

Abstract
Context
Sport specialization is thought to be a primary contributor to the throwing-related injury risk in youth baseball players.
Objective
To (1) establish arm-injury incidence in a cohort of male youth (9–12 years old) baseball players and (2) examine sport specialization and the frequency of arm injuries in the same cohort.
Design
Cohort study.
Setting
Greenville, South Carolina, youth baseball programs and tournaments.
Patients or Other Participants
A total of 159 asymptomatic youth baseball players (age = 11.1 ± 1.1 years) were physically assessed and then were prospectively followed for 6.7 ± 1.5 months.
Main Outcome Measure(s)
Athlete demographics and playing and injury histories were initially recorded. Athlete-exposures and presence of arm injury were prospectively tracked. All injuries were physically confirmed by a licensed physical therapist.
Results
Youth players demonstrated an arm-injury incidence rate of 2.22 per 1000 athlete-exposures. Parents and players underestimated sport-specialization status based on the standard research definition (self versus research based: 31% versus 83%, respectively; P = .001). The frequency of arm injuries was higher in specialized players (100%) than in nonspecialized players (80%, P = .03) but did not differ between pitchers and position players (13.2% each, P = 1.00).
Conclusions
Sport specialization was associated with throwing-related arm injuries in a small cohort of youth baseball players. It is concerning that 57.9% of parents and specialized players were unaware of the athletes' status. Larger studies with longer follow-up periods are needed to further evaluate injury-risk profiles in physically developing youth populations.
Keywords: arm pain, youth baseball, risk factors, position specialization
Key Points
This study was the first to examine the incidence of throwing-related arm injuries in youth baseball players while taking position into account.
Youth baseball players who competed as specialized athletes demonstrated a higher frequency of arm injuries than their nonspecialized counterparts.
The majority of youth baseball players misclassified themselves as nonspecialized athletes but competed as specialized athletes.
Continuing education is needed for youth athletes and their parents to better understand the definition of and risks associated with sport specialization.
Baseball is a popular sport in the United States, with approximately 13 to 17 million athletes under the age of 18 years participating at the club sport and high school levels.1–4 The incidence of baseball-related overuse injuries was fairly low in adolescent players (13–18 years old), with 1.3 to 4.0 injuries per 1000 athlete-exposures (AEs) recorded.5,6 The injury incidence in youth baseball players (9–12 years old) is unknown because epidemiologic data are lacking. The majority of baseball-related overuse injuries affect the shoulder and elbow; however, little is known about the causes and development of these injuries at the youth level.1,6
One potential explanation for the lack of epidemiologic data may be related to difficulties in injury surveillance, particularly of the younger age groups.7,8 Unlike the collegiate and professional ranks, which employ athletic trainers to record and treat athletes' injuries, at the youth and adolescent level, injuries are inconsistently reported and often treated by the athletes' parents and coaches.7,9 The burden of identifying and recording injuries is much greater at this level because most youth players participate on multiple teams and, in some cases, in multiple sports throughout the year.8
Despite evidence10,11 suggesting that sport specialization may be related to the development of overuse injuries in youth and adolescent athletes, specialization rates continue to rise in the United States. Prior researchers2,10,12,13 defined sport specialization on the basis of several criteria: year-round training in a single sport (greater than 8 months per year), identification of a primary sport over additional sports, and the cessation of additional sports to focus on a primary sport. Despite established definitions in the literature, less is understood about parents' and coaches' perceptions of sport specialization.10–14 The effects of sport specialization on the arm-injury risk have not been previously established in the baseball literature. Other risk factors, such as excessive pitch counts, varied pitch types, and faulty throwing mechanics, have been linked to the development of shoulder and elbow pain in youth throwers using self-reported survey data.10,12,15–20 The USA Baseball Medical/Safety Advisory Committee used this research to establish age-appropriate guidelines for pitch counts, pitch types, throwing mechanics and, most recently, a long-term athlete-development model released in 2017.16,21–23 The effectiveness of these recommendations on the incidence of baseball-related overuse injuries is unknown at this time.
