

Abstract
Objective
Sphingolipids, including sphingosine-1-phosphate (S1P) and ceramides, have been associated with vascular tone, blood pressure regulation, cardiovascular outcomes and mortality. However, the relationship between plasma sphingolipids and cerebrovascular disease has not been examined. We aimed to assess the cross-sectional association between plasma sphingolipids and white matter hyperintensity (WMH) volume, which is a marker of cerebrovascular disease.
Approach and Results
We included 588 participants (302 men and 286 women), aged 60–93, enrolled in the population-based Mayo Clinic Study of Aging who had MRI and plasma sphingolipids at the same study visit. Fasting plasma was obtained and ceramides and S1P were assayed using liquid chromatography electrospray ionization tandem mass spectrometry. Fluid-attenuated inversion recovery (FLAIR) was used to measure WMH volume, defined as percent total intracranial volume. We used linear regression to cross-sectionally examine the relationships between plasma sphingolipids and WMH; both were log-transformed. In multivariable analyses adjusting for age, sex, and hypertension, higher levels of ceramide C16:0 (b(95% confidence interval [CI]) = 0.24(0.02, 0.45) and the ceramide ratios C16:0_24:0 (b(95% CI) = 0.30(0.12, 0.48)) and C24:1_24:0 (b(95% CI) = 0.24(0.07, 0.41)) were associated with a higher WMH volume. A higher ceramide score was also associated with higher WMH volume (b(se) = 0.03 (0.01, 0.04)). We did not observe any association between S1P and WMH volume.
Conclusions
Higher plasma ceramide C16:0 and two specific ceramide ratios (C16:0_24:0 and C24:1_24:0) are associated with greater WMH volumes, independent of hypertension, suggesting their utility for measurement of cerebrovascular disease.
Keywords: ceramides, sphingolipids, white matter hyperintensity
Subject Codes: Lipids and Cholesterol, Biomarkers, Clinical Studies, Vascular Biology
Introduction
White matter hyperintensities (WMH), a primary marker of cerebrovascular disease,1 increase with age and are associated with a two-fold increased risk of dementia and a three-fold increased risk of stroke.1,2 The etiology and pathophysiology of WMH are not completely understood but are thought to be related to ischemic, hypoxic, and neurodegenerative processes.3–5 A better understanding of the pathways and mechanisms contributing to WMH is needed to identify potential treatment targets.
Sphingolipids, which contribute to the structure of cell membranes and act as bioactive lipids for multiple cellular pathways, are increasingly being implicated in cardiovascular diseases.6 Ceramides are bioactive lipids that are pro-inflammatory, pro-apoptotic, and involved in cellular stress. In contrast, sphingosine-1-phosphate (S1P), a metabolite of ceramide, induces proliferation in many cell types, including vascular cells, and attenuates the pro-apoptotic actions of ceramides. However, the exact role of S1P depends on the concentration and receptor; activation of S1P receptor 1 has been associated with vasodilation whereas activation of S1P receptor 3 has been associated with vascular constriction.7 Both ceramides and S1P have a role in regulating vascular tone, responses to hypoxia, and blood pressure.8,9
Recent studies suggest that, among individuals with existing vascular disease, elevated levels of plasma ceramides or S1P are associated with subsequent cardiovascular events, stroke, and death.10–15 Over the course of these studies, the following ceramides and ceramide ratios were most strongly associated with risk of cardiovascular events: Cer(d18:1/16:0), Cer(d18:1/18:0), Cer(d18:1/24:1), Cer(C16:0/24:0) ratio, Cer(C18:0/24:0) ratio, and Cer(C24:1/C24:0) ratio. Based on these ceramides and ceramide ratios, Laaksonen R, et al.13 developed a ceramide risk score that was found to be better for predicting subsequent cardiovascular events compared to the standard risk factors (e.g., lipids). However, the association between these ceramides and WMH is not known. Therefore, the aim of the current study was to examine the relationship between plasma ceramides and S1P with WMH volume in a population-based study of aging and cognition. Although we hypothesized that the same ceramides and ceramides ratios found to be associated with cardiovascular events would also be most strongly associated with WMH, we examined all individual ceramides and S1P because the association between these lipids and WMH had not previously been examined. Thus, assessing all lipids would allow us to confirm whether the same ceramides and ceramide ratios were most associated with WMH or whether additional ceramides or S1P were also important. Because hypertension is one of the major risk factors for WMH, we also determined whether the associations were independent of hypertension. In addition, both WMH volume and ceramide levels have been shown to be higher in women after menopause compared to men.28,29 Therefore, in additional analyses we determined whether the relationship between ceramides and S1P interacted with sex in relation to WMH volume.
