
This is a case control study, conducted on women attending outdoor clinic or admitted in the Department of Obstetrics and Gynaecology, KGMU, Lucknow over a period of 1 year from August 2015 to August 2016. The calculated sample size was 30 cases and 30 controls. Thirty non-pregnant women of age 18–40 years with 3 or more spontaneous abortions were included in cases and formed group I. Women with induced abortion/s, postabortal women (within 6 weeks of abortion), pregnant women and patients who refuse to participate in the study were excluded from the cases.
Thirty non-pregnant women of age 18–40 years with at least one successful pregnancy (rest matched with cases) and no spontaneous abortions formed group II, i.e., controls. Women with 1 or more spontaneous abortion, postpartum women (within 6 weeks of abortion or delivery), pregnant women and patients who refuse to participate in the study were excluded from the study.
Ethical clearance was obtained from Institutional ethical committee, Office of research cell, KGMU, Lucknow (ref no 7963/ethics/R cell-15, dated April 12, 2015).
After taking informed consent, cases and controls were recruited for the study and worked up.
Detailed history was taken including age of both partners, duration of marriage, menstrual history, details of previous abortions and live births, whether HPE/chromosomal study of abortus was performed in past, personal history, any known medical illness and relevant family history.
General physical examination including vital parameters (pulse, BP, temperature, respiratory rate), systemic examination, per abdominal examination, per speculum examination and per vaginal examination were performed.
Investigations
Basic investigations which included hemogram, blood group, HIV testing, hepatitis C testing, HBsAg, urine routine microscopy and chest X-ray were done in both groups.
Specific investigations included blood sugar Fasting/Post Prandial/HbA1c level, Serum T3, T4, Thyroid stimulating hormone (fasting sample), coagulation study (Prothrombin Time (PT)/activated Partial Thromboplastin Time (aPTT)), Antiphospholipid syndrome: Lupus Anticoagulant (LAC), anticardiolipin antibody (ACL), β2 glycoprotein; karyotype of both partners and anatomic study of uterus and adnexa either by hysterosalpingography (HSG) or Diagnostic Laparoscopy and Hysteroscopy. These investigations were done in women with recurrent pregnancy loss only.
A 5 mL venous sample was collected in both groups, irrespective of fasting state, serum was separated and stored at − 80 °C for measuring vascular endothelial growth factor (VEGF) level. Human VEGF ELISA kit from Boster Immunoleader company was used to assess the serum VEGF level. The sensitivity of the assay was < 1 pg/mL.
Results
Of the total 30 women in recurrent pregnancy loss (RPL) group, i.e., group I, 23 women (77%) had primary recurrent pregnancy loss, and seven women (23%) had Secondary RPL (Fig. 1).
Fig. 1.
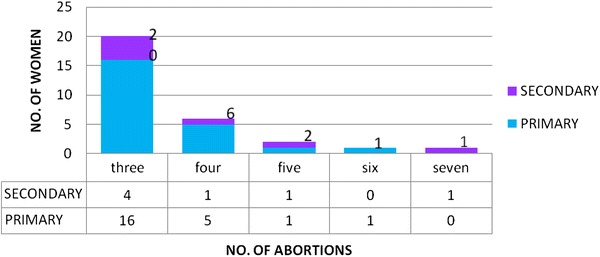
Distribution of women in recurrent pregnancy loss group (cases) according to number of abortions, and their respective distribution into primary and secondary RPL (n = 30)
In a total of 30 women in group I, i.e., cases, 115 conceptions occurred, of which 107 were abortions (106 first trimester and 1st trimester), rest were preterm/term pregnancies.
The basic characteristics are summarized in Table 1. The age, husband’s age, ethnicity, dietary habits, duration of marriage, age at menarche, height, weight, body mass index, blood pressure and hemoglobin level were not significantly different between the two groups. The trend was toward older couple and obesity among women with recurrent pregnancy loss. The age at first conception was significantly lower in fertile women with successful pregnancy outcomes (20 years) compared to women with recurrent pregnancy loss, where the age was 23 years. (p = 0.0001).
Table 1.
