

Abstract
Background.
Children and youth with intellectual disabilities (ID) are known to face obstacles to physical activity participation, yet the activity patterns of this population are not well characterized.
Objective/Hypothesis.
In this study, time spent in moderate to vigorous physical activity (MVPA), type, and frequency of participation in physical activities were assessed in youth with ID and in a comparison group of typically developing (TD) youth.
Methods.
Weekly participation in MVPA in 38 youth with ID and 60 TD youth was assessed via accelerometry. Participants were also administered an interview about the frequency and type of physical activities they engaged in over the past year.
Results.
After adjusting for age and sex, youth with ID spent significantly less time in MVPA (33.5 vs. 46.5 min/day, p=0.03) and were less likely to meet the US Physical Activity Guidelines than TD youth (6% vs. 29%, p=0.01). Although time in MVPA was lower in youth with ID, females with ID participated in physical activities more frequently than TD females (47.1 vs. 28.2 times/month, p=0.008) and also reported engaging in a greater variety of physical activities (7.8 vs. 5.2 activities/year, p=0.01). No differences between males in the frequency of physical activity participation or the number of activities performed were observed. Both groups reported walking/hiking and active video as top activities.
Conclusions.
Findings emphasize the need for targeted efforts to increase MVPA in youth with ID.
Keywords: Youth, disability, accelerometry
Introduction
Fewer than one in four adolescents in the United States (US) achieve the recommended 60 minutes/day of moderate-to-vigorous intensity physical activity (MVPA).1,2 In light of the link between physical activity and chronic disease risk, the low levels of physical activity among children and youth are a public health concern. The US 2018 Report Card on Physical Activity for Children and Youth underscores the need to increase national attention to physical activity promotion, given that the ten indicators for physical activity remain low and relatively unchanged from the 2016 report.3 The 2018 Report Card also noted disparities in certain subgroups who lag behind in acquiring adequate amounts of physical activity; including children with disabilities.
Intellectual disability (ID) is a developmental disability characterized by significant limitations in both intellectual functioning and adaptive behavior.4 These limitations may make it more difficult for children and youth with ID to access physical activity opportunities. Emerging research documents that children and youth with ID fall short of meeting the physical activity guidelines and are less active than their typically developing (TD) peers.5–7
Studies that include objective measurement of physical activity in youth with ID have been limited by small sample sizes and/or no direct comparison group of TD peers.5, 8–10 Furthermore, few studies have aimed to characterize the physical activity behaviors of youth with ID beyond quantifying the duration and intensity of participation. Consequently, more research is needed to understand physical activity participation of youth with ID, which can serve to inform and improve interventions. We aimed to examine and compare time spent in objectively-measured MVPA and the types and frequency of physical activities performed by youth with and without ID. We tested the hypotheses that youth with ID would spend less time in MVPA compared to TD youth, and that they would participate in fewer distinct physical activities, and at lower frequencies.
Methods
This study was part of a larger (parent) project, the Teens Recreation and Activity Choice (TRAC) study. The TRAC study was a cross-sectional observational study designed to examine the activity levels and correlates of physical activity among youth with ID as well as youth with autism spectrum disorder (ASD), and a common comparison group of TD youth.11,12,13 This paper reports on youth with ID only and the TD comparison group.
Participants
The methods employed in this study have been previously described.12 Briefly, youth with ID ages 13–21 years and TD youth ages 13–18 years were recruited to participate in the TRAC study. The upper age limit for youth with ID was extended because students with disabilities may remain in school until their 22nd birthday, and our inclusion criteria required that participants be in secondary school. Participants were required to be in good health and were excluded if they had an acute or chronic medical illness, a developmental disability other than ID (including ASD), a physical disability/mobility impairment, a significant mental health disorder, or an acute or chronic injury that restricted physical activity. Youth who were able to communicate verbally and resided at home with a parent/guardian were eligible. Recruitment materials were distributed across eastern and central areas of two New England states by email, websites, mail, list serves, and in person through disability service agencies, special education parent advisory councils, community organizations, Craigslist™, and schools. Eligibility was initially determined by a telephone interview with a parent. Eligible youth were then invited to attend a study visit. During the visit, youth with ID completed the Kaufman Brief Intelligence Test, 2nd edition (KBIT-2)14 to ensure that they met the criterion for ID, defined as a composite score of 75 or below. Parents of youth with ID also completed the Vineland Adaptive Behavior Scales II (VABS-II)15 to enable us to characterize the sample based on adaptive functioning.