Materials and Methods
Data Sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study Design and Participants
All participants were enrolled in the Mayo Clinic Study of Aging (MCSA), a population-based study of Olmsted County, Minnesota residents.16 The Olmsted County population was enumerated using the Rochester Epidemiology Project medical records-linkage system.17 Complete details of the MCSA study design have been previously described.16,18 MCSA clinical visits included an interview by a study coordinator, a neurological examination, neuropsychological testing, and a blood draw. All participants are invited to participate in a brain MRI; metal in the body (e.g., pacemaker) and claustrophobia are the only exclusionary criteria. About 70% of participants consent. Plasma sphingolipids were assayed on a randomly selected group of participants for another project. The current analysis included 588 participants, aged 60–92, who had MRI and plasma sphingolipids concurrently measured at the same study visit between August, 2008 and March, 2015. Compared to the overall MCSA cohort, individuals with a MRI were significantly younger and healthier (defined as less comorbidities, including hypertension) compared to those without a MRI. The study was approved by Mayo Clinic and Olmsted Medical Center Institutional Review Boards. Written informed consent was obtained from all participants.
Sphingolipid Analyses
During the in-clinic exam, participants’ blood (serum and EDTA plasma) was collected in the fasting state. The blood was centrifuged, aliquoted, and stored at −80°C. LC/ESI/MS/MS analysis of plasma sphingolipids was performed using an AB Sciex quadrupole mass spectrometer 6500 (Sciex, Framingham, MA) equipped with an ESI probe and interfaced with the Agilent 1290 infinity LC system (Agilent, Palo Alto, CA). The UPLC system consisted of an Agilent 1290 binary pump, thermostat, TCC, and sampler. The injection volume was 10 μL for extracted sample. Sphingolipids were separated with a Poroshell 120 EC- C8 column, 2.1×50 mm, 2.7 μm (Agilent, Palo Alto, CA). Mobile phase A was water:methanol:formic acid:ammonium formate (45/55/0.5%/5 mM by v/v). Mobile phase B was acetonitrile:methanol:formic acid:ammonium formate (50/50/0.5%/5 mM by v/v). The valve, sample loop, and needle were washed with acetonitrile:methanol (50/50 by v/v) for 20 sec. Mass spectrometric analyses were performed online using electrospray ionization tandem mass spectrometry in the positive mode.
Samples were prepared using Biomek FX (Beckman Coulter, Brea, CA). A small amount of plasma sample was added to a 2-mL 96-well plate. Internal standard mixture was added to the samples. Sphingolipids were extracted using 1 phase extraction with methanol-dichloromethane. Lipid levels were quantified by the ratio of analyte and internal standard and calibration curves obtained by serial dilution of a mixture of lipid standards. Pure synthetic standards of sphingolipids were purchased from Avanti Lipids. Isotope labeling synthetic standards were synthesized internally at Eli Lilly and Company. All sphingolipids were expressed in ng/ml.
Calculation of the Ceramide Ratios and Score
We utilized the ceramide ratios and calculated the ceramide score based on Laaksonen R, et al.13 Briefly, for each of three ceramides (16:0, 18:0, 24:1) and three ceramide ratios (C16:0/24:0, C18:0/24:0, C24:1/C24:0), individuals received 1 point for being in the third quartile of the whole study population and 2 points for being in the fourth quartile. Thus, the ceramide score ranged from 0–12.
Quantification of White Matter Hyperintensities
Structural magnetic resonance imaging (MRI) was acquired using standardized Magnetization Prepared – Rapid Gradient Echo (MPRAGE) sequences on 3T GE scanners (GE Medical Systems, Milwaukee, WI). WMH on standard 2-dimensional Fluid-attenuated inversion recovery (FLAIR) imaging were segmented and edited by a trained imaging analyst using a semi-automated method.19 WMH volume is presented as the percentage of total intracranial volume (TIV).
