

Abstract
Background and study aims Among vasculitides, IgA vasculitis (IgAV) and eosinophilic granulomatosis with polyangiitis (EGPA) frequently damage the gastrointestinal tract. However, only a few studies have investigated the entire gastrointestinal tract in patients with IgAV or EGPA by endoscopy. The aim of this study was to clarify endoscopic characteristics of patients with IgAV and those with EGPA.
Patients and methods Clinicopathological and endoscopic findings were retrospectively compared between 33 patients with IgAV and 19 patients with EGPA.
Results Gastrointestinal involvement was observed in 33 patients with IgAV (100 %) and in 8 patients with EPGA (42 %; P = 0.0001). Duodenal involvement was more frequent in patients with IgAV (75.8 %) than in those with EGPA (21.1 %, P = 0.0002). Jejunoileal involvement was frequent in both groups (IgAV 94.4 %; EGPA 77.8 %). Gastric mucosal erythema was more frequent in patients with IgAV (18.2 %) than in those with EGPA (0 %, P = 0.0481). Duodenal mucosal erythema (IgAV 54.6 %; EGPA 21.1 %, P = 0.0227), ulcer (IgAV 33.3 %; EGPA 0 %, P = 0.0041), and hematoma-like protrusion (IgAV 21.1 %; EGPA 0 %, P = 0.039) were more frequently observed in patients with IgAV than in those with EGPA.
Conclusions Frequent duodenal involvement, gastric mucosal erythema, and duodenal lesions including erythema, ulcer, and hematoma-like protrusion are characteristic of patients with IgAV. Because jejunoileal involvement was frequent in both groups of patients, small-bowel endoscopies should be performed for diagnosis of small-bowel lesions in patients with IgAV and EGPA.
Introduction
Vasculitis is inflammation of blood vessel walls and its extent and clinical course depend on the size and location of the affected vessels 1 . Vasculitides can be classified into large-, medium- and small-sized vessel vasculitis according to the Chapel Hill Consensus Conference on the Nomenclature of Vasculitidies 2 . Vasculitis affects various organs including kidneys, skin, joints, lungs, and the gastrointestinal tract. Among these organs injury, gastrointestinal involvement can manifest as severe problems such as inflammation, ischemia, hemorrhage, obstruction, or perforation 3 .
Among vasculitides, IgA vasculitis (IgAV) and eosinophilic granulomatosis with polyangiitis (EGPA) frequently damage the gastrointestinal tract 4 5 6 . Endoscopic characteristics of IgAV or EGPA have been described in the literature 7 8 9 10 . To date, however, only a few studies have investigated the entire gastrointestinal tract in patients with IgAV or EGPA by endoscopy. Furthermore, no previous studies have compared endoscopic findings between patients with IgAV and EGPA.
We conducted a retrospective analysis to compare clinical, endoscopic and pathological characteristics between patients with IgAV and those with EGPA whose entire gastrointestinal tract was examined endoscopically.
Patients and methods
Study population
The current investigation was based on retrospective data collection. We reviewed medical records at Iwate Medical University, Kyushu University, and Matsuyama Red Cross Hospital from 2008 to 2017 and identified all patients with a diagnosis of
IgAV or EGPA. Among those patients, we excluded patients in whom gastrointestinal endoscopy was not performed. The study protocol was approved by the Institutional Review Board at Iwate Medical University, Kyushu University, and Matsuyama Red Cross Hospital. The study was conducted in accordance with the Helsinki Declaration (6th revision, 2008).
Data collection
Demographics of study subjects were extracted via chart review. Evaluated characteristics included age, sex, allergic diseases (bronchial asthma or allergic rhinitis), laboratory data, organopathy, endoscopic findings, histologic findings, and treatment. Laboratory assessments included white blood cell (WBC), eosinophil, hemoglobin, platelet, serum creatinine and C-reactive protein (CRP), and urinalysis to screen for hematuria and proteinuria before initial treatment. Organopathy included skin involvement (purpura or urticaria), lung involvement (lung infiltrate, nodules or pleural effusion on chest radiograph or computed tomography), neurologic involvement, muscle involvement, and gastrointestinal involvement (abdominal pain, hematemesis, melena, hematochezia, nausea/vomiting, diarrhea and constipation).
The upper gastrointestinal tract was examined by esophagogastroduodenoscopy (EGD). The jejunum and/or ileum was examined by capsule endoscopy (CE) or balloon-assisted endoscopy (BAE). The colorectum was examined by colonoscopy. Endoscopic examination was performed when patients manifested clinical symptoms suggestive of gastrointestinal involvement, such as abdominal pain, hematemesis, melena, hematochezia, nausea, vomiting, diarrhea and constipation, or when they manifested signs of gastrointestinal bleeding including hematemesis, melena, hematochezia, and anemia (a hemoglobin level < 10 g/dL). We also performed endoscopy for asymptomatic patients in consideration of evaluation of subclinical gastrointestinal involvement or when they had an indication for use of steroids. Endoscopic examinations were performed within 14 days after onset of IgAV or EGPA. Endoscopic findings included mucosal erythema, erosion, ulcer, and/or hematoma-like protrusion.
Characteristic histological findings of IgAV were defined as small vessel vasculitis with polymorphonuclear leucocyte infiltration (leukocytoclastic vasculitis), while those of EGPA were defined as small and medium-sized vessel vasculitis, eosinophilic infiltrates, and/or extravascular granulomas 4 11 . As for treatment, steroid, cyclophosphamide, and/or intravenous immunoglobulin (IVIG) were used. We treated patients with intravenous or oral proton pump inhibitor (PPI) when they had upper gastrointestinal lesions or they were treated with a steroid.
