

Abstract
Background
Currently there are no reference intervals (RIs) of sodium (Na), potassium (K), and chlorine (Cl) on Chinese population. Two kinds of ion‐selective electrode (ISE) methods were commonly used to determine K, Na, and Cl levels in China, the difference between these two methods needs to be evaluated.
Methods
A total of 4,524 healthy participants (1,916 males and 2,608 females) between 20–79 years old from six cities in China were selected by strict criteria. Serum K, Na, and CL were tested on Roche Modular analyzers in six assigned laboratories. According to EP‐9A2, using Roche Modular analyzer (indirect ISE) as comparative method, Olympus AU 5400 analyzer (indirect ISE) and Johnson&Johnson Fusion 5.1 analyzer (direct ISE) were evaluated.
Results
In Chinese population, the RIs for K, Na, and CL are 3.6–5.2, 136–146, and 99–110 mmol/l, respectively. Compared to the Roche indirect ISE method, Johnson direct ISE method showed a positive bias; and Olympus indirect ISE method just showed a very slight bias.
Conclusion
The RIs of K, Na, and Cl of Han Chinese healthy adult population were found to be smaller than those provided by the manufacturer. By a criteria of biological variations for CV, the differences of Na and K between Roche analyzer and Johnson analyzer were not acceptable for clinical application, while the differences of Na, K, and Cl between Roche and Olympus analyzers were acceptable for clinical application.
Keywords: reference intervals, potassium, sodium, chlorine, Chinese population, method comparison
INTRODUCTION
Reference intervals (RIs) are commonly used as “decision support tools” to interpret the reports in the laboratories 1. They are essential to the physicians to differentiate between healthy and unhealthy population. According to ISO 15189 2, “biological reference intervals should be periodically reviewed. A review of biological reference intervals should also been taken when a laboratory changes its analytical procedure or pre‐analytical procedure, if appropriate.” For decades, most laboratories in China used the manufacturers’ reference values or rely on the values from literature. However, most RIs supplied by manufacturers are based on the data from population in western countries. Due to the population difference, the analytical procedure difference, it is necessary to establish the RIs from Chinese population. The balance of electrolytes in body fluid is important to maintain the osmotic pressure and the normal distribution of body fluid. Sodium (Na) and potassium (K) are two of the main positive ions; chlorine (Cl) is one of the main negative ions in body fluid. The objective of this study is to establish the RIs of serum Na, K, and Cl in healthy adult Han population of China, and to compare two ion‐selective electrode (ISE) methods.
In this study, we followed the procedure to establish the RIs recommended by the Clinical and Laboratory Standards Institute (CLSI) document C28‐A3 3. Totally, 4,524 volunteers between 20 and 79 years old were recruited in six representative cities (Shenyang, Beijing, Shanghai, Guangzhou, Chengdu, and Xi'an) in China. EP9‐A2 4 was applied to evaluate the differences between two ISE methods.
MATERIALS AND METHODS
Ethics Approval
This study was approved by the ethics committee of the First Hospital of China Medical University.
Participants
There were 7,612 adults enrolled in this study from six cities in China, including Shenyang, Beijing, Shanghai, Guangzhou, Chengdu, Xi'an, covering cities and suburbs. All the participants were asked to complete a questionnaire including age, sex, ethnic group, career, exercise, diet, smoking history, alcohol consumption status, drug history, environment, etc. Each participant was checked by a complete physical examination (such as blood pressure, electrocardiogram, chest X‐ray, and ultrasonic scanning) and clinical laboratory tests (such as complete blood count, urinalysis, fasting glucose, triglyceride, cholesterol, HBsAg, anti‐HCV, and anti‐HIV).
To select healthy Chinese Han volunteers, the following conditions or history was checked: no acute or chronic infections, no vascular, heart, liver, kidney or endocrine disease; systolic pressure <140 mmHg and diastolic pressure <90 mmHg (average of two measurements); no pregnant or postpartum less than a year; no surgery during the past 6 months or no drugs within 2 weeks; no blood transfusion or blood donation within 4 months; no obesity (body mass index ≥28); no diabetes mellitus; no tumor; no smoking ≥20 cigarettes per day or no drinking ethanol ≥30g per day. Also, fasting blood glucose <7.0 mmol/l, triglyceride <2.26 mmol/l, total cholesterol <6.22 mmol/l, no HBsAg, anti‐HCV, or anti‐HIV, no abnormal results of protein, glucose, complete blood count, or urinalysis; no severe vomiting or diarrhea >3 per day within 2 weeks. The participants were excluded if there were the subject had Lipaemia (TG > 2.26 mmol/l), icterus (TBil > 34.2 μmol/l), or hemolysis (H >0.6 g/l). Totally, 4,524 healthy individuals (1,916 males and 2,608 females) were selected and included in this study, and 3,088 individuals were excluded.