Covariates
Age and sex were determined at the in-person clinical examination. Medical conditions (eg, hypertension, diabetes) were determined for each participant by medical record abstraction using the REP medical records-linkage system, which is more accurate than self-report.17 Hypertension was defined as 1) systolic blood pressure ≥ 140 mmHg or diastolic ≥ 90 mmHg on two occasions, or 2) treatment for hypertension. We did not adjust for diabetes, dyslipidemia, smoking and obesity because we previously determined that these factors were not associated with WMH volume in the MCSA.28
Statistical Analyses
Both the plasma sphingolipids and WMH volume were log-transformed. Linear regression models were run using the plasma sphingolipids to predict WMH volume as a continuous variable. Assumptions of linear regression were checked by examining plots of the residuals versus fitted values and also QQ plots of the residuals; the assumptions were met. Multivariable models adjusted for age, sex, and hypertension. In additional analyses, we examined whether an interaction with sex existed by adding an interaction term in the linear regression model consisting of the plasma sphingolipid and sex. Statistical analysis was completed using SAS, version 9.4 (SAS Institute Inc., Cary, NC). A P value of <0.05 was considered to represent statistical significance.
Results
The clinical characteristics of the 588 participants are shown in Table 1. The median (interquartile range [IQR]) age was 68.0 (64.2, 71.9) years and 302 (51.4%) were men. The median (IQR) WMH volume, as a percent of the TIV, was 0.005 (0.003, 0.010) and all participants had some degree of WMH. There were 335 (57.0%) participants with a medical-record confirmed diagnosis of hypertension.
Table 1.
Baseline Characteristics, Plasma Lipid Levels and WMH Volume (N=588)
| Characteristics | Median (IQR)/N(%) |
|---|---|
| General Information | |
| Age | 68.0 (64.2, 71.9) |
| Male | 302 (51.4%) |
| Hypertension | 335 (57.0%) |
| WMH volume (% TIV) | 0.005 (0.003, 0.010) |
| Plasma lipid levels, ng/ml | |
| Sphingosine-1-phosphate | 223.1 (185.8, 265.1) |
| Ceramides, ng/ml | |
| C14:0 | 9.0 (6.8, 12.5) |
| C16:0 | 88.8 (74.3, 105.3) |
| C18:0 | 78.1 (59.4, 98.3) |
| C18:1 | 2.3 (1.4, 3.6) |
| C20:0 | 226.1 (190.7, 274.9) |
| C22:0 | 701.9 (574.1, 859.8) |
| C23:0 | 418.7 (344.0, 505.9) |
| C24:0 | 1214.8 (993.8, 1461.8) |
| C24:1 | 314.8 (257.1, 376.0) |
| Ceramide ratios | |
| C16:0_24:0 | 0.07 (0.06, 0.09) |
| C18:0_24:0 | 0.06 (0.05, 0.08) |
| C24:1_24:0 | 0.26 (0.21, 0.32) |
| Ceramide score | 4.0 (2.0, 7.0) |
IQR, Interquartile range; WMH, white matter hyperintensity; TIV, Total intracranial volume. WMH is expressed as the percent of the total intracranial volume.