Informed consent was obtained from a parent, and youth indicated their willingness to participate by signing an assent or consent form (depending on guardianship status) that was read aloud. The study protocol and all materials were approved by the University of Massachusetts Medical School Institutional Review Board for the protection of human subjects.
Time Spent in Physical Activity
Physical activity levels were measured via Actical® accelerometers. Participants were asked to wear the accelerometer for 7 days, including 5 weekdays and 2 weekend days. Accelerometers are considered a gold standard for quantifying physical activity and have been used in several previous studies involving youth with ID,5–8, 16–18 Participants wore the accelerometer on a belt positioned over the hip. Instructions to participants and their parents directed the participant to wear the accelerometer for all waking hours except when in water. Parents were asked to complete a daily log in which they recorded when the accelerometer was put on and removed during the day. We also asked parents to note if the day was atypical (e.g., child was home sick). We used information from the log to calculate wear time. To be included in the analyses, accelerometers needed to be worn for a minimum of three “typical” weekdays and one weekend day for ≥600 minutes/day.19–20
Activity counts from the accelerometer were recorded over 15-second epochs. We summed the 15-second epochs to create 60-second activity counts; this was used to estimate the amount of time spent in MVPA, based on previously established cut-points for intensity, defined as activity counts ≥1500.21 We created a composite variable for physical activity that was at moderate-to-vigorous levels. We computed total weekly activity counts and minutes of MVPA per day across weekdays and weekend days. In addition, total average daily physical activity (in activity counts and minutes/day) was computed from a weighted average of weekday and weekend activity data [(5 × weekday average + 2 × weekend average)/7].
Physical Activity Type and Frequency
We developed a questionnaire that was designed to gather information on both the type and frequency of physical activities that youth performed over the past year, as described previously.12 This information would contribute to a better understanding of the variety of activities that youth engaged in and provide a more comprehensive picture of their physical activity participation. The questionnaire was designed to be administered verbally as a structured interview. Because recalling and accurately reporting physical activity participation may be difficult for youth with ID, we interviewed a parent and the youth together. A trained interviewer met with the youth and their parent during the interview, which enabled them to confer and reach consensus on the most accurate estimate. In cases where the parent and youth had different responses to a question, and/or when they were uncertain or disagreed about the type and/or frequency of an activity, the interviewer asked clarifying questions to assist them in reaching consensus. For consistency, the same interview procedure was used for both youth with ID and the comparison group of TD youth.
The interview comprises questions about activities that youth engaged in during out-of-school time, including time after school, on the weekends, and during the summer. The interview queried respondents about 29 physical activities, such as football, dancing, wrestling, bicycling, swimming, active video gaming, baseball/softball, and walking/hiking. The interview included a two-part question for each of activity. Participants were first asked whether they “ever” participated in the activity in the past year. For example, “Did you ever play/do basketball in the last year?” A picture of a person playing basketball was shown to participants when the question was asked. Visual supports of this nature were offered in order to help participants understand the activity contained in the question. If the participant answered “yes” to the question, they were then asked if they had performed that activity 12 or more times in the past year, which we deemed to be a regular activity. Our goal was to determine the physical activities that youth participated in on a regular basis (i.e., a minimum of 1 time/month, on average). For activities that youth endorsed performing 12 or more times in the past year, we asked them to report the frequency of their participation on a month-by-month basis. For example, participants were asked, “In which months last year did you play basketball?” For each month that the participant reported performing the activity, they were asked, for example, “How often did you play basketball in September?” Frequency response options included: 1 time/month, 2–3 times/month, 1 time/week, 2–3 times/week, 4–6 times/week, and 1 time/day or more. These response choices were also included on a printed card for participants to refer to, and the interviewer also repeated the questions and response choices as needed. Upon reporting on all 29 activities, participants were asked to report any other physical activities that they may have performed over the course of the prior year. For each additional activity reported, the interviewer proceeded through the same questioning protocol outlined above. Over the course of the study, 24 additional physical activities were reported.