Specimen Collection
All the subjects signed a consent form. They were instructed to keep usual diet and to avoid strenuous physical exercise at least 3 days before blood collection. Blood was taken between September 2010 and January 2011. All participants were fasted for more than 8 h, but less than 14 h. The blood samples were collected in 5 ml gel separator tubes, and left at room temperature for 30 min to clot, then centrifuged for 10 min at 3,000 rpm. All the samples were analyzed by the assigned laboratories in each city (Lab 1‐Shenyang, Lab 2‐Beijing, Lab 3‐Shanghai, Lab 4‐Guangzhou, Lab 5‐Chengdu, Lab 6‐Xi'an) within 4 h.
Instrument and Assays
All analyses for RIs of K, Na, and CL were performed using Modular Analytics (Roche Diagnostics, Mannheim, Germany) using the manufacturer's reagents, calibrators (ISE Standard Low, High and ISE Compensator) and quality control (QC) products (Precinorm U and precipath U). The assigned values and uncertainties of ISE Standard Low, High and ISE Compensator are 3 ± 0.02, 7 ± 0.05, 4.67 ± 0.0125 mmol/l for K; 120 ± 0.5, 160 ± 0.8, 134 ± 0.5322 mmol/l for Na; 80 ± 0.5, 120 ± 0.8, 96.9 ± 0.1642 mmol/l for Cl. A survey was performed in the six assigned laboratories before analyzing. SRM 956c was used to validate the accuracy. Precinorm U and precipath U were used to evaluate precision according to the EP15‐A protocol recommended by CLSI. Four replicate samples at each concentration were analyzed daily for 5 days. The total CVs were calculated.
For comparison of different ISE method, Modular P800 analyzing system was employed as the comparative method, we evaluated two other analyzing systems: Olympus AU 5400 analyzer with the manufacturer's reagents, calibrators, and QC products, and Johnson&Johnson Fusion 5.1 analyzer with the manufacturer's reagents, calibrators, and QC products. Forty samples were selected in accordance with the concentration distribution proposed by CLSI guidelines (EP9‐A2; 4). The 40 samples were run in duplicates in 5 days by the comparative method and the two evaluated methods. The K, Na, and Cl measurements were compared according to the CLSI guidelines (EP9‐A2; 4).
Statistical Analysis
The general calculation and statistical analysis were conducted by SPSS 19.0. The determination of RIs was done according to the CLSI C28‐A3 guideline on defining, establishing, and verifying RIs. Outliners were removed using the Dixon test. The one‐way ANOVA followed by the Tukey test for paired means was used to compare the values of K, Na, Cl levels among age groups for the Gaussian distributions. A P < 0.05 was considered statistically significant. After excluding outliners, the 2.5th and 97.5th percentiles were calculated.The difference of gender group was tested by the standard normal deviation test, comparing Z and Z* 3. If the Z value exceeds Z*, or if the larger standard deviation exceeds the smaller by 1.5 times, regardless of the Z value, then separate RIs will be calculated for each subclass. For the final RIs, 1 decimal place was supplied for K and 0 for Na and Cl according to routine use.
For method comparison, correlation between methods was evaluated by using Passing–Bablok regression analysis 5, the Pearson correlation coefficient was calculated. Bias between methods was analyzed according to Bland and Altman analyzing. Predicted bias and its 95% confidence interval were calculated. If the acceptable bias is greater than the higher limits of the confidence interval of the predicted bias, the performance of the evaluated method is equivalent to the comparative method and is acceptable for the defined application.
RESULTS
Performance of the Tests
Accuracy
SRM 956c levels I, II, III from National Institute of Standards and Technology (NIST) were measured in each laboratory. The desirable requirements for bias based on group biological variation 7 are quite critical: target value ±1.8% for K, 0.3% for Na, and 0.5% for Cl. Most analyzers could not reach those standards. According to the quality requirements in CLIA’88, acceptable ranges for K and Na are target value ±0.5 mmol/l and ±4 mmol/l, for CL is target value ±5%, which are quite wide. In this article, in order to choose an appropriate criteria, the Health industry standards of China (WS/T 403–2012)6 were applied to compare the biases: target value ±2.0% for K, ±1.5% for Na, and ±1.5% for Cl.
The mean biases of each laboratory are shown in Table 1, for K, the results of three laboratories are over the limits (2%); for Na, the results of two laboratories are over the limits (1.5%); for Cl, the results of two laboratories are over the limits (1.5%). Most laboratories showed very small biases.
Table 1.
