

Abstract
Background
Pedestrian-related injuries are a significant contributor to preventable mortality and disability in children. We hypothesized that interactive pedestrian safety education is associated with increased knowledge, safe crosswalk behaviors, and lower incidence of pedestrian-related injuries in elementary school-aged children.
Methods
An interactive street crossing simulation was implemented at target elementary schools in Los Angeles County beginning in 2009. Mixed-methods were used to evaluate the impact of this intervention. Multiple-choice exams were used to test pedestrian safety knowledge, anonymous observations were used to assess street-crossing behaviors, and statewide traffic records were used to report pedestrian injuries in elementary school-aged (4–11 y) children in participating school districts. Pedestrian injury incidence was compared one year before and after the intervention, standardized to the incidence in the entire city of Los Angeles.
Results
A total of 1424 and 1522 children completed the pre-test and post-test, respectively. Correct answers increased for nine out of ten questions (all p<0.01). Children more frequently looked both ways before crossing the street after the intervention (10% vs 41%, p<0.001). There were 6 reported pedestrian-related injuries in intervention school districts in the year prior to the intervention and 2 injuries in the year after the intervention, resulting in a significantly lower injury incidence (standardized rate ratio 0.28; 95% CI, 0.11–0.73).
Conclusion
Pedestrian safety education at Los Angeles elementary schools was associated with increased knowledge, safe street crossing behavior, and lower incidence of pediatric pedestrian-related injury. Formal pedestrian safety education should be considered with injury prevention efforts in similar urban communities.
Keywords: Injury prevention, pediatric, pedestrian, crosswalk, street, safety
Introduction
Unintentional injury is the leading cause of mortality in children.1 Pedestrian-related injury in children under 15 years old accounted for 380 deaths and 2,404 hospitalizations in 2015 alone.2 Children who sustain injuries during street crossing are at increased risk for traumatic brain injury – a leading cause of long-term morbidity and societal health care expenditures.3 Recognized risk factors for pedestrian-related injury include male gender, age 5–9 years, nonwhite race, urban areas, and low socioeconomic status.4–7 These risk factors suggest that elementary school children in major cities represent an important target for injury prevention efforts.
While several studies have found street safety education to be a valuable means to promote increased knowledge and safe pedestrian behaviors,8–13 there is limited data linking these interventions to a reduction in pedestrian-related injury.14 Incorporation of law enforcement into pedestrian injury prevention efforts has also not been evaluated. This study aimed to 1) determine the association between police-administered education and pedestrian safety knowledge and safe street crossing behaviors, and 2) assess the impact of pedestrian safety education on the incidence of pedestrian injury in elementary school-aged children. We hypothesized that this intervention would be associated with improved knowledge, safer pedestrian behaviors, and a lower incidence of pedestrian-related injury in our target population.
Methods
Study Design and Cohort Selection
This study used a mixed-methods design. Institutional Review Board approval was obtained from the Children’s Hospital Los Angeles. There were two different cohorts that were analyzed for this study. Our Injury Prevention staff administered the education up until 2017, at which point a partnership was forged with the Los Angeles Police Department (LAPD) and police officers became the primary educators thereafter. We therefore measured the specific impact of police-administered education on knowledge and behaviors using data from 7 elementary schools that were educated by law enforcement from 2017–2018. Children in grades one through three were the target participants in the educational intervention. All participants were anonymous and no demographic information was obtained. For the global assessment of the impact of our program on injury incidence, we used registry data from census tracts surrounding a cohort of 10 elementary schools that received pedestrian safety education over a five-year period (2012 to 2017, allowing one-year follow-up for interventions in 2017).
Pedestrian Safety Educational Intervention
Los Angeles Street Smarts is a pedestrian safety educational initiative created by our Injury Prevention team at Children’s Hospital Los Angeles. The program started in 2009 with a goal to prevent pedestrian-related injury in elementary-school children in Los Angeles county. The educational curriculum uses an immersive, life-size set (Richie’s Neighborhood) including controllable street lights/signs (Figure 1) to allow children to practice street safety behaviors and receive feedback in real time. The set is deployed at participating schools for one day and education is typically administered to a single classroom of students at a time over a one-hour period.