The paucity of data describing the incidence of arm injuries in youth baseball players poses a significant knowledge gap because the extent of the problem has not been accurately established in this population. Whereas sport specialization has been associated with increased lower extremity and generalized injury risk in adolescent athletes, no investigators have examined its effect on the arm-injury risk in youth athletes.4,10 Therefore, the purposes of our study were to (1) establish the arm-injury incidence in a cohort of 9- to 12-year-old male baseball players and (2) examine sport specialization and the development of arm injuries in a cohort of 9- to 12-year-old male baseball players.
METHODS
Study Population
This was a prospective pilot study of competitive male youth baseball players (9–12 years old) recruited in the spring of 2016. A total of 261 players were initially recruited from local baseball clubs, baseball tournaments, and Little Leagues in Greenville, South Carolina. Athletes who consented to participate in the study were required to meet the following criteria: (1) no injuries that currently restricted the athlete's ability to participate in baseball activities, (2) no shoulder or elbow injuries that required medical attention during the 3 months before study enrollment, and (3) 3 or more follow-ups with the research team less than 2 months apart. A total of 102 players did not meet these criteria and were excluded from the study (Figure 1).
Figure 1.

Youth baseball study flowchart.
A total of 159 asymptomatic, competitive youth baseball players were included in this study. Players underwent a baseline flexibility and strength assessment by the research team to determine the presence of any preexisting arm injuries or symptoms such as pain, tightness, or weakness that might limit sport participation. Players were then prospectively followed for a 6-month period. All players were male, aged 9 to 12 years, and participating in all baseball activities without restriction at the time of assessment. Pitchers and position players were recruited for this study (Table). A position player was identified as any athlete who did not report pitching for an organized baseball team. The University of South Carolina Institutional Review Board approved this study. Parental consent and athlete assent were obtained for each participant enrolled.
Table.
Analysis of Risk Factors for Arm Injuries Among Youth Baseball Athletes
| Variable |
n (% of Total Cohort) |
Odds Ratio (95% Confidence Interval) |
P Value |
| Position | |||
| Pitchers | 106 (66.7) | 1.0 (0.4, 2.7) | 1.00 |
| Nonpitchers | 53 (33.3) | Referent | |
| Sport specialization? | |||
| Yes | 132 (83.0) | 6.7 (0.4, 118.0) | .03a |
| No | 27 (17.0) | Referent | |
| Position-specific training | |||
| Hitting lessons | 111 (69.8) | 1.1 (0.4, 3.0) | 1.00 |
| No hitting lessons | 48 (30.2) | Referent | |
| Pitching lessons | 72 (45.3) | 2.8 (1.1, 7.3) | .06 |
| No pitching lessons | 87 (54.7) | Referent | |
| Baseball-specific trainingb | 118 (74.2) | 2.3 (0.6, 8.2) | .29 |
| No baseball-specific trainingb | 41 (25.8) | Referent | |
| Generalized physical training | |||
| Strength and conditioning lessons | 36 (22.6) | 1.4 (0.5, 4.0) | .58 |
| No strength and conditioning lessons | 123 (77.4) | Referent | |
Indicates a difference using the Fisher exact test (P < .05).
Baseball-specific training consisted of only hitting lessons (n = 46), only pitching lessons (n = 7), or a combination (n = 65).
Data Collection
At the time of enrollment (spring 2016), each participant completed an initial intake questionnaire (Figure 2), with the help of a parent, before the baseline assessment. After the assessments, participants were contacted using follow-up questionnaires as well as phone and in-person interviews to corroborate data and improve response rates. All study questionnaires were administered via the REDCap online survey system (Nashville, TN).
Figure 2.