We assessed test-retest reliability of the questionnaire by comparing the responses from a subset of participants (n=15 with ID; n=20 TD) who volunteered to repeat the interview within 14–21 days of the original interview. From these data, we calculated a correlation coefficient; the reliability of monthly physical activity frequency was good in both groups (r=0.86, p<0.001 for participants with ID; r=0.75, p<0.01 for TD participants).12 We also assessed the reliability for the variable representing the number of activities done at least 12 times annually, which was fair for youth with ID (r=0.54, p=0.04) and good for TD youth (r=0.85, p<0.01 for TD).12
Only activities that were performed at least 12 times in the past year (i.e., those deemed as regular activities) were included in analyses. We converted the frequency response categories to numeric monthly estimates: 1 time/month = 1; 2–3 times/month = 2.5; 1 time/week = 4.35; 2–3 times/week = 10.88; 4–6 times/week = 21.75; 7 times/week or more = 30.45. We calculated the total monthly physical activity frequency by summing the frequency of participation in all regular activities for each month, and then dividing that number by 12. The number of activities each participant engaged in at least 12 times annually was also calculated to obtain a measure of activity variety.
Statistical Analyses
Demographic characteristics between the groups were compared using independent sample t-tests for continuous variables and chi-square tests for categorical variables. We also used a chi-square test to evaluate whether the proportion of youth with ID meeting physical activity guidelines differed from the comparison group of TD youth. Linear regression was used to evaluate differences between the groups for the accelerometry data (i.e., total activity counts and MVPA minutes/week on weekdays, weekend days, and as a weighted weekly average) as well as for physical activity participation from the interview (i.e., the frequency of activities and number of regular activities). We included age and sex as covariates in our regression models to adjust for differences in the age and sex distributions between the two groups and to facilitate comparisons with other studies. Group-by-age and group-by-sex interactions were also evaluated for each outcome to assess whether differences by group were influenced by age or sex. To characterize the individual physical activities that the youth with ID and TD youth preferred, we calculated the percentage in each group who reported each activity at least 12 per year, and ranked the top 10 for each group. All analyses were conducted using SAS version 9.2 and IBM SPSS Statistics 20. P-values ≤ 0.05 were considered statistically significant.
Results
Thirty-eight youth with ID (17 males and 21 females) and 60 TD youth (36 males and 24 females) participated in the study. Demographic characteristics of the sample are presented in Table 1. Youth with ID were significantly older than TD youth (16.8 years vs. 15.3 years; p<0.001). The sample was predominantly white, and most of the parents of youth in both groups were college-educated.
Table 1.
Characteristics of Youth with ID and TD Youth
| TD Adolescents (n=60) | Adolescents with ID (n=38) | p-value | |
|---|---|---|---|
| Age (y)* | 15.3 (1.5) | 16.8 (1.9) | <0.001 |
| Male (%) | 60% | 45% | 0.14 |
| Race/Ethnicity, % White | 68% | 84% | 0.08 |
| At least 1 parent with college degreea | 82% | 72% | 0.29 |
| KBIT Score*b | - | 53.5 (11.6) | - |
| Vineland Composite*c | - | 66.4 (5.4) | - |
mean, (SD),
n=36,
Kaufman Brief Intelligence Test,
n=31
Accelerometry
Thirty-two (84%) youth with ID and 55 (92%) TD youth met the criteria for wear time and were included in the accelerometry analyses (no significant group differences; p>0.05 by chi-square). Youth with ID wore the accelerometer for significantly fewer minutes than TD youth both on weekdays (836 minutes vs. 925 minutes, p<0.001) and also as a daily weighted average (812 minutes vs. 887 minutes, p<0.001); however, we observed no significant correlations between wear time and physical activity counts or minutes of MVPA in either group. Consequently, wear time was not deemed to be a confounding factor and thus was not included as a covariate in our analyses.
