

Abstract
Background
Cyamella,the sesamoid bones of the popliteus muscle, are rare in humans. Snapping knee is an uncommon problem which can be difficult to diagnose.
Case presentation
In this case, we report a 24-year-old male with snapping knee caused by symptomatic cyamella in the popliteus tendon. A large cyamella was identified upon surgery and was removed. Postoperatively, the patient had immediate relief of preoperative symptoms, and there were no signs of recurrence after 1 years of follow-up.
Conclusions
Although not previously suggested, symptomatic cyamella in the popliteus tendon should be considered as part of the differential diagnosis of the snapping knee.
Keywords: Cyamella, Popliteus, Sesamoid, Snapping knee, Surgery, Knee joint
Background
Cyamellae, the sesamoid bones of the popliteus muscle, are rare in humans [1]. Snapping knee, which is defined as a patient hearing or feeling a snapping or popping of joints at some specific activity [2], is an uncommon problem and can be difficult to diagnose [3]. Some differentials for the snapping knee include the presence of a discoid meniscus [4], rheumatoid nodules [5], iliotibial band (ITB) friction [6], biceps femoris tendon [3, 7], semitendinosus and gracilis tendons [8], popliteus tendon [9, 10] and intra-articular pathological changes. Firstly in this case, we report a 24-year-old male with snapping knee caused by symptomatic cyamella in the popliteus tendon. Secondly, diagnosis and treatment of this rare pathology are discussed. The literature associated with symptomatic cyamella in the popliteus tendon are also reviewed.
Case presentation
A 24-year-old male patient was presented to the outpatient department with a history of right lateral knee snapping and recurrent sensation of discomfort for the past 2 years. Snapping was elicited upon extending the knee and could be reproduced by applyng direct pressure on the posterolateral knee. There was no actual or previously sustained trauma noted on this patient.
The patient was initially and preliminarily diagnosed with knee joint plica syndrome and underwent arthroscopic surgery in a previous institution. This however did not relieve his symptoms. As the snapping continued, the patient became unable to tolerate physical activities or prolonged walking.
Upon thorough physical examination, full active range of motion was observed to be intact, but a reproducible audible and palpable snapping of the lateral knee when moving from flexion to extension. However, this was not consistently reproducible with passive range of motion. (see Additional file 1) Other special tests were negative except for the Cabot sign, which clearly produced a snapping sensation.
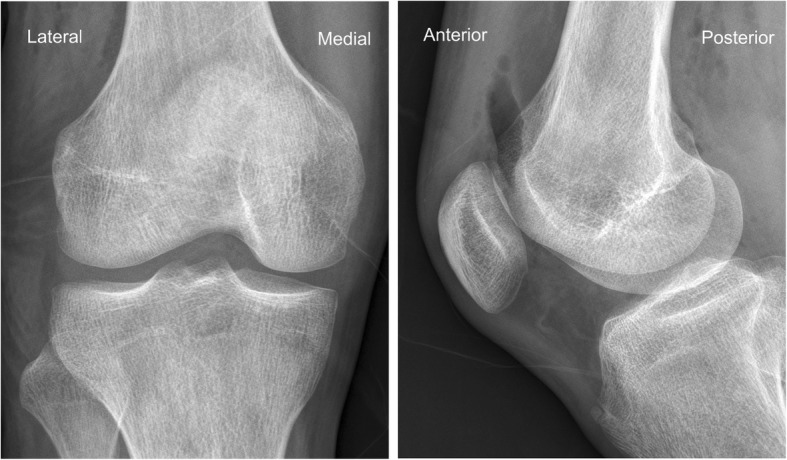
X-rays presented a round osseous structure in the posterolateral part of the joint, similar to the normal sesamoid (Fig. 1). CT scanning and MRI were additionally conducted. No pathological results were obtained apart from a clearly visible ovoid-shaped bone that was located posterior and superior to the proximal musculo-tendinous intersection of the popliteus muscle. The sesamoid bone articulates non-cartilagenously with the lateral dorsal femoral condyle (Figs. 2 and 3). The popliteus muscle and tendon presented signs of inflammation. A steroid injection was administered into the snapping point but did not relieve his symptoms.
Fig. 1.

Radiograph of the right knee. The cyamella may be seen as a round osseous body (arrow). "Lateral" indicates lateral side of the knee, "Medial" indicates medial side of the knee
Fig. 2.