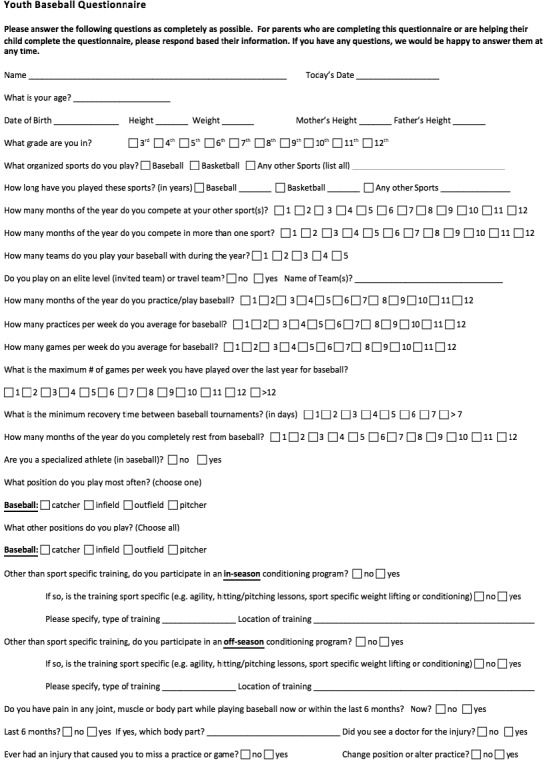
Online youth baseball study survey (REDCap, Nashville, TN). Presented in its original form.
The initial online questionnaire surveyed baseline characteristics, current sports participation, baseball-specific playing history (ie, positions played), current training history (ie, position-specific versus generalized physical training), and injury history (ie, previous injuries that required medical attention in the 3 months before study enrollment). Follow-up questionnaires were completed every 2 weeks over the course of 6 months. They surveyed baseball-related AEs (ie, 1 team practice or game = 1 AE), first by team and then confirmed using individual reports, as well as the presence of injury.
An injury was defined as any shoulder or elbow impairment (ie, pain, injury, tightness, or weakness) that resulted in either (1) an athlete missing >1 practice or game or (2) a change in position (ie, moving from pitcher to first base) related to the upper extremity complaint.6–9 Any player who reported a baseball-related shoulder or elbow impairment was contacted and then physically reassessed by the lead researcher, a licensed physical therapist, to confirm the presence of injury. Athletes who required additional medical care were referred to a board-certified, fellowship-trained sports medicine physician for continued evaluation.
Sport-Specialization Status
Parents and players were asked to classify the study participant as either a specialized or nonspecialized athlete, based on their own perceptions of what constituted a specialized athlete, at the time of enrollment (Figure 2). The research team then reclassified each participant as specialized or nonspecialized, based on whether the athlete met at least 2 of the 3 research-based criteria (Figure 2)2,10,12:
Played on 2 or more organized baseball teams per year
Played organized baseball more than 8 months per year
Pursued additional baseball-specific training (ie, formal hitting or pitching lessons or both)
Statistical Analysis
Incidence rates were calculated per 1000 AEs for all arm injuries. Rate ratios and 95% confidence intervals (CIs) were then determined to identify injury rates in pitchers and position players. Frequency counts were also conducted for each categorical variable. Chi-square analyses and Fisher exact tests were used to compare the frequency of all shoulder and elbow injuries by the following variable groups: sport-specialization status, position played, and participation in position-specific versus generalized physical training outside of team-sanctioned practices or games. Odds ratios with 95% CIs were then established for each group. Additional χ2 analyses were used to compare the frequency of specialized or nonspecialized youth athletes who correctly self-identified according to the research-based classification system used in this study. Statistical significance was set a priori at α = .05. All statistical analyses were performed using SPSS (version 22.0; IBM Corp, Armonk, NY).
RESULTS
Injury Incidence
Competitive youth baseball players (9–12 years old) sustained 21 arm injuries during 9453 AEs, for an injury incidence rate of 2.22/1000 AEs. All 21 arm injuries reported during the 6-month follow-up period occurred in athletes who were classified as specialized (100%). A higher number of injured athletes specialized in baseball compared with uninjured athletes (100% versus 80%, respectively; P = .03). Pitchers represented 66.7% (n = 106) of the cohort and demonstrated an arm-injury incidence rate of 2.10/1000 AEs, whereas position players represented 33.3% (n = 53) of the cohort and demonstrated an incidence of 2.51/1000 AEs. The difference in incidence rates was not significant between positions (rate ratio = 0.84, 95% CI = 0.34, 2.07; P = .70): 14 pitchers (13.2%) and 7 position players (13.2%) sustained arm injuries during the study. The proportion of arm injuries among youth baseball players was greatest at the shoulder (61.9%, n = 13), followed by the elbow (38.1%, n = 8). This pattern was consistent in pitchers (shoulder: 64.3%, n = 9; elbow: 35.7%, n = 5), whereas position players demonstrated a more similar injury distribution between the sites (shoulder: 57.1%, n = 4; elbow: 42.9%, n = 3). Despite these observations, the location of the arm injury was not different between pitchers and position players (P = .75). Of the 21 athletes who sustained injuries, only 1 reported a history of an arm overuse injury before the onset of symptoms. The majority of arm injuries reported were minor muscle strains of the shoulder and elbow. Most athletes returned to sport with participation modifications (ie, position change) and no time lost (n = 17). Athletes were considered to have missed time if they were unable to participate in their next practice or game after the initial complaint. Four athletes did sustain arm injuries that resulted in time away from sport. All 4 athletes required formal medical evaluation followed by a course of active rest and physical therapy. The diagnoses were proximal humeral epiphysitis (n = 2) and elbow apophysitis (n = 2). All athletes who sustained arm injuries in this study fully returned to sport without limitations in 8 weeks or less.