Table 2 depicts the accelerometer data, including total activity counts and time spent in MVPA, both adjusted for age and sex. Total activity counts were lower among youth with ID compared to TD youth on weekdays (p=0.05) and as a daily weighted average (p=0.05); as was time spent in MVPA on weekdays (p=0.03) and as a daily weighted average (p=0.03). Youth with ID engaged in an average of 33.5 minutes/day in MVPA compared to 46.5 minutes/day among TD youth as a daily weighted average. On weekdays, youth with ID spent 36.9 minutes/day in MVPA compared to 50.8 minutes/day by TD youth. There were no significant differences between the groups in activity counts or minutes in MVPA on weekend days. Significantly fewer youth with ID met the recommendation of at least 60 minutes/day of MVPA compared to TD youth (6% vs. 29%, respectively, p=0.01). None of the group-by-age or group-by-sex interactions were statistically significant.
Table 2.
Accelerometer-Measured Physical Activity Level among TD Youth and Youth with ID*
| Weekdays | Weekend Days | Daily Weighted Average | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TD Mean (n=55) | ID Mean (n=32) | Mean Difference (95%CI) | p-value | TD Mean (n=55) | ID Mean (n=32) | Mean Difference (95%CI) | p- value | TD Mean (n=55) | ID Mean (n=32) | Mean Difference (95%CI) | p-value | |
| Total Activity Counts | 243,325 | 192,542 | 50,783 (165 to 101,402) | 0.05 | 191,806 | 150,493 | 41,313 (−18,255 to 100,881) | 0.17 | 228,605 | 180,528 | 48,078 (−422 to 96,577) | 0.05 |
| Time in MVPA (min) | 50.8 | 36.9 | 13.9 (1.4 to 26.3) | 0.03 | 35.7 | 24.7 | 11.0 (−3.1 to 25.1) | 0.13 | 46.5 | 33.5 | 13.0 (1.3 to 24.8) | 0.03 |
Least squares means adjusted for age (continuous) and sex
Structured Interview Data
Physical Activity Frequency.
The data derived from the structured interview are presented in Table 3. We observed a significant group-by-sex interaction for both activity frequency and the number of regular activities performed ≥12 times annually. When we stratified by sex, significant differences between youth with ID and TD youth were observed, but only for females. Female youth with ID reported participating in various physical activities more frequently than female TD youth (47.1 times/month vs. 28.2 times/month, p=0.008). With respect to variety of activities done a regular basis, female adolescents with ID reported engaging in an average of 7.8 activities compared to 5.2 activities reported by female TD youth (p=0.01). We observed no statistically significant differences between males with ID and TD males in the frequency of physical activity participation (45.4 times/month ID vs. 45.3 times/month TD) or the number of regular activities performed (i.e., variety) (7.1 activities ID vs. 7.0 activities TD).
Table 3.
Frequency of Participation in Physical Activities and Number of Regular Activities* among TD Youth and Youth with ID**
| TD Mean | ID Mean | Mean Difference (95% CI) | p-value | ||
|---|---|---|---|---|---|
| Frequency of participation (times/month) | |||||
| Overall**a | 37.8 | 47.6 | −9.8 (−20.8 to 1.2) | 0.08 | |
| Malesb | 45.3 | 45.4 | −0.1 (−17.1 to 16.9) | 0.99 | |
| Femalesc | 28.2 | 47.1 | −18.9 (−32.4 to −5.3) | 0.008 | |
| Number of regular activities | |||||
| Overall**a | 6.3 | 7.6 | −1.3 (−2.8 to 0.05) | 0.06 | |
| Malesb | 7.0 | 7.1 | −0.06 (−2.1 to 1.9) | 0.94 | |
| Femalesc | 5.2 | 7.8 | −2.6 (−4.6 to −0.6) | 0.01 | |
Activities performed ≥12 times/year
Overall adjusted for age and sex; sex-stratified adjusted for age
n=59 TD, 37 ID
n=36 TD, 17 ID
n=23 TD, 20 ID
Type of Physical Activities.
The 10 activities most frequently reported as regular activities among youth with ID were (in rank order): basketball, swimming, walking/hiking, active video gaming, dancing, bowling, running/jogging, bicycling, weightlifting, and baseball/softball. The 10 activities that were most frequently reported as regular activities (in rank order) for the comparison group of TD youth included: running/jogging, active video gaming, walking/hiking, swimming, basketball, bicycling, dancing, football, weightlifting, and baseball/softball (Figure 1). Four of the top 5 activities reported by the TD youth were the same for adolescents with ID, although the rank order was slightly different (Figure 1).