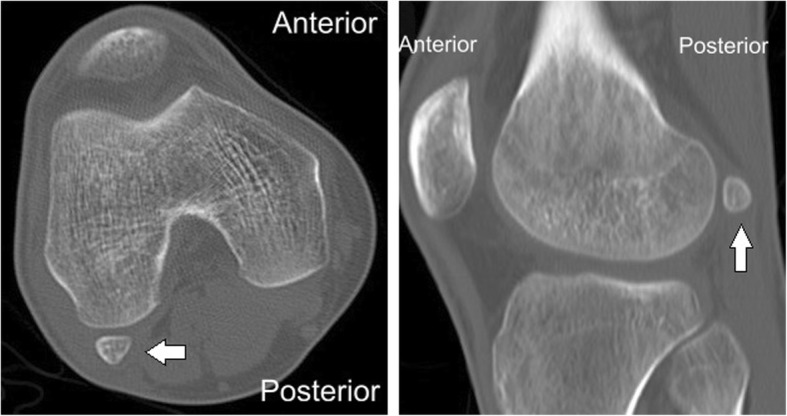
CT of the right knee. "Lateral" indicates lateral side of the knee, "Medial" indicates medial side of the knee, "Anterior" indicates anterior side of the knee, "Posterior" indicates posterior side of the knee. Arrow indicates the cyamella
Fig. 3.
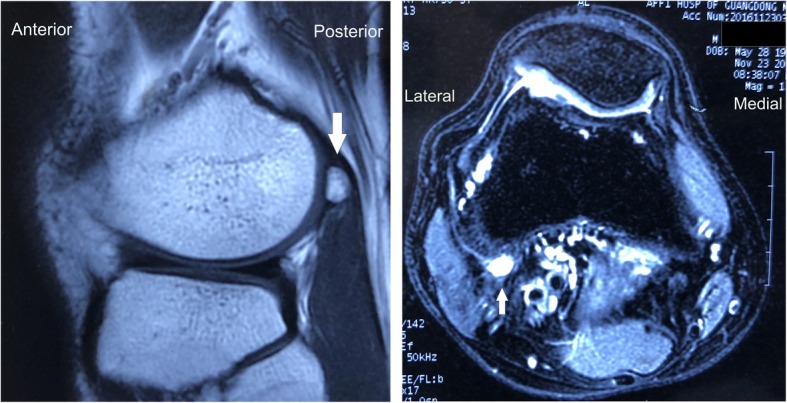
MRI scan of the right knee. The cyamella is shown with cortical and cancellous parts in the popliteal tendon posteriorsuperior. "Lateral" indicates lateral side of the knee, "Medial" indicates medial side of the knee, "Anterior" indicates anterior side of the knee, "Posterior" indicates posterior side of the knee. Arrow indicates the cyamella
A posterior approach was used to incise the bone which lead us to discover that the biceps femoris tendon presented no pathological changes. Deeper in the popliteus tendon, a large cyamella was found. With the knee in a passive range of motion, we found there was snapping of the popliteus tendon over the cyamella. (see Additional file 2) An incision was made directly over the located area and the sesamoid bone was excised (see Additional file 3). The cyamella located near the musculo-tendinous intersection of the popliteus muscle (Fig. 4). The specimen measured 15*7*9 mm (Fig. 5). Radiographs following the procedure demonstrated removal of the cyamella (Fig. 6).
Fig. 4.
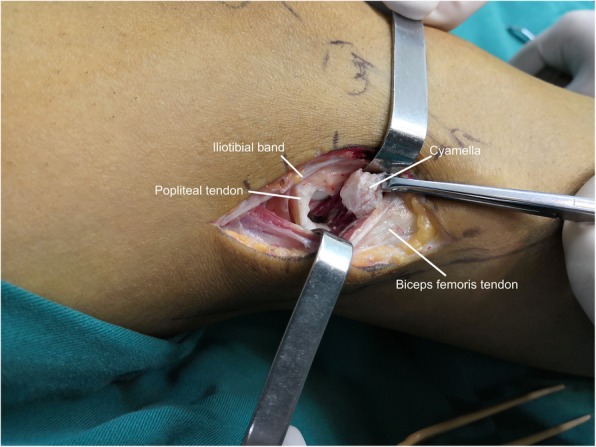
Excising the cyamella through a lateral incision, note the cyamella located near the musculo-tendinous intersection of the popliteus muscle
Fig. 5.
