

Abstract
Background
The aim of this study was to assess the association between foot deformities and type of shoe regularly worn at work.
Material/Methods
We studied 150 employed women ages 30–40 years and divided them into 3 groups according to type of footwear worn: women in Group I wore flat-soled shoes, women in Group II wore mid-heeled shoes (heels 4.0±0.5 cm), and women in Group III wore high-heeled shoes (heels 10.0±0.5 cm). We used the CQ-ST podoscope for measurements.
Results
We found significant differences in right foot γ angle between Groups I and III (p=0.033) and between Groups II and III (p=0.040). For the left foot, differences were noted between Groups I and III (p=0.012). Group III subjects had higher values of α angle compared to Group I (p=0.000) and Group II (p=0.000). Significant correlations were also found between specific type of footwear worn and the incidence of hallux valgus of the right foot (p=0.010) and left foot (p=0.000), and the varus deformity of the fifth toe (β) of the left foot (p=0.015).
Conclusions
The feet of women wearing high-heeled shoes were significantly flatter transversely, with a more laterally flexed hallux, as compared to those wearing low-heeled or flat-soled shoes. Wearing high-heeled shoes was associated with higher incidence of hallux valgus. The incidence of varus deformity of the fifth toe was associated with wearing high-heeled shoes.
MeSH Keywords: Foot Bones, Foot Deformities, Insurance Benefits
Background
The feet are a vital static-dynamic component of human motor system, whose overall functionality is determined by genetic, environmental, and socio-economic factors, as well as by individual lifestyle [1–3].
Gorter et al. [4] highlighted intersex differences in the construction of women’s and men’s feet. Due to a weaker muscle-ligament structure, women’s feet are characterized by a lower capacity and load tolerance than are men’s feet. Female sex a is a bona fide risk factor for any non-traumatic foot problems lasting longer than 4 weeks. Perera et al. [5] established that, in comparison to men, women have a more fragile foot structure, including the heads and bones of the metatarsals, which are smaller and more rounded. This obviously calls for extra care when selecting footwear. Ryan et al. [6] and Wyderka et al. [7] found that wearing properly selected footwear is important in preventing injuries to the lower limbs and deformation of the feet. However, Lorkowski et al. [8] reported that professionally active women, striving to comply with the “business dress code”, were often required to wear uncomfortable and confining footwear. They pointed out that many employers have stringent expectations regarding their female employee’s business attire, and they believe that high-heeled shoes naturally complement women’s outfits worn at work. According to Hsue and Su [9], 59% of women in industrialized countries wear high-heeled shoes every day for 1–8 h. De Oliveira Pezzan et al. [10] distinguished several types of high-heeled shoes: open-toed vs. closed-toed, with tips that are square, round, or conical. The latter, with pointed tips, have limited toe space, which squeezes the metatarsophalangeal joints. Nguyen et al. [11] discussed differences in construction of women’s vs. men’s footwear, especially in sole thickness and width of the front part, concluding that women who follow modern fashion trends tend to change shoes often, and therefore often fail to pay sufficient attention to quality and construction. Most men, however, tend to buy shoes that are sturdier and more durable. Perera et al. [5] argue that women’s footwear should be designed according to a specific pattern, closely reflecting the structure of women’s feet, and that women’s shoes should not differ from men’s in key quality features. According to Duda [12], footwear should be closely adapted to constantly changing trends and user requirements.
The present study aimed to assess the association of foot structure with the height of the heel of footwear worn at work, in conjunction with foot deformities.
The following research questions were addressed:
Does heel height of shoes used for work affect the structure of women’s feet?
Are there any relationships between specific types of footwear worn at work and the incidence of women’s foot deformities?
Material and Methods
Study participants
The study involved professionally active women ages 30–40 years who live in the Brzozów administrative district. The district of Brzozów was randomly selected as a research site out of 380 administrative districts within the country. The sample size needed was estimated to be 352 based on a 95% confidence level and a 5% level error.
Inclusion criteria were: lack of any diseases and/or injuries of the musculoskeletal system; feet with no previous surgical interventions, including lower limbs; no genetically-dependent hallux valgus, as confirmed through an interview; wearing specific type of footwear at work for a minimum of 8 h a day, 5 days a week during the last 5 years preceding the study. To rule out any elements of chance and/or inadvertent errors in recruiting participants, the investigators ensured to have their decisions on admission into the study well-grounded in individual employee records covering the last 5 years preceding the study, primarily with regard to individual “job description” and “dress code” requirements (especially in the formal, professional attire category) actually articulating specific expectations of the management with respect to the footwear to be worn at work by their female staff. The recruitment process was thus highly objective, which increases the credibility of our results.
Exclusion criteria were: pregnancy; underweight, overweight, or obese; refusal to participate in the study.