Figure 1.

Photo of Los Angeles Street Smarts interactive set used for pedestrian safety educational intervention.
Pre-Post Test and Street Crossing Observations
A multiple-choice exam (Supplemental Figure) was used to test pedestrian safety knowledge and perceptions of law enforcement officers before and after the intervention. Responses were anonymous and thus individual test scores could not be linked pre- and post-intervention. The exam was administered by classroom teachers, typically one day before and again immediately after the intervention. The exam included three questions (Q5, 7, & 9) specifically designed to assess the child’s perception of police officers. There was one question related to responsibility for pedestrian safety added to the exam (Q10) during the study period.
Street crossing behavior was anonymously observed by study personnel outside each school one week before and one week after the intervention. The observations were conducted during the morning or afternoon commute to maximize the number of potential observations. Specific behaviors that were evaluated included 1) looked both ways before crossing the street, 2) obeyed traffic signals, 3) crossed at designed crosswalk, and 4) crossed with an adult. Observations were random, but study personnel aimed to alternate observing male and female children. Age was estimated by observers as one of two categories (5–6 or 7–10 years) for observed children.
Pedestrian-Related Injury Incidence
Elementary school zoning maps were used to identify street crossings within participating school districts. These street crossings were then provided to an analyst with the California Highway Patrol that used the Statewide Integrated Traffic Records System (SWITRS) to generate pedestrian-related injury reports for the target school districts. The SWITRS database includes all traffic incidents reported by authorities in the state of California. Data from SWITRS is considered public record and it contains no identifying information. Pedestrian-related injury events were obtained one year before and one year after the intervention. We only recorded injuries in elementary-aged children (4–10 years) before the intervention, and 5–11 years old after the intervention (to account for the intervention group aging one year). The denominator required for calculation of injury incidence was estimated using United States Census Bureau 2010 Census data (https://factfinder-census-gov) to calculate the number of children in the target age strata living in each school district (using zip codes) before and after the intervention. The standard population chosen for this study was all elementary school-aged children residing within the City of Los Angeles from 2011 to 2017.
Statistical Analysis
The frequency of correct answers to individual test questions and the number of safe street crossing behaviors were compared before and after the intervention using the Chi-square test of independence. Comparisons could not be paired between groups because all tests results and observations were anonymous.
The number of pedestrian-related injuries reported in elementary aged children living in the zip codes of 10 target schools were used to calculate the rate of pedestrian-related injury per person-time at risk 1 year pre- and 1-year post-implementation of the intervention. Due to the rarity of observed events, the crude rate ratio was calculated for only the combined total person-time, summed over all participating schools. The relationship between the rate of injuries before and after the intervention was investigated in school-level data by negative binomial regression. An offset term of log (person-time) was fitted in the model to allow for the varying person-time at risk. A rate ratio was calculated using the number of reported injuries and person-time of exposure in each period.
Because the intervention occurred in different calendar years in each of the elementary schools, Los Angeles city census data spanning all analyzed years (2011–2017) were utilized as the standard population to adjust for possible temporal changes in injury rates in the general population. Injury rates from the same calendar year in the overall Los Angeles city population were used along with the person-time of exposure to calculate the expected number of injuries in a given school/year. The standardized risk ratio was calculated as the ratio of the actual number of injuries over the number expected based on the rates in the standard population in a given calendar year. The log of the expected numbers of injuries at each school was used as an offset term in a negative binomial regression model where the estimate of association was the standardized rate ratio. Our threshold for statistical significance was p<0.05. All statistical analyses were conducting using SAS software v. 9.4 (SAS Institute Inc., Cary, NC).
Results
Pre-Post Test Scores
A total of 1424 and 1522 children completed the pre-test and post-test, respectively (Table 1). The number of correct answers significantly increased for nine out of the ten questions, including all three questions assessing perception of police officers (all p<0.01). The highest increase occurred for Q6 (‘How do you know if a driver has seen you?’): 24% vs 59% on the pre- and post-test, respectively. The only question for which there was no significant increase in correct answers was Q1 (‘What sign do you look for to cross the street?’): 83% vs 84%, p=0.45.