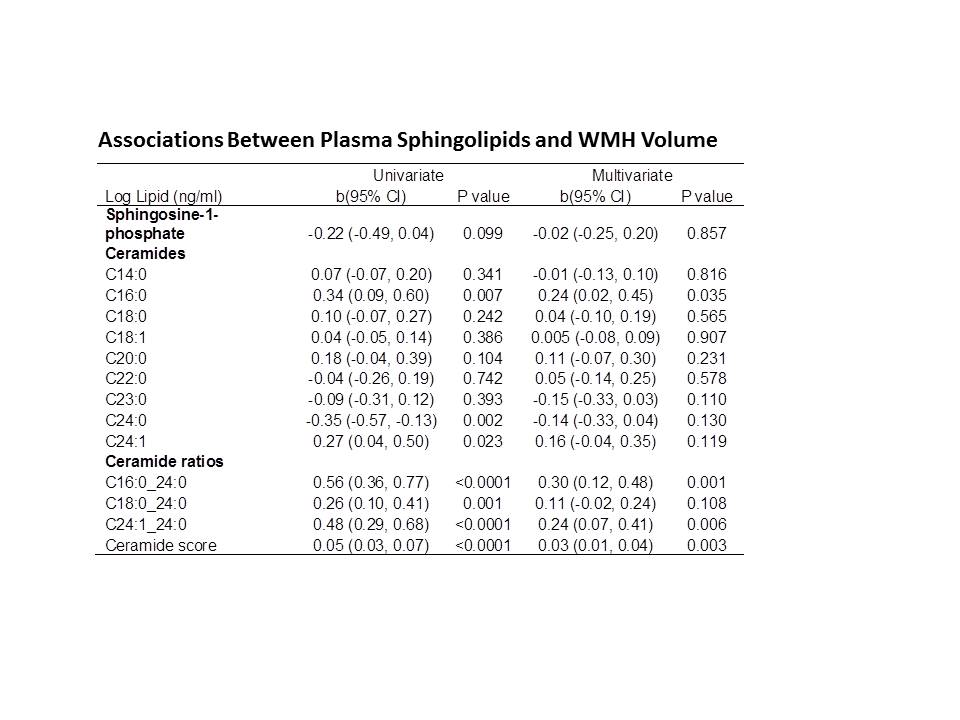
Table 2 provides the univariable and multivariable models for associations between the plasma sphingolipids (in ng/ml) or ratios with WMH volume as a percent of TIV. In multivariable analyses adjusting for age, sex, and hypertension, higher ceramide C16:0 (b(95% confidence interval [CI]) = 0.24(0.02, 0.45) and higher ceramide ratios C16:0_24:0 (b(95% CI) = 0.30(0.12, 0.48)) and C24:1_24:0 (b(95% CI) = 0.24(0.07, 0.41)) were associated with a greater WMH volume. Each one point higher in the ceramide score was also associated with higher WMH volume (b(se) = 0.03 (0.01, 0.04)). We did not observe any association between S1P and WMH volume. Hypertension was the variable associated with the greatest attenuation of significance between the univariable and multivariable models.
Table 2.
Associations Between Plasma Sphingolipids and WMH Volume
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Log Lipid (ng/ml) | b(95% CI) | P value | b(95% CI) | P value |
| Sphingosine-1-phosphate | −0.22 (−0.49, 0.04) | 0.099 | −0.02 (−0.25, 0.20) | 0.857 |
| Ceramides | ||||
| C14:0 | 0.07 (−0.07, 0.20) | 0.341 | −0.01 (−0.13, 0.10) | 0.816 |
| C16:0 | 0.34 (0.09, 0.60) | 0.007 | 0.24 (0.02, 0.45) | 0.035 |
| C18:0 | 0.10 (−0.07, 0.27) | 0.242 | 0.04 (−0.10, 0.19) | 0.565 |
| C18:1 | 0.04 (−0.05, 0.14) | 0.386 | 0.005 (−0.08, 0.09) | 0.907 |
| C20:0 | 0.18 (−0.04, 0.39) | 0.104 | 0.11 (−0.07, 0.30) | 0.231 |
| C22:0 | −0.04 (−0.26, 0.19) | 0.742 | 0.05 (−0.14, 0.25) | 0.578 |
| C23:0 | −0.09 (−0.31, 0.12) | 0.393 | −0.15 (−0.33, 0.03) | 0.110 |
| C24:0 | −0.35 (−0.57, -0.13) | 0.002 | −0.14 (−0.33, 0.04) | 0.130 |
| C24:1 | 0.27 (0.04, 0.50) | 0.023 | 0.16 (−0.04, 0.35) | 0.119 |
| Ceramide ratios | ||||
| C16:0_24:0 | 0.56 (0.36, 0.77) | <0.0001 | 0.30 (0.12, 0.48) | 0.001 |
| C18:0_24:0 | 0.26 (0.10, 0.41) | 0.001 | 0.11 (−0.02, 0.24) | 0.108 |
| C24:1_24:0 | 0.48 (0.29, 0.68) | <0.0001 | 0.24 (0.07, 0.41) | 0.006 |
| Ceramide score | 0.05 (0.03, 0.07) | <0.0001 | 0.03 (0.01, 0.04) | 0.003 |
WMH, white matter hyperintensity; CI, confidence interval. Multivariate models adjust for age, sex, and hypertension. WMH is defined as the percent of total intracranial volume.