The Results of K, Na, and Cl for SRM 956c in Six Selected Labs of China
| 956c‐I | 956c‐II | 956c‐III | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Electrolyte | Lab | Target | Measurement | Bias (%) | Target | Measurement | Bias (%) | Target | Measurement | Bias (%) | Mean bias (%) | Standarda (%) |
| K | 1 | 5.976 | b | b | 3.977 | 3.89 | −2.19 | 1.982 | 1.90 | −4.14 | −3.17c | ±2 |
| (mmol/l) | 2 | 5.83 | −2.44 | 3.95 | −0.68 | 2.22 | 12.01 | 2.96c | ||||
| 3 | 6 | 0.40 | 4.1 | 3.09 | 2.10 | 5.95 | 3.15c | |||||
| 4 | 6.04 | 1.07 | 3.98 | 0.08 | 2.06 | 3.94 | 1.70 | |||||
| 5 | 6.03 | 0.90 | 4.02 | 1.08 | 2.04 | 2.93 | 1.64 | |||||
| 6 | 6.06 | 1.41 | 4.04 | 1.58 | 2.02 | 1.92 | 1.64 | |||||
| Na | 1 | 118.8 | b | b | 137.5 | 137.0 | −0.33 | 157.4 | 152.2 | −3.29 | −1.81c | ±1.5 |
| (mmol/l) | 2 | 120.3 | 1.23 | 136.9 | −0.41 | 161.5 | 2.63 | 1.15 | ||||
| 3 | 121.6 | 2.36 | 139.0 | 1.09 | 154.4 | −1.91 | 0.51 | |||||
| 4 | 120.2 | 1.18 | 139.0 | 1.09 | 166.2 | 5.59 | 2.62c | |||||
| 5 | 120.7 | 1.57 | 139.3 | 1.29 | 158.0 | 0.36 | 1.07 | |||||
| 6 | 123.1 | 3.60 | 140.5 | 2.15 | 154.2 | −2.05 | 1.23 | |||||
| Cl | 1 | 104.9 | b | b | 121.5 | 119.0 | −2.09 | 137.4 | 133.8 | −2.65 | −2.37c | ±1.5 |
| (mmol/l) | 2 | 102.9 | −1.89 | 118.0 | −2.88 | 140.6 | 2.34 | −0.81 | ||||
| 3 | 103.4 | −1.43 | 120.0 | −1.23 | 132.0 | −3.93 | −2.20c | |||||
| 4 | 103.3 | −1.56 | 119.4 | −1.71 | 143.4 | 4.38 | 0.37 | |||||
| 5 | 102.4 | −2.35 | 119.2 | −1.93 | 135.8 | −1.19 | −1.82 | |||||
| 6 | 104.3 | −0.59 | 120.8 | −0.58 | 134.3 | −2.27 | −1.15 | |||||
Health industry standards of China 7 were applied as the standard.
Due to rupture of the container, Lab 1 could not provide the data.
The bias is beyond the range of the standard.
Precision
According to EP15‐A, the total coefficient of variation for K, Na, Cl was calculated and shown in Table 2. The performance of K and Na was much better than that of Cl. All the total CVs of the six laboratories (except Lab 6) of K can reach the desirable requirements of group biological variation 7(±2.4% for K, ±0.4% for Na, and ±0.6% for Cl) and the Health industry standards of China (WS/T 403–2012)6. All the laboratories cannot reach the desirable requirements of group biological variation for Na (±0.4%), but can reach the Health industry standards of China (±1.5% for Na). Most of the total CVs of the six laboratories of Cl are over the limits of the two kinds of standards.
Table 2.
The Total CV (%) of K, Na, and Cl for Roche Quality Control Materials in Six Selected Labs
| Analyte | Electrolyte | Lab 1 | Lab 2 | Lab 3 | Lab 4 | Lab 5 | Lab 6 | Opt | Des | Min | Standarda |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precipath U | K | 0.99 | 1.36 | 1.43 | 1.79 | 0.82 | b | 1.2 | 2.4 | 3.6 | 2.5 |
| Na | 0.96 | 1.24 | 1.16 | 1.05 | 0.66 | b | 0.2 | 0.4 | 0.5 | 1.5 | |
| Cl | 1.85a | 1.17 | 1.53a | 1.18 | 1.65a | b | 0.3 | 0.6 | 0.9 | 1.5 | |
| Precinorm U | K | 1.26 | 1.97 | 1.57 | 1.91 | 0.9 | 1.31 | 1.2 | 2.4 | 3.6 | 2.5 |
| Na | 1.09 | 1.49 | 1.41 | 1.47 | 0.6 | 1.15 | 0.2 | 0.4 | 0.5 | 1.5 | |
| Cl | 1.96a | 1.54a | 2.09a | 1.66a | 1.79a | 1.36 | 0.3 | 0.6 | 0.9 | 1.5 |
Health industry standards of China 7 were applied as the standard.
Due to misoperation of the test, Lab 6 could not provide the data.
Characteristics of the Healthy participants
The main characteristics of the participants are listed in Table 3. In this study, there are no significant differences on age, fasting glucose, and cholesterol between male and female group (P > 0.05). The triglyceride level of male group is higher than that of female group (P < 0.001).
Table 3.