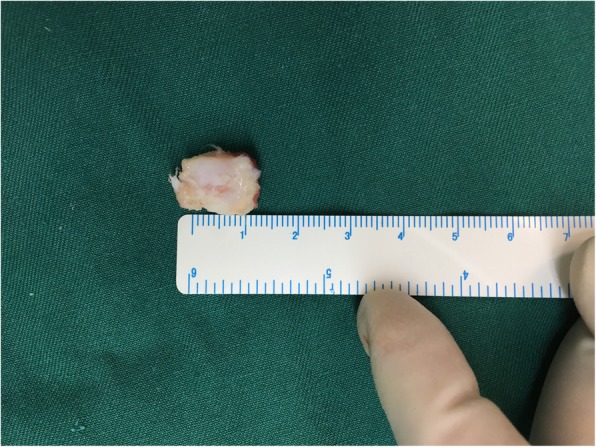
Excised cyamella
Fig. 6.
Postoperative radiograph after excision of cyamella. "Lateral" indicates lateral side of the knee, "Medial" indicates medial side of the knee, "Anterior" indicates anterior side of the knee, "Posterior" indicates posterior side of the knee
Postoperatively, the patient recovered well and had immediate relief after treatment. He was able to return to physical fitness activities at 8-week follow-up.
Discussion and conclusions
Snapping knee is defined as a patient hearing or feeling a snapping or popping of joints at some specific activity [3]. Some differentials for the snapping knee include the presence of a discoid meniscus [4], rheumatoid nodules [5], iliotibial band (ITB) friction [6], biceps femoris tendon [7], semitendinosus and gracilis tendons [8], popliteus tendon [9, 10] and intra-articular pathological changes. Snapping of the knee caused by symptomatic cyamella in the popliteus tendon however, is extremely rare and has never been reported in the literature.
Cyamella, the sesamoid bones of the popliteus muscle, are rare in humans. While in animal research, they are thought to assist in muscle function by modifying pressure, diminishing friction and altering the direction of the pull [1]. Studies have shown a close interaction between intrinsic genetic factors and extrinsic epigenetic stimuli ultimately controls the development and evolution of sesamoid bones [11]. The cyamella is located in either the popliteus muscle or adjacent to its myotendinous junction. Other knee sesamoid bones include the patella and fabella. The fabella is located within the lateral head of the gastrocnemius muscle and posterior to the lateral femoral condyle [12].
In the present case, we found Cabot sign could reproduce the snapping while other spacial tests were unremarkable. The Cabot test is performed on the patient in a supine position with the involved knee flexed with the lower leg crossed over the contralateral leg. The patient is then asked to extend the knee while the examiner palpates the lateral joint line. The sign is considered positive when snapping is elicited upon knee extension. We noted that this is a typical physical examination for differential diagnosis of the snapping knee [10].
Isolated case reports include the imaging appearance of cyamella. CT showed cyamella to be a well-corticated ossicle with a hypodense center due to the presence of marrow fat [13]. On T1-, T2-, and T2*-weighted MRI scans, a cyamella presents as an ossicle with low signal intensity along its borders [14]. According to these results, we were able to exclude an osteochondral flake, a loose body or a periosseous calcification in this case, the diagnosis of a cyamella was given. Ultrasound has its unique value in diagnosis and evaluation of snapping knee. The benefit of musculoskeletal ultrasound includes quick examination, high accuracy and no radiation [15–17]. As the patient did MRI scans in the first place, we did not employ ultrasound for diagnosis.
The review of the literature available via the PubMed online data revealed four case reports associated with symptomatic cyamella in the popliteus tendon [18–21]. The results are summarized in Table 1.
Table 1.
