

Abstract
Purpose
Elbow fractures are common in children and occur during daily activities. The aim of this study is to evaluate the epidemiology of paediatric elbow fractures over a two-year period in Okinawa, a southern subtropical island in Japan.
Methods
This was a retrospective study of 488 elbow fractures in children younger than 15 years old treated at 11 hospitals in Okinawa. Data included age, gender, calendar month, type of fracture, operation rate, mechanism of injury, and aetiology.
Results
The most frequent age was 6 years old, with 47.5% of all elbow fractures occurring in an age range from 6 to 10 years old. The fracture rate for boys was 1.6 times higher than that for girls. The incidence was the highest in May (56 fractures) and the lowest in August (25 fractures). Supracondylar fractures were the most common type (44%), followed by lateral condyle fractures (22%); 45% of all fractures were treated operatively. Medial epicondyle fractures had the highest rate of operative treatment (91%). In the 6 to 10-year-old group, 19% of all fractures occurred while skateboarding or caster-boarding, the most frequent aetiology.
Conclusions
Supracondylar fractures are the most common fracture type in 4 to 7-year-old boys. In the 6 to 10-year-old group, skateboarding and caster-boarding are the most frequent and increasing cause of elbow fractures. Therefore, some preventive measures are needed.
Level of evidence
Level IV, case series
Keywords: elbow fracture, epidemiology, paediatrics, skateboard, caster-board
Introduction
Elbow fractures are common in paediatric populations.1,2 Hussain et al3 reported that 28.4% of all paediatric fractures were elbow fractures, which were the most common type of fractures in India in 2015. The overall incidence of elbow fractures was reported at 30.8/10000 per year.4 Elbow fractures are rarely life-threatening, but may have serious complications, including neurovascular injuries, cubitus varus deformities, and Volkmann’s contractures in supracondylar fractures; nonunion, valgus deformities, and late ulnar nerve palsies in lateral condyle fractures. Understanding common aetiologies is the first step in formulating preventive measures. Paediatric elbow fractures occur during daily life including participation in popular sports and leisure activities. Determining current aetiology is important because children’s activities may differ drastically in different countries, and may change considerably within a short period even in the same country. Okinawa is a southerly subtropical Japanese island which constitutes approximately 1% of the area and population of Japan. Therefore, paediatric elbow fractures in Okinawa may have some unique characteristics and distributions. The aim of this cross-sectional study was to survey regional epidemiologic features of paediatric elbow fractures in Okinawa over a two-year period.
Methods
This retrospective multi-centre study was approved by our institutional review board. The informed consents were disclosed as an opt-out consent process. All elbow fractures in children under 15 years old presenting to emergency departments or orthopaedic outpatient departments at 11 hospitals in Okinawa in the period from 1 January 2015 to 31 December 2016 were included. The population of Okinawa during this study period was about 1,440,000, of whom 275,000 (19%) were children under 15 years old. Exclusion criteria were as follows: pathological fractures, fractures at birth, stress fractures, re-fractures within six months and patients of complete growth plate closure. A total of three patients were excluded (two pathological fractures; one re-fracture within six months). All hospitals had emergency and orthopaedic departments and two or more board-certified orthopaedic surgeons of the Japanese Orthopaedic Association. All hospitals were equipped to perform emergency operations, and paediatric general anaesthesia was available in 10 of the 11 hospitals.
Age at time of injury, gender, calendar month of injury, type of fracture (open/closed, single/combined, and unilateral/bilateral), rate of surgery, fracture mechanism, and aetiology of injury were obtained from records and radiographs. All radiographs were carefully reviewed by two board-certified hand surgeons of the Japanese Society for Surgery of the Hand.
We classified the fracture mechanisms into six categories as follows: tumble, tumbled on outstretched elbow at ground level; fall, fall on outstretched elbow from above ground level; lateral bend, bent the elbow during sports or accidents; direct hit, smashed by an object or the elbow got caught in the door; throw, injured after throwing a ball or other object, and unknown. The aetiologies were categorized by the activity or location of the injuries (e.g. tumble while playing football/skateboarding, fall from chair/bed, or lateral bend during Judo). Subjects were classified into three age subgroups: 0 to 5 years, 6 to 10 years, and 11 to 15 years old.