Table 1:
Comparison of pedestrian safety exam results before and after the educational intervention.
| Question | Pre (N=1424) | Post (N=1522) | P-value* |
|---|---|---|---|
| Q1: What sign do you look for to cross the street? | 1182 (83) | 1280 (84) | 0.453 |
| Q2: Who should be with you when crossing the street? | 1229 (86) | 1365 (90) | 0.006 |
| Q3: What is the first thing you do before crossing the street? | 423 (30) | 688 (45) | <0.001 |
| Q4: Before taking you first step, which way should you look? | 1131 (79) | 1310 (86) | <0.001 |
| Q5: A police officer’s job is to… | 1101 (77) | 1256 (83) | <0.001 |
| Q6: How do you know if a driver has seen you? | 339 (24) | 904 (59) | <0.001 |
| Q7: How do you feel when you see a police officer? | 987 (69) | 1143 (75) | <0.001 |
| Q8: What should you do if you see a friend going after a ball in the street? | 836 (59) | 1273 (84) | <0.001 |
| Q9: Who should you ask for help? | 1224 (86) | 1395 (92) | <0.001 |
| Q10: Who is responsible for your safety? | 98 (26)± | 149 (40)± | <0.001 |
Results reported as N (%).
N=372 (Pre) and N=374 (Post) children answered Q10 when it was added to the exam.
Chi-square
Safe Street Crossing Behaviors
We observed 250 children crossing the street before the intervention and 396 after (Table 2). There was a significant increase in the number of children that looked both ways before crossing the street (41% vs 10%, p<0.001). There was a significant decrease in the number of children who crossed with an adult (85% vs 74%, p=0.013). There was no significant difference in the number of children who obeyed traffic signals or crossed at the designated crosswalk after the intervention.
Table 2:
Street crossing observations before and after the educational intervention.
| Observation | Pre (N=250) | Post (N=396) | P-value |
|---|---|---|---|
| Younger age (5–6 y) | 103 (41) | 146 (37) | 0.320 |
| Male gender | 127 (51) | 231 (58) | 0.073 |
| Looked both ways | 26 (10) | 161 (41) | <0.001 |
| Obeyed traffic signals | 192 (80) | 324 (82) | 0.485 |
| Crossed at designated crosswalk | 207 (83) | 345 (87) | 0.241 |
| Crossed with adult | 121 (85) | 174 (74) | 0.013 |
Results reported as N (%).
Chi-square
Pedestrian Injury Incidence Data
There was a decline in the total number of pedestrian-related injuries in elementary school aged children in the entire City of Los Angeles over the study period (Figure 2). The incidence of reported pedestrian-related injury was 6 out of 49,322 children 1-year pre-intervention (incidence rate 1.22 injuries per 10,000 children, Table 3). In the 1-year post-intervention period, there were 2 reported injuries out of 49,581 children (incidence rate 0.40 per 10,000 children). This resulted in a rate ratio of 0.33 (95% CI, 0.19–0.58; p<0.001) post versus pre-intervention (Table 3). After adjusting for the expected number of injuries in each school based on Los Angeles city census data, the standardized rate ratio was 0.28 (0.11–0.73, p=0.009).
Figure 2.