Details derived from four case reports
| Mishra.1996 [15] | Benthien.2010 [16] | Dheer.2012 [17] | Rehmatullah.2014 [18] | |
|---|---|---|---|---|
| Age of patient | 28Y | 25Y | 14Y | 64Y |
| Symptoms | Unable to bear weight,swelling | Posterolateral knee pain,swelling and discomfort for 6 weeks | Lateral knee pain,swelling, inability to fully extend his knee | Intermittent knee pain for 4 months |
| History of trauma | Y | N | N | Y |
| Treatment | Arthroscopy | Physical therapy | Not mentioned | Hinge brace |
| Follow up | Asymptomatic after 6 weeks | Asymptomatic after 1 year | Not mentioned | Symptoms reoccurred once the brace was removed |
The novelty of this article includes the following points. Firstly, the unique clinical feature in this case is lateral knee snapping while pain, swelling, discomfort were reported in previous case reports. During the surgery, we found a cyamella adjacent to myotendinous junction of popliteus tendon and snapping of the popliteus tendon over the cyamella. This is previously unreported in the existing literature. We postulate that the unique clinical feature is associated with the location and size of cyamella. Secondly, we reported surgical excision in dealing with snapping knee caused by symptomatic cyamella for the first time and achieved satisfied outcome after 8 weeks follow-up. The treatment of existing case reports includes physical therapy, hinge brace and arthroscopy, the pathology of snapping is unclear and the clinical outcome is uncertain. Thirdly, we noted that Cabot sign is a typical physical examination for differential diagnosis of the lateral snapping knee, Cabot sign could reproduce the unique snapping while other spacial tests were unremarkable, thus a symptomatic cyamella should be considered as differential diagnosis. Fourthly, we proposed that symptomatic cyamella in the popliteus tendon should be considered as part of the differential diagnosis of the snapping knee. Many differentials for the snapping knee have been reported as mentioned above, symptomatic cyamella in the popliteus tendon causing snapping knee is identified for the first time and should be considered in clinical works.
The reported case is the first that the authors have evaluated with a symptomatic cyamella in the popliteus tendon as an etiology for snapping knee. This was an unexpected finding intraoperatively and was only discovered by directly visualizing and palpating the popliteus tendon snapping over the cyamella during passive range of motion. This case offers a contribution by adding to the differential diagnosis that should be considered in the evaluation of snapping knee syndrome.
Although not previously suggested, symptomatic cyamella in the popliteus tendon should be considered as part of the differential diagnosis of the snapping knee. Although an early diagnosis could be difficult to establish, the typical MRI is an ovoid structure with internal cancellous bone signal in the popliteus tendon. An open excision of the cyamella is the optimum surgical treatment for this condition.
Supplementary information
Additional file 1. A reproducible audible and palpable snapping of the lateral knee when moving from flexion to extension.
Additional file 2. In the surgery, we found there was snapping of the popliteus tendon over the cyamella.
Additional file 3. After excision surgery, the snapping was gone.
Acknowledgements
Not applicable.
Authors’ contributions
SS did the data collection and writing. YL was a major contributor in writing the manuscript. YC and ZL contributed to the conception and design of the study. All authors read and approved the final manuscript.
Funding
There is no funding received for this paper.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Shouwen Su and Yunxiang Lu contributed equally to this work.
Contributor Information
Shouwen Su, Email: sushouwen@qq.com.
Yunxiang Lu, Email: luyunxiang321@163.com.
Yuxian Chen, Email: 2280702284@qq.com.
Zhiyong Li, Email: doclizhiyong8369@163.com.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s12891-019-2882-8.
References
- 1.Le Minor JM. Brief communication: the popliteal sesamoid bone (cyamella) in primates. Am J Phys Anthropol. 1992;87:107–110. doi: 10.1002/ajpa.1330870109. [DOI] [PubMed] [Google Scholar]
- 2.Marchand AJ, Proisy M, Ropars M, et al. Snapping knee: imaging findings with an emphasis on dynamic sonography. AJR Am J Roentgenol. 2012;199:142–150. doi: 10.2214/AJR.11.7817. [DOI] [PubMed] [Google Scholar]