Characteristics of 4,524 Healthy Chinese Han Adults
| Characteristics | Male | Female | Total |
|---|---|---|---|
| No. (%) | 1,916 (42.4) | 2,608 (57.6) | 4,524 |
| Age (years) | 42.0 ± 16.3 | 42.4 ± 14.5 | 42.2±15.3 |
| Systolic blood pressure (mmHg) | 120.6 ± 10.5 | 116.0 ± 12.4 | 118.0 ± 10.9 |
| Diastolic blood pressure (mmHg) | 78.5 ± 7.2 | 75.4 ± 7.6 | 76.7 ± 7.6 |
| Fasting glucose (mmol/l) | 5.13 ± 0.49 | 5.04 ± 0.46 | 5.08 ± 0.48 |
| Total cholesterol (mmol/l) | 4.63 ± 0.76 | 4.73 ± 0.75 | 4.69 ± 0.76 |
| Triglyceride (mmol/l) | 1.11 ± 0.44 | 0.97 ± 0.42 | 1.03±0.43 |
RIs of K, Na, Cl
Gender group
Participants were divided into two groups by gender. Mean standard deviation and median were calculated for all parameters. Maximums and minimums were used to identify outliners. K, Na, Cl levels did not show statistically significant difference (Z < Z*and P > 0.05) between male and female group (Table 4).
Table 4.
Reference Intervals of K, Na, and Cl in Adult Healthy Chinese Han population
| Percentile | |||||||
|---|---|---|---|---|---|---|---|
| Ion | Group | No. | Method | 2.5th | 50th | 97.5th | RIs by manufacture |
| K (mmol/l) | Male | 1,916 | Indirect | 3.6 (3.61–3.69) | 4.3 | 5.3 (5.22–5.32) | 3.5–5.5 |
| Female | 2,608 | ISE | 3.6 (3.60–3.65) | 4.2 | 5.1 (5.10–5.19) | ||
| Combined | 4,524 | 3.6 (3.61–3.65) | 4.3 | 5.2 (5.18–5.24) | |||
| Na (mmol/l) | Male | 1,916 | Indirect | 136 (136.0–136.6) | 142 | 147 (146.2–147.0) | 130–150 |
| Female | 2,608 | ISE | 136 (135.1–136.0) | 141 | 146 (146.0–146.4) | ||
| combined | 4,524 | 136 (135.9–136.1) | 141 | 146 (146.1–146.5) | |||
| CL (mmol/l) | Male | 1,916 | Indirect | 99 (98.2–98.7) | 104 | 109 (108.7–109.3) | 94–110 |
| Female | 2,608 | ISE | 99 (98.7–99.2) | 104 | 110 (109.6–110.3) | ||
| combined | 4,524 | 99 (98.5–98.9) | 104 | 110 (109.3–109.8) | |||
Ninety percent confidence interval values of 2.5th and 97.5th percentiles were shown in the parentheses.
Age group
The participants were divided into six groups by age (20–29s, 30–39s, 40–49s, 50–59s, 60–69s, and 70–79s). One‐way ANOVA was used to compare mean age among six age groups, if there was a significant different (P < 0.05) between two groups, Z factor was calculated. It showed no significant difference among six groups (Z < Z*). K and Cl demonstrated a slightly increased level as age increased, while Na did not show this trend (Table 5).
Table 5.
Reference intervals of K, Na, and Cl in Adult Healthy Chinese Han Population in Six Age Groups
| K (mmol/l) | Na (mmol/l) | CL (mmol/l) | |||||
|---|---|---|---|---|---|---|---|
| Age group | No. | Mean ± SD | 2.5–97.5th | Mean ± SD | 2.5–97.5th | Mean ± SD | 2.5–97.5th |
| 20–29s | 1,181 | 4.2 ± 0.4 | 3.6–5.1 | 141 ± 3 | 136–146 | 104 ± 3 | 98–109 |
| 30–39s | 938 | 4.3 ± 0.4 | 3.6–5.2 | 141 ± 2 | 137–146 | 104 ± 3 | 99–110 |
| 40–49s | 934 | 4.3 ± 0. 4 | 3.6–5.2 | 141 ± 2 | 136–146 | 104 ± 3 | 99–110 |
| 50–59s | 760 | 4.3 ± 0.4 | 3.6–5.1 | 142 ± 3 | 135–147 | 104 ± 3 | 99–110 |
| 60–69s | 450 | 4.4 ± 0.4 | 3.7–5.4 | 142 ± 3 | 135–147 | 104 ± 3 | 99–110 |
| 70–79s | 261 | 4.6 ± 0.5 | 3.7–5.6 | 141 ± 3 | 136–146 | 104 ± 2 | 99–109 |
| Combined | 4,524 | 4.3 ± 0.4 | 3.6–5.2 | 141 ± 3 | 136–146 | 104 ± 3 | 99–110 |
Area group
Participants were divided into six groups by cities, with mean, standard deviation, and 2.5th, 97.5th percentiles were calculated for each parameter. The results were listed in Table 6. After comparing Z and Z*, for serum Na, it showed slight difference among Lab 1 (Shenyang), Lab 2 (Beijing), Lab 3 (Shanghai), Lab 4 (Guangzhou), Lab 6 (Xi'an; Z > Z*); for serum Cl, it showed slight difference between Lab 1 and Lab 2 (Z > Z*), between Lab 5 (Chengdu) and Lab 6 (Z > Z*); for serum K, it showed no statistically significant difference among six cities (Z < Z*).