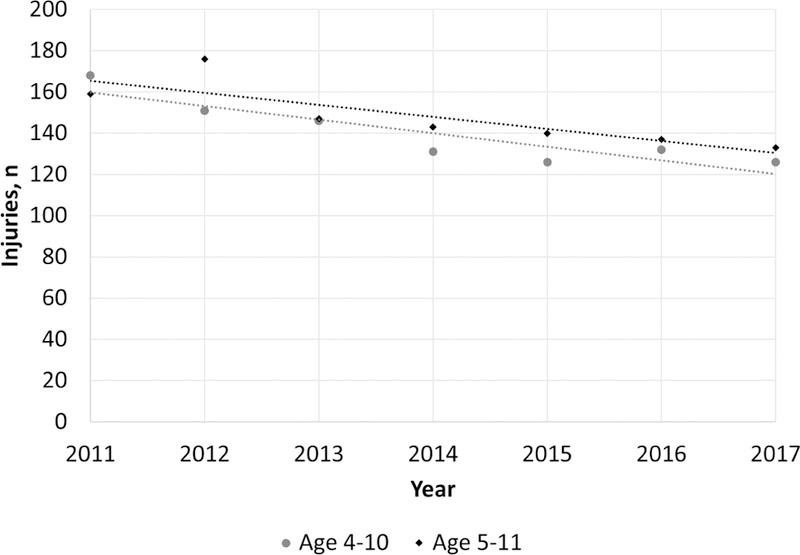
Annual pedestrian-related injuries in the entire City of Los Angeles.
Table 3:
Incidence of pedestrian-related injury by participating school before and after the intervention.
| School | Pre | Post | Model | |||||
|---|---|---|---|---|---|---|---|---|
| Injuries | Total person-time at risk, y a | IR b | Injuries | Total person-time at risk, y a | IR b | Rate ratioc (95% CI) | Standardized rate ratiod (95% CI) | |
| 1 | 1 | 10787 | 0.93 | 0 | 10930 | 0 | ||
| 2 | 3 | 1309 | 22.92 | 1 | 1277 | 7.83 | ||
| 3 | 0 | 10787 | 0 | 0 | 10930 | 0 | ||
| 4 | 0 | 3581 | 0 | 0 | 3498 | 0 | ||
| 5 | 0 | 2476 | 0 | 0 | 2635 | 0 | ||
| 6 | 1 | 4019 | 2.49 | 0 | 4019 | 0 | ||
| 7 | 1 | 3833 | 2.61 | 0 | 3796 | 0 | ||
| 8 | 0 | 5629 | 0 | 0 | 5600 | 0 | ||
| 9 | 0 | 2860 | 0 | 0 | 2880 | 0 | ||
| 10 | 0 | 4041 | 0 | 1 | 4016 | 2.49 | ||
| Total | 6 | 49322 | 1.22 | 2 | 49581 | 0.40 | 0.33 (0.19, 0.58)* | 0.28 (0.11, 0.73)* |
Total number of elementary-age children within the zip coverage of each school during the 1-year pre/post pedestrian safety education.
Incidence rate per 10,000 children/year
Rate ratio (post-vs. pre-) from negative binomial model using person-time denominators in each exposure period.
Standardized rate ratio (post-vs. pre-) from negative binomial regression. Expected number of events calculated using Los Angeles city census data as the standard population.
p<0.01
Discussion
This retrospective cohort study demonstrated the impact of an immersive street safety educational course for elementary school-aged children. Improvements were observed both in measured street safety knowledge and in observed behavior change. We also observed a decline in the number of children who crossed the street with an adult after the intervention, which may reflect increased confidence. Children also more frequently indicated a positive perception of law enforcement officers after the education. School districts that received the education had a lower incidence of pedestrian-related injury one year after the intervention. These findings indicate that Los Angeles Street Smarts may have several societal benefits related to injury prevention and police-community relations.
Previous data supporting the association between educational interventions and pediatric pedestrian-related injury are limited.14 Our finding of a lower injury incidence after education is consistent with Durkin et al,15 a study conducted in northern Manhattan which examined a robust injury prevention program targeting elementary school children. They demonstrated a decline in pedestrian-related injury, with the largest reduction occurring in children 6–10 years old. One of the first reported pedestrian educational campaigns began in the 1970s (“Willy Whistle”) in Los Angeles, Milwaukee, and Columbus, Ohio. The Willy Whistle campaign was associated with a decline in childhood ‘dart and dash’ type injuries.16 A study from Norway found that a multifaceted traffic injury prevention program was associated with a significant decline in both pedestrian and bicycle related injuries in children under 16 years old.17 The ‘WalkSafe’ school-based educational program in Miami-Dade county was similarly associated with a decline in childhood pedestrian injury rates.6
One of the unique aspects of this study was the incorporation of law enforcement as the primary educators. There were two particularly novel findings related to this interaction: 1) children more frequently reported feeling safe when they see a police officer, and 2) children were more likely to report they would ask an officer for help. Although the effect sizes were modest, these findings may reflect a more positive perception of law enforcement. The LAPD has previously acknowledged the past use of biased policing and the presence of discrimination.19 It has also been reported that minority groups are more likely to anticipate discrimination from legal authorities.20 Interventions like LA Street Smarts may be an innovative way to promote positive interactions between police and our communities.