In more common types of fractures, including supracondylar fractures, lateral condyle fractures, and medial epicondyle fractures, classification (Gartland classification in supracondylar fractures, Wadsworth classification in lateral condyle fractures, Watson-Jones classification in medial epicondyle fractures), and operation rates were extracted.
Results
There were 488 elbow fractures, of which 195 (40%) were on the right side, 293 (60%) on the left side, and none were bilateral. Nine combination fractures (1.8%) are summarized in Table 1. The most common combination was supracondylar fracture with distal radius (and ulna) fracture in six cases, and the remainder were unique with one case each. The age and gender distributions of paediatric elbow fractures are shown in Fig. 1. There were 310 boys (63.5%) and 178 girls (36.5%), making the fracture rate of boys 1.6 times higher than that of girls. The most frequent age was 6 years old, with 47.5% of all fractures occurring in children between 6 and 10 years old (Fig. 1a, Fig. 1b). The calendar-month fracture distribution is shown in Fig. 2. The number of elbow fractures was the highest in May (56) and the lowest in August (25). The six summer months (April–September) had 246 fractures and the six winter months (October–March) had 243. In Japan, the school year begins on 1 April and ends on 31 March. And the average temperature of the first six months (April–September) is higher than that of the last six months (October–March). So we classified the first six months as summer months and the last six months as winter months. This classification has also been used in a previous study.5
Table 1.
Combinations of fractures
| Elbow fractures | Combined fracture | Number |
|---|---|---|
| Supracondylar | Distal radius (and ulna) | 6 |
| Forearm shaft | 1 | |
| Rt. lateral condyle | Lt. distal radius | 1 |
| Rt. proximal radius | Lt. distal radius | 1 |
Fig. 1a.

Age and gender distributions; per year.
Fig. 1b.

Age and gender distributions; age subgroup.
Fig. 2.
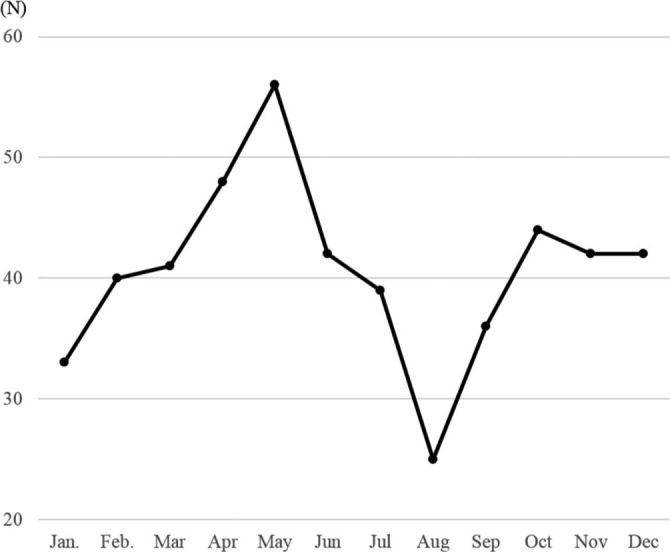
Calendar-month distribution of elbow fractures.
Type and number of fractures, and number requiring surgery are summarized in Tables 2 and 3. Supracondylar fractures were the most common type (43.8%), followed by lateral condyle fractures (22.3%); 44.1% of all elbow fractures were treated operatively. Medial epicondyle fracture was the most commonly operated (85.7%), and olecranon fracture was the least (10.2%). Open fractures comprised only four cases (0.8%) and all of these were Monteggia fractures.
Table 2.
Fracture type, number of patients, number requiring surgery
| Type of fracture | Number of patients (%) | Number requiring surgery (%) |
|---|---|---|
| Supracondylar | 214 (43.8) | 89 (41.6) |
| Lateral condyle | 109 (22.3) | 53 (48.6) |
| Olecranon | 49 (10.0) | 5 (10.2) |
| Medial epicondyle | 35 (7.2) | 30 (85.7) |
| Proximal radius | 26 (5.3) 25 radial neck; 1 radial head | 12 (46.2) |
| Monteggia | 23 (4.7) | 14 (60.9) |
| Others | 32 (6.6) | 12 (37.5) |
| Total | 488 (100) | 215 (44.1) |
Table 3.