Figure 1.
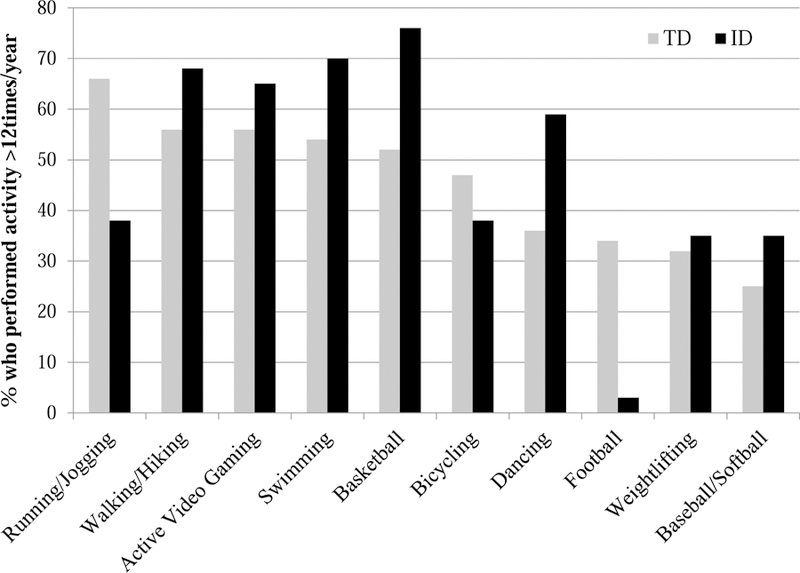
Physical activities most commonly reported as “regular” by group.
Discussion
We sought to characterize the physical activity levels of youth with ID and to compare them to TD youth. Our findings are largely in agreement with several previous studies indicating that adolescents with ID are not meeting the physical activity guidelines of at least 60 minutes/day of MVPA. We recognize that previous studies included youth with ID outside of the age range of our sample, yet similar results across the studies generally support that young people with ID are insufficiently active. For example, Downs and colleagues found that children with ID ages 5–15 years in the United Kingdom accumulated an average of 49.4 minutes/day of MVPA, and that only 23.7% met the 60 minutes/day physical activity recommendation.5 Similar results were observed in a large cross-sectional study of Spanish youth with Down syndrome ages 11–20 years that found 43% of participants engaged in 60 minutes/day of physical activity.7 The authors also found that the average time spent in MVPA was 57 minutes/day, and time in MVPA decreased significantly with age. Esposito and colleagues examined physical activity patterns of youth with Down syndrome between ages 8–16 years, and looked at trends and patterns across age ranges.9 Authors found that the adolescents ages 14–15.9 years in their sample engaged in only 24.7 minutes/day of MVPA, and overall there was a marked decline in physical activity with age. A recent study involving youth with ID ages 7–20 years in Sweden reported that participants accumulated an average of 80 minutes/day of MVPA and 52% of the sample met the WHO activity recommendations.22 In the present study conducted in the U.S., youth with ID ages 13–21 years accumulated an average of 29.7 minutes/day of MVPA, which falls within the range of time spent in MVPA reported in most of these previous studies. Only 6% of youth with ID in this study met physical activity recommendations, which is lower than some previously published work and may reflect the slightly older age of our participants. These highly discrepant estimates of time spent in MVPA suggest that more studies are needed to thoroughly describe physical activity levels of youth with ID.
The direct comparison of physical activity with TD peers in this study also supports that youth with ID are less active that TD youth. Einarsson and colleagues reported that the physical activity of Icelandic TD children ages 6–16 years was 40% higher compared to a group of children with ID, and none of the children with ID achieved physical activity recommendations compared to 40% of TD children.6 In an examination of time spent in MVPA by the same authors, children with ID ages 6–16 years accumulated only 41%, 50%, and 32% of the time that TD children spent in MVPA during an entire weekday, during school hours, and after school, respectively.23 In contrast, the Swedish youth with ID did not engage in significantly less time in MVPA compared to the TD youth.