There were several limitations inherent to this study. First, the educational intervention was only delivered once to each of the examined schools. Repetition may be key to long-lasting effects on behavior, and the lack of which may have lessened the impact of our intervention. We also only measured knowledge and behavior outcomes immediately before and after the intervention, so a sustained improvement could not be determined. Second, pedestrian injury incidence was estimated using traffic incident records and 2010 Census data, thus generating only a rough approximation of the true injury incidence. We were unable to account for injuries that were never reported, or perhaps ‘near-misses’ in which children were struck by a vehicle without sustaining an injury, or almost struck by a vehicle. Third, the standard population utilized in this study (children in the city of Los Angeles) was not ideally assembled. Some schools in the city of Los Angeles may have received pedestrian safety education independent of our program. However, if this were true it would likely bias our results towards the null hypothesis, implying that the true impact of LA Street Smarts may be more dramatic than what we found. Fourth, the multiple-choice exam used in this study has not been validated as an accurate measurement of street crossing knowledge or a child’s perception of law enforcement. Another limitation was the lack of reporting potential environmental risk factors (such as presence of construction, malfunctioning gates, etc.) at intervention schools, possibly resulting in unmeasured confounding. Finally, the low number of overall injuries reported in this study suggests that our main findings may have been subject to type II error, and the true impact of our intervention may be underestimated. The low number of events also implies that our data should be interpreted cautiously, and future analyses with larger sample size of intervention schools are needed to validate our findings.
Despite the limitations to this observational study, our results indicate that LA Street Smarts is an effective pedestrian injury prevention program for elementary school children. Integration of law enforcement led to an improved perception of police officers, in addition to improved knowledge and safe pedestrian behaviors. These results are likely generalizable to most urban communities. Long-term follow-up data is needed to confirm a sustained effect of this intervention.
Supplementary Material
Acknowledgements:
Many thanks to Jose Haro and Gurwinder Rakkar of the California Highway Patrol for providing the SWITRS data. We would also like to thank the Los Angeles Police Department for their continued hard work and dedication to injury prevention education.
Funding: This work was supported by grants KL2TR001854, UL1TR001855, and UL1TR000130 from the National Center for Advancing Translational Science (NCATS) of the U.S. National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest: None of the authors have any conflicts of interest to disclose.
Children’s Hospital Los Angeles Institutional Review Board Exemption: CHLA-18–00155
References
- 1.National Center for Injury Prevention and Control, CDC using WISQARS. Ten Leading Causes of Death by Age Group, United States - 2015 https://www.cdc.gov/injury/wisqars/LeadingCauses.html. Accessed May 17, 2017.
- 2.Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-Based Injury Statistics Query and Reporting System (WISQARS) www.cdc.gov/injury/wisqars. Accessed March 23, 2018.