We further determined whether there was an interaction between the plasma sphingolipids and sex for WMH volume. However, there were no significant interaction terms.
Discussion
Although plasma ceramides and S1P have been associated with cardiovascular disease outcomes, the relationship between these plasma sphingolipids and WMH volume has not been examined. In this population-based sample, higher ceramide ratios of C16:0/C24:0 and C24:1/C24:0 and a higher ceramide score were cross-sectionally associated with greater WMH volume. These associations were slightly attenuated after adjustment for covariates but remained statistically significant. There was no association between plasma S1P and WMH volume. These results suggest that elevated plasma ceramide levels are associated with greater WMH volumes, independent of hypertension and may be a useful plasma marker for predicting cerebrovascular disease.
Ceramides and S1P have key roles in vascular-related pathways. S1P activates endothelial nitric oxide synthase (eNOS)-derived nitric oxide (NO) production, which is important for blood pressure regulation.20 This lipid is also an important regulator of vascular growth,21,22 angiogenesis,23 permeability,24 and vascular tone.20,25 Studies of cellular and animal models have shown that ceramides increase endothelial permeability and either induce vasodilation or vasoconstriction depending on the vascular beds, cell types, vascular diameter, and animal model.8,26 Plasma ceramide levels have been shown to be elevated among patients with hypertension, and increases in ceramides were found to correlate with increased severity of hypertension.27
Although previous studies have reported associations of ceramides, ceramide ratios, and the ceramide risk score and multiple cardiovascular outcomes,10–15 studies have not examined the relationship between plasma ceramides and WMH volume. Given the association between these sphingolipids, hypertension, and vascular pathology, we hypothesized that elevated ceramides and S1P would be associated with greater WMH volume. However, we did not know whether this association would be fully mediated by hypertension. Although we found that hypertension partly attenuated the association between the ceramides and WMH volume, there was still a significant association. Thus, elevated levels of plasma ceramides are independently associated with WMH volume.
In univariate analyses, we did observe a possible association between higher plasma S1P and lower WMH volume, which might be expected given the vascular protective effects of S1P. However, after adjustment for hypertension and other covariates, the results were attenuated and essentially null. It is possible that hypertension more strongly attenuated the association between S1P and WMH compared to ceramides and WMH. Of note, the impact of S1P on the cardiovascular system depends on the S1P concentration and receptor; activation of S1P receptor 1 has been associated with vasodilation whereas activation of S1P receptor 3 has been associated with vascular constriction.7 It is difficult to determine how blood S1P levels impact each receptor in the current study to obtain the observed result.
Recent studies have suggested that ratios of Cer(d18:1/16:0), Cer(d18:1/18:0) and Cer(d18:1/24:1) to Cer(d18:1/24:0), and the corresponding ceramide risk score, are better predictors of vascular outcomes compared to individual chain lengths.13,14 These studies have found that Cer(d18:1/16:0), Cer(d18:1/18:0) and Cer(d18:1/24:1) were associated with increased risk of the outcomes whereas Cer(d18:1/24:0) was associated with reduced risk. Thus, the ratios resulted in stronger associations. In the current study, the only ceramide chain length associated with greater WMH volume was Cer d18:1/16:0. However, the ceramide ratios C16:0_C24:0 and C24:1_C24:0, and the ceramide risk score, were more strongly associated with WMH volume. These results further support the use of the ceramide ratios and risk score for cardio- and cerebrovascular outcomes compared to individual ceramide chain lengths.
WMH volume has been shown to be greater in women compared to men.28 In addition, we have previously shown longitudinal sex-specific trajectories of increasing plasma ceramides with greater increases in ceramide levels for women compared to men.29 Therefore, we determined whether the relationship between ceramide and S1P interacted with sex in relation to WMH volume. We did not find an interaction. This may indicate that the association between plasma ceramides and WMH volume is similar for both women and men. However, since women have higher ceramide levels, they are more affected with WMH. Future research examining sex differences in the relationship between sphingolipids and cerebrovascular pathology is warranted.