In the present study, the significant difference in overall MVPA found between youth with ID and TD youth appears to be driven primarily by the difference in MVPA across weekdays. We found that both groups of youth showed a similar reduction in minutes of MVPA on weekend days compared to weekdays of about 30%; the weekend differences between groups was not significant, however. Participation in school-related activities such as physical education class and walking to/from school likely contributed to the higher weekday minutes in MVPA observed in our sample. The non-significant difference in minutes of MVPA on weekend days between the groups in this study may be attributed partly to the small sample size.
This qualitative assessment of physical activity behavior is meant to enrich the objective physical activity data from accelerometry, and thus provide a more thorough description of activity participation among youth with ID. Asking youth with ID to directly report on their own activities through an interview was an important element of this study, as previously described.24 Findings regarding the variety of physical activities and frequency of participation reported by the youth were unexpected. We found that male youth with ID and male TD youth engaged in a similar array of physical activities; the number of regular activities was almost exactly the same between the two groups of males, as was the overall frequency of participation. Surprisingly, female youth with ID engaged in a greater number of physical activities with higher frequency than did TD females. Females with ID were very similar to both groups of males (ID and TD) in the number of regular activities that they engaged in and the number of times/month that they participated. It may be that girls with ID are more willing to try new activities compared to TD girls. Across groups and by gender, it was the TD girls who were unique in their limited variety and low frequency of physical activity. Notably, our frequency measure was represented only by the number of times each month that an adolescent reported doing an activity, and was not tied to a minimum duration or intensity. Thus, although youth with ID participated with similar or greater frequency than their TD counterparts, they may not participate in the activity for as many minutes or at an intensity level that represents MVPA. Youth in both groups reported that running/jogging, active video gaming, walking/hiking, swimming, and basketball were among the regular activities that they most commonly performed. Previous studies of the physical activities most frequently reported among youth with ID generally support our findings. For example, in a sample of Australian children with Down syndrome ages 5–18 years, the most common physical activities were swimming, bowling, soccer, basketball, and dancing.25 In a study of adolescents with ID ages 16–18 years in Taiwan, caregivers reported that the top three activities of those youth who regularly engaged in physical activity were walking, sports, and jogging.26 The most reported physical activities among a sample of Irish adolescents with ID over age 16 years were walking, swimming, cycling, and football.27 Although some youth with ID may require activity modifications and support to successfully participate alongside their TD peers, the similar activity preferences reported by both groups of youth in our study hold promise for promoting inclusive sports/activity programs.
Further work is needed to determine the factors that underlie the differences in physical activity among these groups, though several barriers to participation for youth with ID have been reported and likely contribute to the lower activity levels we observed. Lack of accessible programs, lack of interest, physical/motor challenges, behavioral difficulties, insufficient time, no location at which to do physical activity, and transportation challenges have been identified as barriers to participation for children with ID.28–30 In our previous report of physical activity correlates within this sample, we found that fewer youth with ID reported that they have someone to do physical activity with compared to TD youth (64% vs. 93%, p<0.001), and a greater proportion of youth with ID perceived that physical activities were too hard to learn (41% vs. 0%, p<0.001).11
This study has limitations that should be considered. We used a small convenience sample from New England of mostly white youth, despite our efforts to recruit a larger and more racially diverse sample in both groups. Also, the group sizes were not even. Accurate self-report of physical activity behavior is known to be difficult, and may be particularly problematic for individuals with ID because of limitations in cognitive ability that affects understanding of questions and the ability to appraise the frequency of engagement in activities. As such, we found that parents of youth with ID were more likely to provide responses during the interview on physical activity whereas the TD youth mostly reported on their own behavior. This means that the comparative results between the ID and TD groups may have been influenced by the differential source of information. Additionally, the one-year recall timeline for the interview was long, which adds challenges. As mentioned above, our interview on physical activity types and frequency did not ask about duration or intensity which would have provided valuable information on participation.
This study also had several strengths. Participants had a high level of compliance with the accelerometry protocol; similar to a study in children with Down syndrome.10 Despite the relatively small sample, we had sufficient power to identify statistically significant differences between groups. Our findings provide objective information on physical activity levels of youth with ID and a comparison group of TD youth measured by accelerometry. Rather than relying on proxy reporting as has been the usual approach, information on the types and frequencies of physical activities that youth engaged in was obtained by jointly interviewing the adolescent with their parent. We believe the additional effort required to gather information directly from youth with ID not only improves the quality of the data, but it is also consistent with principles of inclusion.