Following completion of the allocation procedure, it was established that 188 women could not take part in the study protocol owing to their non-compliance with the study criteria. There were 150 women enrolled into the study, and we assigned them to 3 equal-sized, 50-person groups according to the type of shoe worn. Group I consisted of 50 women wearing the flat-soled shoes, Group II consisted of 50 women wearing medium-heeled shoes (4.00±0.50 cm), and Group III consisted of 50 women wearing high-heeled shoes (10.00±0.50 cm).
The stages of subject inclusion in the study are shown in Figure 1.
Figure 1.
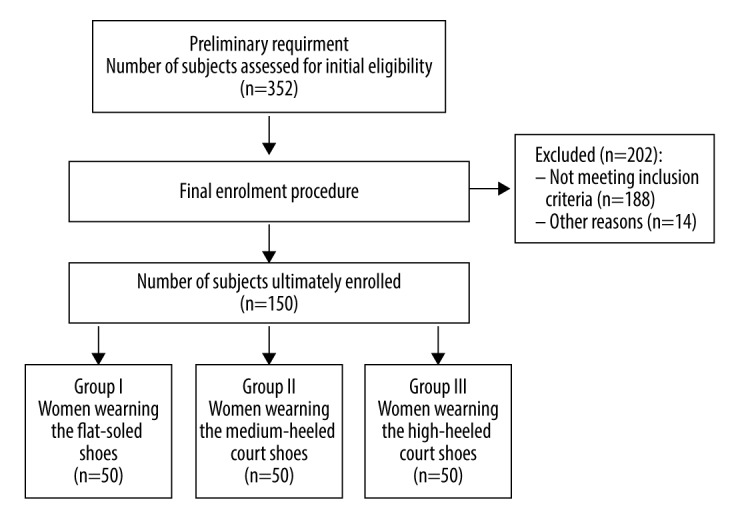
Flow of participants through the study.
The average age of the women in Group I was χ̄=34.08±3.76 years, in Group II χ̄=34.38±3.78 years, and in Group III χ̄=36.10±3.62 years.
Table 1 contains select bodily characteristics of the subjects, indicating their homogeneity within respective groups.
Table 1.
Comparison of select bodily characteristics in respective groups of subjects.
| Group | χ̄±SD | Max.–Min. | Q25 | Me | Q75 | F/H | p |
|---|---|---|---|---|---|---|---|
| Body weight [kg] | |||||||
| I | 61.60±8.24 | 84.00–47.00 | 55.00 | 60.50 | 68.00 | F=2.62 | 0.076 |
| II | 62.12±6.31 | 78.00–48.00 | 57.00 | 62.00 | 68.00 | ||
| III | 59.02±7.06 | 75.00–46.00 | 53.00 | 57.00 | 65.00 | ||
| Body height [cm] | |||||||
| I | 165.38±5.77 | 180.00–150.00 | 163.00 | 165.00 | 168.00 | F=1.60 | 0.202 |
| II | 166.04±4.49 | 176.00–157.00 | 164.00 | 166.00 | 169.00 | ||
| III | 164.06±6.39 | 180.00–151.00 | 158.00 | 164.00 | 168.00 | ||
| BMI | |||||||
| I | 22.45±2.06 | 25.93–18.59 | 20.80 | 22.17 | 24.54 | H=3.19 | 0.203 |
| II | 22.52±1.98 | 26.03–19.23 | 20.96 | 22.18 | 24.68 | ||
| III | 21.88±1.80 | 25.00–18.83 | 20.43 | 21.23 | 23.23 | ||
χ̄ – arithmetical mean value; SD – standard deviation; Max. – maximum value; Min. – minimum value; Q25 – lower quartile; Me – median; Q75 – upper quartile; F – value of one-way variance analysis ANOVA; H – value of the Kruskal-Wallis test; p – probability value.
Examination protocol
The CQ-ST podoscope (manufactured by Electronic System, EU) was applied as the research tool of choice. The device had been entered under PL/DR 009932 reference number in the Register of Medical Devices and corporate entities in charge of their marketing and use for medical purposes. A stringent calibration procedure completed during the manufacturing process guarantees consistent accuracy of the readouts. By correction of geometric distortions, the accuracy of image reproduction is within 1 mm. The device had been granted a Declaration of Conformity (No. DS.05.2014), attesting to its full compliance with the essential requirements, as detailed in the Ordinance of the Minister of Public Health on the medical devices (Journal of Laws of 2003, No. 4, Item 45), issued pursuant to the provisions of Article 12 (2) and Article 16 (3) of the Act of July 27, 2001, on medical devices (Journal of Laws No. 126, Item 1380, and of 2002, No. 152, Item 1264).
We measured the plantar foot surfaces in a relaxed stance, with the upper limbs hanging down freely along the body. Both feet were assessed simultaneously. The width and foot angle were natural and unforced. The calculations comprised the following indices:
Foot length – the line connecting the most distal point of the forefoot (on the pad of the longest toe) with the farthest point within the hindfoot, in cm.