In conclusion, the present results suggest that the sphingolipid pathway, specifically plasma ceramide ratios and the ceramide risk score, is associated with WMH volume and may be useful for detection of cerebrovascular disease. Because MCSA participants who do not consent to a MRI are older and are more frequently diagnosed with hypertension, the observed association is likely a conservative estimate and replication is needed. A limitation of the study is the cross-sectional study design, which can only infer an association. Future studies are needed to evaluate if plasma ceramides have prognostic utility for cerebrovascular damage and to assess the longitudinal association between serial plasma ceramide levels and WMH volume changes.
Supplementary Material
{kind=link}
Highlights.
Plasma ceramides have been associated with risk of major adverse cardiovascular events and death, but have not been examined in relation to cerebrovascular pathology.
Higher levels of specific plasma ceramide ratios are associated with greater white matter hyperintensity volumes.
Elevated levels of specific plasma ceramide ratios may be indicative of brain vascular burden.
Acknowledgments
Sources of Funding
This work was supported by the National Institutes of Health/National Institute on Aging grants U01 AG006786, R01 AG011378, and R01 AG049704, R01 NS097495, the GHR Foundation, and was made possible by the Rochester Epidemiology Project (R01 AG034676).
Disclosures
Dr. Mielke receives unrestricted research grants from Biogen and Lundbeck. Dr. Bai is an employee of Eli Lilly. Dr. Knopman serves on a Data Safety Monitoring Board for Lundbeck Pharmaceuticals and for the DIAN study, and is an investigator in clinical trials sponsored by Biogen, Lilly Pharmaceuticals, and the Alzheimer’s Disease Cooperative Study. Dr. Jack has provided consulting services for Eli Lilly and serves on a DSMB for Roche but he receives no personal compensation from any commercial entity. Dr. Petersen is a consultant for Roche, Inc., Merck, Inc., Biogen, Inc., Genentech, Inc., and GE Healthcare. All other authors have nothing to disclose.
Nonstandard Abbreviations and Acronyms
- eNOS
endothelial nitric oxide synthase
- MCSA
Mayo Clinic Study of Aging
- MRI
magnetic resonance imaging
- NO
nitric oxide
- S1P
sphingosine-1-phosphate
- SD
standard deviation
- WMH
white matter hyperintensity
Contributor Information
Michelle M. Mielke, Department of Health Sciences Research, Mayo Clinic Rochester, MN Department of Neurology, Mayo Clinic Rochester, MN.
Jeremy A. Syrjanen, Department of Health Sciences Research, Mayo Clinic Rochester, MN
Hai H. Bui, Eli Lilly and Company, Indianapolis, IN
Ronald C. Petersen, Department of Health Sciences Research, Mayo Clinic Rochester, MN Department of Neurology, Mayo Clinic Rochester, MN.
David S. Knopman, Department of Neurology, Mayo Clinic Rochester, MN
Clifford R. Jack, Jr, Department of Radiology, Mayo Clinic Rochester, MN.
Jonathan Graff-Radford, Department of Neurology, Mayo Clinic Rochester, MN.
Prashanthi Vemuri, Department of Radiology, Mayo Clinic Rochester, MN.
References
- 1.Alber J, Alladi S, Bae HJ, et al. White matter hyperintensities in vascular contributions to cognitive impairment and dementia (VCID): Knowledge gaps and opportunities. Alzheimers Dement (N Y). 2019;5:107–117. doi: 10.1016/j.trci.2019.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666 10.1136/bmj.c3666 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Thomas AJ, Perry R, Barber R, Kalaria RN, O’Brien JT. Pathologies and pathological mechanisms for white matter hyperintensities in depression. Ann N Y Acad Sci. 2002;977:333–339. [DOI] [PubMed] [Google Scholar]