Fracture type, number of patients in each age subgroup
| Type of fracture | Number of patients in age subgroup (%) | Total | ||
|---|---|---|---|---|
| 0 to 5 years | 6 to 10 years | 11 to 15 years | ||
| Supracondylar | 101 (47.1) | 101 (47.1) | 12 (5.6) | 214 |
| Lateral condyle | 47 (43.1) | 54 (49.5) | 8 (7.3) | 109 |
| Olecranon | 22 (44.9) | 20 (40.8) | 7 (14.3) | 49 |
| Medial epicondyle | 0 (0.0) | 15 (42.9) | 20 (57.1) | 35 |
| Proximal radius | 4 (15.4) | 14 (53.8) | 8 (30.8) | 26 |
| Monteggia | 9 (39.1) | 14 (60.9) | 0 (0.0) | 23 |
Fracture mechanisms are summarized in Table 4. Fall was the most common cause of injury (242 fractures, 49.6%). In the 0 to 5 years subgroup, fall (123 fractures) was the most frequent, and tumble for the 6 to 10 year subgroup (126 fractures). The major aetiology of falls in 0 to 5 year olds were indoor falls (from a chair in 18 cases, a sofa in 11, and a bed in 6). In contrast, falls in 6 to 10 year olds were more often outdoor falls (from playground equipment in 14 cases, trees in 11, iron rod in 11, and aerial ladder in 10). The most frequent aetiology in 6 to 10 year olds was injury while skateboarding or caster-boarding (44 fractures, 19%). In 6 to 10 year olds, elbow fractures while skateboarding and caster-boarding were 4.9 times more common than those during bicycle injuries, the second most common aetiology.
Table 4.
Fracture mechanisms
| Age group (years old) | Tumble | Fall | Lateral bend | Direct hit | Throw | Unknown |
|---|---|---|---|---|---|---|
| 0 to 5 | 55 | 123 | 4 | 5 | 0 | 9 |
| 6 to 10 | 126 | 101 | 1 | 2 | 1 | 1 |
| 11 to 15 | 33 | 18 | 4 | 4 | 1 | 0 |
| Total | 214 | 242 | 9 | 11 | 2 | 10 |
Note. Tumble, tumbled on outstretched elbow at ground level. Fall, fall on outstretched elbow from above ground level. Lateral bend, bent the elbow during sports or accidents. Direct hit, smashed by an object or the elbow got caught in the door. Throw, injured after throwing a ball or other object.
Operation ratios of Gartland grade I, II, and III of supracondylar fracture were 0.0%, 50.5%, and 100.0%, respectively (Table 5). The ratios of Wadsworth grade I, II, III of lateral condyle fracture were 12.0%, 76.7%, and 100.0%, respectively (Table 6). The ratios of Watson-Jones grade I, II, III, IV of medial epicondyle fracture were 81.8%, 94.1%, 100.0%, and 100.0%, respectively (Table 7).
Table 5.
Gartland classification of supracondylar fractures, number of patients, and number requiring surgery
| Gartland classification | Number of patients | Number requiring surgery (%) |
|---|---|---|
| I | 70 | 0 (0.0) |
| II | 109 | 55 (50.5) |
| III | 35 | 34 (100.0)* |
| Total | 214 | 89 (41.6) |
One case transferred to another hospital.
Table 6.
Wadsworth classification of lateral condyle fractures, number of patients, and number requiring surgery
| Wadsworth classification | Number of patients | Number requiring surgery (%) |
|---|---|---|
| I | 57 | 12 (21.1) |
| II | 44 | 33 (76.7)* |
| III | 9 | 8 (100.0)* |
| Total | 110 | (48.6) |
One case transferred to another hospital
Table 7.