Foot width – the line connecting the most medially located point on the head of the first metatarsal bone (metatarsale tibiale, mtt) with the point located most laterally on the head of the 5th metatarsal bone (metatarsale fibulare, mtf), in cm.
Clarke’s angle (longitudinal foot arch) – calculated by drawing a tangent to the medial edge of the foot and the line joining the point of the largest recess of the footprint with the mtt point, in degrees.
Heel angle γ (transverse foot arch) – the angle between the tangents to the medial and lateral edge of the foot, which cross over the heel, in degrees.
Hallux valgus angle (α) – the angle between the tangent line to the medial edge of the foot and the tangent to the pad of the big toe, derived from the mtt point, in degrees.
The angle of the varus deformity of the fifth toe (β) – the angle between the tangent line to the lateral edge of the foot and the tangent to the pad of the fifth toe, derived from the mtf point, in degrees.
The method of determining the individual indicators is demonstrated in Figure 2.
Figure 2.
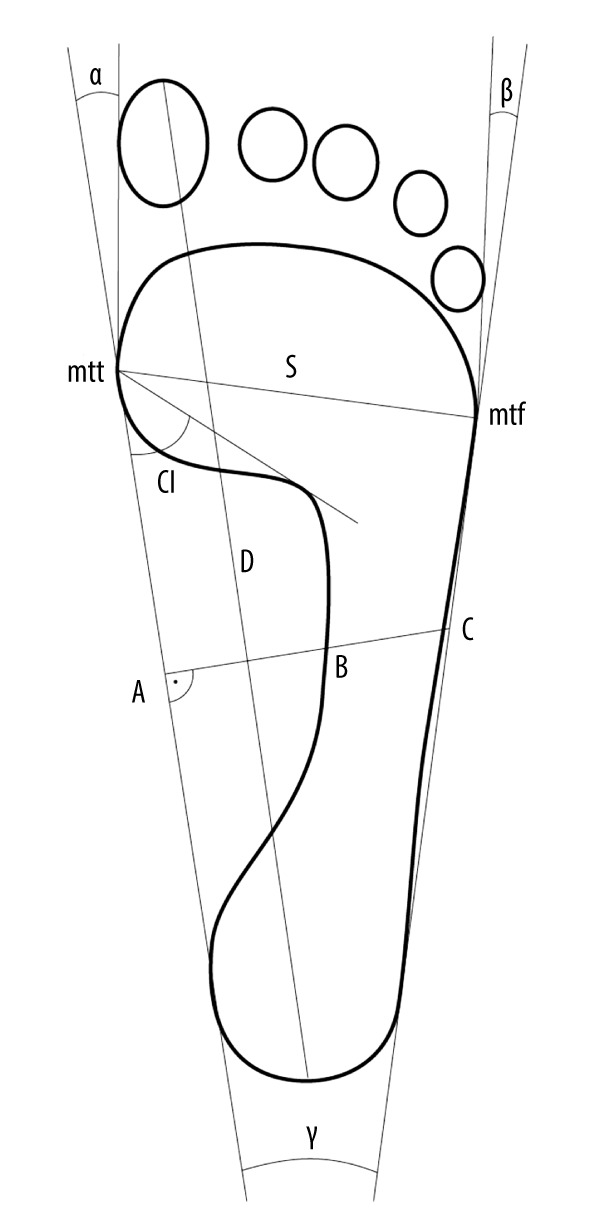
The method of determining the key indicators of foot structure.
To ensure overall integrity of the research process, all tests were carried out in the morning, using the same measuring instrument operated by the authors. Women wore their gym uniforms, and were barefooted. All study protocol procedures were pursued in full compliance with the Helsinki Declaration. All participants received detailed information regarding the study aims and methods to be applied. The study was approved and endorsed by the Bioethics Review Committee.
Statistical analysis
Based on the data collected, the descriptive statistical calculations were made. Consistency of pertinent variables with reference values in normal distribution was verified by Shapiro-Wilk test. To assess intergroup differences in the average level of numerical features, one-way analysis of variance (ANOVA) or, alternatively, Kruskal-Wallis test were applied. With regard to statistically significant differences, a post hoc test was used for multiple comparisons. The analysis of qualitative data was carried out using the Pearson chi-square test. The results were considered statistically significant if the probability level of the test was lower than the predetermined significance level of p<0.05. Stat Soft STATISTICA (version 13.1) was used to process all test results.
Results
We found no significant differences between the 3 groups in terms of right and left lower limbs, foot length and width, Clarke’s angle, and the angle of the varus deformity of the fifth toe (β) (Table 2). There was, however, a significant intergroup variation in the heel angle (γ) of the right (p=0.013) and left (p=0.014) foot, as well as the hallux valgus angle of the right (p=0.000) and left (p=0.000) foot.