IgAV and EGPA diagnosis
Diagnosis of IgAV and EGPA was based on American College of Rheumatology 1990 criteria 4 12 13 . We defined IgAV if patients had two or more of the following four criteria: age 20 or less at disease onset; palpable purpura; acute abdominal pain; and biopsy showing granulocytes in the walls of small arterioles or venules. Also, we defined EGPA if patients have four or more of the following six criteria: asthma; eosinophilia greater than 10 % on differential WBC count; mononeuropathy (including multiplex) or polyneuropathy; non-fixed pulmonary infiltrates on roentgenography; paranasal sinus abnormality; and biopsy containing a blood vessel with extravascular eosinophils.
Statistical analysis
Parametric data are expressed as mean ± SD. Nonparametric data are expressed as numbers and percentages. Comparisons between any two groups were performed by the Mann-Whitney test or chi-squared test where appropriate. P < 0.05 was considered to be significant. All statistical computations were performed with JMP version 13 (Statistical Discovery Program, Cary, North Carolina, United States).
Results
Clinical features and laboratory data on IgAV and EGPA
Fifty-two patients who had a diagnosis of IgAV or EGPA (33 IgAV; 19 EGPA). Table 1 compares clinical and laboratory characteristics between the two groups. There was no significant difference between them groups in terms of age, gender, hemoglobin level, platelet count, creatinine level, CRP, or treatment by steroid.
Table 1. Clinical and laboratory characteristics between patients with IgAV and those with EGPA (%).
| IgAV patients (n = 33) | EGPA patients (n = 19) | P value | |
| Age | 46.4 ± 24.7 | 56.4 ± 15.3 | 0.2061 |
| Gender | 0.5737 | ||
|
16 (48.5) | 11 (57.9) | |
|
17 (51.5) | 8 (42.1) | |
| Allergic diseases | |||
|
2 (6.1) | 19 (100) | 0.0001 |
|
0 (0) | 4 (21.1) | 0.0143 |
| Laboratory data | |||
|
11505 ± 5295 | 24076 ± 5904 | 0.0001 |
|
178 ± 165 | 13824 ± 6792 | 0.0001 |
|
13.5 ± 2.0 | 13.1 ± 1.7 | 0.3467 |
|
268212 ± 95444 | 297000 ± 93761 | 0.3184 |
|
1.0 ± 0.9 | 1.0 ± 1.1 | 0.7466 |
|
4.5 ± 6.8 | 5.6 ± 5.4 | 0.1898 |
|
28 (84.8) | 3 (15.8) | 0.0001 |
|
27 (81.8) | 7 (36.8) | 0.0042 |
| Site of involvement | |||
|
33 (100) | 10 (52.6) | 0.0001 |
|
0 (0) | 13 (68.4) | 0.0001 |
|
0 (0) | 16 (84.2) | 0.0001 |
|
0 (0) | 6 (31.6) | 0.0013 |
|
33 (100) | 8 (42.1) | 0.0001 |
| Treatment | |||
|
32 (97) | 19 (100) | 1 |
|
0 (0) | 3 (15.8) | 0.0438 |
|
0 (0) | 11 (57.9) | 0.0001 |
|
32 (97) | 19 (100) | 1 |
Continuous values are indicated as mean ± SD (standard deviation). IgAV; IgA vasculitis, EGPA; eosinophilic granulomatosis with polyangiitis, WBC; white blood cell, CRP; C-reactive protein, IVIG; intravenous immunoglobulin, PPI; proton pump inhibitor.
Patients with EGPA more frequently had bronchial asthma (100 %) and allergic rhinitis (21.1 %) than patients with IgAV (6.1 % and 0 %, respectively). WBC and eosinophil counts in the peripheral blood at disease onset were significantly higher in patients with EGPA (24,076 ± 5,904/μL and 13,824 ± 6,792/μL) than in those with IgAV (11,505 ± 5295/μL and 178 ± 165/μL, respectively). Conversely, rates of microhematuria and proteinuria were higher in patients with IgAV (84.8 % and 81.8 %) than in those with EGPA (15.8 % and 36.8 %, respectively).
Regarding symptoms of organopathy, the rate of skin involvement and gastrointestinal involvement were higher in patients with IgAV (100 % and 100 %, respectively) than in those with EGPA (52.6 % and 42.1 %, respectively), whereas rates of involvement of lung, nerve, and muscle were higher in patients with EGPA (68.4 %, 84.2 % and 31.6 %, respectively) than in those with IgAV (all none).
As for treatments, 51 of 52 patients (98 %) were treated with steroids and PPI ( Table 1 ). Cyclophosphamide and IVIG were administered to several patients with EGPA and none of those with IgAV.
Frequency of endoscopic abnormalities
EGD was performed in all 52 patients. CE or BAE was performed in 27 patients (IgAV 18; EGPA 9). Colonoscopy was performed in 44 patients (IgAV 26; EGPA 18). Fig. 1 shows frequency of lesions detected by endoscopy. Patients with IgAV had duodenal lesions more frequently than those with EGPA (75.8 % vs. 21.1 %; P = 0.0002). No significant difference was observed between patients with IgAV and those with EGPA regarding frequency of lesions in the esophagus, stomach, jejunum/ileum or colorectum.