Sport-Specialization Status
At the start of the study, parents and players were asked to self-classify the participant as either a specialized or nonspecialized athlete based on their perceptions of sport specialization in youth baseball. Of the youth athletes, 31% (n = 49) self-classified as specialized in baseball, whereas the remaining 69% (n = 110) identified as nonspecialized athletes (Figure 3). The research team then reclassified each participant as specialized or nonspecialized, using research-based criteria from the literature.2,10,12 On the basis of these criteria, 83% of the cohort (n = 132) qualified as specialized athletes, whereas only 17% (n = 27) were classified as nonspecialized athletes (Figure 3). A significant number of youth baseball players were classified as nonspecialized athletes, yet they participated and competed as specialized athletes (57.9%, n = 92; P = .001). The research-based methods were used for athlete classification for the remainder of the statistical analyses. Youth baseball players who competed as specialized athletes demonstrated a higher frequency of shoulder or elbow injuries than their nonspecialized counterparts (odds ratio = 6.7; 95% CI = 0.4, 118; P = .03; Table).
Figure 3.
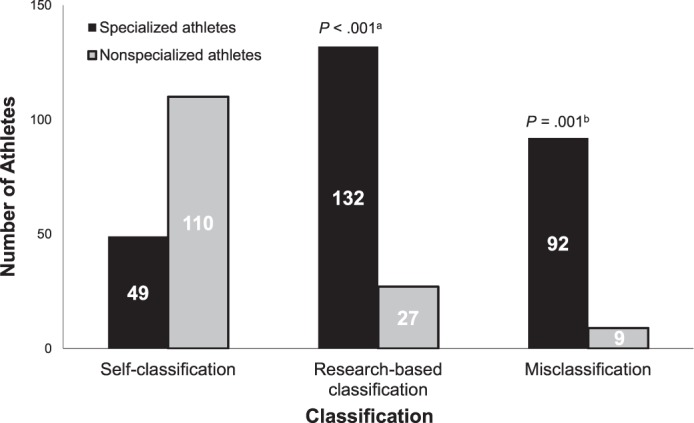
Youth sport specialization: parent and player perceptions versus reality. a The number of athletes who correctly self-classified as specialized (based on reporting ≥2/3 research-based criteria) was lower than in the correctly classified nonspecialized group. b The number of athletes who were misclassified was higher in the specialized group than in the nonspecialized group.
Position-Specialization Status
The majority of youth baseball players in this cohort participated in some type of additional sport-related training, either position specific (ie, hitting and pitching lessons) or generalized (ie, strength and conditioning lessons; 84.9%, n = 135). A total of 111 players took formal hitting lessons (69.8%), 72 took formal pitching lessons (67.9%), and 36 participated in generalized strength and conditioning lessons (22.6%; Table). Youth baseball players who participated in formal hitting lessons demonstrated no differences in injury frequency compared with players who did not (P = 1.00; Table). Players who participated in formal pitching lessons trended toward a higher frequency of shoulder and elbow injuries than those who did not; however, no statistical difference was found (P = .06; Table). Participation in generalized strength and conditioning programs did not affect injury frequency in youth baseball players when compared with athletes who participated solely in baseball-specific training (P = .60; Table).