Table 2.
Comparison of morphological features of the foot structure in respective study groups.
| Group | χ̄±SD | Max.–Min. | Me | χ̄±SD | Max.–Min. | Me |
|---|---|---|---|---|---|---|
| Length of the right foot [cm] | Length of the left foot [cm] | |||||
| I | 23.29±1.18 | 26.10–20.50 | 23.30 | 23.30±1.15 | 26.10–20.50 | 23.30 |
| II | 23.01±1.02 | 26.30–21.20 | 22.95 | 23.01±1.01 | 26.30–21.20 | 22.95 |
| III | 22.76±1.09 | 25.50–20.10 | 22.65 | 22.76±1.11 | 25.50–20.10 | 22.65 |
| H=5.62; p=0.059 | H=5.69; p=0.058 | |||||
| Width of the right foot [cm] | Width of the left foot [cm] | |||||
| I | 8.76±0.49 | 10.00–7.80 | 8.70 | 8.84±0.46 | 10.00–7.80 | 8.80 |
| II | 8.67±0.40 | 10.00–8.00 | 8.60 | 8.73±0.45 | 9.90–7.70 | 8.70 |
| III | 8.65±0.53 | 9.70–7.60 | 8.60 | 8.67±0.54 | 9.70–7.60 | 8.55 |
| H=1.84; p=0.397 | F=1.75; p=0.178 | |||||
| Clarke’s angle of the right foot [°] | Clarke’s angle of the left foot [°] | |||||
| I | 41.84±4.72 | 51.00–26.00 | 41.50 | 41.12±4.25 | 56.00–29.00 | 40.50 |
| II | 42.50±4.78 | 55.00–31.00 | 43.50 | 40.72±5.38 | 54.00–25.00 | 41.00 |
| III | 40.90±6.59 | 55.00–27.00 | 41.00 | 38.60±6.47 | 48.00–20.00 | 40.00 |
| H=1.32; p=0.517 | H=2.81; p=0.244 | |||||
| Heel angle (γ) of the right foot [°] | Heel angle (γ) of the left foot [°] | |||||
| I | 16.20±1.56 | 19.00–12.00 | 16.00 | 15.90±1.64 | 19.00–12.00 | 16.00 |
| II | 16.16±1.73 | 19.00–12.00 | 16.00 | 16.30±1.82 | 20.00–12.00 | 16.00 |
| III | 17.08±1.59 | 21.00–13.00 | 17.00 | 16.88±1.56 | 19.00–13.00 | 17.00 |
| H=8.70; p=0.013* | H=8.57 p=0.014* | |||||
| Hallux valgus angle (α) of the right foot [°] | Hallux valgus angle (α) of the left foot [°] | |||||
| I | 5.98±3.85 | 14.00–0.00 | 6.00 | 8.10±3.69 | 17.00–1.00 | 8.00 |
| II | 5.64±3.90 | 13.00–0.00 | 6.00 | 7.90±3.46 | 16.00–1.00 | 7.00 |
| III | 9.68±4.84 | 20.00–0.00 | 9.00 | 12.24±5.45 | 30.00–3.00 | 12.00 |
| H=21.63; p=0.000* | H=25.70; p=0.000* | |||||
| The V toe varus deformity angle (β) of the right foot [°] | The V toe varus deformity angle (β) of the left foot [°] | |||||
| I | 12.40–4.70 | 23.00–0.00 | 13.00 | 14.84±4.71 | 25.00–4.00 | 15.00 |
| II | 13.52±4.02 | 21.00–4.00 | 13.50 | 15.94±3.67 | 26.00–7.00 | 16.00 |
| III | 13.08±3.87 | 21.00–2.00 | 13.50 | 16.20±3.58 | 25.00–5.00 | 17.00 |
| F=0.90; p=0.409 | F=1.61; p=0.202 | |||||
χ̄ – arithmetical mean value; SD – standard deviation; Max. – maximum value; Min. – minimum value; Me – median; F – value of one-way variance analysis ANOVA; H – value of the Kruskal-Wallis test; p – probability value.
p<0.05.
A more detailed analysis with the post hoc test showed differences in heel angle (γ) of the right foot between Groups I and III (p=0.033) between Groups II and III (p=0.040), and for the left foot, the results differed between Groups I and III (p=0.012). The feet of women from Group III had significantly higher values of this variable (Figure 3).
Figure 3.