Fig. 1 .
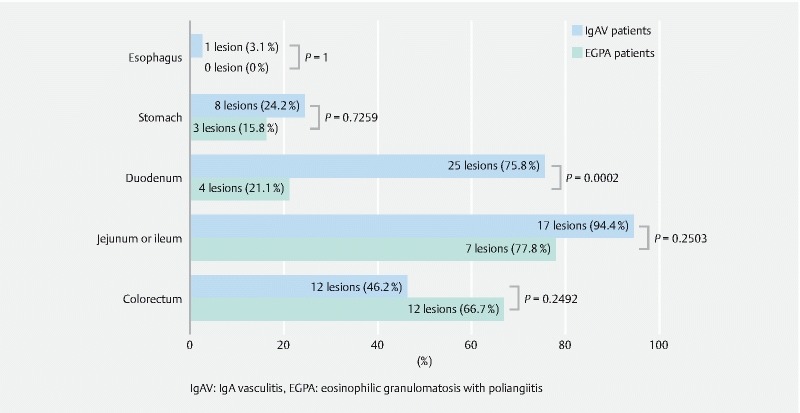
Frequency of lesions see on endoscopy. Esophagus, stomach, and duodenum were observed in 33 IgAV patients and 19 EGPA patients, the jejunum or ileum was observed in 18 IgAV patients and 9 EGPA patients, and the colorectum was observed for 26 IgAV patients and 18 EGPA patients. IgAV patients had more lesions in the duodenum than did EGPA patients (75.8 % of IgAV; 21.1 % of EGPA; P = 0.0002).
EGD findings
EGD findings in patients with IgAV and EGPA are shown in Table 2 and Fig. 2 . In the esophagus, ulcer was observed only in one patient with IgAV, and other findings were not seen in both groups. In the stomach, mucosal erythema was seen in six of 33 patients (18.2 %) with IgAV and none of 19 patients with EGPA ( P = 0.0481). Incidence of other gastric lesions and location of each lesion in the stomach did not differ between the two groups (upper/middle/lower, 7/4/2 in IgAV and 3/0/0 in EGPA).
Table 2. Endoscopic findings in patients with IgAV and EGPA (%).
| IgAV patients | EGPA patients | P value | |
| EGD findings | n = 33 | n = 19 | |
| Esophagus | |||
|
0 (0) | 0 (0) | 0 |
|
0 (0) | 0 (0) | 0 |
|
1 (3.0) | 0 (0) | 1 |
|
0 (0) | 0 (0) | 0 |
| Stomach | |||
|
6 (18.2) | 0 (0) | 0.0481 |
|
5 (15.2) | 2 (10.5) | 1 |
|
2 (6.1) | 1 (5.3) | 1 |
|
1 (3.0) | 0 (0) | 1 |
| Duodenum | |||
|
18 (54.6) | 4 (21.1) | 0.0227 |
|
2 (6.1) | 4 (21.1) | 0.1751 |
|
11 (33.3) | 0 (0) | 0.0041 |
|
7 (21.1) | 0 (0) | 0.039 |
| CE or BAE findings | n = 18 | n = 9 | |
|
13 (72.2) | 3 (33.3) | 0.0969 |
|
10 (55.6) | 4 (44.4) | 0.6946 |
|
10 (55.6) | 5 (55.6) | 1 |
|
3 (16.7) | 0 (0) | 0.5292 |
| Colonoscopic findings | n = 26 | n = 18 | |
|
10 (38.5) | 9 (50) | 0.5419 |
|
8 (30.8) | 9 (50) | 0.225 |
|
6 (23.1) | 3 (16.7) | 0.7161 |
|
4 (15.4) | 0 (0) | 0.1327 |
IgAV; IgA vasculitis, EGPA; eosinophilic granulomatosis with polyangiitis, EGD; esophagogastroduodenoscopy, CE; capsule endoscopy, BAE; balloon-assisted endoscopy
Fig. 2 .
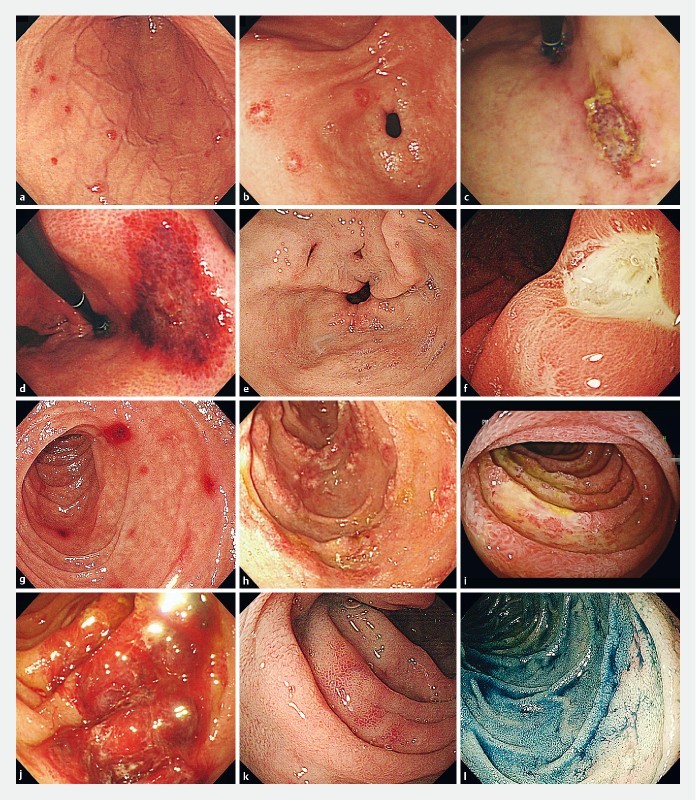
Esophagogastroduodenoscopic findings in patients with IgA vasculitis ( a, b, c ,d, g, h, i, j ) and those with eosinophilic granulomatosis with polyangiitis ( e, f, k, l ). a Mucosal erythemas in the middle third of the stomach. b Erosions in the lower third of the stomach. c Ulcer in the middle third of the stomach. d Hematoma-like protrusion in the middle third of the stomach. e Erosions in the lower third of the stomach. f Ulcer in the middle third of the stomach. g, k Mucosal erythemas in the duodenum. h, l Erosions in the duodenum. i Ulcers in the duodenum. j Hematoma-like protrusion in the duodenum.