Table 6.
Reference Intervals of K, Na, and Cl in Adult Healthy Chinese Han Population in Six Different Cities in China
| K (mmol/l) | Na (mmol/l) | CL (mmol/l) | |||||
|---|---|---|---|---|---|---|---|
| Area | No. | Mean ± SD | 2.5–97.5th | Mean ± SD | 2.5–97.5th | Mean ± SD | 2.5–97.5th |
| Shenyang (Lab 1) | 739 | 4.4 ± 0.4 | 3.7–5.3 | 142±2 | 138–147 | 105 ± 3 | 99–110 |
| Beijing (Lab 2) | 674 | 4.3 ± 0.4 | 3.6–5.1 | 140 ± 3 | 134–144 | 103 ± 2 | 99–107 |
| Shanghai (Lab 3) | 623 | 4.2 ± 0.3 | 3.6–5.0 | 141 ± 2 | 137–146 | 104 ± 2 | 98–108 |
| Guangzhou (Lab 4) | 1,011 | 4.3 ± 0.4 | 3.7–5.4 | 141 ± 2 | 137–145 | 104 ± 2 | 100–108 |
| Chengdu (Lab 5) | 728 | 4.2 ± 0.4 | 3.6–5.0 | 143 ± 2 | 139–148 | 106 ± 3 | 101–111 |
| Xi'an (Lab 6) | 749 | 4.4 ± 0.4 | 3.6–5.3 | 141 ± 3 | 133–147 | 103 ± 3 | 98–110 |
| Combined | 4,524 | 4.3 ± 0.4 | 3.6–5.2 | 141 ± 3 | 136–146 | 104 ± 3 | 99–110 |
According to the guideline of determining reference values (C28‐A3), significant differences between some city groups for K, Na, Cl, it may be due to the large sample numbers. Whether it is necessary to assign subclass RIs for these groups will be depend on the clinical significance and clinical application not only on the statistical data or analysis.
No outliners were detected in each group by the Dixon test. The RIs are presented as the 2.5–97.5th percentile ranges.
The final results for K, Na, and Cl in healthy Chinese Han adult population are shown in Table 4. The combined RIs for K, Na, and Cl were 3.6–5.2, 136–146, and 99–110 mmol/l; the RIs from the manufacturer for K, Na, and Cl were 3.3–5.1, 133–145, and 96–108 mmol/l, respectively. Compared to the RIs provided by the manufacturer, the lower limits of RIs from this study were higher, the upper limits were similar.
Evaluation of Two Other Biochemical Analyzing Systems
Olympus analyzing system and Johnson&Johnson analyzing system in determining K, Na, and Cl intervals were evaluated by Roche analyzing system. Both two evaluated methods were closely correlated to the comparative method (R 2 > 0.92). The correlation coefficients (R 2) and the regression equations were listed in Table 7. At the lower and upper reference limit points (Xr) for serum K, Na, CL (for K, Xr = 3.6, 5.2, mmol/l; for Na, Xr = 136, 146 mmol/l; for Cl, Xr = 99,110 mmol/l), the 95% confidence intervals of the predicted bias for all the evaluated methods were calculated, and the acceptable bias is listed according to the minimal requirements of biological variation for CV 6(±3.6% for K, ±0.5% for Na, and ±0.9% for Cl) in Table 8. For evaluated method 1, all the 95% confidence intervals of the predicted bias of K, Na, and Cl were less than the range of acceptable bias. For evaluated method 2, the 95% confidence intervals of the predicted bias of K and Na were over than the range of acceptable bias, but that of Cl was less than the limit (Table 8).
Table 7.
Regression Equations for Two Evaluated Methods (Y) Versus the comparative method (X)
| Evaluated method 1a | Evaluated method 2a | |||
|---|---|---|---|---|
| Ion | Correlation equation | R 2 | Correlation equation | R 2 |
| K | Y = 1.004X − 0.054 | 0.994 | Y = 1.022X + 0.024 | 0.993 |
| Na | Y = 1.030X − 3.612 | 0.916 | Y = 1.039X − 4.619 | 0.822 |
| Cl | Y = 1.032X − 4.196 | 0.966 | Y = 1.014X − 1.310 | 0.938 |
Roche as the comparative method; Olympus as evaluated method 1, Johnson&Johnson as evaluated method 2.
Table 8.