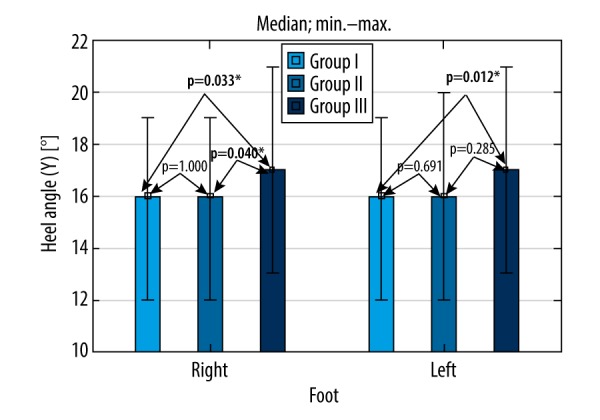
Post hoc test results comparing heel angle (γ) variables in the 3 study groups.
The post hoc test results for the right and left foot showed significant differences in the values of the hallux valgus angle (α) between Groups I and III (p=0.000) and between Groups II and III (p=0.000). Women in Group III had higher angle values than those in Groups I and II (Figure 4).
Figure 4.
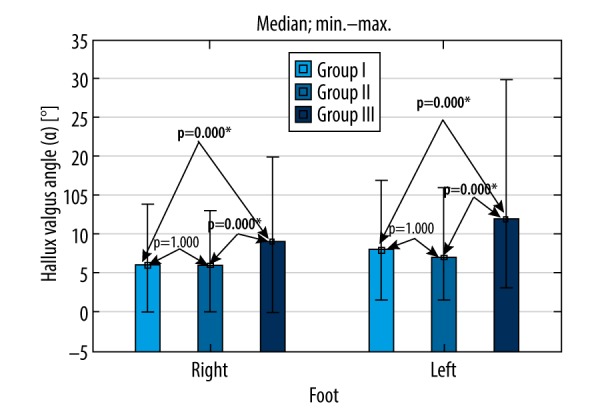
Post hoc test comparing hallux valgus angle (α) variables in the 3 study groups.
Table 3 shows there was a significant dependence between the type of footwear worn and the frequency of hallux valgus of the right foot (p=0.010) and left foot (p=0.000). In Group III, this deformation was more frequent than in Groups I and II.
Table 3.
Prevalence of the types of longitudinal and transverse arch of the feet and the hallux valgus and the varus deformity of the fifth toe in the study subjects, depending on the specific type of footwear worn.
| Feature | I | II | III | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| The medial longitudinal arch based on the Clarke’s angle | rf | Flat foot | 9 | 18.0 | 11 | 22.0 | 16 | 32.0 | 36 | 24.0 |
| Normal foot | 41 | 82.0 | 38 | 76.0 | 33 | 66.0 | 112 | 74.7 | ||
| High arched foot | 0 | 0.0 | 1 | 2.0 | 1 | 2.0 | 2 | 1.3 | ||
| χ2 (4)=4.04; p=0.400 | ||||||||||
| lf | Flat foot | 7 | 14.0 | 11 | 22.0 | 17 | 34.0 | 35 | 23.3 | |
| Normal foot | 42 | 84.0 | 38 | 76.0 | 33 | 66.0 | 113 | 75.3 | ||
| High arched foot | 1 | 2.0 | 1 | 2.0 | 0 | 0.0 | 2 | 1.3 | ||
| χ2 (4)=6.42; p=0.169 | ||||||||||
| Transverse arch based on the heel angle (γ) | rf | Flat foot | 3 | 6.0 | 3 | 6.0 | 6 | 12.0 | 12 | 8.0 |
| Normal foot | 39 | 78.0 | 39 | 78.0 | 41 | 82.0 | 119 | 79.3 | ||
| High arched foot | 8 | 16.0 | 8 | 16.0 | 3 | 6.0 | 19 | 12.7 | ||
| χ2 (4)=6.90; p=0.434 | ||||||||||
| lf | Flat foot | 1 | 2.0 | 6 | 12.0 | 6 | 12.0 | 13 | 8.7 | |
| Normal foot | 41 | 82.0 | 37 | 74.0 | 42 | 84.0 | 120 | 80.0 | ||
| High arched foot | 8 | 16.0 | 7 | 14.0 | 2 | 4.0 | 17 | 11.3 | ||
| χ2 (4)=7.84; p=0.097 | ||||||||||
| Setting of the hallux based on the hallux valgus angle (α) | rf | Normal setting of the hallux | 39 | 78.0 | 39 | 78.0 | 27 | 54.0 | 105 | 70.0 |
| Hallux valgus | 11 | 22.0 | 11 | 22.0 | 23 | 46.0 | 45 | 30.0 | ||
| χ2 (2)=9.14; p=0.010* | ||||||||||
| lf | Normal setting of the hallux | 35 | 70.0 | 37 | 74.0 | 14 | 28.0 | 86 | 57.3 | |
| Hallux valgus | 15 | 30.0 | 13 | 26.0 | 36 | 72.0 | 64 | 42.7 | ||
| χ2 (2)=26.54; p=0.000* | ||||||||||
| Setting of the V toe based on the V toe varus deformity angle (β) | rf | Normal setting of the V toe | 12 | 24.0 | 7 | 14.0 | 7 | 14.0 | 26 | 17.3 |
| The V toe varus deformity | 38 | 76.0 | 43 | 86.0 | 43 | 86.0 | 124 | 82.7 | ||
| χ2 (2)=2.32; p=0.312 | ||||||||||
| lf | Normal setting of the V toe | 8 | 16.0 | 2 | 4.0 | 1 | 2.0 | 11 | 7.3 | |
| The V toe varus deformity | 42 | 84.0 | 48 | 96.0 | 49 | 98.0 | 139 | 92.7 | ||
| χ2 (2)=8.43; p=0.015* | ||||||||||
rf – right foot; lf – left foot; n – number of observations; % – percent of observations; χ2 – value of the Pearson chi-square test; p – probability value.