In the duodenum, mucosal erythema (IgAV 54.6 %; EGPA 21.1 %, P = 0.0227), ulcer (IgAV 33.3 %; EGPA 0 %, P = 0.0041), and hematoma-like protrusion (IgAV 21.1 %; EGPA 0 %, P = 0.039) were observed more frequently in patients with IgAV than in those with EGPA. Incidence of erosion was no different between the two groups. Lesions were more frequently located on the second portion of the duodenum in patients with IgAV (bulb/2nd portion, 12/22) than in those with EGPA (bulb/2nd portion, 3/4; P = 0.0034). All patients with IgAV or EGPA who had EGD findings had multiple lesions.
CE or BAE findings
CE and/or BAE findings in patients with IgAV and EGPA are shown in Table 2 and Fig. 3 . Incidence of mucosal erythema, erosion, ulcer or hematoma-like protrusion did not differ between two groups. All patients with IgAV or EGPA who had CE or BAE findings had multiple lesions. Lesion location was no different between the two groups (jejunum/ileum, 17/15 in IgAV; 7/7 in EGPA).
Fig. 3 a, b, c, d.

Capsule or balloon-assisted endoscopic in patients with IgA vasculitis and e, f, g those with eosinophilic granulomatosis with polyangiitis. a Mucosal erythemas in the ileum. b Erosions in the ileum. c Ulcers in the jejunum. d Hematoma-like protrusion in the jejunum. e Mucosal erythema in the jejunum. f Erosions in the ileum. g Ulcer in the jejunum.
Colonoscopic findings
Colonoscopic findings in patients with IgAV and EGPA are shown in Table 2 and Fig. 4 . Incidence of mucosal erythema, erosion, ulcer or hematoma-like protrusion did not differ between the two groups. Lesion location was no different between the two groups (cecum to transverse colon/descending colon to rectum, 10/10 in IgAV; 4/12 in EGPA).
Fig. 4 a, b, c, d.
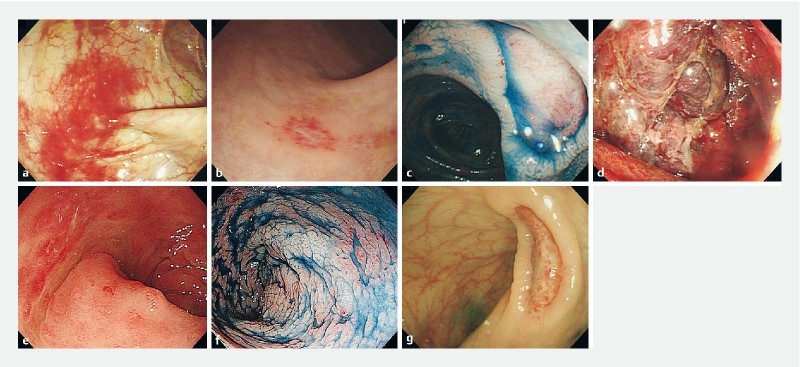
Colonoscopic findings in patients with IgA vasculitis and e, f, g those with eosinophilic granulomatosis with polyangiitis. a Mucosal erythemas in the descending colon. b Erosion in the rectum. c Ulcer in the ascending colon. d Hematoma-like protrusion in ascending colon. e Mucosal erythemas in the rectum. f Erosions in the rectum. g Ulcer in the rectum.
Endoscopic findings in patients with gastrointestinal bleeding
Symptoms and endoscopic findings in patients with gastrointestinal bleeding are shown in Table 3 . There were nine patients with IgAV and two patients with EGPA who manifested gastrointestinal bleeding. Seven patients had hematochezia, two patients had melena and anemia, and one patient had hematemesis. Under EGD, one patient had esophageal lesions, three patients had gastric lesions, and six patients had duodenal lesions. CE or BAE was performed in seven patients, all of whom had small bowel lesions. Of nine patients examined by colonoscopy, four patients had colorectal lesions. However, none of those 11 patients with gastrointestinal bleeding were treated with endoscopic hemostasis.