- 4.Gouw AA, Seewann A, Vrenken H, van der Flier WM, Rozemuller JM, Barkhof F, Scheltens P, Geurts JJ. Heterogeneity of white matter hyperintensities in Alzheimer’s disease: post-mortem quantitative MRI and neuropathology. Brain. 2008;131:3286–3298. doi: 10.1093/brain/awn265 [DOI] [PubMed] [Google Scholar]
- 5.Erten-Lyons D, Woltjer R, Kaye J, Mattek N, Dodge HH, Green S, Tran H, Howieson DB, Wild K, Silbert LC. Neuropathologic basis of white matter hyperintensity accumulation with advanced age. Neurology. 2013;81:977–983. doi: 10.1212/WNL.0b013e3182a43e45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alewijnse AE, Peters SL. Sphingolipid signalling in the cardiovascular system: good, bad or both? Eur J Pharmacol. 2008;585:292–302. doi: 10.1016/j.ejphar.2008.02.089 [DOI] [PubMed] [Google Scholar]
- 7.Cantalupo A, Gargiulo A, Dautaj E, Liu C, Zhang Y, Hla T, Di Lorenzo A. S1PR1 (Sphingosine-1-Phosphate Receptor 1) Signaling Regulates Blood Flow and Pressure. Hypertension. 2017;70:426–434. 10.1161/HYPERTENSIONAHA.117.09088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cogolludo A, Villamor E, Perez-Vizcaino F, Moreno L. Ceramide and Regulation of Vascular Tone. Int J Mol Sci. 2019;20:411. doi: 10.3390/ijms20020411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Spijkers LJ, van den Akker RF, Janssen BJ, Debets JJ, De Mey JG, Stroes ES, van den Born BJ, Wijesinghe DS, Chalfant CE, MacAleese L, Eijkel GB, Heeren RM, Alewijnse AE, Peters SL. Hypertension is associated with marked alterations in sphingolipid biology: a potential role for ceramide. PLoS One. 2011;6:e21817. doi: 10.1371/journal.pone.0021817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang DD, Toledo E, Hruby A, et al. Plasma Ceramides, Mediterranean Diet, and Incident Cardiovascular Disease in the PREDIMED Trial (Prevencion con Dieta Mediterranea). Circulation. 2017;135:2028–2040. doi: 10.1161/CIRCULATIONAHA.116.024261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cheng JM, Suoniemi M, Kardys I, et al. Plasma concentrations of molecular lipid species in relation to coronary plaque characteristics and cardiovascular outcome: Results of the ATHEROREMO-IVUS study. Atherosclerosis. 2015;243:560–566. doi: 10.1016/j.atherosclerosis.2015.10.022 [DOI] [PubMed] [Google Scholar]
- 12.Havulinna AS, Sysi-Aho M, Hilvo M, Kauhanen D, Hurme R, Ekroos K, Salomaa V, Laaksonen R. Circulating Ceramides Predict Cardiovascular Outcomes in the Population-Based FINRISK 2002 Cohort. Arterioscler Thromb Vasc Biol. 2016;36:2424–2430. doi: 10.1161/ATVBAHA.116.307497 [DOI] [PubMed] [Google Scholar]
- 13.Laaksonen R, Ekroos K, Sysi-Aho M, et al. Plasma ceramides predict cardiovascular death in patients with stable coronary artery disease and acute coronary syndromes beyond LDL-cholesterol. Eur Heart J. 2016;37:1967–1976. doi: 10.1093/eurheartj/ehw148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Meeusen JW, Donato LJ, Bryant SC, Baudhuin LM, Berger PB, Jaffe AS. Plasma Ceramides. Arterioscler Thromb Vasc Biol. 2018;38:1933–1939. doi: 10.1161/ATVBAHA.118.311199 [DOI] [PubMed] [Google Scholar]
- 15.Polzin A, Piayda K, Keul P, Dannenberg L, Mohring A, Graler M, Zeus T, Kelm M, Levkau B. Plasma sphingosine-1-phosphate concentrations are associated with systolic heart failure in patients with ischemic heart disease. J Mol Cell Cardiol. 2017;110:35–37. doi: 10.1016/j.yjmcc.2017.07.004 [DOI] [PubMed] [Google Scholar]