Conclusions
Our results provide further evidence that youth with ID are not engaging in sufficient physical activity and fall short compared to their TD peers. These deficits exist despite similarities we observed between the groups regarding the types of activities performed and frequency of engagement. Additional research is needed to fully elucidate the physical activity patterns of this underserved population.
Acknowledgments:
The authors wish to acknowledge posthumously the contributions of James Gleason in designing the study and in cleaning and managing the accelerometer data. We also wish to thank Charmaine Lo, Courtney Dutra, and Renee Scampini (all affiliated with the University of Massachusetts Medical School-E.K. Shriver Center during the study) for their assistance with participant recruitment and data collection. We are very grateful to participants and their parents for their time and effort associated with this project.
Funding Source: This research study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (HD059100), National Institutes of Health; Boston Nutrition Obesity Research Center (DK46200); and Interdisciplinary Research in Intellectual/Developmental Disabilities (HD004147).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest: The authors declare no conflicts of interest.
Previous Presentation of Abstract:
This study was presented as a poster at the American College of Sports Medicine annual research meeting.
References
- 1.Fakhouri TH, Hughes JP, Burt VL, Song M, Fulton JE, Ogden CL. Physical activity in U.S. youth aged 12–15 years, 2012. NCHS Data Brief 2014;141:1–8. [PubMed] [Google Scholar]
- 2.Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40(1):181–188. [DOI] [PubMed] [Google Scholar]
- 3.Katzmarzyk PT, Denstel KD, Beals K, et al. Results from the 2018 United States report card on physical activity for children and youth. J Phys Act Health 2018;15(Suppl 2):S422–S424. [DOI] [PubMed] [Google Scholar]
- 4.Disabilities AAIDD. Definition of Intellectual Disability https://aaidd.org/intellectual-disability/definition# Accessed July 5, 2017.
- 5.Downs SJ, Fairclough SJ, Knowles ZR, Boddy LM. Physical Activity Patterns in Youth With Intellectual Disabilities. Adapt Phys Activ Q 2016;33(4):374–390. [DOI] [PubMed] [Google Scholar]
- 6.Einarsson IO, Olafsson A, Hinriksdottir G, Johannsson E, Daly D, Arngrimsson SA. Differences in physical activity among youth with and without intellectual disability. Med Sci Sports Exerc 2015;47(2):411–418. [DOI] [PubMed] [Google Scholar]
- 7.Izquierdo-Gomez R, Martinez-Gomez D, Acha A, Veiga OL, Villagra A, Diaz-Cueto M. Objective assessment of sedentary time and physical activity throughout the week in adolescents with Down syndrome. The UP&DOWN study. Res Dev Disabil 2014;35(2):482–489. [DOI] [PubMed] [Google Scholar]
- 8.Foley JT, McCubbin JA. An exploratory study of after-school sedentary behaviour in elementary school-age children with intellectual disability. J Intellect Dev Disabil 2009;34(1):3–9. [DOI] [PubMed] [Google Scholar]
- 9.Esposito PE, MacDonald M, Hornyak JE, Ulrich DA. Physical activity patterns of youth with Down syndrome. Intellect Dev Disabil 2012;50(2):109–119. [DOI] [PubMed] [Google Scholar]
- 10.Shields N, Dodd KJ, Abblitt C. Do children with Down syndrome perform sufficient physical activity to maintain good health? A pilot study. Adapt Phys Activ Q 2009;26(4):307–320. [DOI] [PubMed] [Google Scholar]