Table 3. Endoscopic findings in patients with gastrointestinal bleeding.
| Cases | Age/sex | Clinical diagnosis | Signs of gastrointestinal bleeding | EGD findings | CE or BAE findings | Colonoscopic findings | Endoscopic hemostasis |
| 1 | 83/M | IgAV | Hematemesis | Mucosal erythemas and hematoma-like protrusions (D) | Ulcers | Normal | NP |
| 2 | 64/F | IgAV | Hematochezia | Normal | Mucosal erythemas and erosions | Normal | NP |
| 3 | 25/M | IgAV | Hematochezia | Mucosal erythemas (D) | Mucosal erythemas, erosions and hematoma-like protrusions | Mucosal erythemas and erosions | NP |
| 4 | 20/M | IgAV | Hematochezia | Mucosal erythemas (D) | NE | Mucosal erythemas, erosions and hematoma-like protrusions | NP |
| 5 | 78/M | IgAV | Melena, anemia | Ulcers (E, S, D), and hematoma-like protrusions (D) | NE | NE | NP |
| 6 | 55/M | IgAV | Melena | Mucosal erythemas and ulcers (S, D) | Ulcers | Normal | NP |
| 7 | 73/F | IgAV | Anemia | Normal | NE | NE | NP |
| 8 | 53/M | IgAV | Hematochezia | Normal | Mucosal erythemas, erosions and ulcers | Normal | NP |
| 9 | 68/F | IgAV | Hematochezia | Ulcers and hematoma-like protrusions (D) | Mucosal erythemas, ulcers and hematoma-like protrusions | Normal | NP |
| 10 | 61/M | EGPA | Hematochezia | Normal | Ulcers | Mucosal erythemas and ulcers | NP |
| 11 | 27/M | EGPA | Hematochezia | Ulcers (S) | NE | Mucosal erythemas | NP |
M; male, F; female, IgAV; IgA vasculitis, EGPA; eosinophilic granulomatosis with polyangiitis, EGD; esophagogastroduodenoscopy, D; duodenum, E; esophagus, S; stomach, CE; capsule endoscopy, BAE; balloon-assisted endoscopy, NE; not examined, NP; not performed.
Response to therapy in gastrointestinal involvement of IgAV and EGPA
Follow-up endoscopy was performed in a certain proportion of patients with IgAV or EGPA after treatment. Follow-up endoscopy included EGD in 17 patients (15 patients with IgAV and two patients with EGPA), CE or BAE in seven patients (four patients with IgAV and three patients with EGPA), colonoscopy in 12 patients (seven patients with IgAV and five patients with EGPA). Follow-up examinations revealed that the preceding lesions had healed or completely disappeared. All patients were treated with a steroid and PPI. Two patients with EGPA and one patient with EGPA were treated with IVIG and cyclophosphamide, respectively.
Characteristic histologic findings in IgAV and EGPA
Characteristic histologic findings – leukocytoclastic vasculitis, eosinophilic infiltration, small-seized vessel vasculitis, and extravascular granuloma – in IgAV and EGPA are shown in Fig. 5 . Biopsy specimens were taken from the skin, esophagus, stomach, duodenum, jejunum/ileum and colorectum in 41 (IgAV 31; EGPA 10), 11 (IgAV 3; EGPA 8), 36 (IgAV 23; EGPA 13), 50 (IgAV 35; EGPA 15), 31 (IgAV 21; EGPA 10), and 35 (IgAV 18; EGPA 17) patients, respectively. The rate of detection of the above characteristic histologic findings in all regions did not differ between the two groups (IgAV, skin 83.9 %, esophagus 0%, stomach 4.4 %, duodenum 17.1 %, jejunum/ileum 14.3 %, colorectum 11.1 %; EGPA, skin 80 %, esophagus 12.5 %, stomach 23.1 %, duodenum 26.7 %, jejunum/ileum 30 %, colorectum 29.4 %).
Fig. 5.
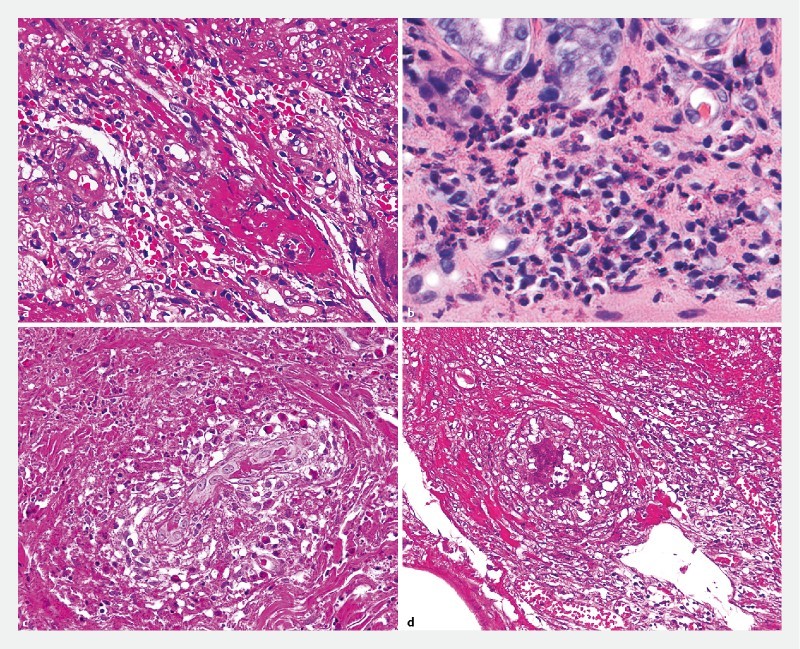
Characteristic histologic findings in a IgA vasculitis and b, c, d eosinophilic granulomatosis with polyangiitis. a Leukocytoclastic vasculitis. b Eosinophilic infiltration. c Small-sized vessel vasculitis. d Extravascular granuloma.