p<0.05.
A similar dependence was found regarding the angle of the varus deformity of the fifth toe (β) of the left foot (p=0.015). Group III women were more likely to have varus deformity of the fifth toe than were women in Groups I and II. There was no significant intergroup diversity in the prevalence of the longitudinal and transverse arches (Table 3).
Discussion
The effect of footwear on overall condition of the motor system and various gait parameters warrant wide-scale research. Our search of the literature found no in-depth research published on the incidence of foot deformities in women wearing different types of shoes in a specific work setting for at least 8 h a day, at least 5 days a week, and for at least 5 consecutive years. Thus, based on our earlier studies assessing how the incidence of foot deformities affect various components of individual functional fitness in later life, we decided to pursue the present study.
According to Yu et al. [13], the human foot has adapted to the body’s standing posture through a longitudinal and transverse arch, whereas wearing poorly fitting shoes disrupts the three-point support of the foot, and consequently contributes to progressive foot defects. Silva et al. [14] assert that walking in high-heeled shoes causes deviations from correct posture, which may manifest through protruding head, increased lumbar lordosis, increased pelvic anteversion, valgus knees, and altered foot shape. Prolonged standing while wearing high-heeled shoes forces the center of gravity to shift forward. This in turn adversely affects the body contouring, especially in young women with developing skeletal system.
Wearing high-heeled shoes causes supination of the feet and increased pressure on the forefoot. Frey et al. [15] studied 356 women ages 20–60 years by applying a shoe outline to the footprints and conducting a diagnostic survey. To ensure reliability of the results, the center of the foot was determined by drawing a line running through the middle of the second toe and the heel, and the center of a shoe was determined by a line running through the center of the heel and the center of the distal tip of the shoe. These studies found that 88% of women wore ill-fitted footwear (too short by 1.2 cm, on average), of which 27% reported wearing high-heeled shoes; 76% had deformed feet, most commonly hallux valgus.
Borchgrevink et al. [16] used X-ray photographs and survey questionnaires in 2 groups of women (ages 40–66 years) – those wearing high-heeled shoes for at least 5 years vs. those who never wore high-heeled shoes – reporting that long-term wearing of high-heeled shoes was not associated with foot deformities, although it did contribute to discomfort and corn formation. Lorkowski et al. [8] found that over 60% of women working in large corporations, banks, and offices wear high-heeled shoes, out of which 70% report having diminished quality of life due to periodic bouts of pain and overall reduction in ability to use their feet. However, Knapik [17] found that foot deformities were not associated with wearing high-heeled shoes, but rather with wearing shoes that are too short or too narrow in the tip.
Zostawa et al. [18] examined 2 groups of women ages 19–25 years: those who reported wearing high-heeled shoes regularly for at least 5 h a day, at least 3 times a week, for a minimum of 2 years vs. those who wore flat-soled shoes only. The results of tests making use of the BTS Smart-E motion analysis system and the 2 Kistler 9286A dynamometric platforms prompted them to infer that long-term wearing of the high-heeled shoes resulted in permanently altered overall gait kinematics. In the support phase of the gait, women wearing high-heeled shoes had a significantly smaller dorsiflexion in the metatarsophalangeal joints, which initiates a chain of adverse changes directly affecting the transverse arch. The authors suggest that the actual cause of these permanent alterations is the abnormal force exerted on the tibialis anterior, gastrocnemius, and soleus muscles, which affects the rigidity of the longitudinal arch [18]. Yu et al. [13] observed that during walking in high-heeled shoes, there was a greater accumulation of pressure forces, combined with an increase in the dorsiflexion value in the metatarsophalangeal joints, as compared to walking in flat-soled shoes.