Comparison of basic characteristics between cases and controls
| S no | Characteristic | Cases | Control | P value |
|---|---|---|---|---|
| 1 | Age (year) | 28.9 | 28.2 | 0.57 |
| 2 | Husband’s age (year) | 31.7 | 30.9 | 0.40 |
| 3 | Ethnicity: Hindu (%) | 86.7 | 86.7 | 1.0 |
| 4 | Ethnicity: Muslim (%) | 13.3 | 13.3 | 1.0 |
| 5 | Diet: vegetarian (%) | 76.7 | 86.7 | 0.31 |
| 6 | Diet: non-vegetarian (%) | 23.3 | 13.3 | 0.31 |
| 7 | Duration of marriage (year) | 7.6 | 8.5 | 0.33 |
| 8 | Age at menarche (year) | 13.23 | 13.0 | 0.85 |
| 9 | Age at first conception (year) | 23 | 20 | 0.001 |
| 10 | Height (cm) | 151 | 149 | 0.36 |
| 11 | Weight (kg) | 57 | 54 | 0.19 |
| 12 | BMI (kg/m2) | 25.2 | 24.0 | 0.20 |
| 13 | Systolic blood pressure (mmHg) | 112.2 | 111.2 | 0.63 |
| 14 | Diastolic blood pressure (mmHg) | 69.4 | 67.2 | 0.22 |
| 15 | Hemoglobin (g%) | 11.2 | 11.7 | 0.11 |
The cause of recurrent pregnancy loss could be identified in 56.7% cases, while it was unidentified in 43.3% cases.
Hypothyroidism was the most predominant factor, present in 30% of total patients. Hyperprolactinemia was present in two (6.6%) patients, and two patients had multiple medical disorders.
Anatomical defects were identified in six women, of which, one had septate uterus, one had bicornuate uterus, two had intra uterine adhesions (both associated with hypothyroidism), and two had fibroids which distorted cavity.
There were three patients of antiphospholipid antibody syndrome (APS): two primary and one secondary APS (was associated with systemic lupus erythematosus and Raynaud’s disease).
Of the total 30 couples, one couple was found to have genetic abnormality in husband [46 XY, t(15; Y) (q12; q11)], while karyotype of wife was found to be normal in all (Fig. 2).
Fig. 2.
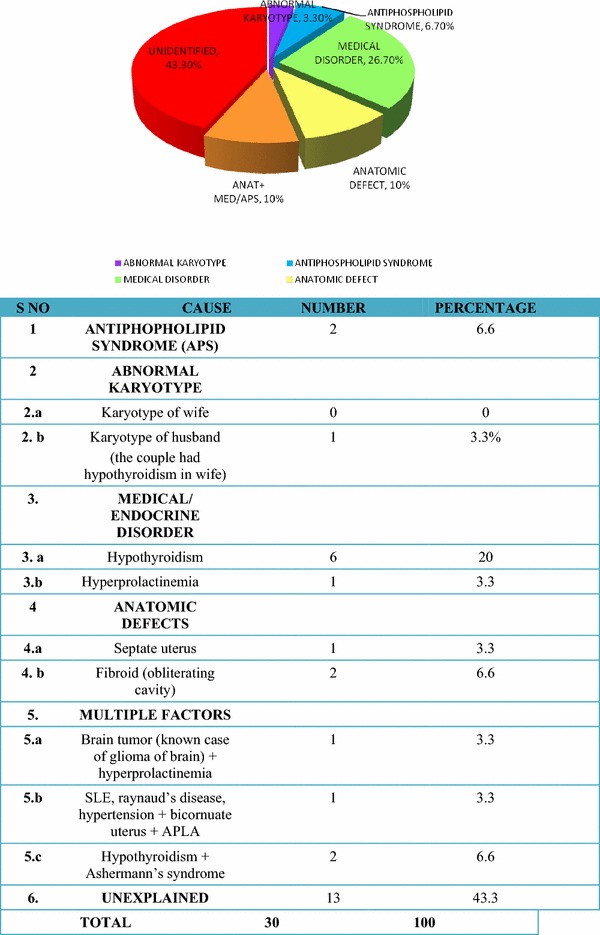
The underlying factors in cases with recurrent spontaneous abortion (n = 30)
The mean value of serum vascular endothelial growth factor was 105.3 pg/mL in cases (women with recurrent pregnancy loss) and 156.06 pg/mL in controls (women with successful pregnancy/pregnancies). (p = 0.01) (Fig. 3).
