

Abstract
We describe an unusual case of a primary evacuated blood collection tube with floating separator gel, which has been collected from a 50‐year‐old man submitted to a percutaneous coronary intervention (PCI). The sample was collected from the femoral artery in a primary evacuated blood collection tube containing lithium‐heparin. After centrifugation of the specimen, an unusual positioning of the separator gel was observed, which migrated at the topmost layer, whereas the packed blood cells remained in the middle and the plasma at the bottom. The potential interfering substance was found to be a contrast dye, 140 ml of which were administered to the patient during a revascularization procedure for acute myocardial infarction. The potential aspiration of the gel inappropriately positioned at the top of the tube by laboratory instrumentation can produce several technical and clinical problems, when not reliably detected. First, the needle of the instrument might be partially or completely obstructed by the gel, thus jeopardizing the integrity and correct functioning of the instrument. The aspiration of gel along with the sample matrix might also spuriously modify the test results, since an inappropriate amount of serum or plasma would be analyzed. J. Clin. Lab. Anal. 26:246‐247, 2012. © 2012 Wiley Periodicals, Inc.
Keywords: blood collection tube, contrast dye, separator gel
We describe an unusual case of a primary evacuated blood collection tube with floating of the separator gel. The sample was collected from a 50‐year‐old man submitted to a percutaneous coronary intervention (PCI). The patient was admitted directly to the cardiologic catheterization laboratory from the emergency department because of an acute coronary syndrome (anterior myocardial infarction with elevation of the ST tract on electrodiagram, STEMI: ST evaluation myocardial infarction). The angiogram showed the presence of an occluded left anterior descending coronary artery at its middle level, which was treated with thrombus aspiration and stent positioning (bare metal stent 3 × 22 mm, Integrity, Medtronic, Minneapolis MN). At the end of the procedure, a blood sample was drawn from the femoral artery through the arterial sheath. The arterial blood sample was collected into siliconized vacuum tubes containing lithium heparin and separator gel (Venosafe, Terumo Europe N.V, Leuven, Belgium), and shipped to the core laboratory immediately after angioplasty for routine control of biochemical parameters (i.e., sodium, potassium, creatinine, and glucose). The specimen arrived at the laboratory within 20 min from collection and was immediately centrifuged at room temperature at 1,500 × g for 10 min.
The separator gel is widely used in primary blood collection tube, since it acts as a barrier between serum and clot, or plasma and the cell pellet after centrifugation. In fact, after centrifugation of primary collection tube according to the manufacturer's instructions, the plasma forms the topmost layer, whereas the separator gel creates a reliable barrier from the corpuscular part of the blood (i.e., white blood cells, platelets, and red blood cells) to prevent the direct contact of plasma and cells, and thereby prevents the traffic of molecules and proteins released from the cells into the lower layer to the plasma in the upper part of the tube.
Since the specific gravities of serum and plasma typically span from 1.026 to 1.031 g/cm3, and that of the clot from 1.092 to 1.095 g/cm3, the specific gravity of the separator gel should be in the range between 1.03 and 1.09 g/cm3 to permit its suitable positioning after centrifugation 1. In this case report, we observed an unusual collocation of the separator gel, which migrated at the topmost layer whereas the packed blood cells remained in the middle and the plasma at the bottom (Fig. 1). This atypical separation was consistent with the hypothesis of an abnormally high specific gravity of the patient's plasma. The sample, which had no evidence of hemolysis, icterus, or lipemia, could not be processed because it was obviously considered as unsuitable by the lab technicians. A second sample was immediately referred from the Department of Cardiology, and the presence of an interference was suspected because there was no evidence of hyperproteinemia after measurement of total protein (i.e., 74 mg/L, assessed on Synchron LXi 725, Beckman Coulter, Fullerton, CA). The potential interfering substance was identified in a tri‐iodinated nonionic water‐soluble contrast dye, 140 ml of which were administered to the patient (Iomeron® 350 mg/ml, Bracco, Milan, Italy) shortly before the coronary revascularization procedure.
Figure 1.