- 3.Wheeler-Martin K, Mooney SJ, Lee DC, Rundle A, DiMaggio C. Pediatric emergency department visits for pedestrian and bicyclist injuries in the US. Inj Epidemiol 2017;4(1):31. doi: 10.1186/s40621-017-0128-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chakravarthy B, Anderson CL, Ludlow J, Lotfipour S, Vaca FE. A geographic analysis of collisions involving child pedestrians in a large Southern California county. Traffic Inj Prev 2012;13(2):193–198. doi: 10.1080/15389588.2011.642034 [DOI] [PubMed] [Google Scholar]
- 5.Rivara FP, Barber M. Demographic analysis of childhood pedestrian injuries. Pediatrics 1985;76(3):375–381. [PubMed] [Google Scholar]
- 6.Hotz G, Kennedy A, Lutfi K, Cohn SM. Preventing pediatric pedestrian injuries. J Trauma 2009;66(5):1492–1499. doi: 10.1097/TA.0b013e31819d9c9b [DOI] [PubMed] [Google Scholar]
- 7.Braddock M, Lapidus G, Gregorio D, Kapp M, Banco L. Population, income, and ecological correlates of child pedestrian injury. Pediatrics 1991;88(6):1242–1247. [PubMed] [Google Scholar]
- 8.Hotz G, Cohn S, Castelblanco A, et al. WalkSafe: a school-based pedestrian safety intervention program. Traffic Inj Prev 2004;5(4):382–389. doi: 10.1080/15389580490510507 [DOI] [PubMed] [Google Scholar]
- 9.Hotz G, de Marcilla AG, Lutfi K, Kennedy A, Castellon P, Duncan R. The WalkSafe Program: Developing and Evaluating the Educational Component. J Trauma-Inj Infect 2009;66(3). doi: 10.1097/TA.0b013e3181937f62 [DOI] [PubMed] [Google Scholar]
- 10.Rivara FP, Booth CL, Bergman AB, Rogers LW, Weiss J. Prevention of pedestrian injuries to children: effectiveness of a school training program. Pediatrics 1991;88(4):770–775. [PubMed] [Google Scholar]
- 11.Schwebel DC, McClure LA, Severson J. Teaching Children to Cross Streets Safely: A Randomized Controlled Trial. Health Psychol 2014;33(7):628–638. doi: 10.1037/hea0000032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schwebel DC, McClure LA. Training Children in Pedestrian Safety: Distinguishing Gains in Knowledge from Gains in Safe Behavior. J Prim Prev 2014;35(3):151–162. doi: 10.1007/s10935-014-0341-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bachman SL, Arbogast H, Ruiz P, et al. A School-Hospital Partnership Increases Knowledge of Pedestrian and Motor Vehicle Safety. J Community Health 2015;40(6):1057–1064. doi: 10.1007/s10900-015-0031-3 [DOI] [PubMed] [Google Scholar]
- 14.Turner C, McClure R, Nixon J, Spinks A. Community-based programmes to prevent pedestrian injuries in children 0–14 years: a systematic review. Inj Control Saf Promot 2004;11(4):231–237. doi: 10.1080/156609704/233/289751 [DOI] [PubMed] [Google Scholar]
- 15.Durkin MS, Laraque D, Lubman I, Barlow B. Epidemiology and prevention of traffic injuries to urban children and adolescents. Pediatrics 1999;103(6):e74. [DOI] [PubMed] [Google Scholar]
- 16.Preusser DF. Reducing pedestrian crashes among children. Bull N Y Acad Med 1988;64(7):623–631. [PMC free article] [PubMed] [Google Scholar]
- 17.Ytterstad B. The Harstad injury prevention study: hospital-based injury recording used for outcome evaluation of community-based prevention of bicyclist and pedestrian injury. Scand J Prim Health Care 1995;13(2):141–149. [DOI] [PubMed] [Google Scholar]
- 18.Tracy ET, Englum BR, Barbas AS, Foley C, Rice HE, Shapiro ML. Pediatric injury patterns by year of age. J Pediatr Surg 2013;48(6):1384–1388. doi: 10.1016/j.jpedsurg.2013.03.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Beck C. Report of the Los Angeles Police Department on the Prevention and Elimination of Biased Policing.; 2016 https://www.documentcloud.org/documents/3219728-161115-LAPD-RacialBias.html. Accessed March 29, 2018.
- 20.Woolard JL, Harvell S, Graham S. Anticipatory injustice among adolescents: age and racial/ethnic differences in perceived unfairness of the justice system. Behav Sci Law 2008;26(2):207–226. doi: 10.1002/bsl.805 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.