DISCUSSION
To our knowledge, we are the first to examine the incidence of throwing-related arm injuries in a cohort of youth baseball players while taking position into account. Youth pitchers demonstrated no difference in the frequency of arm injuries when compared with position players. Players who specialized in baseball did sustain a statistically higher number of injuries when compared with players who did not specialize. We found it interesting that most athletes misclassified themselves, suggesting a disconnect between community perceptions and scientific understanding of youth sport specialization. Furthermore, based on current data trends, youth baseball players who also participated in additional position-specific training, particularly as pitchers, may be at a higher risk for sustaining a shoulder or elbow injury; however, more conclusive data are needed to definitively assess their level of risk.
Injury Incidence
During the 6-month study period, youth baseball players demonstrated an arm injury rate of 2.22/1000 AEs, similar to injury rates previously reported in a cohort of 246 high school players (2.50/1000 AEs) and a 16-year cohort study of collegiate players (1.81/1000 AEs).6,24 Differences in injury rates may be, in part, related to variations in how injury was defined in various studies. Previous researchers17–20 who examined injury profiles in youth baseball players relied on self-reported measures from survey data to establish risk factors associated with arm pain in this population. In addition, methodologic differences existed, including the definition of injury versus the existence of pain, the categorization of injury by time-loss status, and the grouping of athletes according to chronologic age versus competition status.6,16–18,24 Earlier investigations17–20 indicated that nearly 50% of youth athletes experienced shoulder or elbow pain during the course of a baseball season; however, a licensed medical professional did not physically confirm these reports, as was done in our study.
Unlike their high school, collegiate, and professional counterparts, most youth baseball players pitched in some capacity and also played field positions.5,6,24 Whereas pitchers sustained the majority of the injuries reported, injury proportions were equal between positions because pitchers also constituted the largest portion of the sample. Sharing of the physiological stresses of pitching among a greater number of players may help explain why no differences in injury frequency occurred between youth pitchers and position players (Table). This is in contrast to previous findings6,24,25 that high school, collegiate, and professional pitchers were at higher risk for sustaining an arm injury compared with position players.
Sport Specialization
Specialization in a single sport has been repeatedly identified4,10–14,26 as a risk factor for injury across multiple sports. Recent research23,26–29 also suggested that early sport specialization, defined as specializing in a sport before age 13, did not correlate with an athlete's long-term success in sport. Despite these results, youth athletes continue to specialize in baseball at alarming rates. Based on well-established criteria, 83% of the youth baseball players in this study were classified and competed as specialized athletes (Table), yet nearly 60% self-identified or were identified by parents as nonspecialized athletes (Figure 3).10,12 This discrepancy in parent and player perceptions of sport specialization suggests a large number of youth baseball players may be unknowingly at risk for developing a throwing-related arm injury (Figure 3). Athletes who specialized in baseball sustained a greater number of arm injuries than athletes who did not specialize (Table). These findings are consistent with earlier work outlining the risks of sport specialization; however, other factors, such as injury history, physical impairments, and workload, must also be taken into account.4,10,23,30 Additional studies are needed to better understand the relationship between sport specialization and the throwing-related injury risk in youth baseball populations.
One possible reason for the persistence of sport specialization among youth athletes, despite the acknowledged risks, is parents' and players' lack of understanding of its definition.30,31 Sport specialization has been defined in the literature as “intense training for more than 8 months per year in a single sport to the exclusion of other sports.”12(p252),13(p1) At the start of our study, parents and players were asked to classify the participant as either a specialized or nonspecialized athlete. Approximately 30% self-classified as specialized, whereas a higher percentage (83%) were classified as specialized using well-established research criteria (P < .001; Figure 3). These data suggest that a large number of parents and specialized athletes may be unaware of the increased risks these athletes are incurring on the basis of current participation patterns. When asked to expand on their views of sport specialization, parents stated that they encouraged their children to participate in multiple sports in addition to year-round baseball activities. These attitudes seem to contribute to overscheduling, with little time allocated for rest and recovery, and may prove detrimental to an athlete's health and long-term success in sport.13
Position Specialization
The majority of youth players sought out formal pitching lessons (67.9%) in an effort to improve athletic performance. Position-specific training as a pitcher before age 13, in addition to pitching in practices and games, resulted in increased physical loads being placed across immature bony structures at the shoulder and elbow joints.32–34 Also, per USA Baseball's Long-Term Athlete Development Plan position-specific training may not be as beneficial as generalized physical training for youth athletes at this stage of physical development.11–14 Despite age-specific recommendations that emphasize the importance of physical literacy and functional skill acquisition, remarkably few youth baseball players in this cohort (22.6%) took generalized strength and conditioning lessons. Future authors should examine the effects of participation in generalized physical training programs compared with position-specific training programs on injury risk and performance in a larger cohort of youth athletes.