The Predictive Bias and the 95% Confidence Intervals at the Medical Decision Points for two Evaluated Methods
| Evaluated method 1 | Evaluated method 2 | |||
|---|---|---|---|---|
| Ion (mmol/l) | Xrb (mmol/l) | 95% CI of predictive biasa | 95% CI of predictive biasa | Acceptable bias (mmol/l) |
| K | 3.6 | −0.04 (−0.15–0.07) | 0.10 (−0.04–0.24) | ±0.13 |
| 5.2 | −0.03 (−0.14–0.08) | 0.14 (0.01–0.28) | ±0.19 | |
| Na | 136 | 0.43 (0.34–0.53) | 1.11 (0.64–1.57) | ±0.68 |
| 146 | 0.63 (0.54–0.73) | 1.50 (1.03–1.96) | ±0.73 | |
| Cl | 99 | −1.03 (−1.11–0.94) | 0.13 (−0.25–0.51) | ±0.89 |
| 110 | −0.68 (−0.75–0.59) | 0.12 (−0.26–0.49) | ±0.99 |
Ninety‐five percent CI of predictive bias was listed in parentheses; the minimal requirements of biological variation for CV (7) were applied as acceptable bias (±3.6% for K, ±0.5% for Na, and ±0.9% for Cl).
Xr stands for reference limits.
Applying Olympus indirect ISE method as evaluated method 1, Johnson&Johnson direct ISE method as evaluated method 2, Roche indirect ISE method as the comparative method.
The differences between methods expressed as Bland–Altman plots were reported in Figure 1A–F. Compared to the Roche method, Olympus‐K method showed a very small bias (Fig. 1A, mean ± SD: −0.04 ± 0.05 mmol/l); Olympus‐Na method also showed a small bias (Fig. 1B, mean ± SD: 0.60 ± 1.10 mmol/l); whereas Olympus‐Cl method showed a very small negative bias (Fig. 1C, mean ± SD: −0.74 ± 0.82 mmol/l). Compared to the Roche method, Johnson‐K method showed a small positive bias (Fig. 1D, mean ± SD: 0.12 ± 0.06 mmol/l); and Johnson‐Na and Johnson‐Cl methods showed positive biases (Fig. 1E, mean ± SD: 0.86 ± 1.54 mmol/l; Fig. 1F, mean ± SD: 0.23 ± 1.09 mmol/l).
Figure 1.
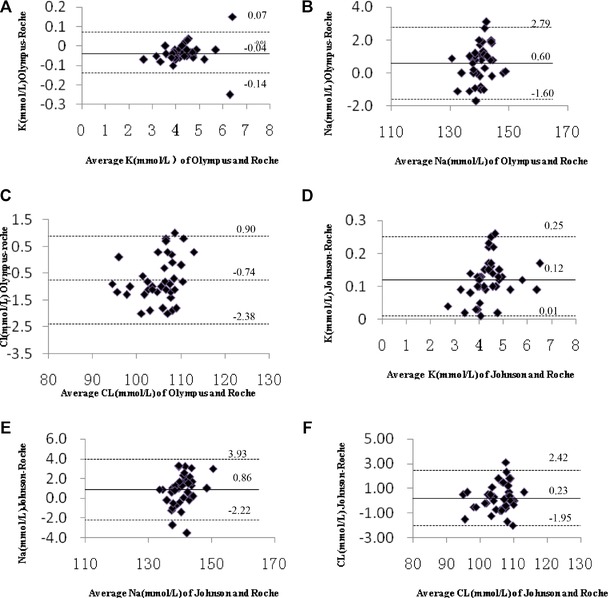
Differences of K, Na, Cl determinations between two evaluated methods and the reference method (Bland– Altman plots). Solid line (—) represents mean, dotted line (…..) represents mean ± 2SD.
DISCUSSION
It is the responsibility for the clinical laboratories to set up the RIs correctly, However, it is time consuming and a costly procedure. Setting up the RIs of electrolytes is very important for clinical diagnosis. In this study, six laboratories from six cities in China were involved to establish the common RIs of K, Na, and Cl for healthy Chinese Han population. These six cities (Beijing, Shenyang, Shanghai, Guangzhou, Chengdu,and Xi'an) are representative for most areas in China.
The most critical steps in the determination of reference values were to select participant individuals according to the specifically developed inclusion and exclusion criteria and use of quality‐controlled analytical procedures 8, 9. Some studies have used hospital inpatients databases or the population for healthy check‐up 10, other studies have recruited healthy subjects 11, 12. Sometimes, meaning of “healthy” is a relative concept, and it is difficult to set a universal definition 11. In this study, all the participants completed a detailed questionnaire and were checked by an overall physical examination. Since the K, Na, and Cl levels may be affected by dietary habits 14, the participants were questioned on lifestyle, diet, water drinking habits. Some screening tests were also performed, such as fasting glucose, triglyceride, cholesterol, hemoglobulin, and urinalysis. Participants with any abnormal results were excluded. Totally, among 7,612 participants, 4,524 individuals were selected as healthy adults from Chinese Han volunteers. For the process of establishing RIs, the conditions of samples, performance of assays, and statistics analysis were all considered key factors to ensure credible RIs.