Watson-Jones classification of medial epicondyle fractures, number of patients, number requiring surgery
| Watson-Jones classification | Number of patients | Number requiring surgery (%) |
|---|---|---|
| I | 11 | 9 (81.8) |
| II | 18 | 16 (94.1)* |
| III | 2 | 2 (100.0) |
| IV | 4 | 3 (100.0)* |
| Total | 35 | (85.7) |
One case transferred to another hospital
Discussion
This study is the first epidemiological study of paediatric elbow fractures in Okinawa and provided some unique information about such fractures’ characteristics and aetiologies. The peak incidence of elbow fractures was at 6 years old, with the majority (47.5%) occurring in children in range from 6 to 10 years old, as has been noted in previous studies.4,6,7 The male:female ratio was 1.6:1.0 in our study, which was also similar to that in previous studies.6,7 Elbow fractures more commonly occur on the non-dominant side. This is likely because the dominant upper extremity is in use, and the non-dominant assumes the protective role during injury. Approximately 90% of Japanese people are right-handed. In our study, 40% of fractures were on the right side and 60% on the left, again similar to previous studies.4,7 General frequencies by age, gender, and fracture side were similar to earlier elbow fracture research findings, even in other countries or other generations (Table 8).
Table 8.
Comparison of previous and current studies
| Highest frequent age or age group (years old) | Male/female | Right/left | Calendar month | ||
|---|---|---|---|---|---|
| Highest | Lowest | ||||
| Landin AL, et al6 | 6 | 1.6 | 0.7 | Jul. | Jan. |
| Houshian S, et al4 | 5 | 0.9 | 0.7 | Aug. | Dec. |
| Behdad A, et al7 | 4 to 8 | 2.6 | 0.7* | – | – |
| Current study | 6 | 1.7 | 0.7 | May | Aug. |
Analysis of supracondylar, radius head, lateral condyle, radius neck, and olecranon fractures.
Some authors have reported that elbow fracture incidence rates were higher in the summer and lower in the winter in Denmark4 and Sweden.6 Khoshbin et al5 reported supracondylar fracture incidence in summer months (April–September) was 2.7 times greater than in winter months (October–March) from 2002 to 2010 in a population-based study in Canada. Some authors have attributed the increased incidence of elbow fractures during the summer to greater involvement in outdoor activities, or to the fact that many children leave the city during summer holidays.5,6 Masterson et al8 reported a positive correlation between sunshine hours and monthly fracture rates, with the prevalence of fractures in the summer being 2.5 times greater. In the current study, elbow fractures in August (25 fractures) were the lowest, and fractures in the summer months were almost equal to those in the winter months (246 versus 243). Okinawa is a southern subtropical island and the climate is warm. In 2015, the lowest average temperature in Okinawa was 17.0°C in January, and the highest was 28.9°C in August. And the average temperature of summer months is 6.7°C higher than that of winter months (27.5 vs. 20.5°C). Children are able to participate in outdoor activities throughout the year, due to the warm climate and lack of snow. We consider it likely that the elbow fracture incidence in summer in our study is low compared with that in the etiological studies of Sweden,6 Denmark,4 and Canada5 because of the warm climate throughout the year. And recently, the dangerousness of heat stroke has become well known. So children might avoid going outside when the temperature is so high. We consider avoidance of heat stroke is another reason for the decreasing incidence in August. However, we cannot attribute the pattern of seasonal variation only to temperature because there are many other factors influencing the fracture rate, including sunshine hours, culture, urban or rural location, summer holidays, and religious observances (Table 8).