Strengths
To our knowledge, this is the first study to examine the arm-injury incidence in youth baseball players. This research is novel with respect to both the study population and its prospective design. Fewer than 10% of all injury-prevention data have been collected on athletes younger than 18 years of age, with even fewer data describing youth athletes (9–12 years old).35 Despite the fact that youth and adolescent athletes comprise the majority of the population competing in sports, they continue to be significantly understudied.36 Our prospective design allowed us to establish the arm-injury incidence in a cohort of youth baseball players, though larger prospective studies are certainly warranted. In addition, the study was strengthened because all reported injuries were confirmed via physical assessment as opposed to being potentially unconfirmed self-reports. Our findings provide initial insight into the injury profiles and participation levels of an understudied population of youth baseball players as compared with their well-studied collegiate and professional counterparts.
Limitations
Certain limitations should be noted while interpreting the results of this research. The relatively low incidence of throwing-related arm injuries as well as the small sample size likely affected the strength of our results and our ability to detect differences in injury frequency and risk between groups of youth baseball players. The limited number of injuries may have also been affected by the abbreviated length of the follow-up period, given that many players in this study reported playing baseball more than 8 months per year, which was at least 2 months longer than the 6 months during which they were tracked. Future studies with larger sample sizes and longer follow-up periods are needed to further examine injury risks in this population. Additional limitations of this study include the disparities in the numbers of youth pitchers versus position players and specialized versus nonspecialized athletes. Although the groups were uneven for statistical analysis, the proportions for each position and participation level were representative of the population being studied. Last, previous authors5,6,24,25,37 who examined injury rates and sports performance among high school, collegiate, and professional athletes were often able to provide greater levels of detail with regard to training volume (ie, number of innings played per game, number of pitches thrown per game). Whereas these data are helpful and provide insight into the relationships among training volume, fatigue, and injury, they are challenging to consistently and reliably obtain at the youth level. No single organization oversees all the different factions of youth baseball or youth sports. The practice-, game-, and training-related data collected in this study relied on parental and coach reports and participation, ultimately limiting the amount of training detail we could realistically obtain at the youth level without a significant increase in resources.
CONCLUSIONS
The arm-injury incidence rate of youth baseball players was similar to rates reported for adolescent baseball players. Athletes who specialized in baseball before age 13 demonstrated a higher frequency of arm injuries than those who did not specialize. It is concerning that 57.9% of specialized players and their parents were unaware of their specialization status. These findings emphasize the need for continued education of parents and athletes regarding sport specialization, as well as future studies to better understand the factors driving the specialization phenomenon.
REFERENCES
- 1.American Academy of Pediatrics Council on Sports Medicine and Fitness. Policy statement: baseball and softball. Pediatrics. 2012;129(3):842–856. doi: 10.1542/peds.2011-3593. [DOI] [PubMed] [Google Scholar]
- 2.Bell DR, Post EG, Trigsted SM, Hetzel S, McGuine TA, Brooks MA. Prevalence of sport specialization in high school athletics: a 1-year observational study. Am J Sports Med. 2016;44(6):1469–1474. doi: 10.1177/0363546516629943. [DOI] [PubMed] [Google Scholar]
- 3.Hidden demographics of youth sports: “Hey, data data—swing!”. ESPN Web site. 2013 http://www.espn.com/espn/story/_/id/9469252/hidden-demographics-youth-sports-espn-magazine. Published. Accessed September 1, 2017.