- 11.Stanish HI, Curtin C, Must A, Phillips S, Maslin M, Bandini LG. Physical activity enjoyment, perceived barriers, and beliefs among adolescents with and without intellectual disabilities. J Phys Act Health 2016;13(1):102–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stanish H, Curtin C, Must A, Phillips S, Maslin M, Bandini L. Physical activity levels, frequency, and type among adolescents with and without autism spectrum disorder. J Autism Devel Disord 2017;37(3): 785–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stanish H, Curtin C, Must A, Phillips S, Maslin M, Bandini L. Enjoyment, barriers, and beliefs about physical activity in adolescents with and without autism spectrum disorder. Adapt Phys Activ Q 2015;32(4): 302–317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kaufman AS, Kaufman NL. Kaufman Brief Intelligence Test: KBIT Circle Pines, MN: AGS (American Guidance Service) Publishing; 1990. [Google Scholar]
- 15.Sparrow S, Cicchetti D, Balla D. Vineland adaptive behavior scales: (Vineland II), survey interview form/caregiver rating form In. Livonia, MN: Pearson Assessments; 2005. [Google Scholar]
- 16.McGarty AM, Penpraze V, Melville CA. Accelerometer use during field-based physical activity research in children and adolescents with intellectual disabilities: a systematic review. Res Dev Disabil 2014;35(5):973–981. [DOI] [PubMed] [Google Scholar]
- 17.Hinckson EA, Curtis A. Measuring physical activity in children and youth living with intellectual disabilities: a systematic review. Res Dev Disabil 2013;34(1):72–86. [DOI] [PubMed] [Google Scholar]
- 18.Phillips AC, Holland AJ. Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without Down’s syndrome. PLoS One 2011;6(12):e28618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wolff-Hughes DL, Bassett DR, Fitzhugh EC. Population-referenced percentiles for waist-worn accelerometer-derived total activity counts in U.S. youth: 2003 – 2006 NHANES. PLoS One 2014;9(12):e115915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wolff-Hughes DL, McClain JJ, Dodd KW, Berrigan D, Troiano RP. Number of accelerometer monitoring days needed for stable group-level estimates of activity. Physiol Meas 2016;37(9):1447–1455. [DOI] [PubMed] [Google Scholar]
- 21.Puyau MR, Adolph AL, Vohra FA, Zakeri I, Butte NF. Prediction of activity energy expenditure using accelerometers in children. Med Sci Sports Exerc 2004;36(9):1625–1631. [PubMed] [Google Scholar]
- 22.Lobenius-Palmér K, Sjöqvist B, Hurtig-Wennlöf A, Lundqvist L. Accelerometer-assessed physical activity and sedentary time in youth with disabilties. Adapt Phys Activ Q 2018;35(1):1–19. [DOI] [PubMed] [Google Scholar]
- 23.Einarsson I, Jóhannsson E, Daly D, Arngrímsson S. Physical activity during school and after school among youth with and without intellectual disability. Res Dev Disabil 2016;56:60–70. [DOI] [PubMed] [Google Scholar]
- 24.Curtin C, Bandini LG, Must A, et al. Including youth with intellectual disabilities in health promotion research: Development and reliability of a structured interview to assess the correlates of physical activity among youth. J Appl Res Intellect Disabil 2016;29(4):378–386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oates A, Bebbington A, Bourke J, Girdler S, Leonard H. Leisure participation for school- aged children with Down syndrome. Disabil Rehabil 2011;33(19–20):1880–1889. [DOI] [PubMed] [Google Scholar]
- 26.Wuang Y, Su CY. Patterns of participation and enjoyment in adolescents with Down syndrome. Res Dev Disabil 2012;33(3):841–848. [DOI] [PubMed] [Google Scholar]
- 27.Buttimer J, Tierney E. Patterns of leisure participation among adolescents with a mild intellectual disability. J Intellect Disabil 2005;9(1):25–42. [DOI] [PubMed] [Google Scholar]
- 28.Lin J, Lin P, Lin L, Chang Y, Wu S, Wu J. Physical activity and its determinants among adolescents with intellectual disabilities. Res Dev Disabil 2010;31(1):263–269. [DOI] [PubMed] [Google Scholar]
- 29.Barr M, Shields N. Identifying the barriers and facilitators to participation in physical activity for children with Down syndrome. J Intellect Disabil Res 2011;55:1020–1033. [DOI] [PubMed] [Google Scholar]
- 30.Yazdani S, Yee C, Chung P. Factors predicting physical activity among children with special needs. Prev Chronic Dis 2013;10:E119. [DOI] [PMC free article] [PubMed] [Google Scholar]