Fig. 3.
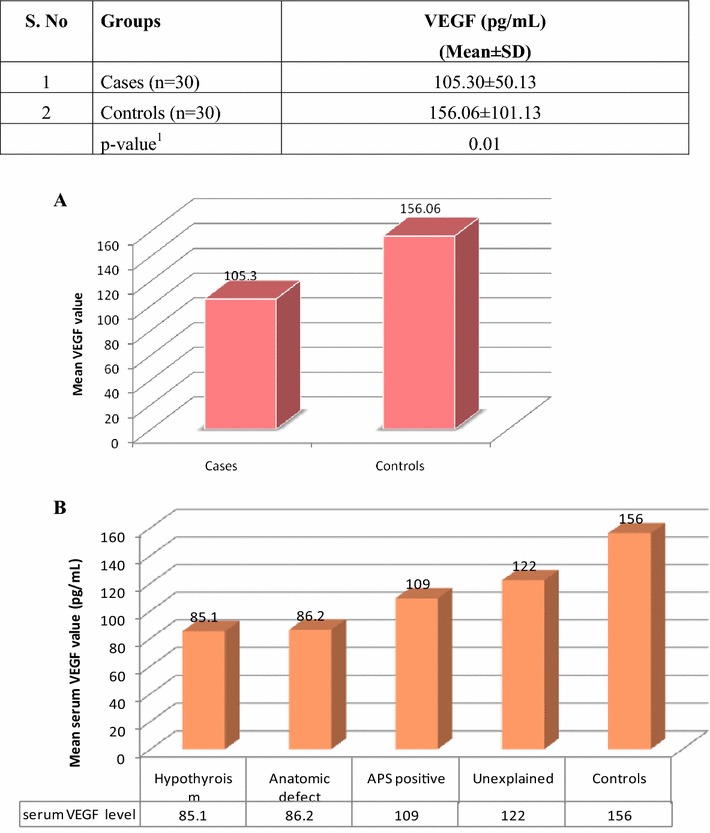
a Comparison of serum VEGF level between cases and controls (n = 60). b Comparison of mean serum VEGF level with number of abortions and underlying etiology in recurrent pregnancy loss cases (n = 30)
VEGF level was inversely related to number of abortions.
The mean VEGF level in patients with hypothyroidism was 85.1 pg/mL, in patients with anatomical defects was 86.2 pg/mL, in patients with antiphospholipid syndrome was 109 pg/mL, and in unexplained RPL was 122 pg/mL, while in controls (group II) it was 156 pg/mL (Fig. 3).
The area under the curve was 0.65 for the serum VEGF cutoff of ≤ 120 pg/mL (95% CI 0.51–0.79), and the p value was calculated to be 0.04, which was statistically significant. At this cutoff, the sensitivity of the test was predicted to be 63.3%, specificity was 56.7%, positive predictive value of 59.4%, negative predictive value of 60.7% and accuracy of 60% (Fig. 4).
Fig. 4.
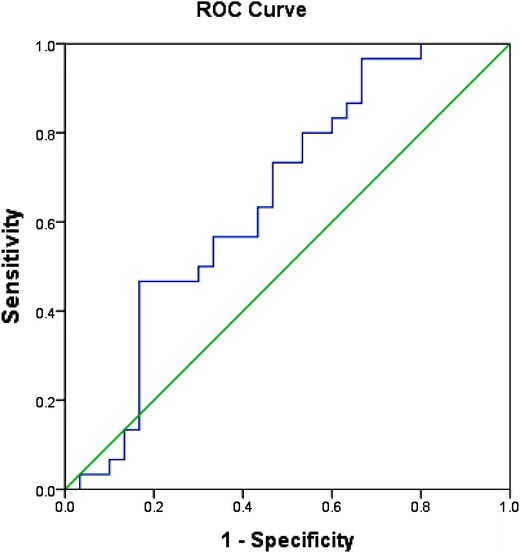
Receiver operating characteristic (ROC) curve for VEGF at a cutoff of 120 pg/mL
Discussion
Main Findings
Recurrent pregnancy loss continues to be one of the major obstetric problems faced by couples visiting our outpatient clinic. With changing lifestyle, the incidence of recurrent pregnancy loss is expected to rise.