- 4.McGuine TA, Post EG, Hetzel SJ, Brooks MA, Trigsted S, Bell DR. A prospective study on the effect of sport specialization on lower extremity injury rates in high school athletes. Am J Sports Med. 2017;45(12):2706–2712. doi: 10.1177/0363546517710213. [DOI] [PubMed] [Google Scholar]
- 5.Collins CL, Comstock RD. Epidemiological features of high school baseball injuries in the United States, 2005–2007. Pediatrics. 2008;121(6):1181–1187. doi: 10.1542/peds.2007-2572. [DOI] [PubMed] [Google Scholar]
- 6.Shanley E, Rauh MJ, Michener LA, Ellenbecker TS. Incidence of injuries in high school softball and baseball players. J Athl Train. 2011;46(6):648–654. doi: 10.4085/1062-6050-46.6.648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dompier TP, Powell JW, Barron MJ, Moore MT. Time-loss and non–time-loss injuries in youth football players. J Athl Train. 2007;42(3):395–402. [PMC free article] [PubMed] [Google Scholar]
- 8.Kerr ZY, Lynall RC, Roos KG, Dalton SL, Djoko A, Dompier TP. Descriptive epidemiology of non–time-loss injuries in collegiate and high school student-athletes. J Athl Train. 2017;52(5):446–456. doi: 10.4085/1062-6050-52.2.15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nabhan D, Walden T, Street J, Linden H, Moreau B. Sports injury and illness epidemiology during the 2014 Youth Olympic Games: United States Olympic Team surveillance. Br J Sports Med. 2016;50(11):688–693. doi: 10.1136/bjsports-2015-095835. [DOI] [PubMed] [Google Scholar]
- 10.Jayanthi NA, LaBella CR, Fischer D, Pasulka J, Dugas LR. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med. 2015;43(4):794–801. doi: 10.1177/0363546514567298. [DOI] [PubMed] [Google Scholar]
- 11.Myer GD, Jayanthi N, Difiori JP, et al. Sport specialization, part I: does early sports specialization increase negative outcomes and reduce the opportunity for success in young athletes? Sports Health. 2015;7(5):437–442. doi: 10.1177/1941738115598747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jayanthi N, Pinkham C, Dugas L, Patrick B, LaBella C. Sports specialization in young athletes: evidence-based recommendations. Sports Health. 2013;5(3):251–257. doi: 10.1177/1941738112464626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.LaPrade RF, Agel J, Baker J, et al. AOSSM early sport specialization consensus statement. Orthop J Sports Med. 2016;4(4):2325967116644241. doi: 10.1177/2325967116644241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Myer GD, Jayanthi N, DiFiori JP, et al. Sports specialization, part II: alternative solutions to early sport specialization in youth athletes. Sports Health. 2016;8(1):65–73. doi: 10.1177/1941738115614811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bohne C, George SZ, Zeppieri G., Jr Knowledge of injury prevention and prevalence of risk factors for throwing injuries in a sample of youth baseball players. Int J Sports Phys Ther. 2015;10(4):464–475. [PMC free article] [PubMed] [Google Scholar]
- 16.Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39(2):253–257. doi: 10.1177/0363546510384224. [DOI] [PubMed] [Google Scholar]
- 17.Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30(4):463–468. doi: 10.1177/03635465020300040201. [DOI] [PubMed] [Google Scholar]
- 18.Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33(11):1803–1810. doi: 10.1097/00005768-200111000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Olsen SJ, 2nd, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34(6):905–912. doi: 10.1177/0363546505284188. [DOI] [PubMed] [Google Scholar]
- 20.Yang J, Mann BJ, Guettler JH, et al. Risk-prone pitching activities and injuries in youth baseball: findings from a national sample. Am J Sports Med. 2014;42(6):1456–1463. doi: 10.1177/0363546514524699. [DOI] [PubMed] [Google Scholar]
- 21.Little League regulations, rules and policies. Little League Baseball Web site. 2019 https://www.littleleague.org/playing-rules/rules-regulations-policies Accessed July 11.
- 22.Youth baseball pitching injuries. USA Baseball Web site. 2008 https://www.usabaseball.com/news/youth-baseball-pitching-injuries/c-246193056?tid=216639934. Published. Accessed April 2, 2016.