According to Szczygieł et al. [19], wearing high-heeled shoes limits overall mobility in the ankle joints and extends the gait phases. When any such non-physiologically designed footwear is worn for extensive periods of time, it overloads and widens the forefoot. Pointed and narrow tips of shoes restrain the forefoot and push the large toe sideways, towards the other toes. Wearing high-heeled shoes also has an adverse effect on the first radius of the foot. As the foot is set in plantar flexion, inversion of the first metatarsophalangeal joint and subluxation of the head and metatarsal bones occur. Hensl and Sands [20] found that hallux valgus occurred 15 times more often in people who wear shoes, but it may also occur in populations that do not wear shoes on a daily basis. In people who walk barefoot, this type of deformity is painless. Hallux valgus is more common in women than in men, with a 9: 1 sex ratio.
Women’s shoes worn during office work should first and foremost ensure foot comfort. One of the key footwear manufacturing challenges consists in offering attractive and stylish women’s shoes that are adequately tailored to requirements such as ensuring stability of the foot, adequate cushioning, adhesion, and protection.
The results of the present study suggest that high-heeled shoes could easily be replaced by attractive shoes in a variety of styles not exceeding the critical 4 cm height of the heel, which ensure stylish appearance for all female staff, but without the hazard, discomfort, and potential long-term deformities associated with wearing high-heeled shoes.
Our findings revealed that the heel height of women’s shoes was associated with the actual shape of the feet in women aged 30–40 years. The feet of women wearing high-heeled shoes were flatter and had higher incidence of valgus hallux compared to women who wore flat-soled and/or low-heeled footwear. These results suggest that wearing shoes with the heels no more than 4 cm in height may not actually be an independent factor instrumental in altering the morphology of women’s feet.
As the height of the heel increases, the pressure exerted on the forefoot becomes proportionally greater, while less pressure is placed onto the heel. Hence, walking in high-heeled footwear (i.e. heels over 10 cm in height) is significantly associated with foot morphology.
Wearing high-heeled shoes causes excessive overload of the forefoot and flexion of the toes in the interphalangeal joints, which stretches the ligaments stabilizing the transverse arch, as well as lowers the arch. Uneven distribution of pressure forces within the forefoot increases compression of the second and third metatarsal bones, which can lead to formation of calluses under the heads of these bones. As the calluses deepen, walking becomes more painful.
Mika et al. [21] reported that wearing high-heeled shoes is associated with detrimental overloading of the musculoskeletal system, and that walking in high-heeled shoes increased exertion of the gastrocnemius muscle of the calf, straight thigh muscle, and anterior tibial muscle. It follows that long-term wearing of high-heeled shoes causes overload of the muscles and damages muscle tissues. It is therefore reasonable to believe that long-term wearing of high-heeled shoes damages foot structure.
The feet of women who wear high-heeled shoes become more susceptible to degenerative changes in the active-passive stabilizers area, as well as to more appreciable deformations within their anterior-central edge. The accompanying painfulness naturally prompts women to seek ways to relieve the antero-medial edge, which in turn can further hurt the feet [22]. Our previous studies demonstrated that foot deformities reduced overall postural stability in later life [23].
The results of the present study contribute to on-going research in this subject, although further studies, to be pursued on much larger population samples and broader age groups, are still required. Given the seriousness and large scale of this issue, a target-oriented, public educational campaign should also be considered as a viable option.
Conclusions
The feet of women wearing high-heeled shoes were flatter transversely and had a more laterally flexed hallux compared to the feet of those wearing low-heeled or flat-soled shoes. Wearing high-heeled shoes was associated with hallux valgus. The incidence of varus deformity of the fifth toe was associated with the type of shoe worn – high-heeled vs. low-heeled or flat-soled.
Study limitations
A limitation of this study is that the size of the population of potential subjects was reduced by use of inclusion criteria to ensure homogeneity within each group.
Footnotes
Source of support: Departmental sources
Conflicts of interest
None.