Of the epidemiological characteristics, the most important factor identified was age at first conception. It was seen that women with recurrent pregnancy loss had their first pregnancy at older age compared to women with successful pregnancies, and this result was statistically significant. Also, there was a trend toward increased body mass index.
The underlying etiology for recurrent pregnancy loss could be identified in about 56.7% patients: of which 26.7% had endocrine/medical disorder; 10% had anatomical defect of the uterus; 10% had a combination of anatomical and endocrine factor; 6.7% patients were APLA positive, and 3.3% patients had genetic abnormality, while in 43.3% patients cause was unexplained.
The mean serum VEGF was lower in women with RPL, and the difference was statistically significant (Fig. 3).
Previous studies by Wassim et al. and Al-Khateeb et al. [7] which studied VEGF level only in unexplained recurrent pregnancy loss, found the level to be reduced as compared to healthy controls, while study by Amirchaghmaghi et al. [9] found higher VEGF level in recurrent pregnancy loss patients. These studies present a conflicting result as far as the serum VEGF level is considered in women with RPL.
In our study, we included all patients of recurrent pregnancy loss, and the level of VEGF was correlated with underlying cause. It was found that the level of VEGF was lower in cases compared to healthy controls (105.3 ± 30 vs. 156 ± 101 pg/mL). Women with RPL, where an underlying cause could be identified, had a lower level as compared to women with unexplained RPL.
The level of VEGF was found to be lowest in hypothyroidism, followed by women with anatomical abnormality, followed by women who were antiphospholipid antibody positive. In either case, the level was lower than unexplained RPL.
This finding is different from all the previous studies, and this aspect has been undiscovered till now.
While the previous studies focused on the possible role of VEGF-gene polymorphism leading to a lower serum VEGF level in women with unexplained RPL as a cause of their pregnancy loss, our study included women with RPL who had an underlying etiology and found that such women also had lower VEGF level compared to women with successful term pregnancies. VEGF level in patients with an identified underlying etiology for RPL.
Our study has shown a completely new dimension to the topic. The possibility of all the etiologies leading to a lower serum VEGF level and hence recurrent pregnancy loss is proposed by us. The mechanism for the same needs to be further studied.
What we propose is that VEGF may be a final common pathway of action of all these other factors. Different factors may lead to low VEGF level that ultimately leads to recurrent pregnancy loss.
Strengths
Limited number of studies have been done on the matter with conflicting results. Our result is consistent with the larger studies by Wassim et al. and Al-Khateeb et al. [7].
No study has been done to evaluate serum VEGF level in Indian subcontinent.
Our study evaluates the causes of recurrent pregnancy loss and studies association of VEGF with underlying cause which has not been done previously.
Also, this study evaluates the VEGF level with underlying etiology, which has not been studied previously.
Limitations
Sample size is small, and hence larger studies need to be done to confirm the findings.
The study is done in Indian population, and the results may not be applicable to other populations.
Interpretation
Serum VEGF level is reduced in women with recurrent pregnancy loss. The more the number of abortions, the lower is the serum VEGF level. Serum VEGF level was lower in women with underlying etiology compared to women with unexplained RPL. In either case, the level was lower than controls.
Previous studies on the matter have focused on the role of VEGF polymorphism and resultant serum VEGF level in women with unexplained RPL.
Our study clearly points toward the role of serum VEGF in women with an underlying etiology. How the different etiologies cause a reduction in serum VEGF level needs to be further studied.
Conclusion
The serum vascular endothelial growth factor level is lower in women with recurrent pregnancy loss as compared with women with one or more successful term pregnancy. The VEGF level is lower in women with underlying etiology as compared to unexplained recurrent pregnancy loss.