- 23.Myers JB, DeFreese JD, DiStefano L, et al. USA Baseball long-term athlete development model. USA Baseball Web site. 2017 http://usabltad.com. Published. Accessed September 25, 2017.
- 24.Dick R, Sauers EL, Agel J, et al. Descriptive epidemiology of collegiate men's baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):183–193. [PMC free article] [PubMed] [Google Scholar]
- 25.Posner M, Cameron KL, Wolf JM, Belmont PJ, Jr, Owens BD. Epidemiology of Major League Baseball injuries. Am J Sports Med. 2011;39(8):1676–1680. doi: 10.1177/0363546511411700. [DOI] [PubMed] [Google Scholar]
- 26.DiFiori JP, Benjamin HJ, Brenner JS, et al. Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Br J Sports Med. 2014;48(4):287–288. doi: 10.1136/bjsports-2013-093299. [DOI] [PubMed] [Google Scholar]
- 27.Lloyd RS, Oliver JL, Faigenbaum AD, et al. Long-term athletic development, part 1: a pathway for all youth. J Strength Cond Res. 2015;29(5):1439–1450. doi: 10.1519/JSC.0000000000000756. [DOI] [PubMed] [Google Scholar]
- 28.Lloyd RS, Oliver JL, Faigenbaum AD, et al. Long-term athletic development, part 2: barriers to success and potential solutions. J Strength Cond Res. 2015;29(5):1451–1464. doi: 10.1519/01.JSC.0000465424.75389.56. [DOI] [PubMed] [Google Scholar]
- 29.Solomon J. 7 charts that show why we need to fix youth sports. Aspen Institute Web site. 2017 https://www.aspeninstitute.org/blog-posts/7-charts-show-fix-youth-sports. Published. Accessed March 21, 2018.
- 30.Bell DR, Post EG, Biese K, Bay C. Valovich McLeod T. Sport specialization and risk of overuse injuries: a systematic review with meta-analysis. Pediatrics. 2018;142(3):e20180657. doi: 10.1542/peds.2018-0657. [DOI] [PubMed] [Google Scholar]
- 31.Bell DR, Post EG, Trigsted SM, Schaefer DA, McGuine TA, Brooks MA. Parents' awareness and perceptions of sport specialization and injury prevention recommendations. Clin J Sport Med. doi: 10.1097/JSM.0000000000000648. [epub ahead of print. [DOI] [PubMed]
- 32.Davis JT, Limpisvasti O, Fluhme D, et al. The effect of pitching biomechanics on the upper extremity in youth and adolescent baseball pitchers. Am J Sports Med. 2009;37(8):1484–1491. doi: 10.1177/0363546509340226. [DOI] [PubMed] [Google Scholar]
- 33.Sabick MB, Kim YK, Torry MR, Keirns MA, Hawkins RJ. Biomechanics of the shoulder in youth baseball pitchers: implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med. 2005;33(11):1716–1722. doi: 10.1177/0363546505275347. [DOI] [PubMed] [Google Scholar]
- 34.Sabick MB, Torry MR, Lawton RL, Hawkins RJ. Valgus torque in youth baseball pitchers: a biomechanical study. J Shoulder Elbow Surg. 2004;13(3):349–355. doi: 10.1016/j.jse.2004.01.013. [DOI] [PubMed] [Google Scholar]
- 35.McBain K, Shrier I, Shultz R, et al. Prevention of sports injury I: a systematic review of applied biomechanics and physiology outcomes research. Br J Sports Med. 2012;46(3):169–173. doi: 10.1136/bjsm.2010.080929. [DOI] [PubMed] [Google Scholar]
- 36.Lawson BR, Comstock RD, Smith GA. Baseball-related injuries to children treated in hospital emergency departments in the United States, 1994–2006. Pediatrics. 2009;123(6):e1028–e1034. doi: 10.1542/peds.2007-3796. [DOI] [PubMed] [Google Scholar]
- 37.Krajnik S, Fogarty KJ, Yard EE, Comstock RD. Shoulder injuries in US high school baseball and softball athletes, 2005–2008. Pediatrics. 2010;125(3):497–501. doi: 10.1542/peds.2009-0961. [DOI] [PubMed] [Google Scholar]