References
- 1.D’Aout K, Pataky TC, De Clerq, Aerts P. The effects of habitual footwear use: Foot shape and function in native barefoot walkers. Footwear Sci. 2009;2(1):81–94. [Google Scholar]
- 2.Ukoha UU, Egwu OA, Umeasalugo KE, et al. Estimation of stature using footprints in an adult student population in Nigeria. Int J of Biomed Adv Res. 2013;11(4):827–33. [Google Scholar]
- 3.Vangara SV, Gopichand PVV, Bedi M, Puri M. Effect of barefoot walking on foot arch structure in Tribal children. Asian J Med Sci. 2016;7(5):108–16. [Google Scholar]
- 4.Gorter KJ, Kuyvenhoven MM, de Melker RA. Nontraumatic foot complaints in older people. A population-based survey of risk factors, mobility, and well-being. J Am Podiatr Med Assoc. 2000;90(8):397–402. doi: 10.7547/87507315-90-8-397. [DOI] [PubMed] [Google Scholar]
- 5.Perera AM, Mason L, Stephens MM. The pathogenesis of hallux valgus. J Bone Joint Surg Am. 2011;93(17):1650–61. doi: 10.2106/JBJS.H.01630. [DOI] [PubMed] [Google Scholar]
- 6.Ryan BM, Mac Lean Cl, Taunton J. A review of anthropometric, biomechanical, neuromuscular and training related factors associated witch injury in runners. Int Sport Med J. 2006;7(2):120–37. [Google Scholar]
- 7.Wyderka MI, Gronowska T, Szeląg E. The crooked foot and the quality of life. Polish Nursing. 2013;49(3):169–75. [Google Scholar]
- 8.Lorkowski J, Mrzygłód MW, Kotela I, et al. Footwear according to the “business dress code”, and the health condition of women’s feet – computer-assisted holistic evaluation. Ann Acad Med Stetin. 2013;59(2):118–28. [PubMed] [Google Scholar]
- 9.Hsue BJ, Su FC. Kinematics and kinetics of the lower extremities of young and elder women during stairs ascent while wearing low and high-heeled shoes. J Electromyogr Kinesiol. 2009;19(6):1071–78. doi: 10.1016/j.jelekin.2008.09.005. [DOI] [PubMed] [Google Scholar]
- 10.De Oliveira Pezzan PA, João SM, Ribeiro AP, et al. Postural assessment of lumbar lordosis and pelvic alignment angles in adolescent users and nonusers of high-heeled shoes. J Manipulative Physiol Ther. 2011;34(9):614–21. doi: 10.1016/j.jmpt.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 11.Nguyen US, Hillstrom HJ, Li W, et al. Factors associated with hallux valgus in a population-based study of older women and men: The MOBILIZE Boston Study. Osteoarthritis Cartilage. 2010;18(1):41–46. doi: 10.1016/j.joca.2009.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Duda I. Problems of comfort and safety of footwear use. Zeszyty Naukowe Akademii Ekonomicznej w Krakowie. 2005;685:5–17. [Google Scholar]
- 13.Yu J, Cheung JT, Fan Y, Zhang Y, Leung AK, Zhang M. Development of a finite element model of female foot for high-heeled shoe design. Clin Biomech. 2008;23(1):31–38. doi: 10.1016/j.clinbiomech.2007.09.005. [DOI] [PubMed] [Google Scholar]
- 14.Silva AM, de Siqueira GR, da Silva GA. Implications of high-heeled shoes on body posture of adolescents. Rev Paul Pediatr. 2013;31(2):265–71. doi: 10.1590/s0103-05822013000200020. [DOI] [PubMed] [Google Scholar]
- 15.Frey C, Thompson F, Smith J, et al. American orthopaedic foot and ankle society women’s shoe survey. Foot Ankle. 1993;14(2):78–81. doi: 10.1177/107110079301400204. [DOI] [PubMed] [Google Scholar]
- 16.Borchgrevink GE, Viset AT, Witsø E, et al. Does the use of high-heeled shoes lead to fore-foot pathology? A controlled cohort study comprising 197 women. Foot Ankle Surg. 2016;22(4):239–43. doi: 10.1016/j.fas.2015.10.004. [DOI] [PubMed] [Google Scholar]
- 17.Knapik H. The angles of valgity of the first toe and varus deformity of the fifth toe in school age children from the physiotherapeutic, orthopedic, and ergonomic perspective. Pol J Physiother. 2001;2:135–42. [Google Scholar]
- 18.Zostawa P, Uscinowicz N, Klich S, et al. [Kinematic assessment of women’s gait in high-heeledshoes]. Prz Med Uniw Rzesz Inst Leków. 2014;12(3):216–23. [in Polish] [Google Scholar]
- 19.Szczygiel E, Golec E, Golec J, et al. Comparative analysis of distribution on the sole surface of arched feet and flat feet. Przeg Lek. 2008;65(1):4–7. [PubMed] [Google Scholar]
- 20.Hensl EK, Sands A. Hallux valgus Foot & ankle: Core knowledge in orthopaedics. New York: Elsevier Inc; 2007. [Google Scholar]
- 21.Mika A, Oleksy Ł, Mika P, et al. The influence of heel height on lower extremity kinematics and leg muscle activity during gait in young and middle-aged women. Gait Posture. 2012;35(4):677–80. doi: 10.1016/j.gaitpost.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 22.Puszczalowska-Lizis E, Bujas P, Omorczyk J, Nosiadek L. Relations between morphological features of feet in elderly people. Medical Studies. 2018;34(1):57–63. [Google Scholar]
- 23.Puszczalowska-Lizis E, Bujas P, Omorczyk J, et al. Feet deformities are correlated with impaired balance and postural stability in seniors over 75. PLoS One. 2017;12(9):e0183227. doi: 10.1371/journal.pone.0183227. [DOI] [PMC free article] [PubMed] [Google Scholar]