Dr. Pallavi Gupta
graduated with Bachelor of Medicine and Bachelor of Surgery (MBBS) from Gandhi Medical College (GMC) Bhopal in 2013 where she was awarded with distinction in Obstetrics and Gynecology and Ophthalmology; topper in Obstetrics and gynecology and ENT; and KK Munjal award for outstanding performance in ENT. She pursued postgraduation (MD) in Obstetrics and Gynecology from King George’s Medical University, Lucknow, India from 2014 to 2017. Following her postgraduation, she served as a senior resident in Hamdard Institute of Medical Sciences and Research (HIMSR) and HAHC hospital, New Delhi before joining University College of Medical Sciences (UCMS) and Guru Teg Bahadur Hospital (GTBH), New delhi, where she is currently working as a senior resident in obstetrics and gynecology. Her research activities are focussed on infertility and high-risk pregnancies.
Author’s contributions
PG collected patient data and samples, ELISA test of VEGF, statistical analysis, research and review of the literature, write-up of the article, submission and correspondence with editors. SD conceived the idea for the project and literature search, data analysis and write-up. SPJ reviewed the article and contributed to data analysis. PLS reviewed final article and did proofreading and data analysis.
Compliance with Ethical Standards
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical Standards
Ethical clearance was obtained from Institutional ethical committee, Office of research cell, KGMU, Lucknow, India, for the project titled “study of serum Vascular Endothelial Growth Factor (VEGF) level in cases of recurrent spontaneous abortion,” dated 4/12/2015, ref no 7963/ethics/R cell-15.
Research Involving Human Participants
Written and informed consent was taken from all participants.
References
- 1.Speroff L. Clinical gynaecologic endocrinology and infertility. 8. Philadelphia: Lippincott Williams & Wilkins; 2011. pp. 1191–1220. [Google Scholar]
- 2.Lathi RB, Schust DJ. Berek and Novak’s gynecology. 15. Philadelphia: Lippincott Williams & Wilkins; 2012. pp. 1190–1222. [Google Scholar]
- 3.Cunningham GF, Leveno K. Williams obstetrics. 24. New York: McGraw Hill Education; 2013. pp. 350–376. [Google Scholar]
- 4.Ford HB, Schust DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol. 2009;2:76–83. [PMC free article] [PubMed] [Google Scholar]
- 5.Goodman C, Jeyendran RS, Coula RS. Vascular endothelial growth factor gene polymorphism and implantation failure. Repr Biomed. 2008;16:720–723. doi: 10.1016/S1472-6483(10)60487-7. [DOI] [PubMed] [Google Scholar]
- 6.Egerup P, Kolte AM, Larsen EC, et al. Recurrent pregnancy loss: what is the impact of consecutive versus non-consecutive losses. Hum Reprod. 2016;31:2428–2434. doi: 10.1093/humrep/dew169. [DOI] [PubMed] [Google Scholar]
- 7.Al-Khateeb GM, Mustafa FE, Sater MS, et al. Effect of the functional VEGFA-583C/T variant on vascular endothelial growth factor levels and the risk of recurrent spontaneous miscarriage. Fertil Steril. 2011;95:2471–2473. doi: 10.1016/j.fertnstert.2011.03.010. [DOI] [PubMed] [Google Scholar]
- 8.Almawi WY, Saldanha FL, Mahmood NA, et al. Relationship between VEGFA polymorphisms and serum VEGF protein levels and recurrent spontaneous miscarriage: Department of Medical Biochemistry, College of Medicine and Medical Sciences, Manama, Bahrain. Department of Obstetrics and Gynecology Salmaniya Medical Complex, Manama, Bahrain; 2013. [DOI] [PubMed]
- 9.Amirchaghmaghi E, Rezaei A, Moini A, et al. Gene expression analysis of VEGF and its receptors and assessment of its serum level in unexplained recurrent spontaneous abortion. Cell J (Yakhteh) 2015;16:538. doi: 10.22074/cellj.2015.498. [DOI] [PMC free article] [PubMed] [Google Scholar]