All the data of K, Na, and Cl in our study showed Gaussian distributions. Gender, age, and area are the factors to be observed for determining whether subclasses of RIs are needed. The differences were tested by the standard normal deviate tests. According to C28‐A3 3, if the calculated statistic Z values exceed the critical value Z*, separating RIs for subclasses should be considered. Since there were no significant difference between male and female group (Z < Z*), it was not necessary to set up subclasses of genders. There were significant differences between some of the six age groups (20–29s, 30–39s, 40–49s, 50–59s, 60–69s, and 70–79s; P < 0.05) through one‐way ANOVA analysis. The statistic Z values were calculated, and all of them were less than the critical value Z*, therefore, again it was not necessary to set up age subclasses. It was a little different for area groups. After comparing Z and Z*, for serum Na, it showed slight difference between Lab 1 (Shenyang) and Lab 2 (Beijing), Lab 3 (Shanghai), Lab 4 (Guangzhou), Lab 6 (Xi'an; Z > Z*); for serum Cl, it showed slight difference between Lab 1 and Lab 2 (Z > Z*), between Lab 5 (Chengdu) and Lab 6 (Z > Z*); for serum K, it showed no significant difference among six cities (Z < Z*). The subclasses of areas were not set up for two reasons: first, the differences were very small (the differences between means are all less than 2 mmol/l), which may be due to the large sample number, and this may not affect the clinical significance. Second, the aim of this study was to establish the common RIs, it would be inconvenient for clinical application to set up many subclasses with slight differences. The differences of Na and Cl among the areas may be due to the differences of dietary habits 14. There are 56 ethnic groups in China, and Han is the highest population (>90%), so the RIs in the Han population were preliminarily established.
In this study, the combined RI for K, Na, Cl was 3.6–5.2, 136–146, 99–110 mmol/l, respectively. Compared to the RIs provided by manufacturer (3.5–5.5 mmol/l for K, 130–150 mmol/l for Na, and 94–110 mmol/l for CL), ours showed smaller intervals. The lower limits of ours were higher, and the upper limits were lower. Therefore, it is inappropriate to adopt manufacturer's RIs without verification. Compared to A.O.K. Chan's study in Hong Kong (12)(3.7–4.7 mmol/l for K, 138–145 mmol/l for Na), which enrolled 337 volunteers and with only 22 were over 60 years, the upper limits of K in our study are much higher because much more subjects were over 60 years (711), and the RIs of Na were similar.
In China, many types of analyzers were used in different laboratories. Before this study began, a survey was conducted to choose a proper analyzing system. After the accuracy and precision tests, Roche Modular analyzing system (indirect ISE method) with manufacturer's reagents was employed in the six assigned laboratories to test the samples of the participants in this study. There are many methods to detect serum K, Na, and Cl. For serum K and Na detection, flame emission spectrophotometry is used as reference method, while ion selective electrode method is commonly used in most laboratories. However, indirect ISE is used more frequently used than direct ISE. For indirect ISE, sample dilution is needed and the results will show false decreasing if the samples are hyperproteinemia or hyperlipemia. For direct ISE, dilution is not needed, so this will not be affected by hyperproteinemia or hyperlipemia. In this study, indirect ISE was applied on Roche Modular analyzer and Olympus analyzer, and direct ISE was used on Johnson&Johnson dry chemistry analyzer. As shown in Figure 1, compared to the Roche method, Johnson‐K, ‐Na, and ‐Cl methods all showed a small positive bias; and Olympus‐K, ‐Na, and ‐Cl methods showed a very slight bias.
According to the criteria of CLSI EP9‐A2 4, when evaluating the difference between the evaluated methods and the comparative method, the confidence intervals of the predicted bias should be compared with the definition of acceptable error at the medical decision points. In our study, instead of medical decision points, reference limits were applied. If the confidence interval for predicted bias includes the defined acceptable bias, then the data did not show that the bias of evaluated method was different from the acceptable bias. If the acceptable bias is less than the lower limit of the confidence interval of the predicted bias, the performance of the evaluated method is not equivalent to the current method and may not be acceptable for the defined application. If the acceptable bias is greater than the higher limit of the confidence interval of the predicted bias, the performance of the evaluated method is equivalent to the comparative method and is acceptable for the defined clinical application. In this study, for Olympus system, the confidence intervals of the predicted bias of K, Na, and Cl were less than the limit of the acceptable bias at the medical decision points, respectively; for Johnson system, the 95% confidence intervals of the predicted bias of K and Na were over the range of acceptable bias, while those of Cl were less than the range of acceptable bias. Therefore, the difference between Roche and Olympus system in detecting K, Na, and Cl is acceptable for clinical application, and the RIs established by Roche systems can be validated and then applied on Olympus system. The difference between Roche and Johnson systems for detecting serum K and Na is not acceptable for clinical application, but the biases are very small. The CV of K (mean = 4.0 mmol/l) on this Johnson analyzer was 1.5%, and the CV of Na (mean = 143 mmol/l) was 1.4%, which may have caused the difference. The RIs of Cl established by Roche systems can be validated and then applied on Johnson system. The biological variations based on groups for CV were used as acceptant biases, which are very critical (±3.6% for K, ±0.5% for Na, and ±0.9% for Cl). In this study, the 40 samples we selected to compare the methods were within normal total protein levels (62–83 g/l), total cholesterol levels (<5.18 mmol/l), and triglyceride levels (<2.26 mmol/l), which will not cause the obvious difference between direct and indirect ISE methods. The plasma Na, K, and chloride measurements are affected by changes in plasma protein concentration when measured by indirect ISE methods 15. Clinicians must be aware of those differences.