- 16.Roberts RO, Geda YE, Knopman DS, Cha RH, Pankratz VS, Boeve BF, Ivnik RJ, Tangalos EG, Petersen RC, Rocca WA. The Mayo Clinic Study of Aging: design and sampling, participation, baseline measures and sample characteristics. Neuroepidemiology. 2008;30:58–69. doi: 000115751 [pii] 10.1159/000115751 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.St. Sauver JL, Grossardt BR, Yawn BP, Melton LJ 3rd, Pankratz JJ, Brue SM, Rocca WA. Data resource profile: the Rochester Epidemiology Project (REP) medical records-linkage system. Int J Epidemiol. 2012;41:1614–1624. doi: 10.1093/ije/dys195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256:183–194. [DOI] [PubMed] [Google Scholar]
- 19.Raz L, Jayachandran M, Tosakulwong N, Lesnick TG, Wille SM, Murphy MC, Senjem ML, Gunter JL, Vemuri P, Jack CR Jr., Miller VM, Kantarci K. Thrombogenic microvesicles and white matter hyperintensities in postmenopausal women. Neurology. 2013;80:911–918. doi: 10.1212/WNL.0b013e3182840c9f [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dantas AP, Igarashi J, Michel T. Sphingosine 1-phosphate and control of vascular tone. Am J Physiol Heart Circ Physiol. 2003;284:H2045–2052. doi: 10.1152/ajpheart.01089.2002 [DOI] [PubMed] [Google Scholar]
- 21.Liu Y, Wada R, Yamashita T, Mi Y, Deng CX, Hobson JP, Rosenfeldt HM, Nava VE, Chae SS, Lee MJ, Liu CH, Hla T, Spiegel S, Proia RL. Edg-1, the G protein-coupled receptor for sphingosine-1-phosphate, is essential for vascular maturation. J Clin Invest. 2000;106:951–961. doi: 10.1172/JCI10905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kono M, Mi Y, Liu Y, Sasaki T, Allende ML, Wu YP, Yamashita T, Proia RL. The sphingosine-1-phosphate receptors S1P1, S1P2, and S1P3 function coordinately during embryonic angiogenesis. J Biol Chem. 2004;279:29367–29373. doi: 10.1074/jbc.M403937200 [DOI] [PubMed] [Google Scholar]
- 23.Lee OH, Kim YM, Lee YM, Moon EJ, Lee DJ, Kim JH, Kim KW, Kwon YG. Sphingosine 1-phosphate induces angiogenesis: its angiogenic action and signaling mechanism in human umbilical vein endothelial cells. Biochem Biophys Res Commun. 1999;264:743–750. 10.1006/bbrc.1999.1586 [DOI] [PubMed] [Google Scholar]
- 24.Lee MJ, Thangada S, Claffey KP, Ancellin N, Liu CH, Kluk M, Volpi M, Sha’afi RI, Hla T. Vascular endothelial cell adherens junction assembly and morphogenesis induced by sphingosine-1-phosphate. Cell. 1999;99:301–312. [DOI] [PubMed] [Google Scholar]
- 25.Cantalupo A, Zhang Y, Kothiya M, Galvani S, Obinata H, Bucci M, Giordano FJ, Jiang XC, Hla T, Di Lorenzo A. Nogo-B regulates endothelial sphingolipid homeostasis to control vascular function and blood pressure. Nat Med. 2015;21:1028–1037. doi: 10.1038/nm.3934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Goggel R, Winoto-Morbach S, Vielhaber G, Imai Y, Lindner K, Brade L, Brade H, Ehlers S, Slutsky AS, Schutze S, Gulbins E, Uhlig S. PAF-mediated pulmonary edema: a new role for acid sphingomyelinase and ceramide. Nat Med. 2004;10:155–160. doi: 10.1038/nm977 [DOI] [PubMed] [Google Scholar]
- 27.Spijkers LJ, Janssen BJ, Nelissen J, Meens MJ, Wijesinghe D, Chalfant CE, De Mey JG, Alewijnse AE, Peters SL. Antihypertensive treatment differentially affects vascular sphingolipid biology in spontaneously hypertensive rats. PLoS One. 2011;6:e29222. doi: 10.1371/journal.pone.0029222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fatemi F, Kantarci K, Graff-Radford J, Preboske GM, Weigand SD, Przybelski SA, Knopman DS, Machulda MM, Roberts RO, Mielke MM, Petersen RC, Jack CR Jr., Vemuri P. Sex differences in cerebrovascular pathologies on FLAIR in cognitively unimpaired elderly. Neurology. 2018;90:e466–e473. doi: 10.1212/WNL.0000000000004913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mielke MM, Bandaru VV, Han D, An Y, Resnick SM, Ferrucci L, Haughey NJ. Demographic and clinical variables affecting mid- to late-life trajectories of plasma ceramide and dihydroceramide species. Aging Cell. 2015;14:1014–1023. doi: 10.1111/acel.12369 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.