Discussion
In the current study, we found more frequent gastric mucosal erythema, duodenal lesions including erythema, ulcer and hematoma-like protrusion in patients with IgAV than in those with EGPA. We also revealed that incidence of jejunoileal involvement was high in both patients with IgAV and those with EGPA.
IgAV, previously referred to as Henoch-Schönlein purpura, is a systemic small-vessel vasculitis that develops via an allergic mechanism and is characterized by purpura associated with leukocytoclastic vasculitis 2 . Gastrointestinal symptoms occur in up to 85 % of patients with IgAV 14 . Therefore, endoscopy has been used to detect the gastrointestinal involvement in IgAV. Nishiyama et al. 8 reported that gastrointestinal involvement under EGD and colonoscopy was observed in seven of 10 cases (70 %) in the stomach and in the duodenum, five cases (50 %) in the terminal ileum, and six cases (60 %) in the colon. In a report of seven cases by Esaki et al. 9 , involvement with IgAV was found in two cases (28.6 %) in the stomach, six cases (85.7%) in the duodenum, six cases (85.7 %) in the ileum, and four cases (57.1 %) in the colon.
On the other hand, EGPA, formerly known as Churg-Strauss syndrome, is a multisystem disorder characterized by allergic granulomatosis and necrotizing vasculitis developing after the appearance of peripheral and tissue eosinophilia 2 6 . The gastrointestinal tract is involved in approximately 20 % to 50 % of patients with EGPA. Pagnoux C et al. 15 reported that incidence of gastrointestinal involvement using EGD and colonoscopy was 17 of 62 cases (27 %) using EGD and six of 62 cases (10 %) using colonoscopy. In those studies, however, the entire gastrointestinal tract was not examined by endoscopy. To our knowledge, no previous studies have examined entire gastrointestinal tracts in patients with IgAV or EGPA using EGD, CE, BAE and colonoscopy.
Our results showed that incidence of esophago-gastric involvement was low, that of colorectal involvement was intermediate, and that of jejunoileal involvement was high in patients with both diseases. In addition, incidence of duodenal involvement was higher in patients with IgAV than in those with EGPA. The previously reported incidence of esophago-gastric and colorectal involvement was unstable, because the number of cases in the previous studies is small. However, our results suggested that IgAV seems to involve predominantly the small bowel including the duodenum.
Endoscopic findings of IgAV were first reported in 1973 16 . Akadamar et al. 16 showed that the main endoscopic findings of IgAV in the stomach and duodenum were mucosal congestion, redness, petechial, multiple ulcers, nodular change and hematoma-like protrusion. In another study, it thus seems likely that multiple irregular ulcers in the second portion are characteristic of duodenal involvement in IgAV 9 . As for colonoscopic findings in patients with IgAV, only a few case series or reports are available. Zhang et al. 7 showed that erythema, edema and petechia were common in the colon. There have been several cases regarding the diagnostic role of CE in patients with IgAV. The main endoscopic findings were erythema throughout the small bowel, and severe erosions or ulcers were found in some cases 17 18 19 20 21 . In the current study, we also confirmed similar findings in our patients. Thus, the above-mentioned endoscopic findings are considered characteristic in the entire gastrointestinal tract including the jejunoileum of patients with IgAV.
As for patients with EGPA, only a few studies with endoscopic findings are available, probably because most of the gastrointestinal lesions previously discussed have been in patients with gastrointestinal tract perforation 22 23 . In such previous studies, ulcers or erythematous and nodular mucosa in the stomach, and/or ulcers or multiple small polyps in the duodenum were identified 15 24 . In some case reports, CE or BAE revealed that erosions, submucosal edema with lymphangiectasias and erythema, or ulcers of various shapes, such as multiple punched-out, small or irregular ulcers, were seen in the jejunum and ileum 25 26 27 28 . Colonoscopy showed mucosal erythema, erosion, ulceration, dark red sign or various red flares 10 29 . In the current study, we also confirmed similar findings in our patients. Thus, the above-mentioned endoscopic findings in the entire gastrointestinal tract seem characteristic in EGPA.
In the current investigation, we compared endoscopic findings between patients with IgAV and those with EGPA. As a result, mucosal erythema in the stomach, and mucosal erythema, ulcer, and hematoma-like protrusion in the duodenum were seen more frequently in patients with IgAV than in those with EGPA. Incidence of mucosal erythema, erosion, ulcer or hematoma-like protrusion in the jejunum/ileum and colorectum was no different between the two groups. In a previous study regarding EGD findings in primary vasculitis, the duodenum was the most frequently involved site 30 . Also, EGD findings including erosion, petechiae, submucosal hemorrhage or ulcers were seen in 142 of 148 patients (95.9 %). However, that study did not clarify what EGD findings are characteristic of each disease.
To date, no previous studies have compared characteristic endoscopic findings between patients with IgAV and EGPA. In the current study, we compared the endoscopic findings between the two groups. As a consequence, we found that incidence of jejunoileal involvement was high in both groups, and we also presume that gastric mucosal erythema, and mucosal erythema, ulcer, and hematoma-like protrusion in the duodenum may be characteristic endoscopic signs for IgAV.