Acceptance of common RIs by laboratories also requires adoption of common reporting formats and acceptance of assumptions concerning the intervals. Thus, an agreement needs to be reached before common intervals can be set, such as use of the same units, reporting the number in the same decimal format, and rounding the RI limits 16 .The standardization of the test results, control of precision, and the CV among different laboratories are also important for RIs to be adequately applied. The RIs of serum K, Na, and Cl levels in Chinese Han adult population have been established, however there are still work to be done before it can be applied in the clinical laboratories in China.
CONCLUSIONS
The RIs of K, Na, and Cl of Han Chinese healthy adult population were found to be smaller than those provided by the manufacturer. By criteria of biological variation for CV, only the difference of CL between Roche and Johnson methods was acceptable for clinical application, and that of Na, K, and Cl between Roche and Olympus methods was acceptable for clinical application.
ACKNOWLEDGMENTS
We acknowledge and thank all participants for their cooperation and sample contributions. We thank all the staff of research centers involved in this study.
Grant sponsor: Ministry of Health, the People's Republic of China; Grant sponsor: National key Technologies R&D Program of China; Grant number: 2012BAI37B01.
REFERENCES
- 1. Jones G, Barker A. Reference intervals. Clin Biochem Rev 2008;29(Suppl 1):S93–S97. [PMC free article] [PubMed] [Google Scholar]
- 2. Medical laboratories particular requirements for quality and competence ISO 15189 [S] . International Organization for Standardization (ISO), 2007.
- 3. CLSI Approved Guideline‐Third Edition (EP28‐A3): Defining, establishing, and verifying reference intervals in the clinical laboratory . Clinical Laboratory and Standards Institute (CLSI) 2008.
- 4. CLSI Approved Guideline‐Second Edition (EP9‐A2): Method Comparison and Bias Estimation Using Patient samples . Clinical Laboratory and Standards Institute (CLSI), 2002.
- 5. Passing H, Bablok W. A new biometrical procedure for testing the equality of measurements from two different analytical methods. Clin Chem Clin Biochem 1983:21:709–720. [DOI] [PubMed] [Google Scholar]
- 6. National Health and Family Planning Commission of the People's Republic of China . Health industry standards of the People's Republic of China: Analytical quality specifications for routine analytes in clinical biochemistry. WS/T 403–2012.
- 7. Petersen PH, Fraser CG. Strategies to set global analytical quality specifications in laboratory medicine: 10 years on from the Stockholm consensus conference. 2010;15:323–330. [Google Scholar]
- 8. Horn PS, Pesce AJ. Reference intervals: An update. Clin Chim Acta 2003;334:5–23. [DOI] [PubMed] [Google Scholar]
- 9. Geffre A, Friedrichs K, Harr K, Concordet D, Trumel C, Braun JP. Reference values: A review. Vet Clin Pathol 2009;38:288–298. [DOI] [PubMed] [Google Scholar]
- 10. Pottel H, Vrydags N, Mahieu B, Vandewynckele E, Croes K, Martens F. Establishing age/sex related serum creatinine reference intervals from hospital laboratory data based on different statistical methods. Clin Chim Acta 2008;396:49–55. [DOI] [PubMed] [Google Scholar]
- 11. Southcott EK, Kerrigan JL, Potter JM, et al. Establishment of pediatric reference intervals on a large cohort of healthy children. Clin Chim Acta 2010;411:1421–1427. [DOI] [PubMed] [Google Scholar]
- 12. Chan AOK, Lee KC, Leung JNS, Shek CC. Reference intervals of common serum analytes of Hong Kong Chinese. J Clin Pathol 2008;61:632–636. [DOI] [PubMed] [Google Scholar]
- 13. Walton RM. Establishing reference intervals: Health as a relative concept. Semin Avian Exot Pet Med 2011;10:66–71. [Google Scholar]
- 14. Ichihara K, Itoh Y, Lam CW, et al. Sources of variation of commonly measured serum analytes in 6 Asian cities and consideration of common reference intervals. Clin Chem 2008;54:356–365. [DOI] [PubMed] [Google Scholar]
- 15. Dimeski G, Barnett RJ. Effects of total plasma protein concentration on plasma sodium, potassium and chloride measurements by an indirect ion selective electrode measuring system. Crit Care Resusc 2005;7:12–15. [PubMed] [Google Scholar]
- 16. Jones GD, Barker A, Tate J, Lim CF, Robertson K. The case for common reference intervals. Clin Biochem Rev 2004;25:99–104. [PMC free article] [PubMed] [Google Scholar]