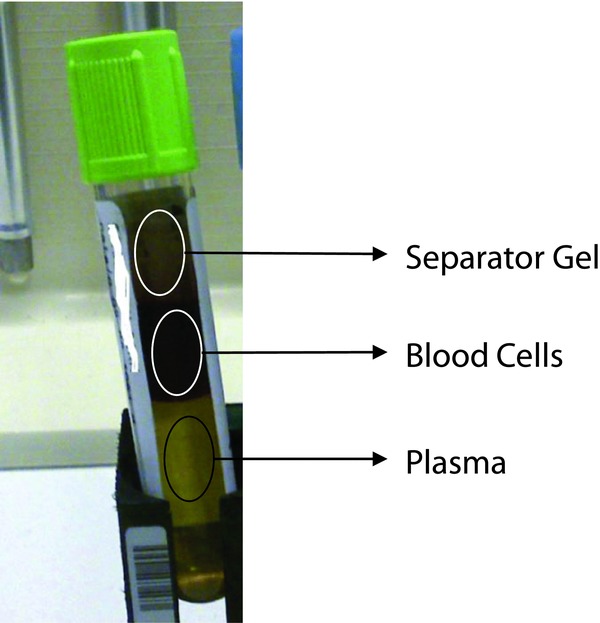
Inappropriate positioning of the separator gel in a primary lithium heparin blood collection tube. The gel represents the upper layer in the tube, the blood cells lie in the middle, and the plasma at the bottom.
Furthermore, we checked the behavior of this colorless contrast medium in the collection tube routinely used in our laboratory the same type used for the patient. One collection tube was filled with the contrast dye alone and a second tube was filled with 1 ml of dye and 3 ml of discarded venous blood. After the centrifugation performed at room temperature at 1,500 × g for 10 min, we observed the typical floating gel in both tubes.
The aspiration of gel not appropriately positioned in the tube by the sample needle of laboratory instrumentation might occur, especially in clinical laboratories with a high degree of preanalytical and analytical automation, where primary collection tubes might be centrifuged and analyzed without direct visual inspection by the laboratory personnel. Faught et al. recently observed remarkable differences in the specific gravity of separator gels contained in blood collection tubes from different manufacturers, with a consequent difference in the frequency of gel flotation events 2. The aspiration of the gel by laboratory instrumentation can be the cause of several technical and clinical problems, when not reliably detected. The needle of the instrument might be partially or completely obstructed by the gel, thus jeopardizing the integrity and correct functioning of the instrument. The aspiration of gel along with the sample matrix might also spuriously modify the test results, since an inappropriate amount of serum or plasma would be analyzed. The causes which have been anecdotally implicated in an inappropriate gel barrier formation include the administration of radio contrast dye 3, as well as the presence of hyperproteinemia 4 or trisodium citrate solution 5 in the specimen. In these circumstances, the specific gravity of serum or plasma is considerably high, thus preventing the appropriate positioning of the gel in the primary tube, since the migration of the gel during centrifugation of the tube is mainly determined by the density rather than the viscosity of the sample matrix 6.
REFERENCES
- 1. Bowen RAR, Hortin GL, Csako G, Otanez OH, Remaley At. Impact of blood collection devices on clinical chemistry assays. (Review) Clin Biochem 2010;43:4–25. [DOI] [PubMed] [Google Scholar]
- 2. Faugth RC, Marshall J, Bornhorst J. Solution densities and estimated protein contents associated with inappropriate flotation of separator gel in different blood collection tubes. Arch Pathol Lab Med 2011;135:1081–1084. [DOI] [PubMed] [Google Scholar]
- 3. Spiritus T, Zaman Z, Desmet W. Iodinated contrast media interfere with gel barrier formation in plasma and serum separator tubes. Clin Chem 2003;49:1187–1189. [DOI] [PubMed] [Google Scholar]
- 4. Van den Ouweland JMW, Church S. High total protein impairs appropriate gel barrier formation in BD Vacutainer blood collection tubes. Clin Chem 2007;53:364–5. [DOI] [PubMed] [Google Scholar]
- 5. Srivastava R, Murphy MJ, Card J, Severn A, Frase CG. The case of floating gel. J Clin Pathol 2004;57:1333–1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Fatàs M, Franquelo P, Franquelo R. Anomalous floation of separator gel: Density or viscosity? Clin Chem 2008;54:771–772. [DOI] [PubMed] [Google Scholar]