Supracondylar fractures are the most common type of elbow fracture in children, with a reported incidence of 177.3/100,000 children.9 Among all elbow fractures, 55% to 58% were supracondylar fractures in previous studies.4,6,7 In the current study, the supracondylar fracture was the most common at 43.8%, followed by lateral condyle fracture at 22.3%. In previous studies, however, the second most frequent type was reported to be proximal radius fracture (radius neck and head) and the rates were reported to vary from 11% to 18%.4,6,7 In the current study, the rate of proximal radius fractures was only 5.3%, making it the fifth most common type of fracture. In contrast, the frequency of lateral condyle fracture was reported at 9% to 12% in previous studies,4,6,7 much lower than that in current study (22.3%). Looking at only Japanese articles and textbooks, however, lateral condyle fracture is the second most common type of fracture, followed by supracondylar fracture. Kang and Park10 reported the majority of cases with an injury mechanism of hyperextension with valgus stress caused proximal radius fractures, while hyperextension with varus stress caused lateral condyle fractures. They also reported that a more anatomically valgus-deviated elbow predisposed individuals to radial neck fracture, while a more varus-deviated elbow predisposed them to lateral condyle fracture. In other words, the carrying angle in elbows with radial neck fractures was significantly greater than that in elbows with lateral condyle fractures.10 In Japanese children, the elbow alignment may be more varus-deviated than in children of other nationalities or ethnicities. However, to our knowledge, there is no English-language scientific article describing differences in elbow alignment between national or ethnic groups.
In this study, injuries while skateboarding or caster-boarding were the most common cause of elbow fractures in 6 to 10 year olds (19%, 44/232 cases). A caster-board is a two-wheeled vehicle that resembles a skateboard. It has two narrow platforms joined by a bar, and one caster with a wheel is mounted to each platform. It moves forward when a rider stands with one foot on each platform and twists, as opposed to skateboards, which are moved by pushing with the rider’s feet on the ground. It was awarded ‘2008 Toy of the Year’ in the United States and released in November 2008 in Japan. It is more popular for primary-school children than skateboarding. It may be that more elbow fractures while skateboarding or caster-boarding occurred in Okinawa because the children can ride the boards throughout a year due to the warm climate without snow. These board activities may help train children’s sense of balance. However, board injuries were the most common elbow fracture aetiology in 6 to 10 year olds, so preventive measures (such as wearing protective elbow pads or e-learning a lecture how to ride and prevent injuries) to reduce elbow fracture while skateboarding or caster-boarding in this age group should be encouraged.
In this study, the operation rate of medial epicondyle fractures was the highest (85.7%). In medial epicondyle fracture, absolute indications for operative treatment are limited to open fractures and non-reducible incarcerated fracture fragments. Relative indications include ulnar nerve dysfunction, elbow instability, high-level upper extremity athletic participation, and displaced fractures.11 Farsetti et al12 have reported that nonsurgical management of displaced (5–15 mm) medial epicondyle fractures yields results similar to those of surgery, even when bone union is not achieved. When this fracture occurs, the capsular ligaments and anteromedial muscular structures can be damaged. Several studies have noted that injury to these medial stabilizing structures, far more than fragment displacement, can influence joint stability and eventual outcomes.13,14 Lee et al15 reported that more than 60% of patients have radiographic nonunion that commonly causes elbow stiffness and may cause valgus instability. Louahem et al14 recommend surgical intervention for such fractures, with anatomic reduction to achieve solid bone union and thus prevent valgus instability. Stepanovich et al16 reported in their prospective study that operative management resulted in higher rates of both fracture union and return to sport. These recent recommendations may have contributed to the high rate of operative intervention for medial epicondyle fractures in our study.
There was a limitation in this study that the fractures in the study population may be atypically severe because the children in this study were those who presented to hospitals with emergency departments. Some children, with no or minor displaced elbow fracture, went to orthopaedic clinics.
In conclusion, frequencies by age, gender, and fracture side for elbow fractures in Okinawa were similar to those in previous studies, even in other countries or other generations. Low frequency rates of elbow fractures in summer may be unique to Okinawa. Higher rates of lateral condyle fracture may be unique to Japan. Nineteen percent of all elbow fractures in 6 to 10 year olds during our study period were sustained while skateboarding or caster-boarding; therefore, use of protective equipment during these activities should be encouraged.
Open access
This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) licence (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.
Compliance with ethical standards
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical statement
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Institutional review board approval was obtained from our hospital for this retrospective multi-centre study.
Informed consent: Not required for this retrospective study.
ICMJE Conflict of interest statement
None declared.