- 3.Date H, Hayakawa K, Nakagawa K, et al. Snapping knee due to the biceps femoris tendon treated with repositioning of the anomalous tibial insertion. Knee Surg Sports Traumatol Arthrosc. 2012;20:1581–1583. doi: 10.1007/s00167-011-1778-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen LX, Ao YF, Yu JK, et al. Clinical features and prognosis of discoid medial meniscus. Knee Surg Sports Traumatol Arthrosc. 2013;21:398–402. doi: 10.1007/s00167-012-1979-5. [DOI] [PubMed] [Google Scholar]
- 5.Chu A, Ginat D, Terzakis J, et al. Chronic sarcoid arthritis presenting as an intra-articular knee mass. J Clin Rheumatol. 2009;15:190–192. doi: 10.1097/RHU.0b013e3181a61c29. [DOI] [PubMed] [Google Scholar]
- 6.Ilizaliturri JVM, Camacho-Galindo J. Endoscopic treatment of snapping hips, iliotibial band, and iliopsoas tendon. Sports Med Arthrosc. 2010;18:120–127. doi: 10.1097/JSA.0b013e3181dc57a5. [DOI] [PubMed] [Google Scholar]
- 7.Bernhardson AS, LaPrade RF. Snapping biceps femoris tendon treated with an anatomic repair. Knee Surg Sports Traumatol Arthrosc. 2010;18:1110–1112. doi: 10.1007/s00167-009-1018-3. [DOI] [PubMed] [Google Scholar]
- 8.von Dercks N, Theopold JD, Marquass B, et al. Snapping knee syndrome caused by semitendinosus and semimembranosus tendons. A case report. Knee. 2016;23:1168–1171. doi: 10.1016/j.knee.2016.10.003. [DOI] [PubMed] [Google Scholar]
- 9.Krause DA, Stuart MJ. Snapping popliteus tendon in a 21-year-old female. J Orthop Sports Phys Ther. 2008;38:191. doi: 10.2519/jospt.2008.2698. [DOI] [PubMed] [Google Scholar]
- 10.Mariani PP, Mauro CS, Margheritini F. Arthroscopic diagnosis of the snapping Popliteus tendon. Arthroscopy. 2005;21:888–892. doi: 10.1016/j.arthro.2005.04.103. [DOI] [PubMed] [Google Scholar]
- 11.Sarin VK, Erickson GM, Giori NJ, et al. Coincident development of sesamoid bones and clues to their evolution. Anat Rec. 1999;257:174–180. doi: 10.1002/(SICI)1097-0185(19991015)257:5<174::AID-AR6>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- 12.Zeng S, Dong X, Dang R, et al. Anatomic study of fabella and its surrounding structures in a Chinese population. Surg Radiol Anat. 2012;34:65–71. doi: 10.1007/s00276-011-0828-4. [DOI] [PubMed] [Google Scholar]
- 13.Akansel G, Inan N, Sarisoy HT, et al. Popliteus muscle sesamoid bone (cyamella): appearance on radiographs, CT and MRI. Surg Radiol Anat. 2006;28:642–645. doi: 10.1007/s00276-006-0134-8. [DOI] [PubMed] [Google Scholar]
- 14.Munk PL, Althathlol A, Rashid F, et al. MR features of a giant cyamella in a patient with osteoarthritis. Skelet Radiol. 2009;38:69. doi: 10.1007/s00256-008-0582-9. [DOI] [PubMed] [Google Scholar]
- 15.Chang KV, Wu WT, Han DS, et al. Static and dynamic shoulder imaging to predict initial effectiveness and recurrence after ultrasound-guided subacromial corticosteroid injections. Arch Phys Med Rehabil. 2017;98:1984–1994. doi: 10.1016/j.apmr.2017.01.022. [DOI] [PubMed] [Google Scholar]
- 16.Chang KV, Wu WT, Huang KC, et al. Limb muscle quality and quantity in elderly adults with dynapenia but not sarcopenia: an ultrasound imaging study. Exp Gerontol. 2018;108:54–61. doi: 10.1016/j.exger.2018.03.019. [DOI] [PubMed] [Google Scholar]
- 17.Wu W, Chang K, Mezian K, et al. Basis of shoulder nerve entrapment syndrome: an Ultrasonographic study exploring factors influencing cross-sectional area of the Suprascapular nerve. Front Neurol. 2018;9:902. [DOI] [PMC free article] [PubMed]
- 18.Mishra AK, Jurist KA. Symptomatic cyamella. Arthroscopy. 1996;12:327–329. doi: 10.1016/S0749-8063(96)90068-7. [DOI] [PubMed] [Google Scholar]
- 19.Benthien JP, Brunner A. A symptomatic sesamoid bone in the popliteus muscle (cyamella) Musculoskelet Surg. 2010;94:141–144. doi: 10.1007/s12306-010-0083-6. [DOI] [PubMed] [Google Scholar]
- 20.Dheer S, Silverberg C, Zoga AC, et al. A 14-year-old with lateral knee pain and locking. Skelet Radiol. 2012;41:1339–1340. doi: 10.1007/s00256-011-1286-0. [DOI] [PubMed] [Google Scholar]
- 21.Rehmatullah N, McNair R, Sanchez-Ballester J. A cyamella causing popliteal tendonitis. Ann R Coll Surg Engl. 2014;96:1–3. doi: 10.1308/003588414X13824511649931. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. A reproducible audible and palpable snapping of the lateral knee when moving from flexion to extension.
Additional file 2. In the surgery, we found there was snapping of the popliteus tendon over the cyamella.
Additional file 3. After excision surgery, the snapping was gone.
Data Availability Statement
Not applicable.