There have only been a few studies on frequency of gastrointestinal bleeding in patients with IgAV and EGPA. In previous studies, clinical signs of gastrointestinal bleeding were found in 17 % to 49 % of patients with IgAV and 9 % of patients with EGPA 7 8 9 31 32 . Our results showed that frequency of gastrointestinal bleeding was 27 % (9 of 33) in patients with IgAV and 11 % (2 of 19 patients) in patients with EGPA. We can also confirm that gastrointestinal involvement of IgAV and EGPA favorably responds to therapy regardless of presence of bleeding. There have been several case series showing fair to good response of gastrointestinal lesions in the diseases observed by endoscopy 7 20 28 29 . It thus seems likely that medical treatment is the first choice of treatment for gastrointestinal involvement in IgAV and EGPA.
We can also confirm that incidence of characteristic histologic findings in the gastrointestinal tract was lower compared with that of the skin. Histopathological findings of IgAV are characterized by leukocytoclastic vasculitis 4 . Nishiyama et al. 8 reported that all 11 biopsy specimens from EGD and colonoscopy in patients with IgAV showed nonspecific inflammatory cell infiltration and diagnoses were made from skin biopsies. The main histopathological findings in EGPA are extravascular granulomas, small and medium-sized vessels vasculitis, and eosinophilic infiltrates 11 . These findings are rarely seen on biopsy sections. This was probably because most biopsies are limited to the superficial portion of the mucosa and cannot reach the deeper vessels. A vasculitis diagnosis should be made with consideration of all clinical and pathologic information, but gastrointestinal involvement in patients with vasculitis may be life-threatening because of complications such as severe ischemia, infarction, and perforation. Therefore, accurate diagnosis and early treatment is important to avoid fatal outcomes, and endoscopic examination helps to define the site and extent of gastrointestinal involvement.
The current study has some limitations. We were not able to examine the entire gastrointestinal tract in all the patients diagnosed as having IgAV or EGPA from 2008 to 2017. Considering the rarity of the disease, we consider that our 52 patients are a decent number on which to base a study on IgAV and EGPA. In addition, this was retrospective study with a small sample size. Additional prospective studies of large cohorts are, therefore, needed in the near future.
Conclusion
In conclusion, our study revealed frequent duodenal involvement, gastric mucosal erythema, and duodenal mucosal erythema, ulcer, and hematoma-like protrusion in patients with IgAV. We also foound that incidence of jejunoileal involvement was high in patients with IgAV and those with EGPA. These findings support use of small-bowel endoscopy as a helpful procedure for diagnosis of small-bowel lesions in IgAV or EGPA.
Footnotes
Competing interests None
References
- 1.Jennette J C, Falk R J, Andrassy K et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–192. doi: 10.1002/art.1780370206. [DOI] [PubMed] [Google Scholar]
- 2.Jennette J C, Falk R J, Bacon P A et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65:1–11. doi: 10.1002/art.37715. [DOI] [PubMed] [Google Scholar]
- 3.Louie C Y, DiMaio M A, Charville G W et al. Gastrointestinal tract vasculopathy: clinicopathology and description of a possible “new entity” with protean features. Am J Surg Pathol. 2018;42:866–876. doi: 10.1097/PAS.0000000000001060. [DOI] [PubMed] [Google Scholar]
- 4.Mills J A, Michel B A, Bloch D A et al. The American College of Rheumatology 1990 criteria for the classification of Henoch-Schönlein purpura. Arthritis Rheum. 1990;33:1114–1121. doi: 10.1002/art.1780330809. [DOI] [PubMed] [Google Scholar]
- 5.Martinez-Frontanilla L A, Haase G M, Ernster J A et al. Surgical complications in Henoch-Schönlein Purpura. J Pediatr Surg. 1984;19:434–436. doi: 10.1016/s0022-3468(84)80269-9. [DOI] [PubMed] [Google Scholar]
- 6.Chumbley L C, Harrison E G, Jr, DeRemee R A. Allergic granulomatosis and angiitis (Churg-Strauss syndrome). Report and analysis of 30 cases. Mayo Clin Proc. 1977;52:477–484. [PubMed] [Google Scholar]
- 7.Zhang Y, Huang X. Gastrointestinal involvement in Henoch-Schönlein purpura. Scand J Gastroenterol. 2008;43:1038–1043. doi: 10.1080/00365520802101861. [DOI] [PubMed] [Google Scholar]
- 8.Nishiyama R, Nakajima N, Ogihara A et al. Endoscope images of Schönlein-Henoch purpura. Digestion. 2008;77:236–241. doi: 10.1159/000150697. [DOI] [PubMed] [Google Scholar]
- 9.Esaki M, Matsumoto T, Nakamura S et al. gastrointestinal involvement in Henoch-Schönlein purpura. Gastrointest Endosc. 2002;56:920–923. doi: 10.1067/mge.2002.129592. [DOI] [PubMed] [Google Scholar]
- 10.Tsurikisawa N, Oshikata C, Tsuburai T et al. Th17 cells reflect colon submucosal pathologic changes in active eosinophilic granulomatosis with polyangiitis. BMC Immunol. 2015;16:75. doi: 10.1186/s12865-015-0138-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gioffredi A, Maritati F, Oliva E et al. Eosinophilic granulomatosis with polyangiitis: an overview. Front Immunol. 2014;5:549. doi: 10.3389/fimmu.2014.00549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fries J F, Hunder G G, Bloch D A et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Summary. Arthritis Rheum. 1990;33:1135–1136. doi: 10.1002/art.1780330812. [DOI] [PubMed] [Google Scholar]