Acknowledgements
We thank Rina Arasaki, Tomota Gima, Takashi Toma, Tadakatsu Kinjo, Norihiro Kawagoe, Hirota Kohama, Yoshiyuki Akamine, Hiroaki Komesu, Kenji Horikiri, Tomohiro Isa, Wataru Oshiro, Goichi Okahara, Manabu Tokeshi, Hideyuki Sunagawa, and Tomohiro Moriyama for their contributions to our data collection.
Author Contributions
HO: Study conception, Data collection, Data analysis, Manuscript preparation.
MN: Study conception, Data analysis, Manuscript preparation.
MK: Data collection, Data analysis.
KO: Data collection, Data analysis.
CF: Data collection, Data analysis.
FK: Study conception, Manuscript preparation.
References
- 1.Tandon T, Shaik M, Modi N. Paediatric trauma epidemiology in an urban scenario in India. J Orthop Surg (Hong Kong) 2007;15:41–45. [DOI] [PubMed] [Google Scholar]
- 2.Issin A, Kockara N, Oner A, Sahin V. Epidemiologic properties of pediatric fractures in a metropolitan area of Turkey. Medicine (Baltimore) 2015;94:e1877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hussain S, Dar T, Beigh AQ, et al. Pattern and epidemiology of pediatric musculoskeletal injuries in Kashmir valley, a retrospective single-center study of 1467 patients. J Pediatr Orthop B 2015;24:230–237. [DOI] [PubMed] [Google Scholar]
- 4.Houshian S, Mehdi B, Larsen MS. The epidemiology of elbow fracture in children: analysis of 355 fractures, with special reference to supracondylar humerus fractures. J Orthop Sci 2001;6:312–315. [DOI] [PubMed] [Google Scholar]
- 5.Khoshbin A, Leroux T, Wasserstein D, et al. The epidemiology of paediatric supracondylar fracture fixation: a population-based study. Injury 2014;45:701–708. [DOI] [PubMed] [Google Scholar]
- 6.Landin LA, Danielsson LG. Elbow fractures in children: an epidemiological analysis of 589 cases. Acta Orthop Scand 1986;57:309–312. [DOI] [PubMed] [Google Scholar]
- 7.Behdad A, Behdad S, Hosseinpour M. Pediatric elbow fractures in a major trauma center in Iran. Arch Trauma Res 2013;1:172–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Masterson E, Borton D, O’Brien T. Victims of our climate. Injury 1993;24:247–248. [DOI] [PubMed] [Google Scholar]
- 9.Mulpuri K, Hosalkar H, Howard A. AAOS clinical practice guideline: the treatment of pediatric supracondylar humerus fractures. J Am Acad Orthop Surg 2012;20:328–330. [DOI] [PubMed] [Google Scholar]
- 10.Kang S, Park SS. Predisposing effect of elbow alignment on the elbow fracture type in children. J Orthop Trauma 2015;29:e253–e258. [DOI] [PubMed] [Google Scholar]
- 11.Gottschalk HP, Eisner E, Hosalkar HS. Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg 2012;20:223–232. [DOI] [PubMed] [Google Scholar]
- 12.Farsetti P, Potenza V, Caterini R, Ippolito E. Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299–1305. [DOI] [PubMed] [Google Scholar]
- 13.Schwab GH, Bennett JB, Woods GW, Tullos HS. Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop Relat Res 1980;146:42–52. [PubMed] [Google Scholar]
- 14.Louahem DM, Bourelle S, Buscayret F, et al. Displaced medial epicondyle fractures of the humerus: surgical treatment and results. A report of 139 cases. Arch Orthop Trauma Surg 2010;130:649–655. [DOI] [PubMed] [Google Scholar]
- 15.Lee HH, Shen HC, Chang JH, Lee CH, Wu SS. Operative treatment of displaced medial epicondyle fractures in children and adolescents. J Shoulder Elbow Surg 2005;14:178–185. [DOI] [PubMed] [Google Scholar]
- 16.Stepanovich M, Bastrom TP, Munch J III, Roocroft JH, Edmonds EW, Pennock AT. Does operative fixation affect outcomes of displaced medial epicondyle fractures? J Child Orthop 2016;10:413–419. [DOI] [PMC free article] [PubMed] [Google Scholar]