- 13.Masi A T, Hunder G G, Lie J T et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis) Arthritis Rheum. 1990;33:1094–1100. doi: 10.1002/art.1780330806. [DOI] [PubMed] [Google Scholar]
- 14.Szer I S. Henoch-Schönlein purpura: when and how to treat. J Rheumatol. 1996;23:1661–1665. [PubMed] [Google Scholar]
- 15.Pagnoux C, Mahr A, Cohen P et al. Presentation and outcome of gastrointestinal involvement in systemic necrotizing vasculitides: analysis of 62 patients with polyarteritis nodosa, microscopic polyangiitis, Wegener granulomatosis, Churg-Strauss syndrome, or rheumatoid arthritis-associated vasculitis. Medicine (Baltimore) 2005;84:115–128. doi: 10.1097/01.md.0000158825.87055.0b. [DOI] [PubMed] [Google Scholar]
- 16.Akdamar K, Agrawal N M, Varela P Y. The endoscopic appearance of anaphylactoid purpura. Gastrointest Endosc. 1973;20:68–69. doi: 10.1016/s0016-5107(73)73878-5. [DOI] [PubMed] [Google Scholar]
- 17.Kishikawa H, Nishida J, Takarabe S et al. “Circular reddish lesions”: a possibly characteristic endoscopic finding in Henoch-Schönlein purpura. Endoscopy. 2013;45:E33–E34. doi: 10.1055/s-0032-1325886. [DOI] [PubMed] [Google Scholar]
- 18.Skogestad E. Capsule endoscopy in Henoch-Schonlein purpura. Endoscopy. 2005;37:189. doi: 10.1055/s-2004-826188. [DOI] [PubMed] [Google Scholar]
- 19.Stancanelli B, Vita A, Vinci M et al. Bleeding of small bowel in Henoch-Schönlein syndrome: the successful diagnostic role of video capsule endoscopy. Am J Med. 2006;119:82–84. doi: 10.1016/j.amjmed.2005.05.034. [DOI] [PubMed] [Google Scholar]
- 20.PreudʼHomme D L, Michail S, Hodges C et al. Use of wireless capsule endoscopy in the management of severe Henoch-Schonlein purpura. Pediatrics. 2006;118:904–906. doi: 10.1542/peds.2005-3111. [DOI] [PubMed] [Google Scholar]
- 21.Ichikawa R, Hosoe N, Imaeda H et al. Evaluation of small-intestinal abnormalities in adult patients with Henoch-Schönlein purpura using video capsule. Endoscopy. 2011;43:162–163. doi: 10.1055/s-0030-1256266. [DOI] [PubMed] [Google Scholar]
- 22.Assmann G, Molinger M, Pfreundschuh M et al. Gastrointestinal perforation due to vasculitis at primary diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) despite a high dose glucocorticosteroids treatment. Springerplus. 2014;3:404. doi: 10.1186/2193-1801-3-404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ohnuki Y, Moriya Y, Yutani S et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss Syndrome) complicated by perforation of the small intestine and cholecystitis. Intern Med. 2018;57:737–740. doi: 10.2169/internalmedicine.8975-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Franco D L, Ruff K, Mertz L et al. Eosinophilic granulomatosis with polyangiitis and diffuse gastrointestinal involvement. Case Rep Gastroenterol. 2014;8:329–336. doi: 10.1159/000369129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sánchez R, Aparicio J R, Baeza T et al. Capsule endoscopy diagnosis of intestinal involvement in a patient with Churg-Strauss syndrome. Gastrointest Endosc. 2006;6:1082–1084. doi: 10.1016/j.gie.2006.01.003. [DOI] [PubMed] [Google Scholar]
- 26.Beye B, Lesur G, Claude P et al. Small bowel involvement documented by capsule endoscopy in Churg-Strauss syndrome. Pan Afr Med J. 2015;22:41. doi: 10.11604/pamj.2015.22.41.7810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Suzuki T, Matsushima M, Arase Y et al. Double-balloon endoscopy-diagnosed multiple small intestinal ulcers in a Churg-Strauss syndrome patient. World J Gastrointest Endosc. 2012;4:194–196. doi: 10.4253/wjge.v4.i5.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kawasaki K, Eizuka M, Murata O et al. Eosinophilic granulomatosis with polyangiitis involving the small intestine: radiographic and endoscopic findings. Endoscopy. 2015;47:492–494. doi: 10.1055/s-0034-1393140. [DOI] [PubMed] [Google Scholar]
- 29.Yoshioka T, Kusaka T, Seno H. Colonic findings in Churg-Strauss syndrome. Endoscopy. 2013;45:185–186. doi: 10.1055/s-0033-1344062. [DOI] [PubMed] [Google Scholar]
- 30.Gong E J, Kim do H, Chun J H et al. Endoscopic findings of upper gastrointestinal involvement in primary vasculitis. Gut Liver. 2016;10:542–548. doi: 10.5009/gnl15198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Audemard-Verger A, Terrier B, Dechartres A et al. Characteristics and Management of IgA vasculitis (Henoch-Schönlein) in adults: data from 260 patients included in a French multicenter retrospective survey. Arthritis Rheumatol. 2017;69:1862–1870. doi: 10.1002/art.40178. [DOI] [PubMed] [Google Scholar]
- 32.Durel C A, Berthiller J, Caboni S et al. Long-term followup of a multicenter cohort of 101 patients with eosinophilic granulomatosis with polyangiitis (Churg-Strauss) Arthritis Care Res (Hoboken) 2016;68:374–387. doi: 10.1002/acr.22686. [DOI] [PubMed] [Google Scholar]